
Abstract
Background:
Chronic pain remains a significant challenge for individuals following limb amputation, with incidence of painful neuromas, phantom limb pain (PLP), and residual limb pain (RLP). Targeted muscle reinnervation (TMR) is a surgical technique designed to restore motor control information lost during amputation by redirecting residual nerves to new muscle targets. This systematic review and meta-analysis aims to compare patient-reported and functional outcomes following amputation with either TMR or standard neurological treatment (SNT). The study also includes an examination of primary versus secondary TMR and explores outcomes in highly comorbid patient populations.
Methods:
A search of central databases was performed, and meta-analysis was completed on extracted data where possible.
Results:
Eleven studies were identified. Results indicate a significant reduction in PLP and RLP in patients undergoing TMR compared to SNT using various pain scores. TMR also demonstrates improved functional outcomes and decreased opioid use. Furthermore, results indicated patients who underwent TMR at the time of amputation (primary TMR) had improved pain scores compared with those who had TMR performed later (secondary TMR).
Conclusions:
The review emphasizes the benefits of TMR as a valuable surgical adjunct for amputee patients, while also highlighting the need for further research, especially in comorbid populations.
Introduction
Chronic pain is a challenge following limb amputation, with painful neuromas, phantom limb pain (PLP) and residual limb pain (RLP) reported to afflict up to 85% of amputees.1 –3 The presence of these pathologies contributes to reduction in prostheses usage, impairment of functional outcomes, and decreased quality of life for many amputees. 4
Targeted muscle reinnervation (TMR) aims to recapture motor control information in the central and peripheral nervous system that has been lost due to a lack of motor effectors following an amputation and involves transfer of residual nerves to new muscle targets. Originally conceived to allow more intuitive control of upper limb prostheses with multiple degrees of freedom following the modification of residual limb anatomy, TMR has also been found to reduce the likelihood of symptomatic neuroma formation, and the development of PLP and RLP.5,6 Targeted muscle reinnervation (TMR) can be performed at the time of surgical amputation (primary TMR), or later if needed (secondary TMR). The rationale underpinning the analgesic effects of TMR is the provision of a physiologically appropriate environment for regenerating axons, which results in organized nerve regeneration into the denervated target muscles, without the chaotic and misguided growth that causes symptomatic neuroma formation.7,8
Previous studies have compared TMR to standard neurological treatment (SNT) during amputation (in which a traction neurectomy is performed, or the nerves are buried into innervated muscle or bone) and found improvements in pain and analgesic requirements.7,9,10 However, no consensus has been established on whether TMR should be adopted as standard practice during limb amputation. Furthermore, there has been little focus on the outcomes of TMR in highly comorbid patients (such as those with cancer or end-stage diabetes), despite this cohort being overrepresented in those receiving amputations.11,12
Thus, this study aims to assess optimal treatment of nerves during amputation by systematically reviewing the literature and comparing patient reported and functional outcomes following amputation with either TMR or SNT. It provides a comparison of outcomes following primary and secondary TMR, as well as a summary on outcomes following TMR in highly comorbid patients.
Materials and Methods
This systematic review was registered a priori on PROSPERO (CRD42023411514) and was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta Analyses Statement (PRISMA) guidelines. 13
A systematic electronic search of the MEDLINE, PubMed, EMBASE, and Cochrane Library databases was performed in March 2023, with no limit on publication date. The keywords utilized were “targeted muscle reinnervation,” with all variants on this phrase included (see Supplemental Appendix). All English language studies published in peer-reviewed journals and comparing the outcomes of TMR against SNT (defined as any nonreinnervation strategies in the setting of amputation), or the outcomes of primary TMR against secondary TMR, were eligible for inclusion. Patients who underwent alternate reinnervation strategies, such as regenerative peripheral nerve interfaces (RPNI), were excluded from the comparison. Conference abstracts that included relevant data were included, while case reports, opinion articles, and technical notes without results were excluded.
The population assessed were adult patients who underwent amputation of either an upper or lower limb for any reason, with those with major comorbidities identified for subanalysis. Patients were stratified by the intervention of TMR (via any technique and approach) or SNT for comparison. Outcomes assessed included demographic data, patient-reported outcome measures (such as RLP and PLP Patient Reported Outcomes Measurement Information System [PROMIS], numerical rating scale [NRS] and visual analog scale [VAS] scores), and the development of neuromas, at any time point postintervention. The PROMIS, NRS, and VAS scoring systems are validated for clinical pain assessment and are utilized in diverse patient populations.14,15 In addition to pain scores, the degree of narcotic usage and proportion of pain free patients was extracted where possible.
The search was undertaken by 2 authors (AJZ and VVGA) who independently assessed the retrieved studies. Title and abstract screening was performed to identify appropriate texts for full-text assessment. Data were then independently collected. Any discrepancies were discussed between the 2 authors, and escalated to the senior author, until consensus was met. The reference lists of all papers included were manually vetted to identify any potential articles for inclusion.
Data analysis was performed using the Review Manager 5.3 program (Cochrane Collaboration). 16 Where possible, data from the included studies were meta-analyzed via a random-effects model. Weighted mean differences with 95% confidence intervals were used as a summary statistic for continuous outcomes. Random effects meta-analysis was also conducted for any dichotomous data. Alpha was 0.05 and all calculated P-values were 2-sided. 17
Results
Study Selection
The initial electronic search identified 721 studies. After removal of duplicates, the titles, and abstracts of 267 studies were screened, resulting in 22 studies for full-text assessment. A further 11 studies were excluded based on eligibility criteria. Eleven studies were included for systematic review and meta-analysis (Figure 1).
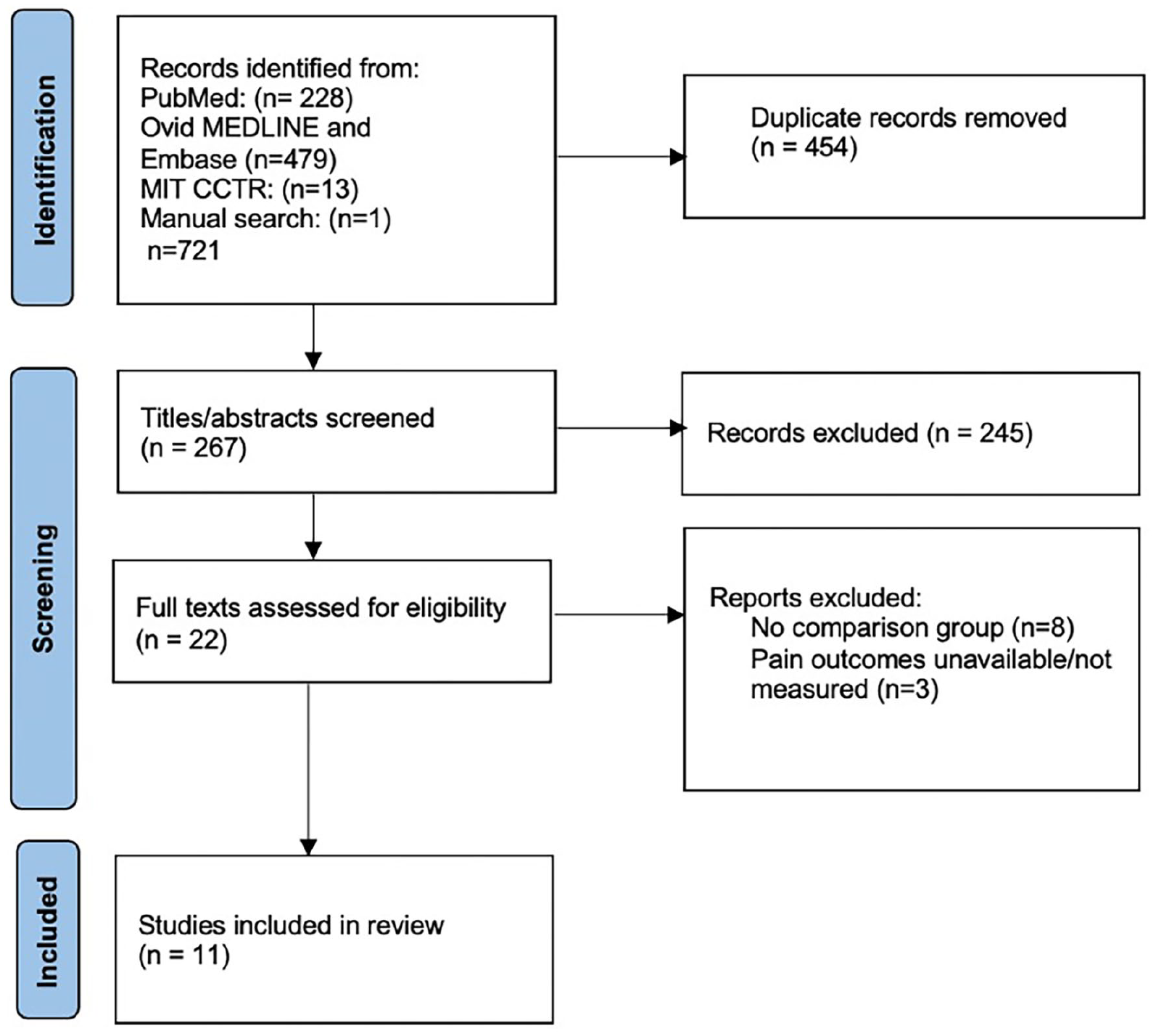
PRISMA flow diagram of search strategy.
Risk of Bias
Assessment of risk of bias was performed on suitable nonrandomized studies by utilization of the ROBINS-I tool. 18 All studies included were deemed as having low to moderate risk of bias overall. A risk-of-bias plot was created using Robvis (Figure 2). 19 Domains found to have higher risk of bias in the included studies related mostly to the inclusion and control of confounding factors, as well as moderate subjectivity in the measurement of patient outcomes, such as pain and ambulation.
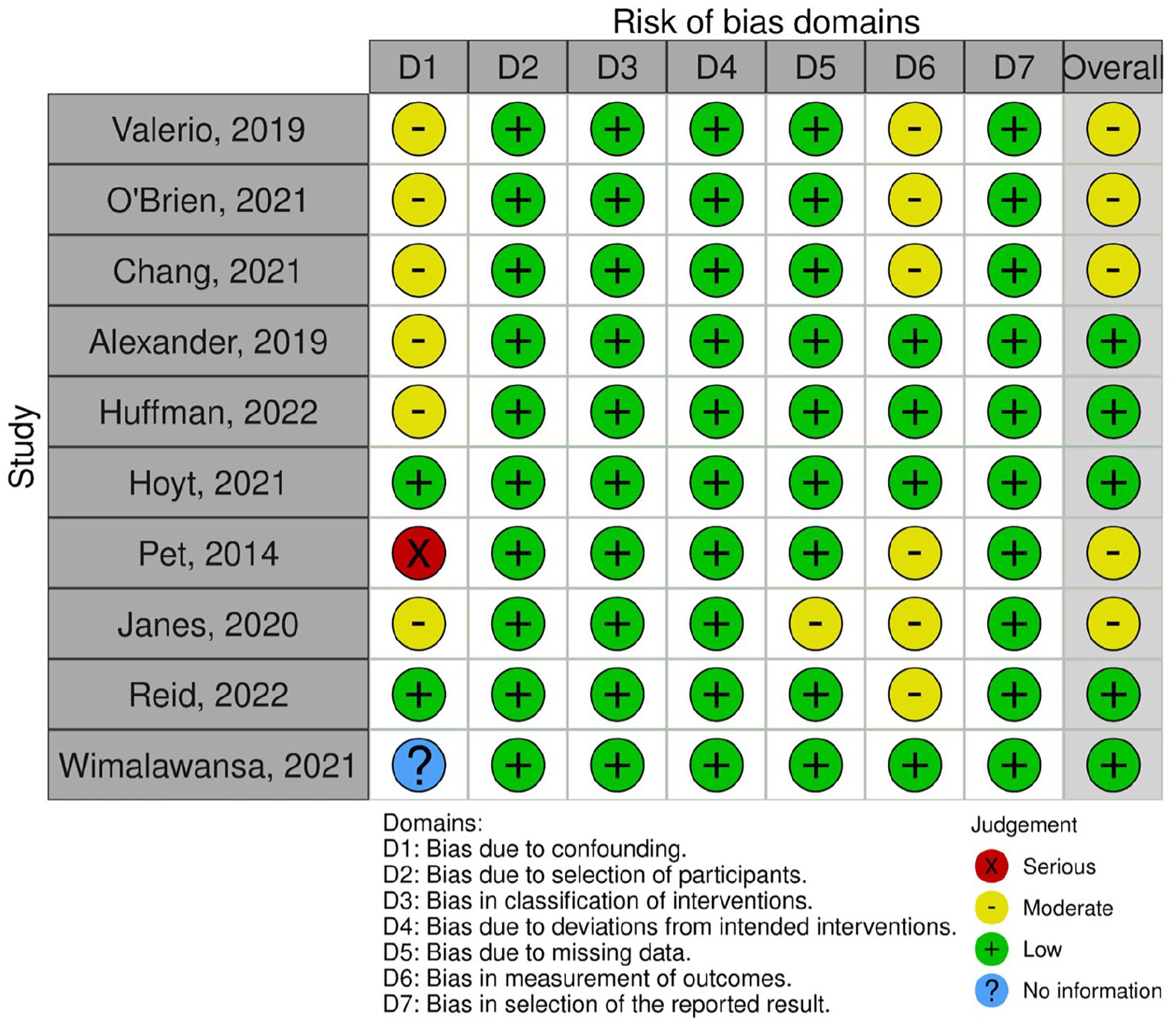
Risk of bias assessment on eligible nonrandomized studies using the ROBINS-I tool.
Characteristics of Included Studies
Of the 11 included studies, 10 were cohort studies and 1 was a randomized controlled trial (Table 1), with a total cohort of 1117 patients. TMR was compared to SNT in 6 studies, with 216 patients receiving TMR and 708 undergoing SNT. Primary TMR was compared to secondary TMR in the remaining 5 studies, with 87 patients receiving primary TMR, and 119 receiving secondary TMR.
Summary Table of Included Studies and Designs.
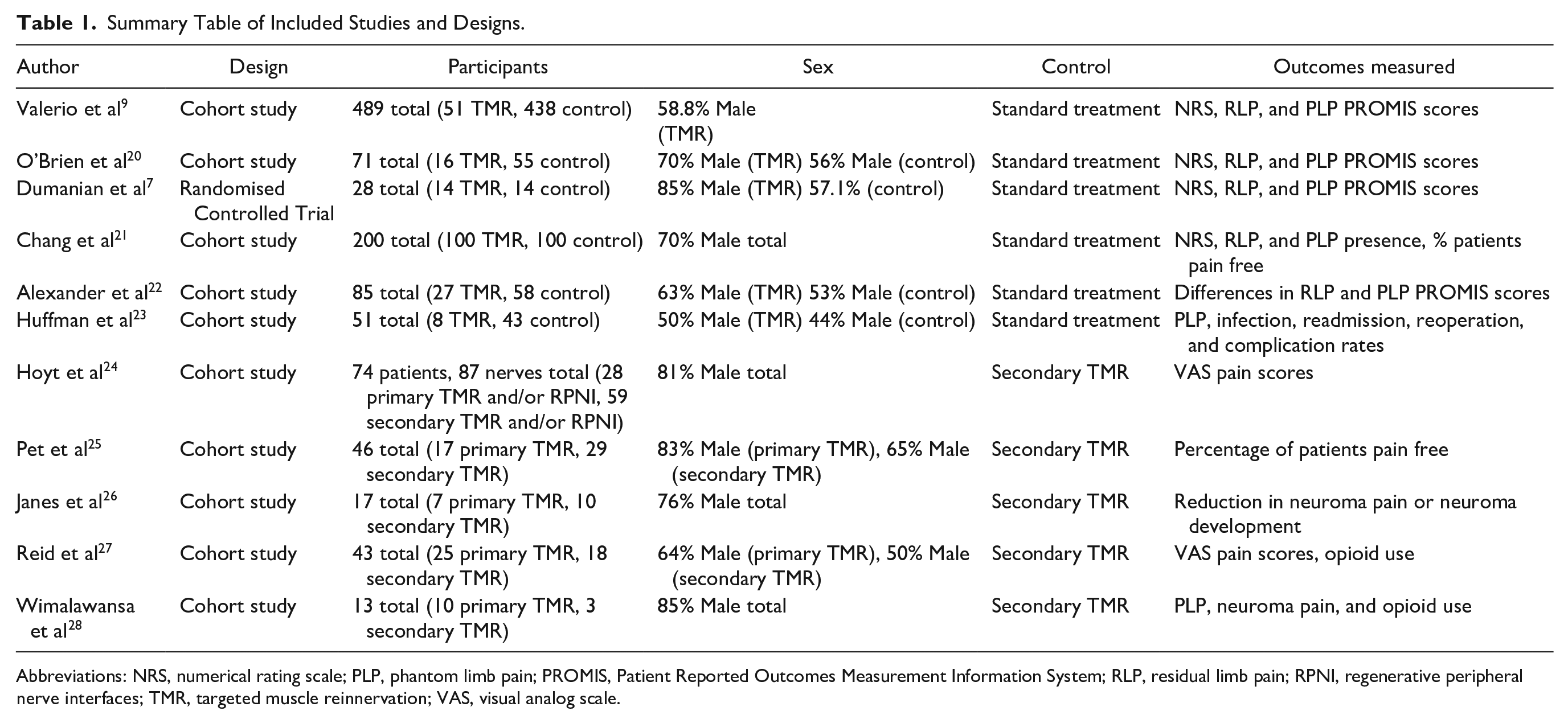
Abbreviations: NRS, numerical rating scale; PLP, phantom limb pain; PROMIS, Patient Reported Outcomes Measurement Information System; RLP, residual limb pain; RPNI, regenerative peripheral nerve interfaces; TMR, targeted muscle reinnervation; VAS, visual analog scale.
Phantom Limb Pain
Phantom limb pain (PLP) was a primary outcome measure in 7 studies.7,9,20 –22,28 Differences in PLP between treatment groups were measured in a variety of ways, including NRS, PROMIS questionnaires and VAS scores. Two studies were suitable for random effects meta-analysis on both PROMIS scores and NRS scores.
Random effects meta-analysis on PLP scores from PROMIS Pain Intensity Short-Form 3a found a mean difference between the TMR and SNT groups of −12.03 (95% CI −13.97 to −10.08). On scores from PROMIS Pain Behaviour Short-Form 7a, random effects meta-analysis found a mean difference between the TMR and SNT groups of −9.37 (95% CI −12.25 to −6.49). Random effects on scores determined from PROMIS Pain Interference Short Form 8a found a mean difference between the TMR and SNT groups of −6.42 (95% CI −12.27 to −0.57).
These results indicate a statistically significant decrease in patient-reported PLP intensity, behavior, and interference in patients treated with TMR compared to those who received SNT. No significant heterogeneity for PLP PROMIS scores was detected (Figure 3).
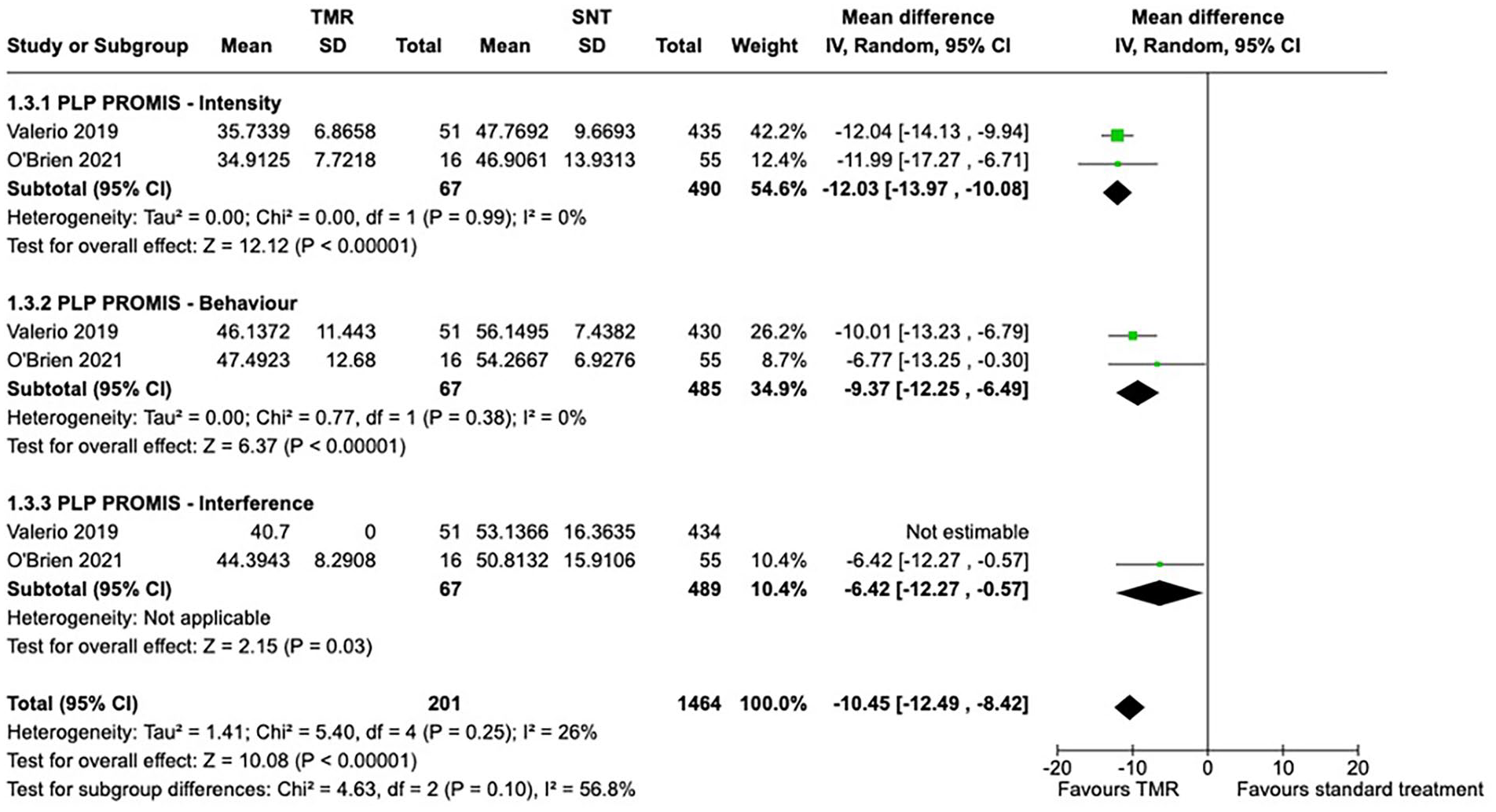
Random effects meta-analysis of PROMIS scores related to intensity, behavior, and interference of PLP.
Random effects meta-analysis on patient NRS scores of worst PLP pain found a mean difference between the TMR and SNT groups of −2.52 (95% CI −3.48 to −1.55). Numerical rating scale (NRS) scores of patients’ level of best PLP was unable to be analyzed quantitatively. Random effects meta-analysis on scores from NRS scores of patient PLP at the time of survey found a mean difference between the TMR and SNT groups of −1.54 (95% CI −2.18 to −0.91).
These results indicate a statistically significant decrease in patient-reported PLP scores on NRS when asked to determine their current and worst level pain in patients treated with TMR compared to those who received SNT. No significant heterogeneity for PLP NRS scores was detected (Supplemental Figure 1).
Although an improvement was noted in chance of worst PLP being rated on NRS as “severe” in the TMR group when compared to those receiving SNT, this difference was not significant (odds ratio 0.24, 95% CI 0.05 to 1.17; P = .20) (Supplemental Figure 2).
Residual Limb Pain
Residual limb pain was reported in 5 studies, with 2 studies suitable for random effects meta-analysis of PROMIS and NRS scores.7,9,20 –22
Random effects meta-analysis on RLP scores from PROMIS Pain Intensity Short-Form 3a found a mean difference between TMR and SNT groups of −11.63 (95% CI −17.82 to −5.43); a mean difference of −11.57 (95% CI −20.46 to −2.68) when considering scores from PROMIS Pain Behaviour Short-Form 7a; and a mean difference of −4.78 (95% CI −10.93 to 1.37) when assessing PROMIS Pain Interference Short Form 8a scores.
These results indicate a statistically significant decrease in patient-reported RLP intensity, behavior, and interference in patients treated with TMR compared to those who received SNT. No significant heterogeneity for PLP PROMIS scores was detected (Figure 4).
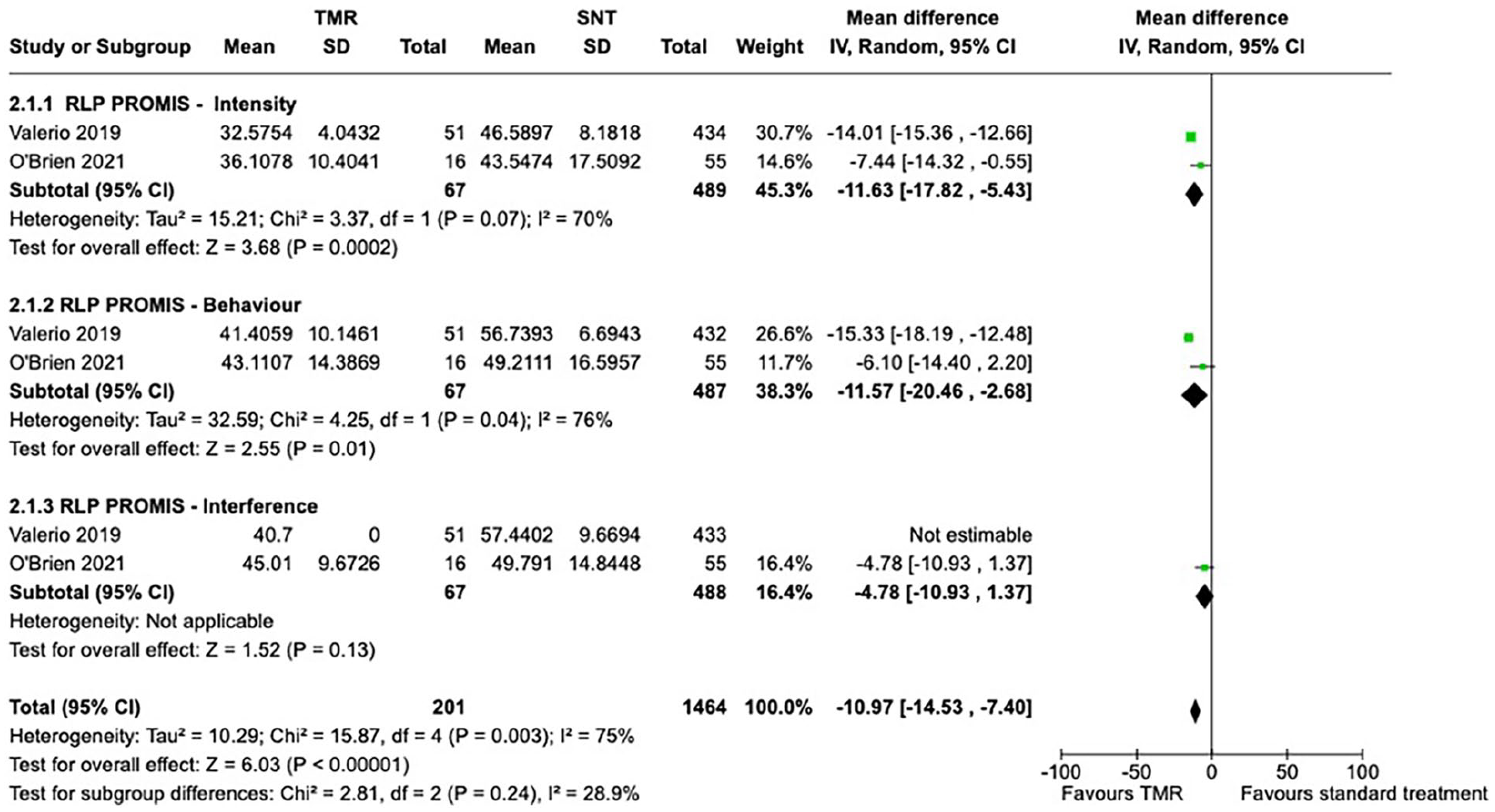
Random effects meta-analysis of PROMIS scores related to intensity, behavior, and interference of RLP.
Random effects meta-analysis on NRS scores of worst RLP found a mean difference between TMR and SNT groups of −2.61 (95% CI −3.32 to −1.91), while NRS scores of best RLP were unable to be analyzed quantitatively. Random effects meta-analysis on NRS scores of patient RLP at time of survey found a mean difference between TMR and SNT groups of −1.07 (95% Cl −2.14, −0.01).
These results indicate a statistically significant decrease in patient-reported NRS scores concerning level of worst and current RLP in patients treated with TMR, compared to those who received NST. No significant heterogeneity for was detected for these domains (Supplemental Figure 3).
Patients receiving TMR had an odds ratio of 0.33 (95% CI 0.16 to 0.68, P = .003) when compared to those receiving SNT for the development of RLP described as “severe” on NRS (Supplemental Figure 4).
Random effects meta-analysis of postoperative VAS pain scores found a mean difference of −1.70 in favor of primary TMR when compared to secondary TMR (95% CI −3.13 to −0.28, P = .01) (Figure 5).
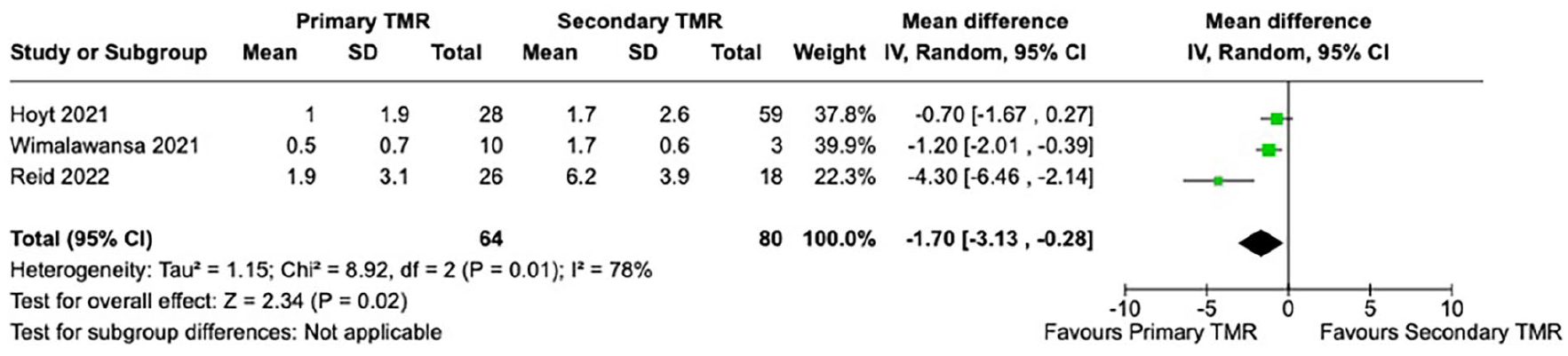
Random effects meta-analysis of VAS pain score outcomes between primary and secondary TMR groups.
Patients receiving primary TMR had an odds ratio of 2.09 (95% CI 0.30 to 14.32, p = .75) of being “pain-free” post-treatment, when compared to those undergoing secondary TMR (Figure 6).
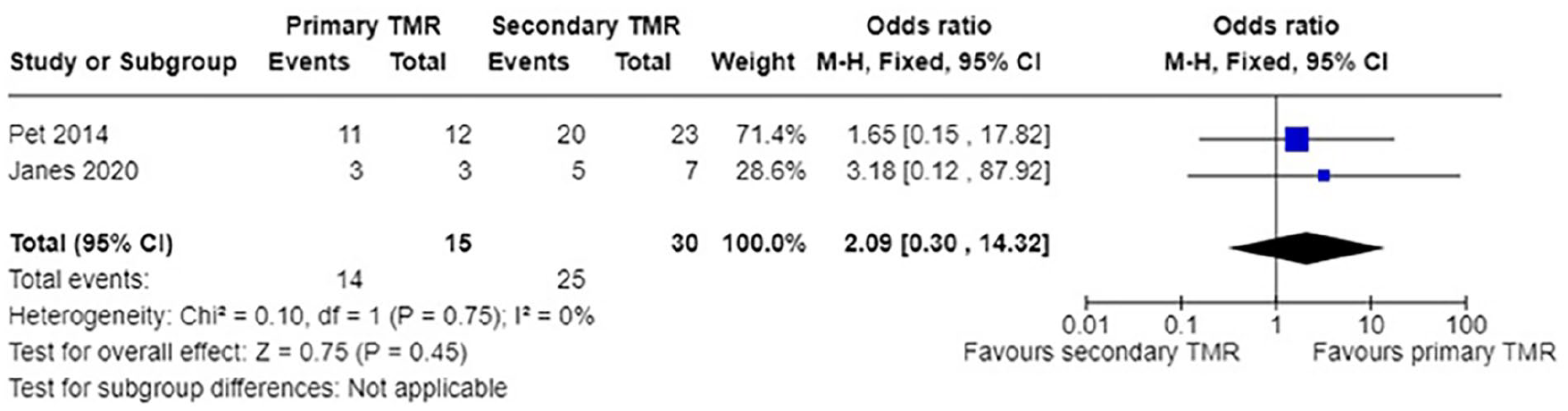
Meta-analysis of number of patients reported as “pain-free” postsecondary TMR versus postprimary TMR. TMR, targeted muscle reinnervation.
Symptomatic Neuroma Formation
Neuroma formation and pain was investigated in 2 studies. Alexander et al found reductions in both frequency and intensity of neuroma symptoms in TMR patients compared to standard treatment. 22 Pet et al reported that the majority of patients receiving both primary TMR and secondary TMR (92% and 87%, respectively) were free of palpation-induced neuroma pain at final follow up. 25
Quality of Life Measures
Functional outcomes were reported in 2 studies—Dumanian et al reported on NEURO-QOL scores in a cohort of lower extremity amputees, finding greater scores (reflecting improved quality of life) at final follow up in those receiving TMR. 7 Chang et al assessed ambulation status as a measure of functional improvement postsurgery and found a significantly higher rate of ambulation in the TMR group compared to controls receiving SNT (90.9% and 70.5% respectively, P < .01). 21
Opioid use
Opioid use was assessed in 4 studies. Alexander et al found a 34% reduction in opioid use in TMR patients at 1 year postoperatively; however, data on opioid use in patients receiving SNT was not available. 22 O’Brien et al successfully weaned over 80% of TMR patients off opioids at final follow up, although the level of opioid use in controls receiving SNT was again not reported. 20 When comparing opioid use between primary and secondary TMR, Hoyt et al found a significant decrease in opioid consumption in primary TMR compared to secondary TMR, whereas Reid et al found no statistically significant differences between groups (though consumption of opioids at final follow up had decreased to 21% and 12% in patients receiving primary and secondary TMR, respectively).24,27
TMR in the Highly Comorbid Population
A single paper aimed to explore the role of TMR in highly comorbid patients compared to SNT, precluding a formal meta-analysis. In the study, Chang et al found significantly higher rates of TMR patients who were ambulatory and pain free, as well as reduced rates of PLP and RLP compared to those receiving SNT. 21 Multiple other studies included patients with a variety of comorbidities (particularly those with oncological conditions), and the details are summarized in Supplemental Table 1.
Discussion
Targeted muscle reinnervation (TMR) is believed to capitalize on the regenerative properties of severed nerves, facilitating their coaptation and integration with motor nerves to allow propagation of signals to defined and denervated muscular targets. This results in a closed afferent-efferent pathway, which does not occur with traction neurectomy or burying of severed nerves in surrounding but innervated tissue.7,10,25
This systematic review and meta-analysis assessed the existing literature to compare pain outcomes following TMR or SNT following an amputation. Meta-analysis of available data demonstrated a reduction in PLP and RLP in patients undergoing TMR compared to those undergoing SNT, although it should be noted that only a limited number of studies were able to be formally meta-analyzed.
More specifically, the reduction in pain was noted in PROMIS scores relating to intensity, behavior, and interference, as well as NRS domains identifying worst and current levels of pain. Improvements were seen in worst pain scores labeled “severe” when patients underwent TMR, as compared to SNT. Patients undergoing TMR were also found to demonstrate improved functional outcomes and reduced opioid utilization.
The current study demonstrates that primary TMR results in significantly reduced postoperative VAS pain scores when compared to secondary TMR. However, due to limited available studies and significant heterogeneity, no definitive conclusion could be drawn. Hoyt et al did not find a significant difference in PLP and RLP related to timing of TMR but did note several improvements when transfers were performed early, including reduced rates of opioid consumption. 24 Both Reid and Pet, however, reported that primary TMR resulted in improved pain at intermediate and long term follow up when compared to patients receiving secondary TMR.25,27 Meta-analysis of VAS pain scores reported by Hoyt et al, Reid et al, and Wimalawansa et al favored primary TMR over secondary TMR (Figure 5).24,27,28 A higher proportion of patients reported being pain free post primary TMR when compared to secondary TMR, although this result was not statistically significant (Figure 6). A recent retrospective analysis of prospectively collected data in 94 amputees reported a more rapid reduction of pain to a “mild” level in patients undergoing primary TMR as compared to secondary TMR, with significant differences in pain level noted between the 2 cohorts in the 6 to 30 month postoperative period. 29 Thus, it seems that TMR at the time of primary amputation is worthwhile, although further long-term corroborative evidence would be informative.
The reductions in pain scores noted in this study are comparable to the minimum clinically important difference (MCID) reported for these measures previously in the literature in cohorts of patients with chronic and postoperative pain. The MCID for the PROMIS scale has been determined to range from 3.5 to 5.5—the various domains of PLP reduced by between 6.42 to 12.03 points in this study, while those for RLP dropped by 4.78 to 11.63 points. 30 Similarly, the alterations in NRS scores for worst and current PLP and RLP were greater than the MCID of 1 point, while the difference in VAS between primary and secondary TMR was comparable to the MCID for that metric (1.7).31 –34 Thus, the use of TMR (particularly at the time of amputation) results in clinically relevant improvements to patient outcomes, although it must be noted that the MCIDs were determined from populations dissimilar to those in this study.
The utilization of TMR in highly comorbid patients remains poorly assessed, with only one study in this review investigating its role in this population. 21 This is of particular importance, given that this population is overrepresented in those receiving an amputation—indeed, a series of over 40 000 below knee amputees found that almost half suffered from PVD. 35 Many of these patients may be at higher risk of morbidity following TMR, due to increased operative time, additional dissection in areas of compromised vascularity, and poor underlying physiology. 35
Oncologic patients may be at increased risk of postoperative pain due to long-standing analgesic use from tumor burden or prior interventions and may lack suitable nerve targets following adequate resection. 36 Future research carefully mapping outcomes in these cohorts would be beneficial in the development of an evidence-based treatment algorithm. One notable single arm study of oncologic amputees undergoing TMR or RPNI by Roubaud et al (not included in the formal review due to lack of preoperative data and a formal control group) found postoperative final follow-up NRS pain scores to be close to that of national averages, with reductions in opioid consumption. Furthermore, univariate regression analysis found BMI to be a significant influence on PLP scores. 37 Similarly, Anderson et al found oncologic amputee patients reported no neuroma pain post-TMR surgery, and the presence of pain ranging from absent to mild. 38 Findings of these 2 single-arm studies are outlined in Supplemental Table 2. These studies should be the vanguard in continued investigation of the benefit of TMR in highly comorbid patients.
This review is not without its limitations. Only a few studies were suitable for meta-analysis, with just 2 available for assessment of PROMIS and NRS scores, limiting the interpretation of cause and effect. The limited reporting of demographic data (including medical comorbidities) and heterogenous scoring methods utilized for pain across studies also precluded in-depth analysis in populations of interest. As TMR as a therapeutic modality is still in its infancy, medium to long-term data is limited. Most of the included studies are retrospective cohort in nature, and larger prospective randomized studies with standardized outcomes measuring would be beneficial.
Conclusion
This meta-analysis finds that TMR is a valuable surgical adjunct for reducing PLP and RLP in amputee patients. Targeted muscle reinnervation (TMR) also shows measurable benefit in improving functional outcomes and reducing opioid use. Additional research, particularly in comorbid patient populations, is needed to provide evidence-based guidelines for the use of TMR in amputation surgery.
Supplemental Material
sj-docx-1-han-10.1177_15589447241284811 – Supplemental material for Targeted Muscle Reinnervation Compared to Standard Peripheral Nerve Management Following Amputation: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-han-10.1177_15589447241284811 for Targeted Muscle Reinnervation Compared to Standard Peripheral Nerve Management Following Amputation: A Systematic Review and Meta-Analysis by Alexis J. Zimbulis, Vincent V.G. An, Michael Symes, Liron S. Duraku, R. Glenn Gaston, Kyle R. Eberlin and Brahman Sivakumar in HAND
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All studies included in this systematic review and meta-analysis were performed in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5), to the best of the authors’ knowledge. This article does not include any studies with animal subjects.
Statement of Informed Consent
The study was a systematic review and meta-analysis of pre-existing available studies pertaining to TMR as per the search strategy outlined. As such, no informed consent was required or obtained from patients for this article, and no identifying information of individual participants is included.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.