
Abstract
Introduction:
Many patients have spiritual or cultural preferences regarding the disposal and reclamation of amputated parts, yet little is known about the current process. Our goal was to understand patient preferences and increase patient education regarding amputation disposal and reclamation.
Methods:
A quality improvement approach was used. Stakeholders were interviewed to process map current methods. Amputation patients were surveyed to determine preferences for amputation disposal and reclamation. Using the Plan-Do-Study-Act, change concepts were applied and outcomes measured through the same survey. Descriptive methods, analysis of variance, unpaired t-tests, and run/statistical process control charts were used for analysis.
Results:
Stakeholders identified barriers against amputation reclamation, including lack of patient access to resources, limited provider clarity surrounding the process, and no standardized policies. Baseline preferences were first gathered from 31 patients: 42% felt educated about the disposal process, 42% were concerned about the treatment of their amputated part, 74% wished to be more informed, and 16% wanted to reclaim their part. Change concepts were then implemented. First, a presentation was given at teaching rounds for medical trainees and staff. Results showed no significant change. Second, an educational handout about amputation disposal was distributed to patients. This showed a significant improvement in patient education, decreased concern for the management of amputated parts, and decreased needs for further discussion with health care providers.
Conclusions:
Many patients have preferences for amputation disposal. Patients mostly value education and awareness. The format through which education is provided is important—access to educational material may be most beneficial for patients.
Introduction
An estimated 57.7 million people worldwide live with a limb amputation from a traumatic cause. 1 Although there is existing literature surrounding lower limb amputations, much less research has been conducted on upper extremity amputations. 2 Upper extremity amputations can be particularly stressful, as they can significantly impact range of motion and functional outcomes, therefore affecting activities of daily living and work. 3 As such, health care providers have a duty to make the process as patient-centered as possible to ease each patient’s stress.
A lack of transparency regarding the management of one’s amputated part postoperatively can also be a source of anxiety. 4 The dignified disposal and reclamation of amputated parts may hold great significance to patients, but their preferences are often not considered, despite ownership of their body part. 4 Although this affects all amputation patients, it can be of particular importance to minority patients who tend to have culturally or spiritually driven preferences. 1 Yet, patients’ wishes for disposal are not routinely taken into consideration.
A review of the literature revealed a lack of patient and provider awareness of amputation disposal and reclamation policies, as well as no standardized policies in place across North America. 5 Medical waste, including excised specimens from patients, is regulated by individual state environmental and health departments, rather than federal governments. 6 This may lead to a lack of clarity surrounding a centralized process for amputated part disposal. Similarly, at our institution, a tertiary-level care hospital in a major urban setting that specializes in province-wide coverage for replantation and complex hand injuries, no standard protocol facilitates the disposal and reclamation of amputated digits and limbs. Postoperatively, amputated parts are either sent to the Pathology department or disposed of as biohazardous infectious medical waste. The handling and disposal of medical waste primarily consists of using techniques such as thermal treatment (eg, microwave technologies), autoclaving, electropyrolysis, and chemical mechanical systems. 7
Patient preferences are not routinely considered, as patients are not offered the option to preserve the amputated part upfront nor are they informed of the process. Some cultures may have specific preferences and wish to dispose of amputated parts in a particular way. 8 For example, in Islamic culture, all body parts should be washed, purified, and shrouded inside mosques before burial; cremation is taboo. 9 In some Roman Catholic communities, individuals may prefer to bury their body parts in consecrated ground and may prefer to be buried wholly with their body part at death. 10 The current process for amputation disposal is neither culturally sensitive nor patient-centered, and patients must initiate the conversation themselves to reclaim their parts, which may be a barrier.
As such, the goal of our study was to further understand patient preferences and increase education regarding management of amputated parts. Our specific aims were:
To understand patient preferences from surveying at least 70% of the patient population who are treated for a digit amputation at the Hand and Wrist Clinic of our institution more than 1 year.
To increase the proportion of patients who feel educated about amputation disposal from ~40% to >80% more than 1 year at the Hand and Wrist Clinic of our institution.
Methods
Institutional ethics review was approved from the University Health Network for this quality improvement study.
To gain insight into the current institutional amputation disposal and reclamation process, relevant stakeholders were interviewed, including pathologists, Operating Room nurses, Emergency Room nurses, orthopedic technicians, hand therapists, staff surgeons, and trainees (Figure 1). The Patient Relations and Legal Operations and Privacy Teams were also interviewed to obtain a systems-level understanding of the existing policies. A process map was collated based on the findings of these interviews (Figure 2). 11 A fishbone diagram, an effective method for analyzing root cause analysis, 12 was also created to highlight barriers to patient education and amputation reclamation (Figure 3).

A diagram that highlights the stakeholders involved in the amputation disposal and reclamation process.
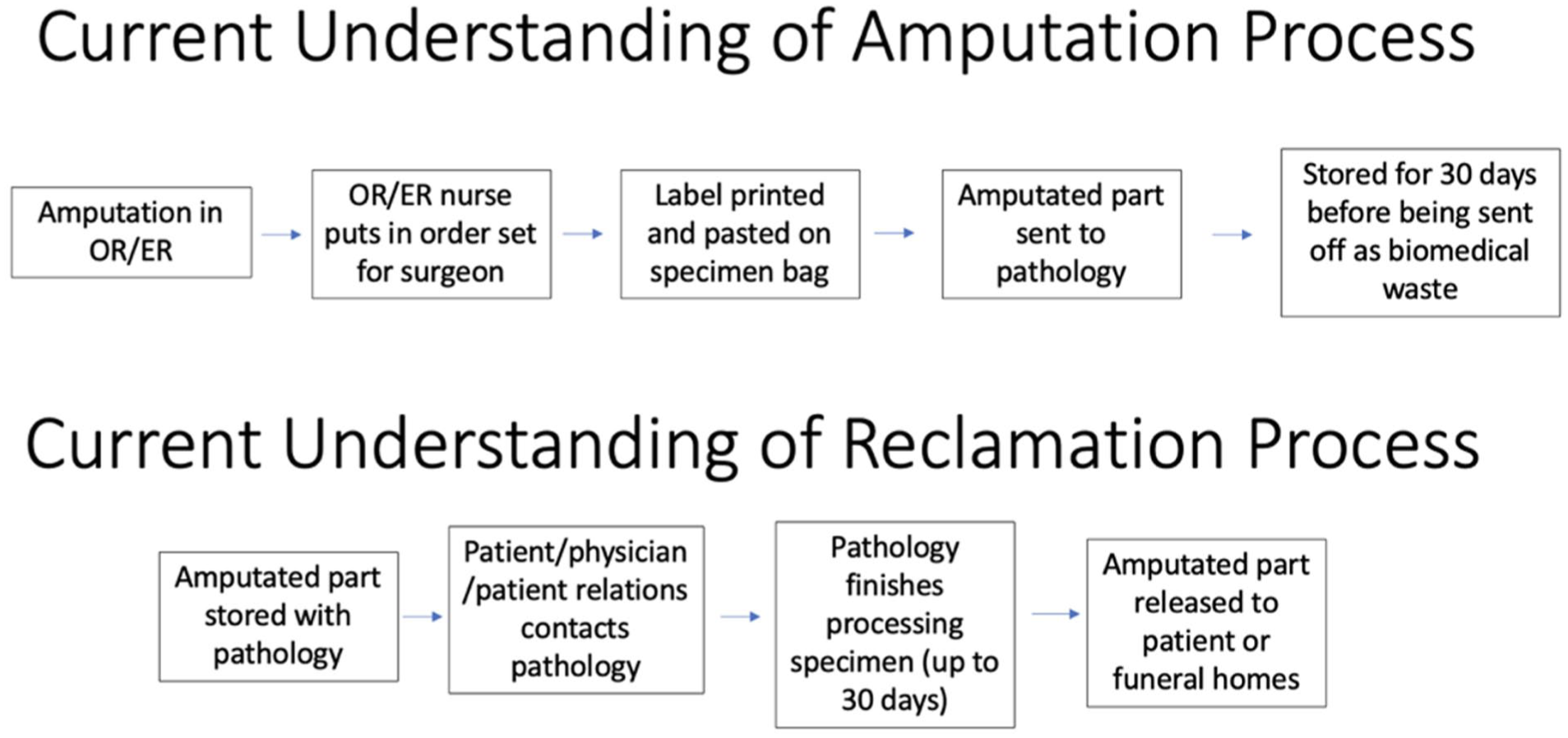
A process map of how amputation disposal and reclamation takes place at our institution.
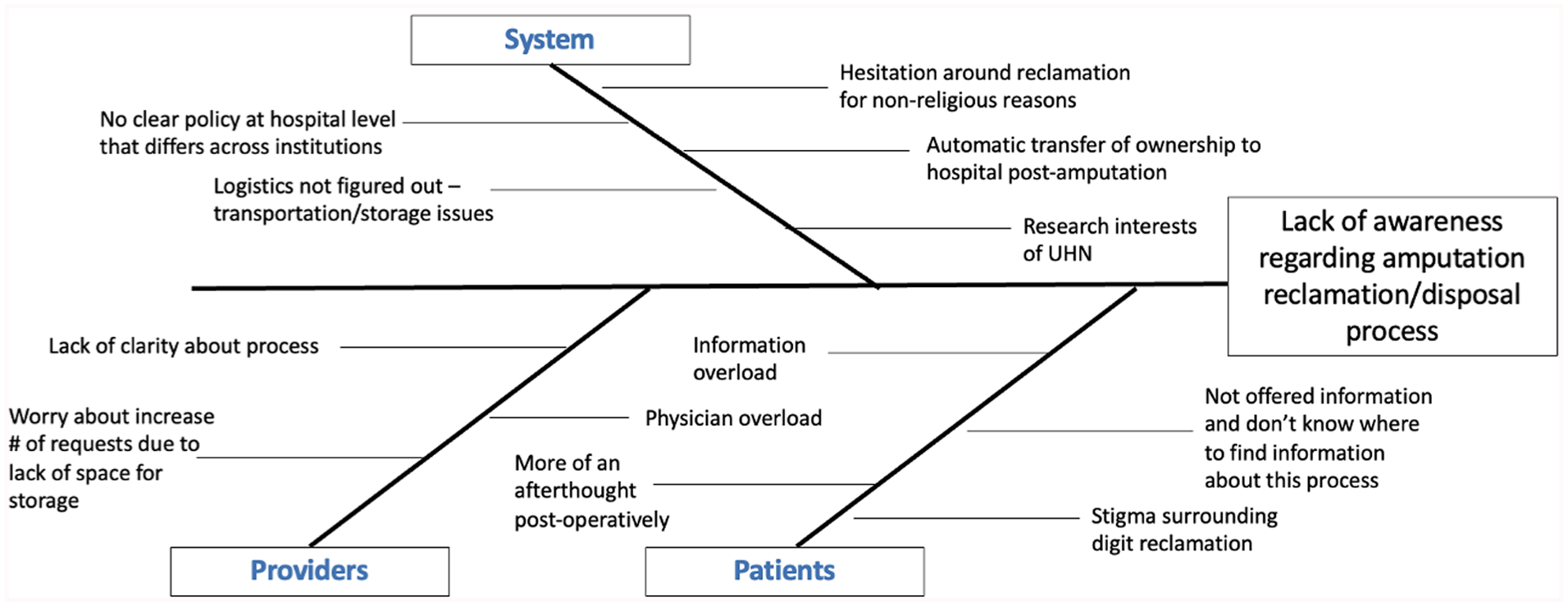
A fishbone diagram of barriers to amputation reclamation at the patient, provider, and systems level.
To gather a baseline understanding of patient preferences, a brief questionnaire was administered to patients aged 18 or older who had sustained a digital or partial hand amputation (Supplemental Material 1, Supplemental Material 2). Baseline patient preferences were collected for 3 months and were re-assessed throughout the study period via ongoing administration of the survey.
After initial diagnostics and generation of potential interventions, we proceeded with implementing 2 separate change concepts sequentially based on surgeon and patient education. This followed the Plan-Do-Study-Act, a quality improvement framework that iteratively improves current processes and assesses the effectiveness of change. 13 First, we gave an online presentation to educate attending surgeons and trainees on baseline patient preferences and the results of the stakeholder interviews. After 4 months, we re-assessed the survey results. Second, patient educational material on the amputation disposal process was distributed at follow-up appointments (Supplemental Material 3). The handout was a 1-page document that described how amputated parts are disposed of at our institution, including the typical pathway that includes Pathology review and incineration. Changes in survey results were subsequently measured for another 6 months.
We defined our outcomes via the Yes/No statements from the survey, namely patient-reported: awareness of the amputation disposal and reclamation process, interest in learning more about the process, concern about the process, interest in having further discussions with the health care team, and desire to reclaim the amputated part.
Descriptive methods were used to process map and define barriers to our project. Data were organized using run/statistical process control charts (p-charts). A 1-way analysis of variance (ANOVA) and unpaired t-tests were used to analyze independent samples of data (2-tailed) before and after the implementation of each change concept. Statistical significance was set a priori at P < .05.
Results
Before examining patient preferences, preliminary data were collected from stakeholders to create a process map of the amputation disposal and reclamation methods (Figure 2).
They were also interviewed regarding barriers that hindered amputation reclamation, which can be visualized with a fishbone diagram (Figure 3). At the patient level, barriers included: (1) the potential stigma surrounding reclamation of amputated parts; and (2) not being offered information about the process or option for amputate reclamation. On the provider level, barriers included a lack of clarity around the process and concern for further overload for physicians and storage in hospital. From a systems perspective, stakeholders understood no clear policy in place and wondered if the logistics of storage and transportation of the amputated part postoperatively would be too burdensome. There was uncertainty about potential competing interests, as the hospital may wish to preserve the amputated part for research, whereas patients may wish to reclaim their part for religious or personal reasons.
After interviewing stakeholders, 64 of 76 eligible patients (84%) were surveyed between June 2022 and 2023. Their demographics can be seen in Table 1. Four patients refused, 2 were no-shows, and 6 were missed.
A Table of Demographics for All the Patients Who Answered the Survey.
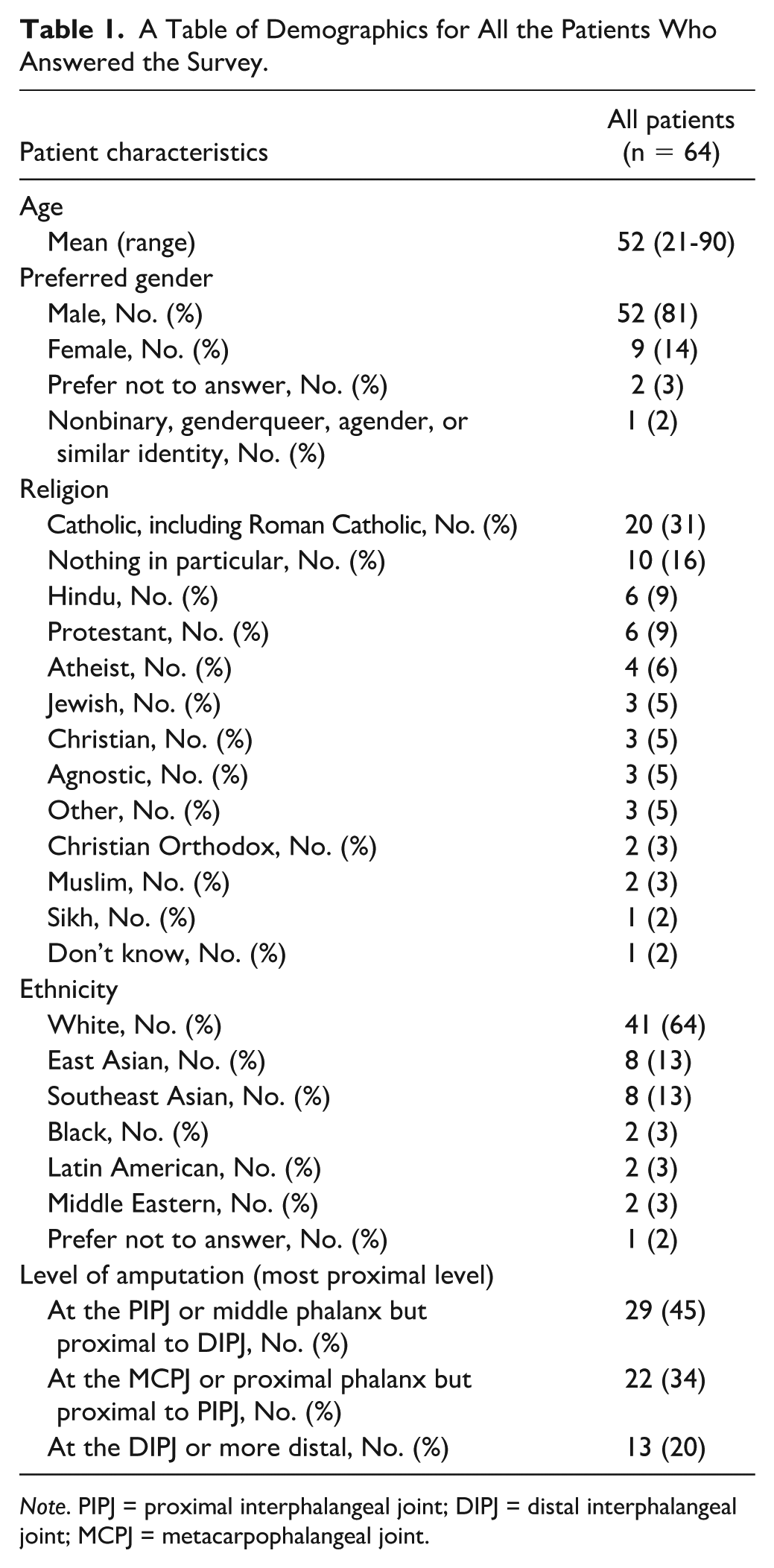
Note. PIPJ = proximal interphalangeal joint; DIPJ = distal interphalangeal joint; MCPJ = metacarpophalangeal joint.
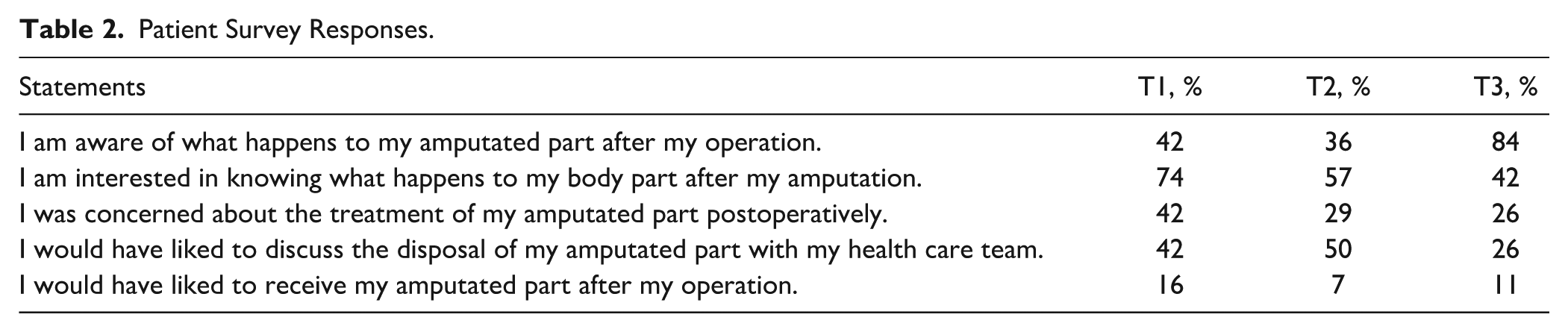
We collected results regarding baseline patient preferences (T1), after the online presentation (T2), and after distribution of the educational printout (T3). Significant results from the survey are displayed as a run chart, a tool that is frequently used to highlight the quality of the performance of a process in quality improvement frameworks. 14 This can be seen in Figure 4, which shows the change in patient awareness of the amputation disposal process during our study period. We were able to achieve our aim of increasing patient awareness from ~40% to greater than 80% between T1 and T3. The answers from the remainder of the survey can be seen in Table 2, which highlights patient responses during each time period. After the patient educational printout was introduced at T3, there was less interest in knowing further information about the amputation disposal process, less interest in further discussion with health care providers, and less concern about the overall process.
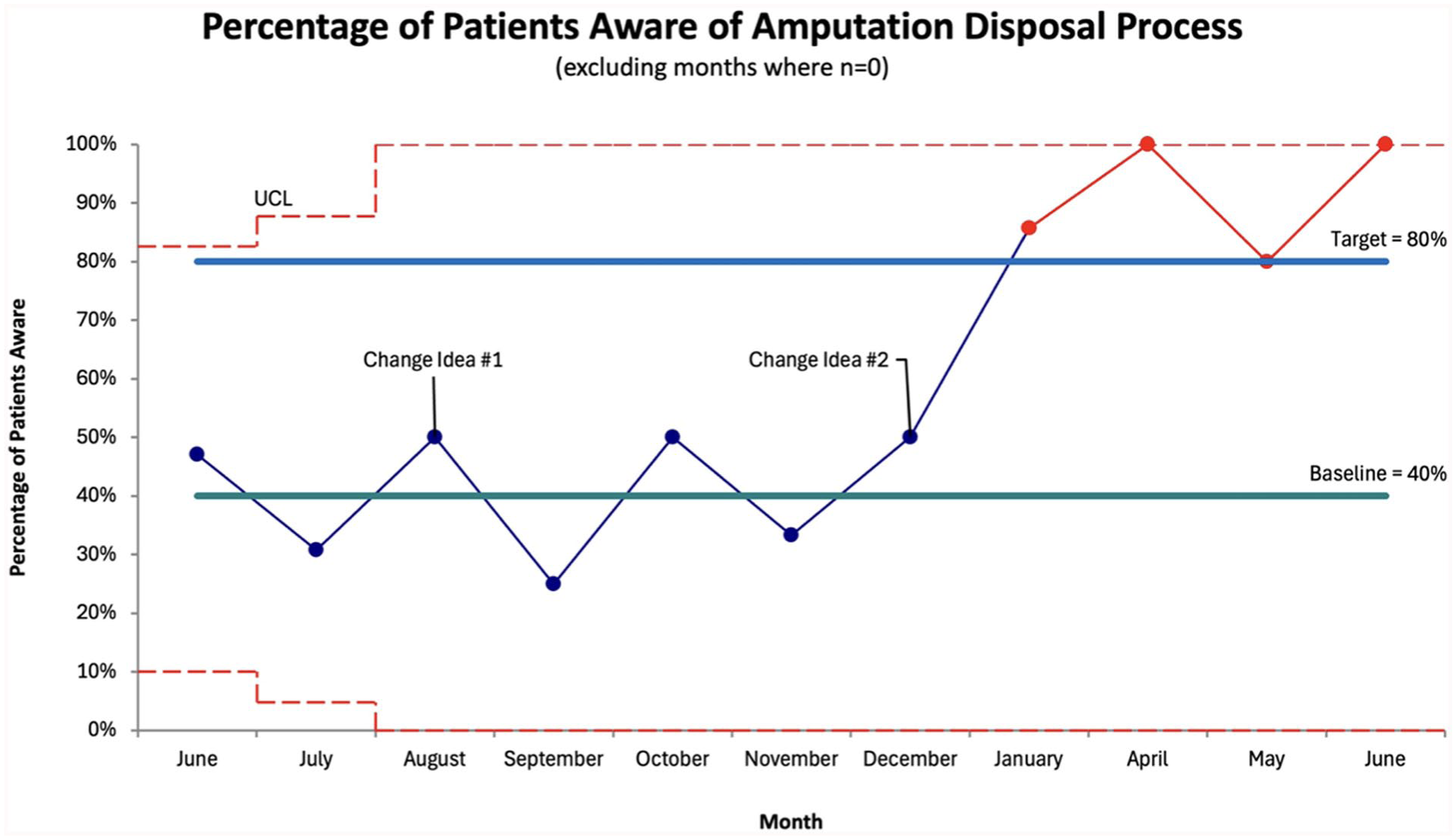
Statistical process control chart of percentage of patients aware of amputation disposal process.
Patient Survey Responses.
One-way ANOVA was also used to evaluate statistical significance between the 3 time periods. The P values can be found in Supplemental Material 4, with statistical significance demonstrated in awareness of the amputated part disposal process postoperatively (P = .00017).
We then used a 2-tailed unpaired t-test for independent samples to analyze data between T1 and T2, and then T2 and T3 separately (Supplemental Material 5). Similarly, significant results were found in awareness of the amputated part disposal process between T2 and T3 (P < .0004).
Discussion
Awareness of amputated part disposal and reclamation can be important to patients, especially for those with spiritual or cultural preferences. 15 This study highlights the value of patient education through a 2-pronged approach, offering qualitative and quantitative perspectives from interviews with stakeholders and patient surveys.
Interviewing stakeholders highlighted no clear pathway for patients to reclaim amputated parts. Each staff had a different understanding of the process and felt that it should be more culturally sensitive for patients. They found the project had good acceptability.
Results from T1 showed that most patients did not wish to reclaim their amputated part but wanted to be informed about the process. The first and second change concepts were tailored to this. T2 showed no change to any outcomes, indicating that educating staff and trainees did not translate into increased patient awareness. Significant results were seen at T3 with focused educational material for patient distributed at follow-up appointments. As demonstrated in the statistical process control chart, during the study period, our target of >80% awareness was consistently achieved only after the implementation of our second change idea in T3. Decreased concern and decreased desire for further discussion with health care providers were also noted. Our handout was effective in educating patients on amputated part disposal upfront, so they do not have to initiate the discussion.
Limitations of our study included systemic barriers to the implementation of our change concepts. Our Pathology Team noted concerns for limited staffing and storage for amputated parts. They were concerned that there would be an increase in reclamation requests after the introduction of our handout. As such, only information on amputation disposal was distributed to patients. In addition, our sample was from a single urban center from Toronto, Canada, which can limit the generalizability of our study. It may not be representative of experiences of patients from more rural areas or from other geographic locations. Patients from other settings or requiring amputation of another body part may also have other preferences. Last, our patient survey was binary and did not collect qualitative data from patients, which may have limited our understanding of the full spectrum of patient preferences and values within our sample population.
Last, certain types of strategies are known to be more effective than others for long-term sustainability. This project highlights the importance of directly educating patients; our researchers currently distribute the printout to patients. Although this is low on the hierarchy of effectiveness, it proved to be effective in the short term for our project. Higher leverage strategies such as standardization and automation can be implemented in the future to ensure that resources are consistently available, delivered, and effective beyond the focused boundaries of the current study. 16 This includes having printouts readily available in clinic or automated into the electronic medical record system to remind our staff to provide each amputation patient with a copy of the printout. This printout has already been made into an electronic version, so patients can also access it online. By providing patients with this information upfront, patients will not have to bear the burden of initiating this conversation. The automation of delivery of this handout will mitigate the disruption to clinic flow and allows it to be delivered in an accessible manner. We hope this increases cultural sensitivity and that these discussions carry forward to other hospitals. This project primarily focuses on culturally sensitive care but also highlights a knowledge gap in provider understanding of how institutions process medical waste. In addition to distributing handouts to educate patients, further research can look at systems-level education initiatives to integrate culturally sensitivity into providing patient-centered care.
Supplemental Material
sj-jpg-1-han-10.1177_15589447251387287 – Supplemental material for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project
Supplemental material, sj-jpg-1-han-10.1177_15589447251387287 for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project by Tiffany K. Y. Tse, Annie Wang, Daniel Antflek, Ryan A. Paul and Heather L. Baltzer in HAND
Supplemental Material
sj-jpg-2-han-10.1177_15589447251387287 – Supplemental material for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project
Supplemental material, sj-jpg-2-han-10.1177_15589447251387287 for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project by Tiffany K. Y. Tse, Annie Wang, Daniel Antflek, Ryan A. Paul and Heather L. Baltzer in HAND
Supplemental Material
sj-jpg-3-han-10.1177_15589447251387287 – Supplemental material for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project
Supplemental material, sj-jpg-3-han-10.1177_15589447251387287 for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project by Tiffany K. Y. Tse, Annie Wang, Daniel Antflek, Ryan A. Paul and Heather L. Baltzer in HAND
Supplemental Material
sj-jpg-4-han-10.1177_15589447251387287 – Supplemental material for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project
Supplemental material, sj-jpg-4-han-10.1177_15589447251387287 for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project by Tiffany K. Y. Tse, Annie Wang, Daniel Antflek, Ryan A. Paul and Heather L. Baltzer in HAND
Supplemental Material
sj-jpg-5-han-10.1177_15589447251387287 – Supplemental material for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project
Supplemental material, sj-jpg-5-han-10.1177_15589447251387287 for Improving Culturally Sensitive Care in Digit Amputations: A Quality Improvement Project by Tiffany K. Y. Tse, Annie Wang, Daniel Antflek, Ryan A. Paul and Heather L. Baltzer in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Animal and Human Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study. This study was approved by the Research Ethics Board from UHN.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received a $5000 grant from the UHN QI Physician’s Grant Competition in 2022. There was no other funding allocated for this project.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.