
Abstract
Background:
Currently, there is no recommended standard set of outcomes to report in Dupuytren disease treatment studies, nor are there guidelines on how the outcomes themselves should be reported. This study aimed to elicit the most salient issues for patients living with and undergoing treatment for Dupuytren disease, as well as for the hand surgeons, occupational therapists, and physical therapists caring for these patients.
Methods:
A qualitative, interpretive description study employing one-on-one semi-structured interviews was conducted. Ten surgeons, 12 occupational and physical therapists, and 10 patients were interviewed.
Results:
Priorities related to Dupuytren disease treatment and recovery differed by stakeholder group. Surgeons prioritized range of motion, recovery time, and recurrence. Physical and occupational therapists frequently mentioned range of motion, grip strength, activities of daily living, return to meaningful activities, wound healing, edema, lack of sensation, and pain as important treatment outcomes. Patients described extension deficit, activities of daily living, holding objects, and lack of sensation.
Conclusions:
Through the present study, we have identified outcomes of high importance to patients, hand surgeons, occupational therapists, and physical therapists. These results can be used to inform the development of a core outcome set for Dupuytren contracture.
Introduction
Dupuytren disease is a fibroproliferative disorder of the palmar and digital fascia, with an estimated prevalence of 7.3%. 1 The diseased fascia leads to a progressive contracture of one or more digits, causing impaired hand function. The possibility of regaining this function is the main motivation for patients to seek treatment. 2 Several minimally invasive and invasive treatment options are available for Dupuytren disease, including Clostridium histolyticum collagenase injections, fasciectomy, and fasciotomy. These treatments are targeted toward weakening, division, or excision of the diseased fascia to restore digital extension. 3
Currently, there is no recommended standard set of outcomes to report in Dupuytren disease treatment studies, nor are there guidelines on how the outcomes themselves should be measured or reported. In a recent systematic review, Karpinski et al 4 characterized outcome reporting practices in Dupuytren disease and found substantial variation in outcome measures. This heterogeneity precludes pooling of data across clinical populations, settings, and meta-analyses, making it difficult to elucidate the relative effectiveness of available treatments, and limiting the usefulness of existing research in informing clinical practice.
A core outcome set (COS) is a standard set of outcomes determined to be most important to the stakeholders of a particular health condition. 5 Development of a COS in Dupuytren disease would facilitate standardized outcome selection and reporting in Dupuytren disease research to promote uniformity amongst different studies, and to ensure the production of applicable research. A COS aids selection of relevant outcomes as important stakeholders (eg, patients and health care providers) have been included in the identification of outcomes for the COS, ensuring that the research will be meaningful to all important persons.
There are various methods for the development of a COS, including the Delphi technique, nominal group technique, consensus development conference, and semi-structured group discussion. 5 Including qualitative methods into COS development can allow for better inclusion of patient and other stakeholder’s opinions as well as preserve their distinct perspectives. 5 Qualitative research can be used in adjunct to the aforementioned COS methods to help enhance the COS recommendations.
Using qualitative, one-on-one interviews, this study aimed to elicit the most salient issues for patients living with and undergoing treatment for Dupuytren disease, as well as for the hand surgeons, occupational therapists (OTs), and physical therapists (PTs) caring for these patients, to inform the future development of a Dupuytren disease COS. We hypothesized that the differing experiences of patients and health care professionals in the context of Dupuytren disease would be reflected in discrepant outcomes of importance between the 3 groups.
Materials and Methods
Approach
This is a qualitative, interpretive description study employing one-on-one semi-structured interviews, as the researchers came to the project with a clinical framework and sought to apply the results to our existing framework to impact clinical practice. 6 The research paradigm for this study was a constructivist approach as the goal of such is to produce or reconstruct better knowledge which is developed as the investigation proceeds. 7
Study Setting and Recruitment
This study was conducted virtually out of an academic hospital in Canada (McMaster University). Patients were recruited from a community plastic surgery clinic associated with the institution. Surgeons were recruited from hand and plastic surgical units across Canada. OTs were recruited from the Canadian Association of Occupational Therapists (CAOT) research-listing page and PTs were recruited from hand and plastic surgery academic divisions across Canada. This project received research ethics board approval from Hamilton Integrated Research Ethics Board (Project #11450).
Patient Selection
A purposive sample was used to recruit a study sample of varying gender, age, Dupuytren disease characteristics (bilateral vs unilateral, primary vs recurrent), and treatment stage (pretreatment, posttreatment) in patients. 8 Adult (18 years or older) patients who were seeking or had received limited palmar and digital fasciectomy for Dupuytren disease within the past 1 year were approached. We limited our recruitment of postoperative patients to those who received treatment within the past year to ensure their experience of undergoing a Dupuytren disease procedure was still salient, and to minimize potential for inaccurate or limited recall of memories and experiences. Patients who were unable to communicate in English or to provide informed consent due to cognitive impairments were excluded.
Surgeon and OT/PT Selection
Convenience sampling was used for surgeons and OTs/PTs as a comprehensive representation of views with varying Dupuytren case load and duration of practice was achieved. 8
Sample Size
Based on previous protocols for conducting semi-structured interviews with plastic surgeons for the purpose of ultimately generating a COS, a total of 10 participants from each group were recruited. Sampling was continued beyond the minimum 10 participants for OTs/PTs until data saturation was achieved. Data saturation was reached when no new analytical information arose from consecutive interviews according to the view of Strauss and Corbin who saw saturation as a degree, not a discrete point. 9
Research Characteristics
Three investigators participated in data collection and analysis (MK, CH, and LG), including 2 medical students and 1 plastic surgery resident. They were trained by a researcher skilled in qualitative methodology (MNK). They were familiar with the clinical care and research surrounding Dupuytren disease appropriate to their educational level.
Data Collection
The one-on-one interviews followed a semi-structured format and were conducted by 1 of 3 researchers (MK, CH, and LG). Such a format is commonly used in qualitative research as it allows for open-ended questions that permit participants to discuss the issues most salient to them. 10 The interview questions were initially created following a preliminary interview with the senior author (AT) based on his experience interacting with patients, surgeons, and OTs/PTs in the clinical management of Dupuytren disease, as well as from key outcomes and themes identified from a systematic review of the literature by Karpinski et al. 4 Different scripts were used for surgeons, OTs/PTs, and patients, and are available in Supplementary 1. The interviews were conducted over the phone as opposed to a video call to enhance participant comfortability. 11 Audio-recordings were transcribed by the electronic Trint transcription software verbatim into written Microsoft Word documents. The documents were verified and double-checked against the recordings by an individual in the study team (MK, CH).
Data Analysis
Deductive content analysis was performed as the researchers had a previous framework of outcomes from the paper by Karpinski et al. 4 An unconstrained categorization matrix was developed, and interviews were coded accordingly by two investigators (MK and CH). 12 The identified themes are presented with narrative descriptions as well as with descriptive statistics.
Rigor
Due to the subjective nature of qualitative research, all steps of the data analysis process were performed independently and in duplicate by the 2 investigators (MK and CH) with disagreements resolved through consensus. This is otherwise termed as “investigator triangulation.” Member checking was performed to confirm results with the stakeholders themselves. A representative of each stakeholder group was reached via phone or email to discuss the results. This study was reported according to the Standard for Reporting Qualitative Research. 8
Results
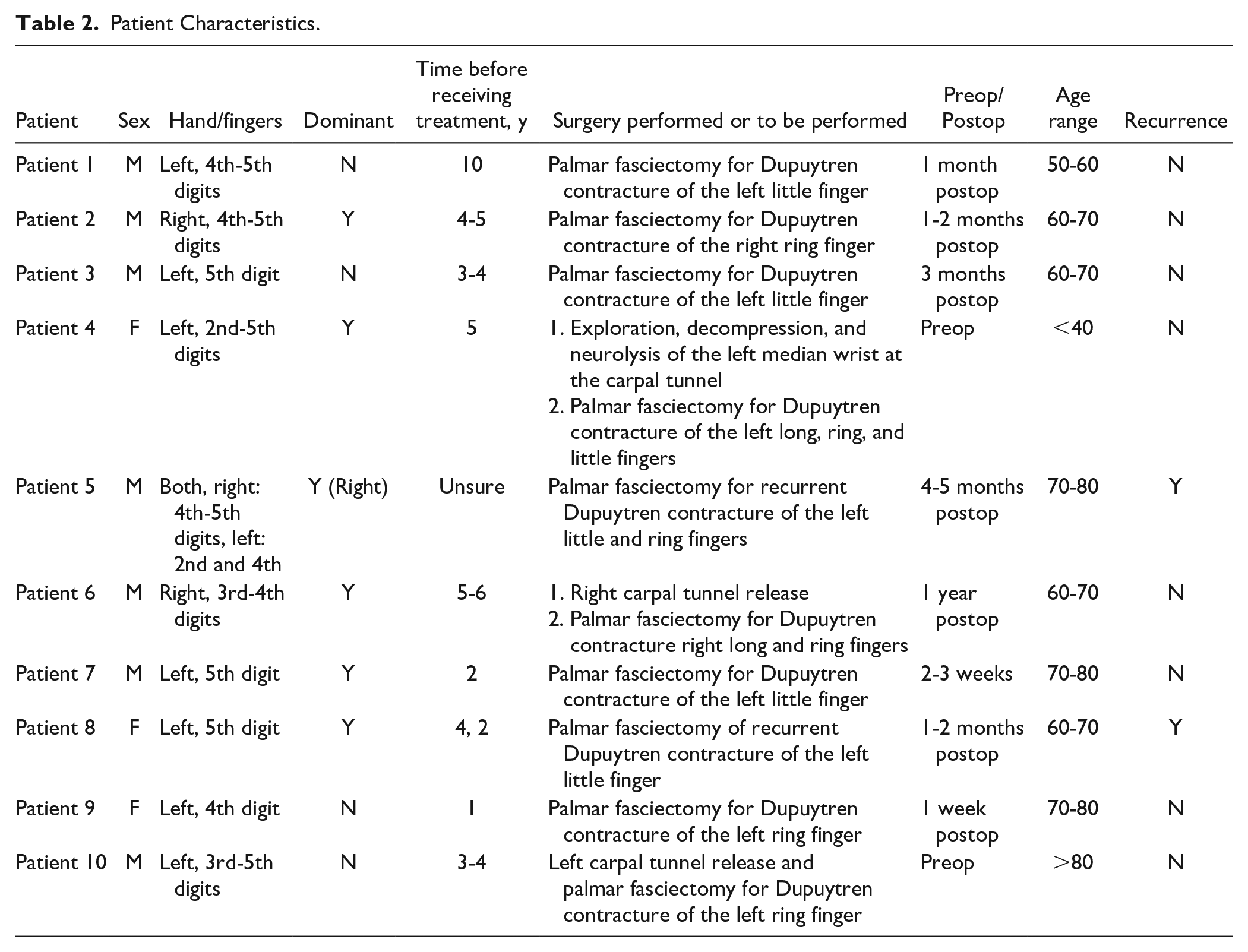
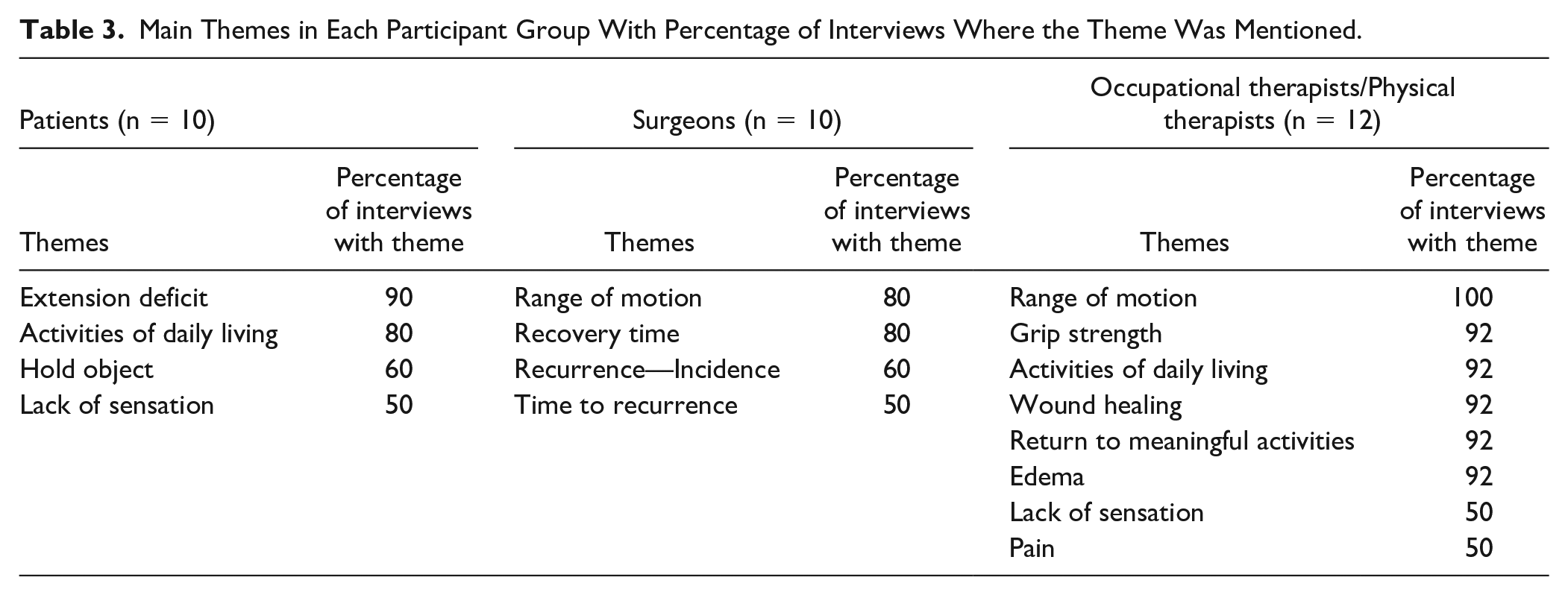
Interviews were conducted with stakeholders from September 2021 to January 2023. Ten surgeons, 12 OTs/PTs, and 10 patients were interviewed for this study. Stakeholder characteristics are included in Tables 1 and 2. Interviews lasted an average of 22 minutes (minimum: 8 minutes, maximum: 40 minutes). Dominant themes were identified in each participant group (Figure 1, Table 3, Supplementary 2).
Characteristics of Surgeons, Occupational Therapists, and Physical Therapists.
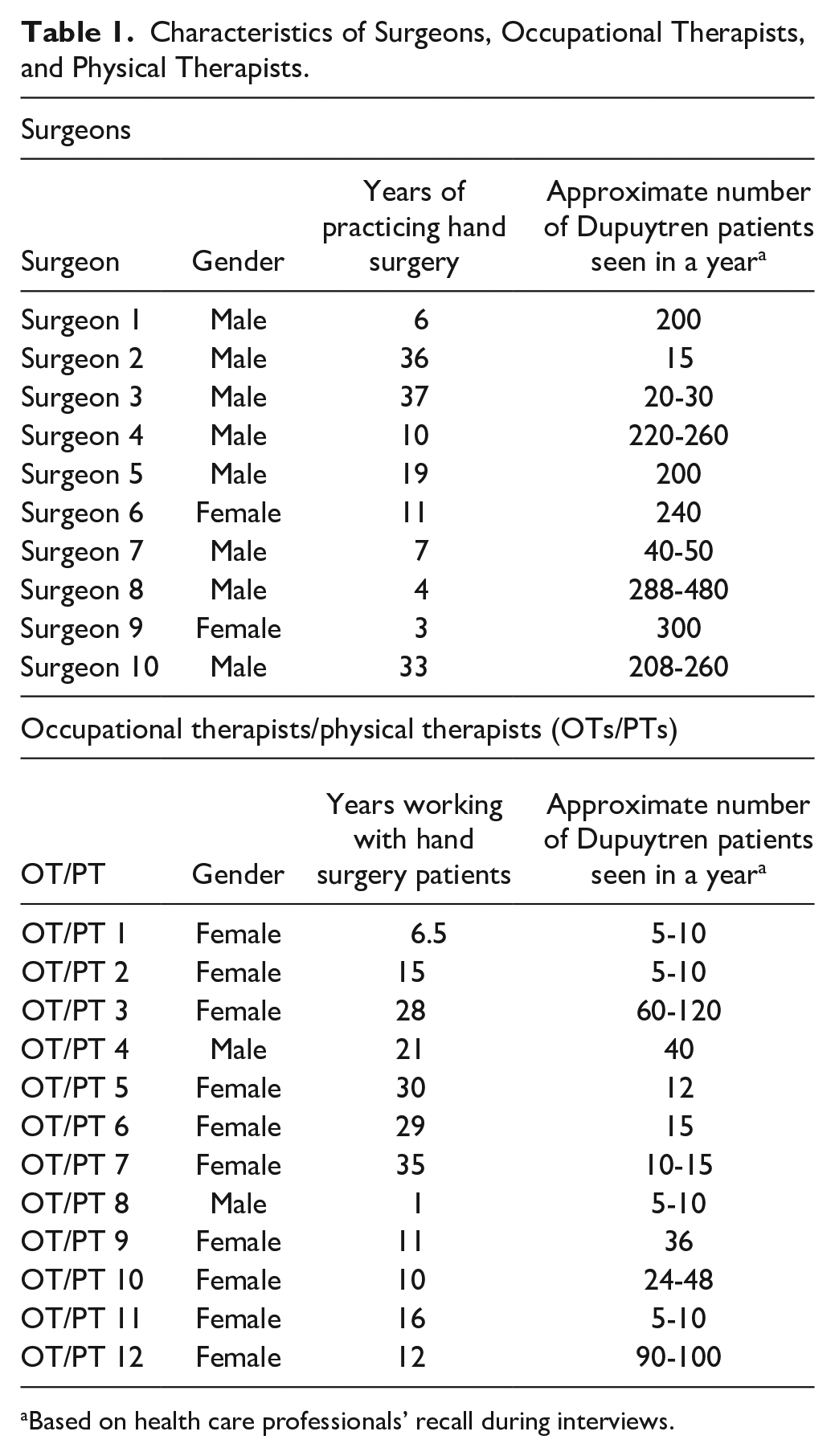
Based on health care professionals’ recall during interviews.
Patient Characteristics.
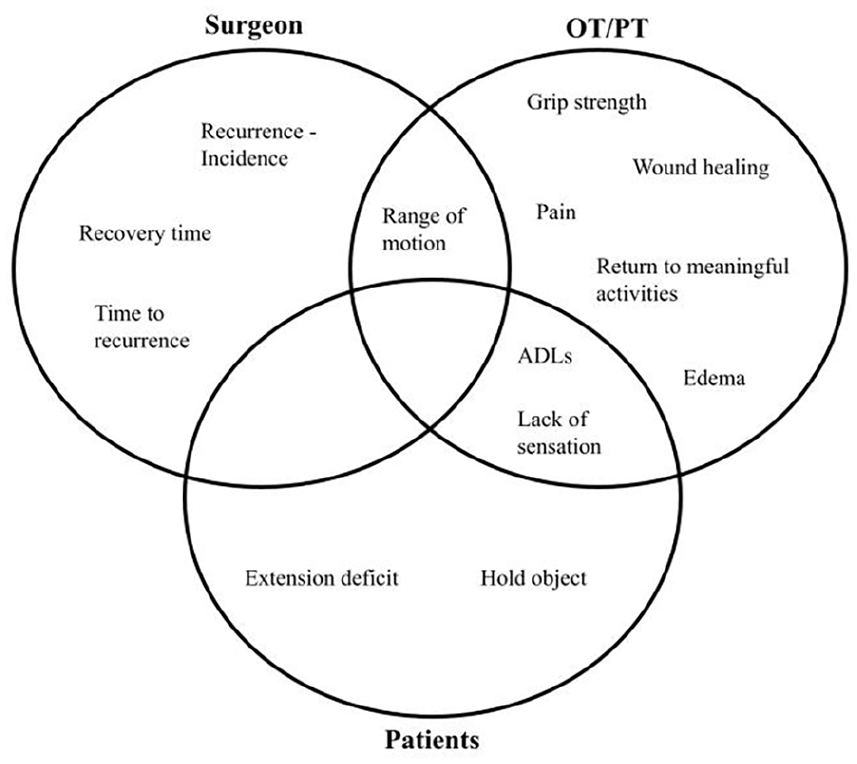
A Venn diagram of themes showing overlap or lack thereof between the 3 stakeholder groups (patients, surgeons, and OTs/PTs).
Main Themes in Each Participant Group With Percentage of Interviews Where the Theme Was Mentioned.
Patient Themes
Dominant themes identified from patient interviews were extension deficit, activities of daily living (ADLs), holding objects, and lack of sensation in descending order of frequency.
The main outcome of concern to patients was extension deficit. They described disliking the curling of their fingers, and wanted a treatment which could allow them to straighten their finger again.
The patients described how their Dupuytren disease affected their ADLs. These activities ranged from putting on gloves, to washing their face. Specifically, the inability to hold objects was frequently mentioned. When contacted for member checking, a participant mentioned the importance of expanding on the definition of ADLs to include impact on work or other noticeable deficits in a patient’s life. This was described to influence their decision on seeking treatment.
Finally, patients found intact sensation to be an important part of their treatment. Some patients mentioned being displeased with their fingertips being numb postoperatively, whereas preoperative patients mentioned wanting their sensation intact after the surgery.
Surgeon Themes
The dominant themes for surgeons included: range of motion (ROM) of hand, recovery time, and recurrence.
When describing outcomes for Dupuytren disease, surgeons highlighted ROM as a primary outcome. As opposed to fully straightening the fingers, surgeons noted how improving ROM can bring functionally meaningful changes to the patient.
Recovery time was also frequently mentioned. When comparing different treatment strategies, recovery time from the procedure influenced surgeons’ treatment recommendations. They recognized how a prolonged recovery could potentially lead to increased time off work, increased hospital visits, and increased cost for the patients.
Recurrence was mentioned in 2 forms: incidence and time to recurrence. Surgeons recognized that Dupuytren disease was not curable, and that it can recur after procedures. Surgeons recalled that they would discuss, with patients, the risk for recurrence and that the time to recurrence differed depending on the treatment received.
OT and PT Themes
The dominant themes among OTs/PTs were ROM, grip strength, ADLs, return to meaningful activities, wound healing, edema, lack of sensation, and pain.
All OTs and PTs mentioned ROM. Like surgeons, they recognized the importance of developing a functional ROM. Along with ROM, grip strength was often mentioned as a priority of rehabilitation for optimal hand function.
The OTs/PTs frequently described the impact of improving hand function including allowing patients to perform ADLs. In addition, the OTs/PTs referred to examples of certain goals or hobbies that patients found to be interrupted by their Dupuytren disease that were separate from daily function, which we termed return to meaningful activities in our present study. Both ADLs and return to meaningful activities were frequently mentioned in the OT/PT interviews.
Wound healing was also of importance among the OTs/PTs. They discussed ensuring the wound had proper healing and ideal scar formation throughout the therapy process.
Uniquely, OTs/PTs were the only subgroup to mention edema as an outcome. Nearly every therapist interviewed discussed how one of their goals of treatment was to control any edema or swelling in their patients.
Finally, lack of sensation and pain were mentioned by half of the OTs and PTs. Sensation was considered as another component of function alongside ROM and grip strength. Pain was described as a potential barrier in meeting therapy goals.
Discussion
The current study provides novel information to the current literature by identifying outcomes of high importance to patients and health care providers. While previous studies have sought to understand the experiences of patients living with Dupuytren disease,2,13 the present study is the first to additionally explore the experiences and priorities of the hand surgeons and therapists who care for these patients. In collecting this data, we sought the perspectives of a diverse group of Canadian patients and health care providers, with the understanding that their experiences and priorities can be shaped by their life circumstances, sociocultural factors, and the norms/practices in different health care settings, where relevant. This is important information and will be used in our future aim to develop a COS for Dupuytren disease. Next, we plan to apply the Delphi method in a subsequent study to validate our findings here and ultimately develop a COS.
The differing themes identified between stakeholders highlight the different focus and priorities of the three groups, as there was no single outcome with complete overlap. Surgeons and hand therapists frequently emphasized concepts related to posttreatment recovery, with hand therapists specifically concerned about wound healing and edema. The health care professionals cite the importance of considering posttreatment recovery in reducing the physical, social, and financial burdens on their patients; however, this was not a commonly expressed concern of the patients. Surgeons also frequently discussed disease recurrence and the importance of managing patient expectations regarding the potential for recurrence. Meanwhile, patients concentrated on regaining and maintaining function of their hands with the hope of performing ADLs and retaining sensation. This is in keeping with a recent qualitative study by Turreson et al, 13 where patients with Dupuytren disease expressed concern about their impaired fine motor skills, and concomitant functioning in leisure and self-care activities. The heterogeneity of opinions among stakeholders signals the importance of adequate representation from these groups for the development of a COS. Ultimately, the COS should reflect the priorities of patients receiving treatment for Dupuytren disease, while incorporating opinions of health care professionals who may have greater insight into treatment efficacy and safety.
Furthermore, there is a discrepancy in the concepts identified in the present study and the frequency with which these outcomes have previously been reported in the Dupuytren disease literature. For example, while the ability to perform ADLs was one of the most frequently mentioned outcomes by the patients and OTs/PTs in the present study, the systematic review by Karpinski et al 4 showed that ADLs were only assessed in 3.2% of Dupuytren disease studies. This suggests that existing Dupuytren disease literature may not measure the outcomes most meaningful to patients and health care providers.
Results from the current study should be interpreted considering the following limitations. First, all participants lived and practiced in Canada. While efforts were made to recruit a sample that was diverse in disease characteristics (for patients) and location of training and clinical practice (for health care professionals), there may be differences in priorities for patients and health care providers living/practicing in other countries with different health care systems and sociocultural norms. As such, generalization from this population to other countries may not be appropriate; future research should explore perspectives of patients and health care providers in other countries. Second, as the research team only spoke English, patients and health care providers who did not speak English were not able to be interviewed for this study. In addition, our sample does not include late postoperative patient experiences extending beyond one year posttreatment, which may limit our understanding of long-term patient perspectives and experiences after undergoing treatment. Furthermore, some patients in the study had concurrent additional hand conditions which may have influenced their symptoms. Specifically, 2 of the 5 patients who mentioned sensation also had carpal tunnel syndrome, which may have increased reporting of this issue. Finally, when collecting data on health care professionals’ Dupuytren disease patient volume, surgeons and OTs/PTs gave their best estimates on the number of patients they treat per year, but these numbers were not formally verified. Given the error inherent in human recall, the reported numbers may not be an accurate characterization of clinical practice patterns in our sample, and may also account for some of the discrepancy in patient volume seen between providers.
Similar to the heterogeneity within the literature, there are differing priorities between patients, surgeons, and OTs/PTs regarding outcomes for Dupuytren disease. While all mentioned hand function, they had different ways of describing it with patients focusing on improving their current abilities, and health care providers concentrating on postoperative recovery. In addition, outcomes identified in this study were not represented in current research. The development of COS will greatly enhance research in this field by providing a standardized set of outcomes that are important to all stakeholder groups.
Supplemental Material
sj-docx-1-han-10.1177_15589447241306143 – Supplemental material for Understanding Stakeholder Priorities in Dupuytren Disease: A Qualitative Study
Supplemental material, sj-docx-1-han-10.1177_15589447241306143 for Understanding Stakeholder Priorities in Dupuytren Disease: A Qualitative Study by Marta Karpinski, Caroline Hircock, Lucas Gallo, Emily Dunn, Jessica Murphy, Manraj N. Kaur and Achilles Thoma in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447241306143 – Supplemental material for Understanding Stakeholder Priorities in Dupuytren Disease: A Qualitative Study
Supplemental material, sj-docx-2-han-10.1177_15589447241306143 for Understanding Stakeholder Priorities in Dupuytren Disease: A Qualitative Study by Marta Karpinski, Caroline Hircock, Lucas Gallo, Emily Dunn, Jessica Murphy, Manraj N. Kaur and Achilles Thoma in HAND
Footnotes
Acknowledgements
The authors thank the hand surgeons, hand OTs, hand PTs, and patients who participated in this study.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all individual participants in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.