
Abstract
Background:
Claw deformity is a devastating consequence of low ulnar nerve palsy, resulting in loss of finger function. Traditionally, the Brand transfer is a favored intervention but requires lengthy grafts and bulky tenorrhaphies, risking adhesions in the lumbrical canal. We present a modified Brand tendon transfer, which extends the extensor carpi radialis brevis (ECRB) into 4 tails for individual grafting into the lateral band, decreasing adhesion risk and graft length need.
Methods:
Nine consecutive patients with claw hand were examined in detail to confirm the diagnosis and appropriateness for claw-correction surgery by the senior author. All patients underwent our modified Brand transfer. Follow-up for a minimum of 6 months was pursued for each patient, with range of motion, grip strength, and pinch strength recorded at that time.
Results:
Treated patients demonstrate maintained grip and pinch strength, coordinated grasp, and improvement in metacarpophalangeal posture. One patient required reoperation for extensive scarring and underwent tenolysis of the tendon grafts and revision grafting for the small finger.
Conclusion:
We concluded that our modified weave of a 4-tailed tendon graft through the ECRB is a synergistic transfer that maintains acceptable hand strength in the setting of a chronic low ulnar nerve palsy with a lower risk of tendon adhesion and length of grafting, offering an additional tool in the armamentarium of the hand surgeon approaching the ulnar nerve–injured hand.
Introduction
Low ulnar nerve injuries, defined as injuries to the nerve distal to the innervation of the extrinsic finger flexors, are uncommon but challenging problems for hand surgeons. Often, they present with the hallmark of a claw deformity, which causes complex functional issues that require surgical intervention.1,2
Clawing results from the paralysis of interossei and the ulnar-innervated lumbricals, in the presence of functioning extrinsic flexors.1,2 This causes a loss of interphalangeal (IP) joint extension and metacarpophalangeal (MCP) joint flexion.1,2 Furthermore, as the intrinsic muscles are important for rotational and precise finger positioning, low ulnar nerve palsy results in substantial impairment of fine motor function.1,2 In addition, given the loss of adductor pollicis and first dorsal interosseous muscle function, key pinch is lost.
Established techniques to address the ulnar claw posture and resultant functional impairments include a plethora of static and dynamic procedures. Static options help improve the resting position of the hand and include osseous blocks, volar capsulorrhaphies, and tenodesis procedures.3 -5
However, dynamic correction of clawing restores active flexion at the MCP joint and improves coordinated grasp. Several tendon transfers for active correction of clawing have been described. The Zancolli “lasso” transfer utilizes the flexor digitorum superficialis (FDS) to correct MCP hyperextension by folding a slip proximally as a volar bulwark against MCP hyperextension. 6 In the Burkhalter and Strait 7 transfer, the FDS to the middle finger is divided into 4 and weaved with the lumbrical tendon, again to bolster MCP flexion from the volar aspect. The Brand 8 transfer, which utilizes the extensor carpi radialis longus or brevis (ECRL/ECRB) with an interposed tendon graft as a donor to the lateral band of each finger to correct MCP hyperextension, provides support from a dorsal approach, opposing MCP hyperextension by augmenting intrinsic function. Although each of these transfers has inherent benefits and indications, each is limited in the resulting function.
Limitations of the Brand transfer include formation of adhesions, decreased strength, and challenges with tensioning.9 -12 The senior author (A.M.M.) developed an anticlaw tendon transfer of ECRB to lateral bands of the index, middle, ring, and small fingers with a 4-tailed palmaris longus (PL) tendon graft, which is fixed at the midpoint of the graft and fixed distally on the lateral bands with smaller-caliber suture, as a variation to the prior Brand tendon transfer, which uses a broadened tendon graft as compared to the PL, which theoretically increases bulkiness, consumes more graft, and decreases gliding. We hypothesized that this modification would require less tendon graft length and additionally will result in less stiffness than the classically described Brand transfer. We present this modified technique as well as a retrospective case series of this procedure at a minimum of 6 months in follow-up.
Methods
This study was approved by our institutional review board.
Patient Selection and Chart Review
We reviewed the medical records of the senior author’s operative cases and identified nine consecutive patients with chronic low ulnar nerve palsy with MCP hyperextension and IP flexion over a 5-year period, indicated for claw correction. Index and middle fingers showed MCP hyperextension as well, with the transfers addressing MCP balance in these fingers, not only pinch via index adduction. Bouvier’s maneuver and active and passive range-of-motion assessments were performed to test the integrity of the extensor apparatus and for joint contracture. If blocking MCP joint hyperextension does not allow for IP joint extension, then a diagnosis of rigid claw is made, and the proximal IP joint capsule or extensor mechanism are interrogated for treatment prior to consideration of tendon transfer. 13 All patients also underwent a preoperative therapy for optimization and to assess the willingness of a patient to adhere to protocols. Patients who need an ECRB as a donor for an adductorplasty were excluded, as this changes the options for claw correction.14,15
For all patients who underwent surgery, charts were reviewed for demographic data; length of palsy prior to surgical intervention; preoperative and postoperative clinical measures, including grip, pinch, and range of motion; and complications.
Surgical Technique
All surgeries were done under tourniquet.
We begin by identifying the PL to ensure appropriate length of graft material. If a PL is not available for grafting, the plantaris tendon or toe extensors are used as an alternative source of tendon graft. There was no limitations in using an alternate tendon donor.
We next proceed to the ECRB dissection. We place an incision over the dorsal axis of the third metacarpal (Figure 1). Dissection proceeds through subcutaneous tissue, and the tendon is identified at its insertion, fully dissected, and freed from surrounding tissues.
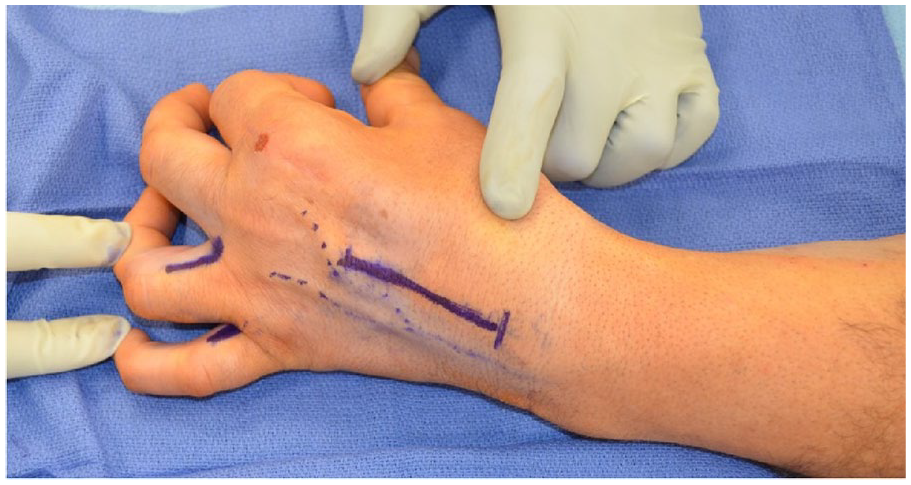
Incision markings, including incisions for the identification of the lateral bands to the ring and small fingers as well as the dorsal incision for identification of the extensor carpi radialis brevis.
Once the ECRB is identified, the lateral bands are then addressed. These are exposed through 1.5-cm incisions along the dorsal radial aspect of the long, ring, and small fingers as well as the ulnar aspect of the index finger at the dermal glabrous junction (Figure 2). Once the lateral bands are identified, vessel loops are passed around the lumbrical to label the canal.
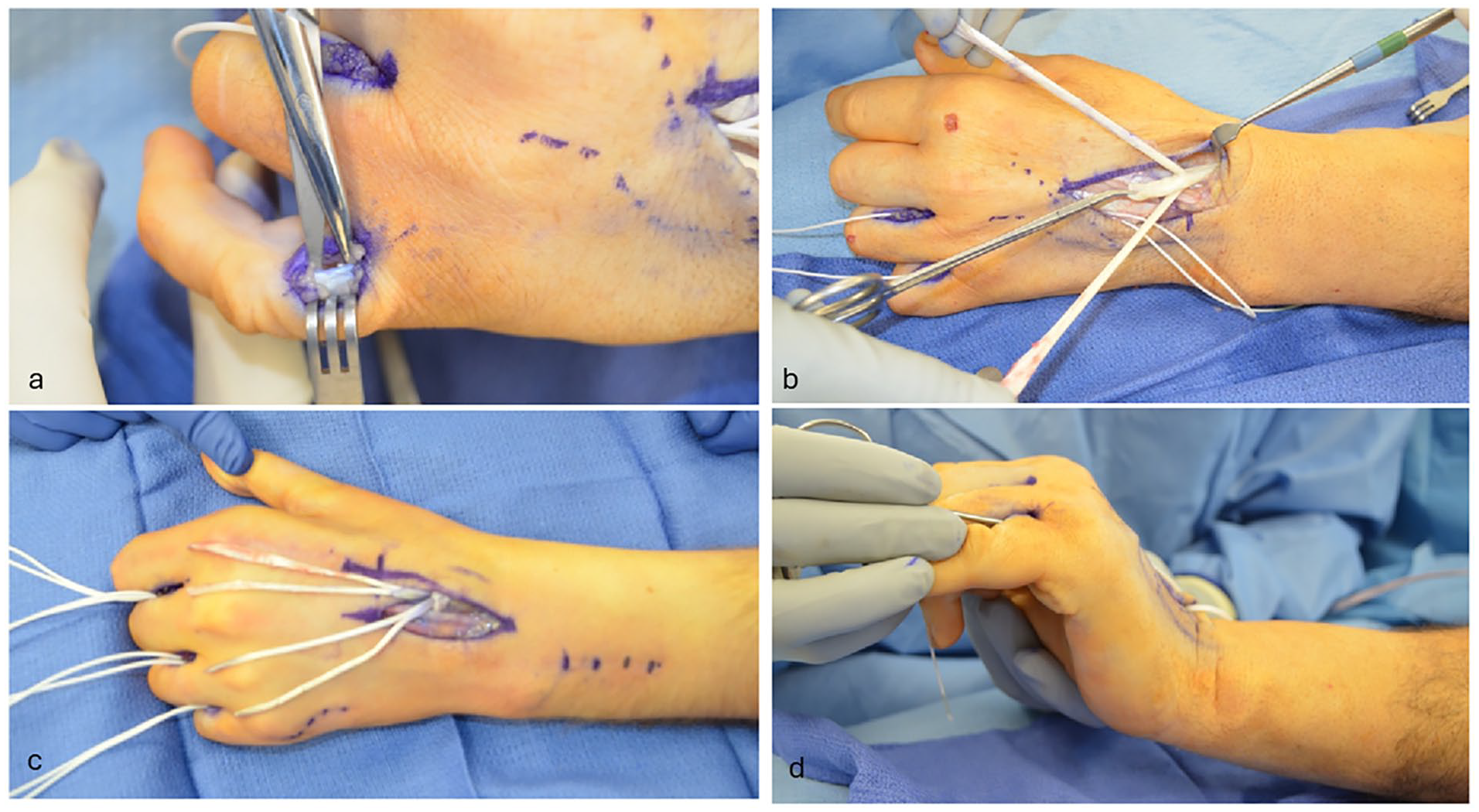
(a) Identification of the lateral band on the radial aspect of the small finger. (b) Disinsertion of extensor carpi radialis brevis and weave of palmaris longus 2 cm proximal to the distal aspect of extensor carpi radialis brevis. (c) Palmaris longus woven through extensor carpi radialis brevis with 2 limbs split to 4 tails and aligned with donor lateral band sites. (d) Palmaris longus tails passed through the lumbrical canals, volar to the intermetacarpal ligament using a Mosquito clamp.
Once the lateral bands of all four fingers are identified, harvesting of the PL tendon graft may then proceed. Sequential 1-cm transverse incisions are used to identify, confirm, and harvest the PL tendon. Tension is placed at each end, and smooth gliding is confirmed by alternating tension distally and proximally. The tendon graft is cut distally, and the distal end is delivered into the proximal wound. Using a tendon stripper, maximal length is obtained along the musculotendinous junction for the proximal graft cut. This should provide roughly 15 cm of tendon for a 4-tail tendon graft. In our series, the width of the graft was never too narrow to divide, and the length of the graft was never too short to complete the transfer.
After securing the graft, the ECRB is transected at its insertion. Three Pulvertaft weaves of the PL through the ECRB is performed 2 cm proximal to the distal end of the ECRB tendon at approximately the midpoint of the PL graft. This is secured with two 3-0 Ethibond sutures. With the tendon weave secured, 2 PL limbs of equal length should remain. These two limbs are each split, creating 4 tails.
Once the four tails for transfer are constructed, the tunnels of the lateral band in the lumbrical canals are opened. A passage is made deep and volar to the intermetacarpal ligament and proceeds dorsally. Each limb of the tendon graft to each of the fingers is passed through this passage and weaved through the lateral bands with the wrist at 45° and the MCP joints at 70° of flexion, with the IP joints held in full extension (Figure 3). Each transfer is secured with 3-0 Ethibond suture with 2 weaves for each finger. The surgeon should utilize tenodesis to adjust the tension to allow for extension of the IP joints without hyperextension.
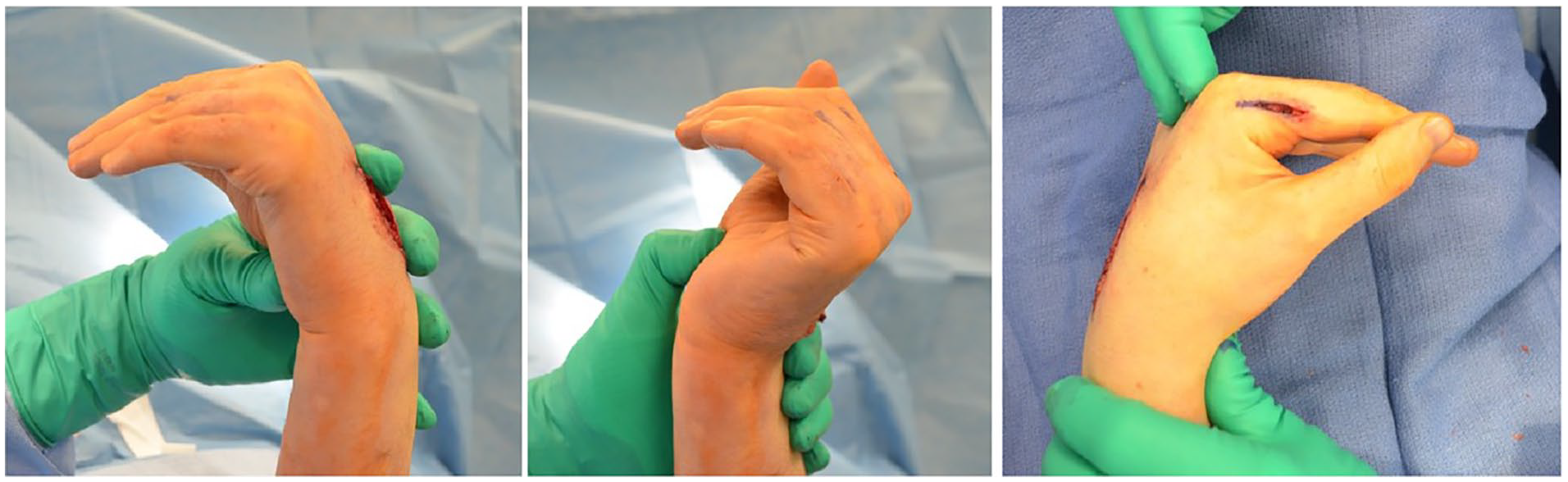
Tensioning with the wrist in 45° of extension, metacarpophalangeals in 70° of flexion, and interphalangeals in extension.
All incisions are then closed. The patient is splinted in a bulky dressing, and local anesthetic should be used for pain control.
Postoperative Course
A bulky plaster splint or cast is made in the operating room. The splint should keep the MCP joints flexed, the IP joints extended, and the wrist should be placed in 30° of extension to de-tension the extensor transfer.
The postoperative splint should be changed in 1 to 2 weeks postoperatively to check the surgical incisions and re-fit the splint to accommodate postoperative swelling. At 4 weeks, it is appropriate for an occupational therapist to fashion a thermoplastic splint. As with any period of immobilization, it is important to maintain mobility in the non-immobilized joints during splint wear (Table 1).
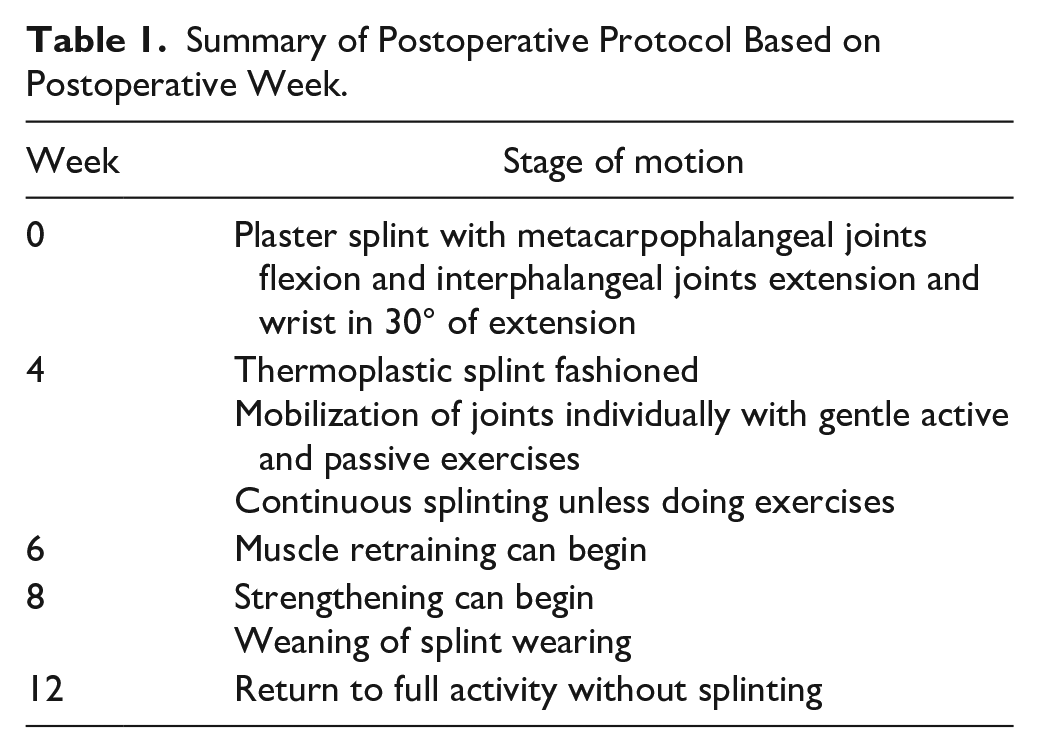
Summary of Postoperative Protocol Based on Postoperative Week.
At 4 weeks, the patient may begin mobilization with the assistance of an occupational therapist. Exercises should commence mobilizing one joint at a time. For example, the MCP joints should be mobilized in exercises separate from the IP joints. Motion should commence with gentle active and assisted exercises. Except for when participating in guided therapy protocols and home exercises, the patient should continue to wear their splint.
At the 6-week postoperative time point, the patient may begin muscle retraining, activating the muscles used in the tendon transfer. Electrical stimulation and biofeedback may be used to assist with retraining. 16 Whether these techniques decrease muscle atrophy is debated; however, it may enhance the patient’s familiarity with activation of the transferred muscles. Electromyography (EMG) biofeedback similarly allows the patient to attempt to control muscle signals as he or she attempts to activate the transferred muscles. 17 This has been described as improving the speed of recovery, although this was not directly studied.16,17 Strengthening exercises may be initiated at postoperative week eight, and the splint may be weaned for activities of daily living through week twelve, at which point the patient may resume full activity.
Results
We identified nine patients who underwent dynamic tendon transfer using a four-tailed tendon transfer with a modified weave through the ECRB tendon. Seven patients underwent transfer with a palmaris graft; one required a plantaris, and one required a toe extensor graft due to absent PL tendon.
The average age of patients at surgery was 45.0 years with an average follow-up duration of 1.1 years (min: 6 months, max: 3.4 years). Eight of nine patients were male, and the average length of time between injury and tendon transfer was 3.7 years (min: 1.3 years, max: 13.9 years). Six patients had undergone prior intervention but presented with persistent clawing secondary to the low ulnar nerve injury. Prior interventions included nerve reconstructions and repairs.
The length of surgery averaged 165 min with a tourniquet time of 116 min. Three patients were kept overnight for observation. All patients had a four-tailed graft anti-claw procedure to treat the index, middle, ring, and small fingers.
At the final follow-up, the range of motion in these patients was excellent. All patients had full flexion in the MCP, proximal interphalangeal (PIP), and distal interphalangeal joints. Eight patients had no residual MCP hyperextension; one had residual hyperextension of 15° (Figure 4, Supplemental Video 1). Grip was coordinated in all patients (Supplemental Video 2). Four patients exhibited slight joint contractures in flexion of the IP joints: one in the PIP of the small to 20°, and three with 15° of contracture in the PIP of the ring and small (Table 2). All patients had full active extension in the IP joints, up to the point where the joint contracture set in. Based on the Brand 8 criteria, all patients had excellent results.
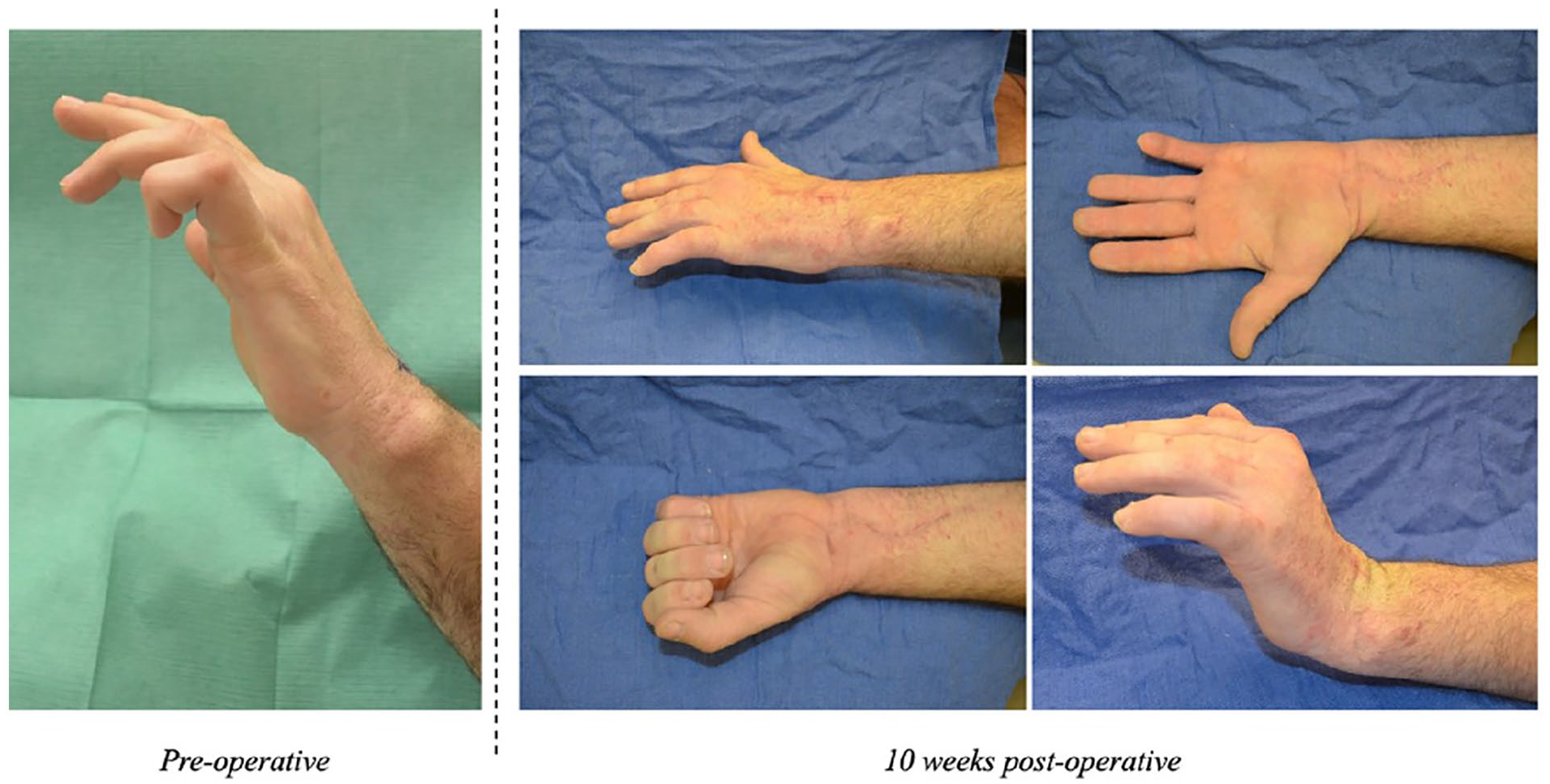
Comparison of hand posture preoperatively and at 10-week postoperative follow-up.
Summary of Patient Data.
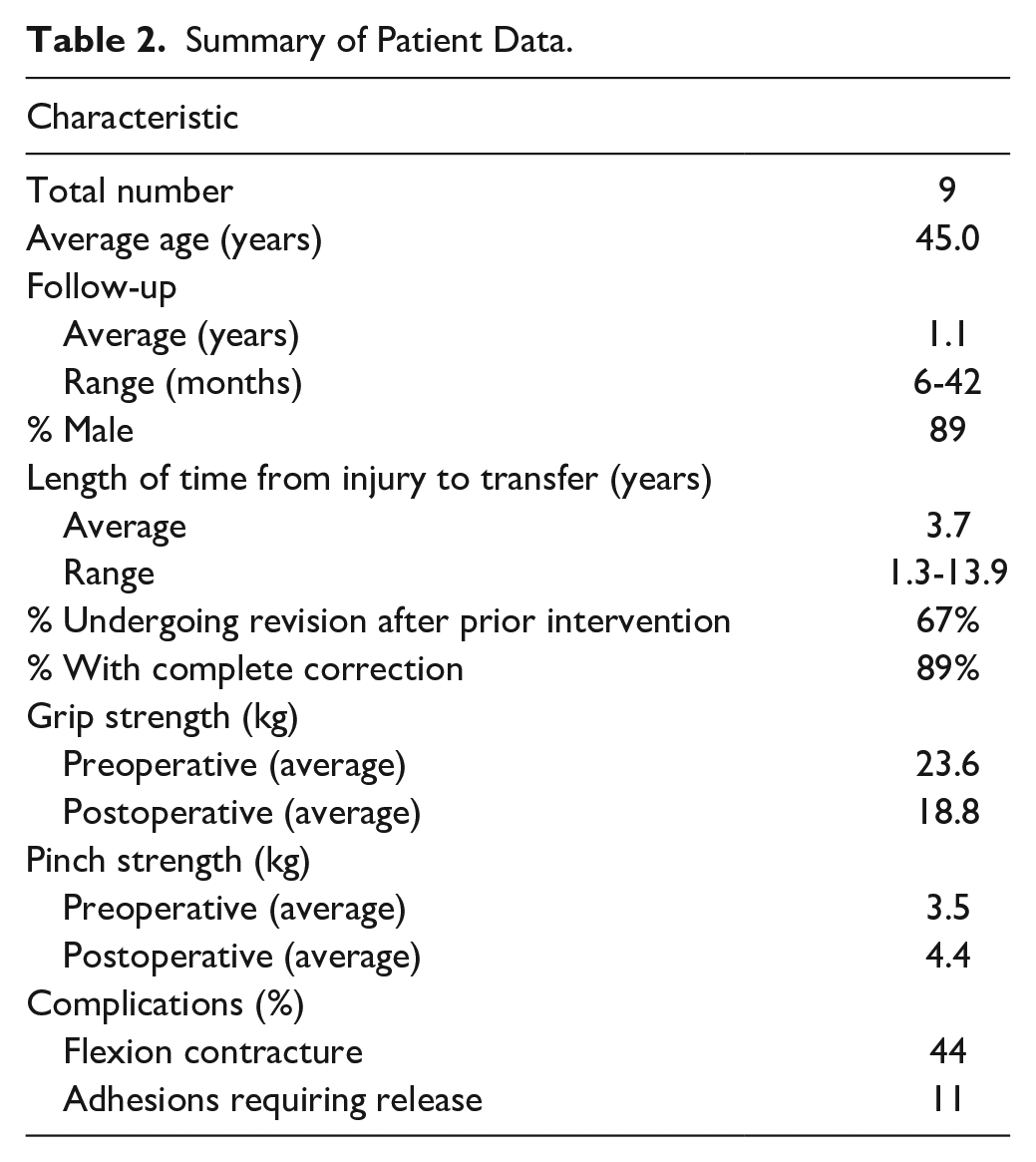
Average preoperative and postoperative grip strength were similar at 23.6 kg and 18.8 kg, respectively. Similarly, average preoperative and postoperative pinch strength were similar at 3.5 kg and 4.4 kg, respectively.
The only complication noted occurred approximately 2 years after the index operation. One patient, out of the four with greater than 1 year in follow-up, developed scarring in the extensor mechanism requiring tenosynovectomy and tenolysis of the extensor tendons and tendon grafts, along with a revision of the anticlaw procedure to the ring finger at the proximal tendon insertion and the small fingers at the level of the lateral band. The patient also had hypermobility of the small finger MCP joint and required capsulodesis. No other complications were noted in any patient.
Discussion
The patient with a low ulnar nerve palsy has an array of deficits: (1) absent flexion at the MCP joints and, if the extrinsic muscles are intact, resultant finger clawing; (2) synchronism for MCP and IP joint flexion, resulting in fingers curling into palm and pushing objects away rather than grasping; (3) deficits in key pinch; and (4) lateral mobility of fingers in extension. 18 Together, these can provide gross difficulty in hand function that is difficult to correct.
In this series, we present 9 patients who underwent a modification of the Brand procedure, where the ECRB was used as a four-tailed transfer to the lateral bands with a PL graft. Eight patients had total elimination of any MCP hyperextension. Although some patients had joint contracture, all patients had normal extension from full flexion to the point where the joint contracture set in, allowing for excellent range of motion in coordinated grasp, thus relaxing the intrinsic minus deformity. One patient had residual MCP hyperextension but without any clawing. A second patient required revision surgery.
There are several tendon transfers to provide dynamic correction of clawing, integrate MCP flexion and IP extension, and in some cases, augment grip strength. These transfers can be divided into superficialis transfers and transfers powered by wrist motors. While both sets of transfers reliably correct clawing, superficialis transfers do not augment grip strength, and Ozkan et al 19 demonstrated that the average grip strength improved in only 7% of patients who underwent superficialis transfer. Notably, however, grip strength declined in 3 of 9 patients. In addition, superficialis transfers can lead to the development of swan neck deformity, if overtensioned.6,7 Our series demonstrates no improvement in grip strength, but importantly no downgrading of grip strength in any patient and no development of a swan neck deformity at the 6-month follow-up visit.
Transfer of the extrinsic wrist extensors using a tendon graft–routed volar to the deep transverse metacarpal ligament (DTML) maintains hand strength and synergism. Classically described, the Brand tendon transfer utilizes ECRL or ECRB as motor with tendon graft passed through interosseous spaces, volar to the DTML and sutured to the edge of the lateral band and dorsal expansion of each finger (index, long, ring, and small), proximal to the proximal IP joint. 10
In the traditional Brand 8 transfer, the tendon graft for each finger is broadened and secured to the distal end of the ECRB, after which is it tunneled and fixed to the lateral bunds with heavy suture, such as stainless-steel wire. This results in a bulky transfer, both proximally and distally, which increases the risk of adhesions and decreases the gliding potential of the tendon. Furthermore, the broadening on insertion into the ECRB utilizes more of the tendon length; for patients with multiple clawing fingers, more tendon graft is thus needed.
In contrast, our modification of the Brand tendon transfer utilizes a single PL graft with a modified Pulvertaft weave wherein the graft is routed through the ECRB, and the middle of the graft is fixed into the donor tendon and split into 4 tails. This provides theoretical benefit by not requiring each finger to have a separate graft, reducing both bulk at the transfer site and the amount of graft needed. Furthermore, the tendon weave distally is done with smaller suture (3-0 Ethibond) and at a distal position on the lateral bands compared to the traditional Brand transfer, increasing the gliding potential of the tendon. Together, this suggests an improved outcome compared to the traditional transfer. Although our series reports on only patients who underwent our modified transfer without comparison to a control with traditional Brand transfer, our patients demonstrated excellent motion at the final follow-up and is an encouraging first step in improving outcomes, as historical reports have often been compromised by adhesions. One patient did require tenolysis, which we attributed to damage to the lumbrical canal during tendon passing.
In comparison to the results from Brand’s 8 original patient set, our modified transfer does demonstrate a higher rate of “excellent results” than the original transfer. Pinch in our data set is similar to previous sets of the Brand transfer (4.4 vs 4.5 kg). 20 Although detail discussions on grip strength after the traditional transfer were not present in the literature, descriptions of long-term adhesions were. 21
As with any retrospective study, this series is limited by study design. Furthermore, given the relatively rare nature of this condition, the number of patients in this series is limited. Follow-up time is also limited for some patients, precluding any discussion of long-term success or complications, such as the need for tenolysis for adhesion development, when compared to other transfers. This is the nature of the patient population who undergo these transfers. Future, prospective work, with direct comparison to other forms of claw hand reconstruction, is needed to fully clarify the role and success of this transfer, although early data are encouraging.
Conclusions
Claw deformity is a devastating sequela of low ulnar nerve injury that greatly impacts hand function. For many patients, addressing the MCP joint hyperextension through a variety of tendon transfers allows for alleviation of the clawing effect and finger extension. The Brand transfer is one of the many described approaches for this condition but suffers from an increased risk of tendon adhesions through the lumbrical canal. We describe a modification of the Brand transfer that utilizes a distal weave to prevent adhesion in the lumbrical canal and allow for smoother motion, with great success in a small series of patients. Given this initial success, our modification of the Brand transfer should be considered for patients with claw deformity from ulnar nerve pathology.
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All human and animal studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Statement of Informed Consent
All patients were informed of possible participation in any 165-minute-long experimental treatment in this study and agreed to participate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.