
Abstract
Background:
The objective of this study was to examine the effect of wrist rotation on the scapholunate interval in the posteroanterior radiograph and to identify radiographic landmarks on the posteroanterior projection that can be used to assess position.
Methods:
Eleven healthy cadaveric wrists were radiographed in the neutral position and subsequently were rotated and imaged from 30° pronation to 30° supination in 10° intervals. At each interval, the scapholunate interval was measured as well as the following landmarks: (1) the visible perimeter of the base of the hook of the hamate; (2) the radial-ulnar distribution of the dorsal nonarticular surface of the distal third metacarpal head; (3) the radial-ulnar distribution of the pisiform about the longitudinal axis of the ulna; and (4) the overlap of the pisiform and triquetrum.
Results:
The scapholunate interval was largest in the neutral position and linearly decreased by 34% for every 10° of pronation and decreased nonlinearly by 86% after the first 10° of supination. The appearance of the distal third metacarpal head was shown to be sensitive to both pronation and supination. The perimeter of the hook of the hamate and the distribution of the pisiform compared to the ulna were both shown to be sensitive to supination, whereas overlap of the pisiform and triquetrum was not shown to be sensitive to either direction of rotation.
Conclusions:
Our results highlight the significant effect of rotation on radiographic landmarks at the wrist, indicating that 10° of supination can drastically alter the developed radiograph.
Introduction
Scapholunate ligament instability (SLI) secondary to a scapholunate ligament (SL) tear is the most common form of carpal instability, occurring most frequently in working-age men.1,2 The most common causes of SL tears are wrist hyperextension with or without wrist fracture, caused by a fall onto an outstretched hand. Left untreated, SLI can contribute to scapholunate advanced collapse with associated osteoarthritis. Scapholunate advanced collapse is responsible for 55% of wrist osteoarthritis. 3 Due to the young demographic of those with SL injuries, it is essential to identify these injuries quickly to avoid years of chronic pain, reduced joint range of motion, and missed time at work. 4
Radiography is the oldest wrist imaging modality and is still the most commonly used.5,6 Standard wrist radiographs include the lateral and the posteroanterior (PA) projection, with PA axial (scaphoid) and anteroposterior radiographs being useful ancillary projections for identifying SLIs.1,5 The sensitivity of plain radiography is dependent on proper anatomical positioning, which can be difficult for patients to maintain, especially when pain is present. The most effective noninvasive diagnostic test for SL ligament instability is MRI 7 ; however, access is variably limited, largely due to the high cost associated with this imaging technology. Stress x-rays are an extension of static radiographs, typically used to help visualize dynamic SLIs not seen on static radiographs but with limited consensus in clinical practice due to poor reliability.1,8
There are multiple carpal indices associated with SLI on PA and lateral radiographs. One of the most commonly used indices is the scapholunate interval, measured at midscaphoid and lunate on the PA radiograph with an interval greater than 3 mm associated with SLI. 1 Well-positioned PA radiographs can be difficult to acquire given limited hand and wrist range of motion in the presence of injury and disease; a lack of understanding of the ideal patient positioning by the radiographer may also contribute. Several studies demonstrated that wrist rotation affects the measurement of carpal indices9 -11 but focused primarily on the sensitivity of carpal indices on lateral radiographs, used small sample sizes, used different imaging techniques, or did not examine the SL interval as an outcome. The primary objective of this study was to examine the effect of wrist rotation on the SL interval on the PA radiograph. Our secondary objective was to identify radiographic landmarks on the PA projection that can be used to assess wrist position.
Materials and Methods
This project was approved by the institutional research ethics board. Eleven fresh-frozen cadaveric arms, 9 amputated at the midhumerus and 2 full arms, were radiographed. The specimens (4 right arms, 7 left arms) were from 10 men and 1 women with a mean age of 70 years (range 39-88). Specimens with radiographic evidence of disease or trauma to the carpal or forearm bones were excluded from the study, and all specimens were skeletally mature with closed epiphyseal plates. Specimens with radiographic evidence of SL widening (SL intervals ≥ 3 mm in the “true PA” position) were excluded. 1
A custom radiolucent device was fabricated to control the internal and external rotations of the wrist. The device consisted of 3 stackable 10° hardwood wedges, which allowed the controlled rotation of the wrist through a 30° arc in 10° intervals. The anterior surface of the forearms and wrists was positioned and strapped to the wedges. The arms were rotated about the long axis of the ulna. The arms were secured in the neutral radial-ulnar deviation position, with the long axis of the third metacarpal aligned with the radial long axis. The arms were constrained such that they could not rotate relative to the wedge system when inclined. The arms were rotated from our predetermined “expert neutral” position both through supination and pronation (Figure 1). For the purposes of this study, the expert neutral position was considered the “true” PA and is defined as the degree of pronation required to compensate for the subject’s thenar eminence, placing the coronal carpal plane perpendicular to the incident x-ray beam. This is the radiographic definition of the “true” PA used in our center.
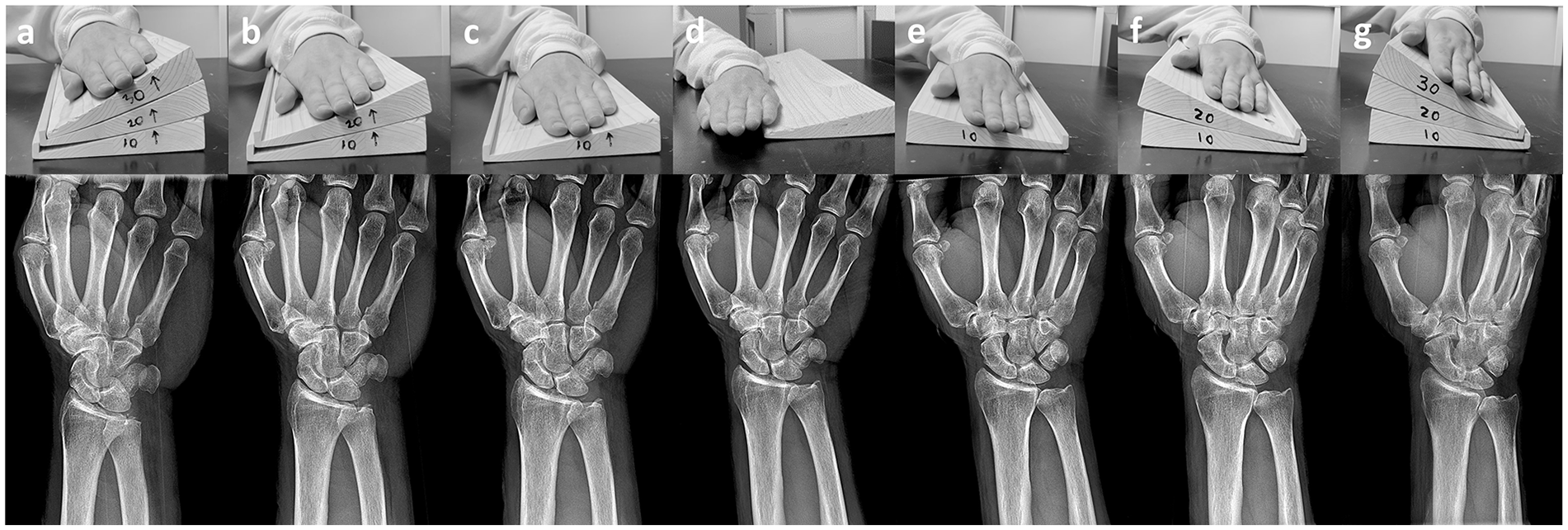
Full rotation series indicating wrist position and associated radiographs at (a) +30° pronation, (b) +20° pronation, (c) +10° pronation, (d) expert neutral, (e) +10° supination, (f) +20° supination, and (g) +30° supination.
Subsequent PA radiographs of the wrist were taken at each interval of rotation, producing 7 distinct positions: +30° pronation, +20° pronation, +10° pronation, expert neutral, +10° supination, +20° supination, and +30° supination (Figure 1). All radiographs were taken with a GE Discovery XR656 system (GE Healthcare, Milwaukee, Wisconsin) from a standardized source image receptor distance of 100 cm. Radiograph markers were used to label each radiograph. The central ray of the x-ray was focused perpendicular to the carpus and collimated from just distal to the metacarpophalangeal joints to just proximal to the distal radioulnar joint and from 2.5 cm lateral to 2.5 cm medial to the hand as outlined by Long et al. 12
Radiographs were exported as TIFF files to the hard drive of a workstation for analysis. The 4 proposed landmarks, as well as the SL interval, were evaluated on each radiograph using ImageJ, Version 1.53q (National Institutes of Health, Bethesda, Maryland).
The first author measured the SL interval according to the protocol outlined by Said et al, 13 which was further confirmed via consensus with 2 independent hand surgeons blinded to the degree of rotation in each film. Once the SL interval was measured for each subject’s rotation sequence, the values were normalized to the subject’s largest SL interval across the entire rotation sequence, expressed as a percentage. This gave results as a percentage of the maximum visible SL interval, an attempt to normalize anatomical variation in the SL interval among subjects.
The following radiographic landmarks were measured on each radiograph: the length of the visible portion of the margin of the hook of the hamate (teardrop), the ratio of the radial and ulnar area of the dorsal nonarticular surface of the head of the third metacarpal (balanced metacarpal heads), the ratio of the radial and ulnar area of the pisiform about the ulnar longitudinal axis to the total pisiform area (pisiform position), and the percentage of the triquetral area overlapped by the pisiform (pisiform overlap). The detailed measurement protocol for each landmark is as follows:
Teardrop
The circumferential border of the hook of the hamate is demarcated by a layer of cortical bone and appears as a crisp, radiopaque outline. The length of the unbroken visible circumferential perimeter of the proximal base of the hook of the hamate was measured, tracing radially to ulnarly for each specimen (Figure 2b). Once the perimeter was measured for each subject’s rotation sequence, the values were normalized to the subject’s largest perimeter across the entire rotation sequence, expressed as a percentage. This gave results as a percentage of the maximum visible perimeter, an attempt to normalize anatomical variation in the hook of the hamate among subjects.
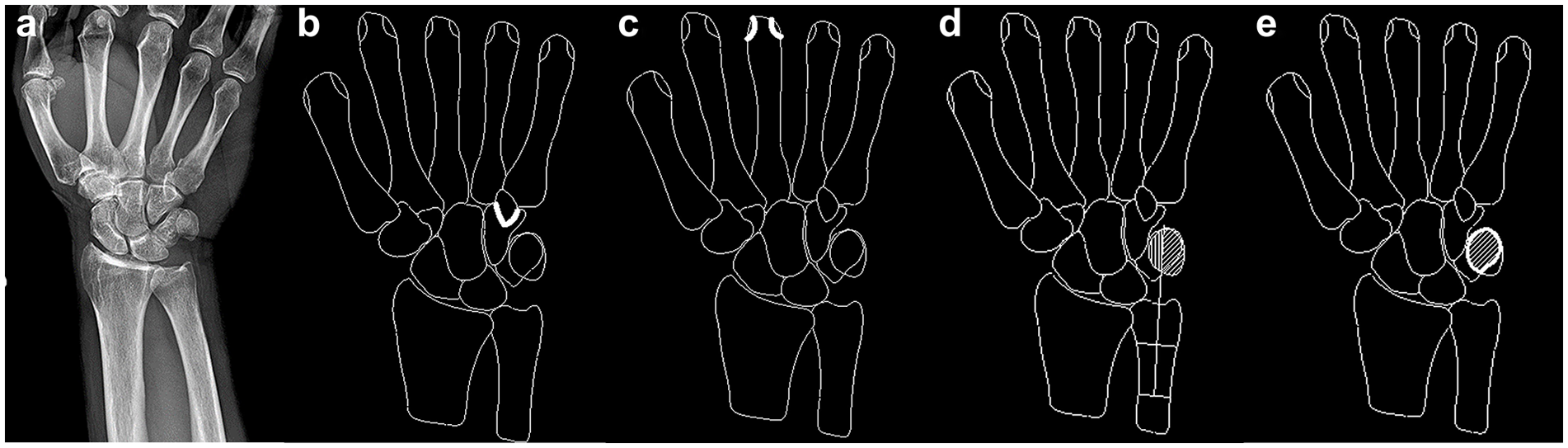
(a) Expert neutral radiograph, with (b) the perimeter of the hook of the hamate traced, (c) the dorsal surface of the distal third metacarpal head traced, (d) the ulnar axis within the pisiform traced, and (e) the overlap of the pisiform and triquetrum traced.
Balanced Metacarpal Heads
The concave-superficial radial and ulnar aspects of the dorsal nonarticular surface of the distal third metacarpal heads can be seen to project just inside the radial and ulnar aspects of the convex-superficial articular surface of the third metacarpal on the expert neutral PA radiograph. The area between the dorsal nonarticular surface and the metacarpal articular surface was measured separately for the radial and ulnar aspects (Figure 2c). The ratio of the radial and ulnar areas over the total area was calculated, again potentially normalizing for anatomical variation among subjects.
Pisiform Position
The ulnar longitudinal axis was defined as the line which connects the midpoints of two lines that perpendicularly bisect the visible medial and lateral ulnar cortices. Next, the visible margin of the pisiform was traced, following the curvature of the pisiform cortex. The areas projecting within the pisiform lying radially and ulnarly of the axis were measured separately (Figure 2d). These radial and ulnar areas were then normalized to the total visible dorsal pisiform area, giving results as a percentage of total visible pisiform area.
Pisiform Overlap
The projected areas of the triquetrum and pisiform were measured after tracing the margin of each bone. The area common to both regions, represented by the overlapping area between the pisiform and triquetrum, was also measured (Figure 2e). The overlapping area was normalized to the total visible triquetrum surface area, giving results as a fraction of visible surface area.
Radiographs of the entire rotational sequence from four randomly selected subjects were measured twice, separated by a minimum washout period of 1 month by the first author and an independent observer to assess the intraobserver and interobserver reliability. An instructional session with an illustrated manual was provided before data measurement to ensure that observers used identical definitions of each measurement. The first author was trained on how to read wrist radiographs by a senior radiographer, who confirmed the measurement protocols used. The observers were blinded to the results of the previous reading for each measurement.
All statistical analyses were completed with a 95% confidence interval (CI) for all measures. The first step in the statistical analyses was to compare the intraobserver and interobserver reliability of the measurements of the carpal indices. Pearson’s correlation coefficient, r, was used to determine the linearity between the observers’ measurements, with the absolute values of Pearson correlations defined as weak (<0.30), moderate (0.30-0.50), or strong (>0.50). 14 Moderate and strong correlations were considered satisfactory. Next, the mean and standard deviation for each carpal index from pronation to supination of the wrist were calculated, with the assumption of a single measurement and absolute agreement. The mean of each carpal index was plotted against wrist rotation to estimate change in each carpal measurement per degree of pronation and supination. To evaluate the effects of pronation and supination of the wrist on carpal indices, one-way analysis of variance (ANOVA) tests were used (P ≤ .05). The last step of the analysis was to compare carpal indices from pronated and supinated radiographs, respectively, with those on the expert neutral radiographs. Tukey’s honestly significant difference (HSD) was used to determine the level of significance between the carpal indices in the varying degrees of rotation with that in expert neutral.
Results
Satisfactory interobserver and intraobserver reliability was found for all proposed landmarks (Table 1) in all degrees of rotation, with the exception of the hook of the hamate measurements in 20° pronation (interobserver) and 10° pronation (intraobserver). Most measurements showed moderate-to-strong correlations. There was no variability in the measurements of the perimeter of the hook of the hamate and the distribution of the third metacarpal head at extreme pronation and supination. As a result, the correlation coefficient could not be computed for these frames. Specimen means and standard deviations for the SL interval and the 4 landmarks were plotted against the degree of rotation to better illustrate the effect rotation had on each measure (Table 2).
Interobserver and Intraobserver Reliability of Radiographic Measurements Expressed as Pearson’s Correlation Coefficients (95% CI).
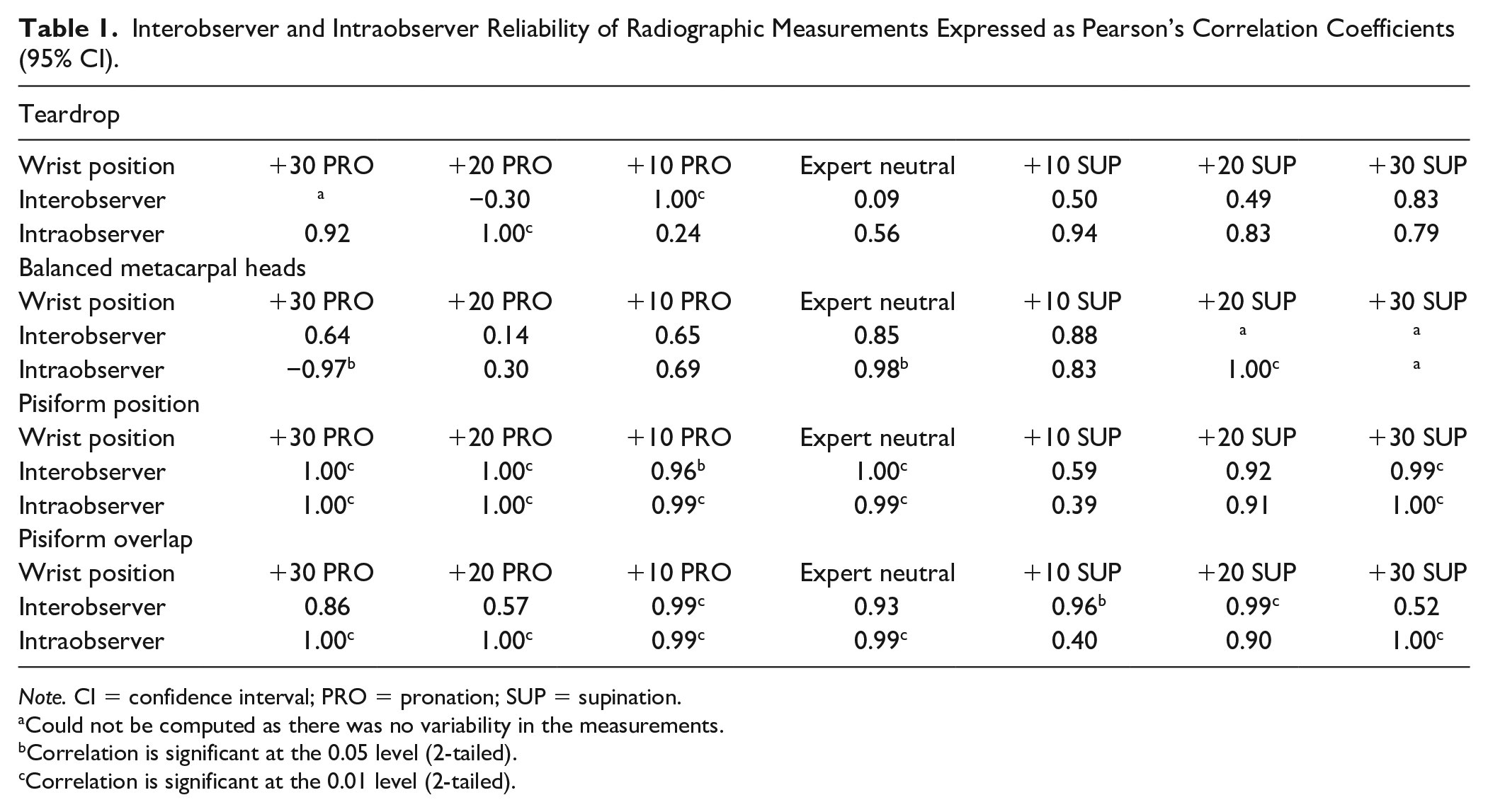
Note. CI = confidence interval; PRO = pronation; SUP = supination.
Could not be computed as there was no variability in the measurements.
Correlation is significant at the 0.05 level (2-tailed).
Correlation is significant at the 0.01 level (2-tailed).
Specimen Means and Standard Deviations for the Scapholunate Interval and Carpal Landmarks at Each Degree of Wrist Pronation-Supination.
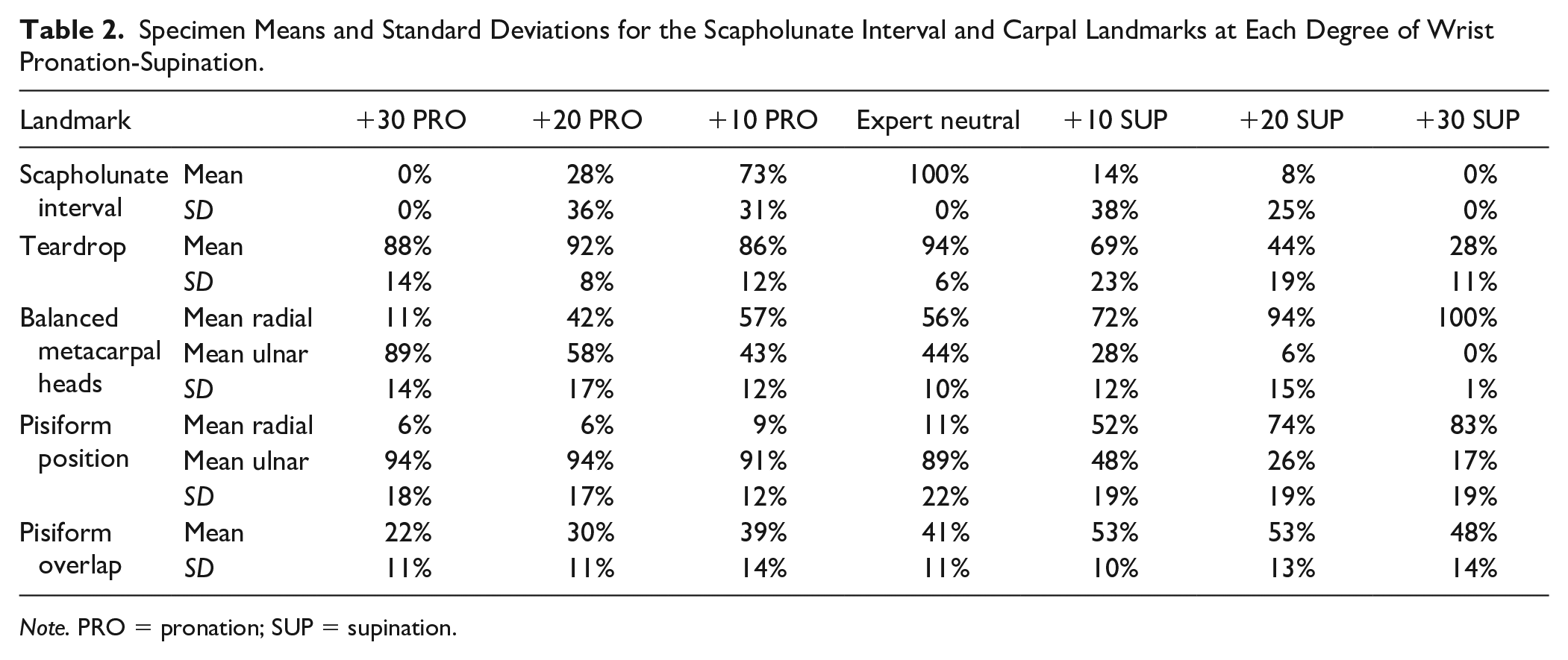
Note. PRO = pronation; SUP = supination.
The mean SL interval in the expert neutral position was 2.20 mm, consistent with reported normal values.13,15 -17 The largest SL interval was consistently measured in the expert neutral position. The SL interval was found to be sensitive to wrist rotation, decreasing progressively as the wrist rotates away from the expert neutral in both pronation and supination (Figure 3). Wrist rotation significantly impacted the SL interval, decreasing linearly (R2 = 0.99) 35% for every 10° of pronation compared to that of the neutral position. The SL interval was also shown to decrease in supination but did not exhibit the same linear trend, rather decreasing rapidly by 86% when rotated 10° from the expert neutral position.
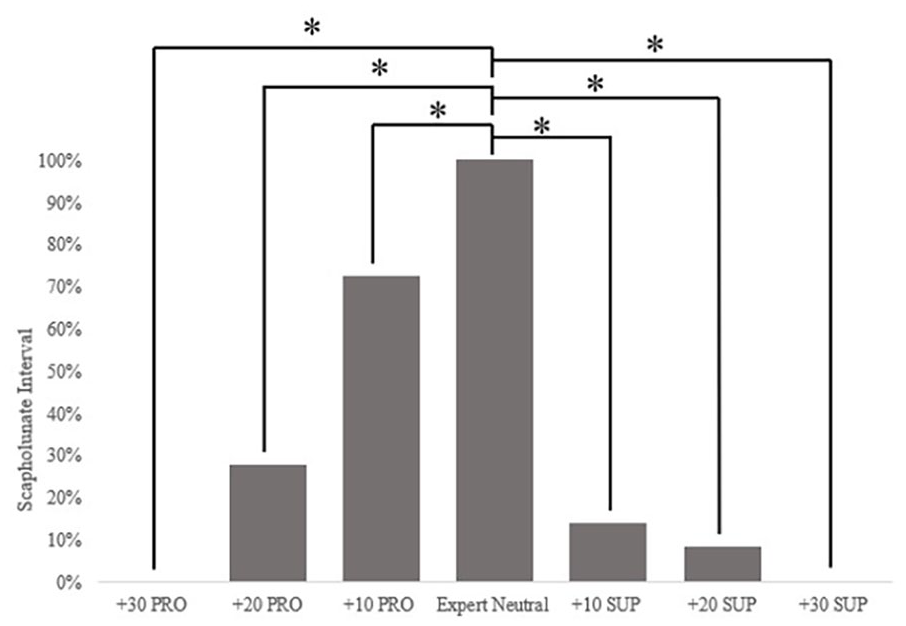
The effect of pronation and supination of the wrist on the mean measured scapholunate interval. Results are presented as a fraction of the largest measured interval to account for variations in individual specimen anatomy.
All 4 proposed bony landmarks were shown to change as a function of wrist rotation. The visible perimeter of the hook of the hamate was found to decrease with supination while remaining unchanged throughout pronation (Figure 4a). In supination, the visible perimeter was shown to decrease by 22% for every 10° of rotation away from the expert neutral position. The R2 value of 0.99 confirms the linear trend. One-way ANOVA results validate that there is no statistically significant difference between pronated rotation and that of the expert neutral frame and that the visible perimeter remained unchanged as a function of pronation (Table 3).
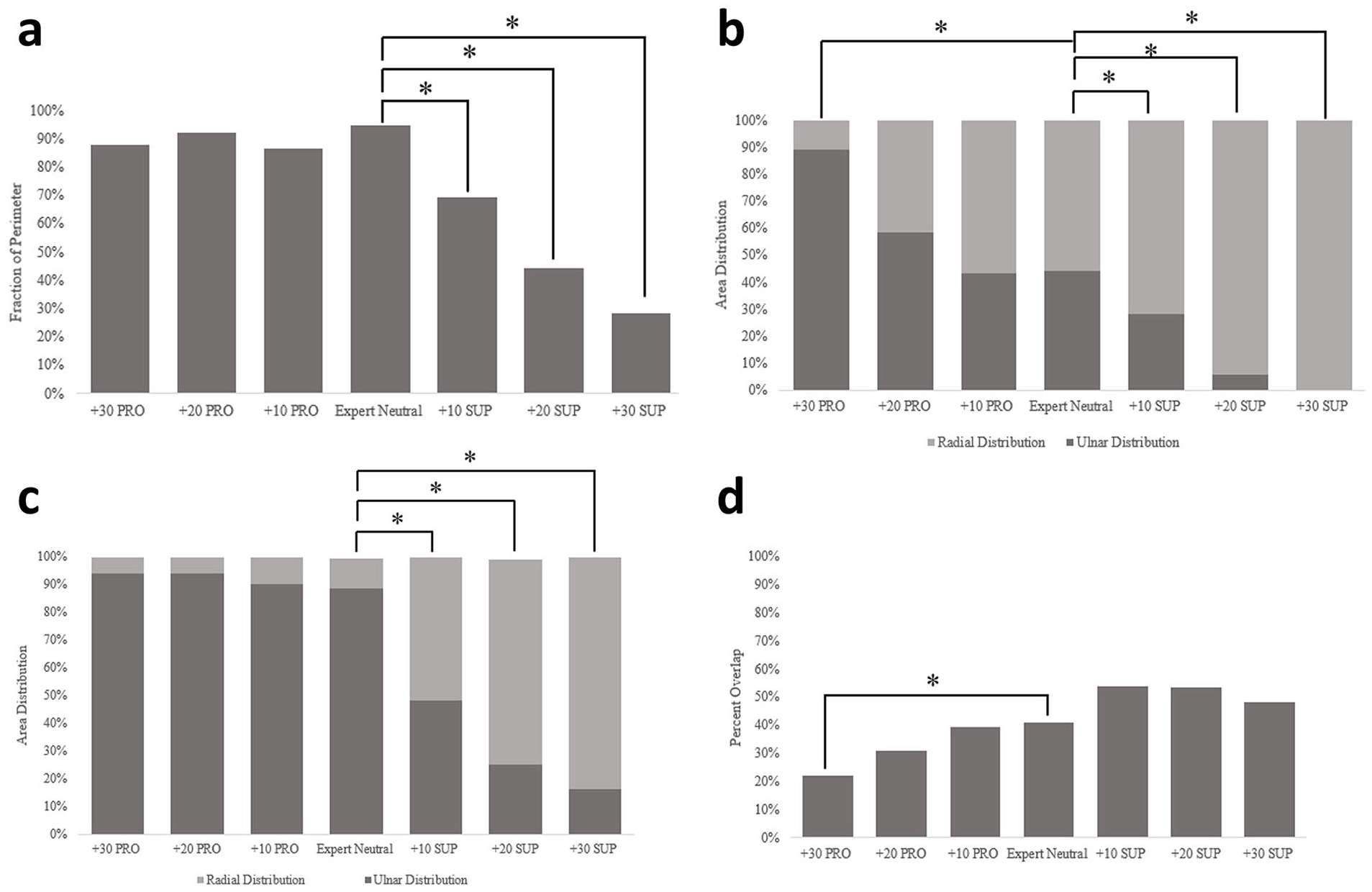
The effect of pronation and supination of the wrist on (a) the mean visible perimeter of the hook of the hamate, (b) the mean area superficial to the dorsal nonarticular surface of the distal third metacarpal heads, (c) the mean area of the pisiform about the long axis of the ulna, and (d) the mean overlap of the pisiform and the triquetrum. Results are presented as a fraction of total measurement to account for variations in individual specimen anatomy.
Tukey HSD Post-hoc for Multiple Comparisons Between Rotated Carpal Index Means and the Reference Neutral Frame.
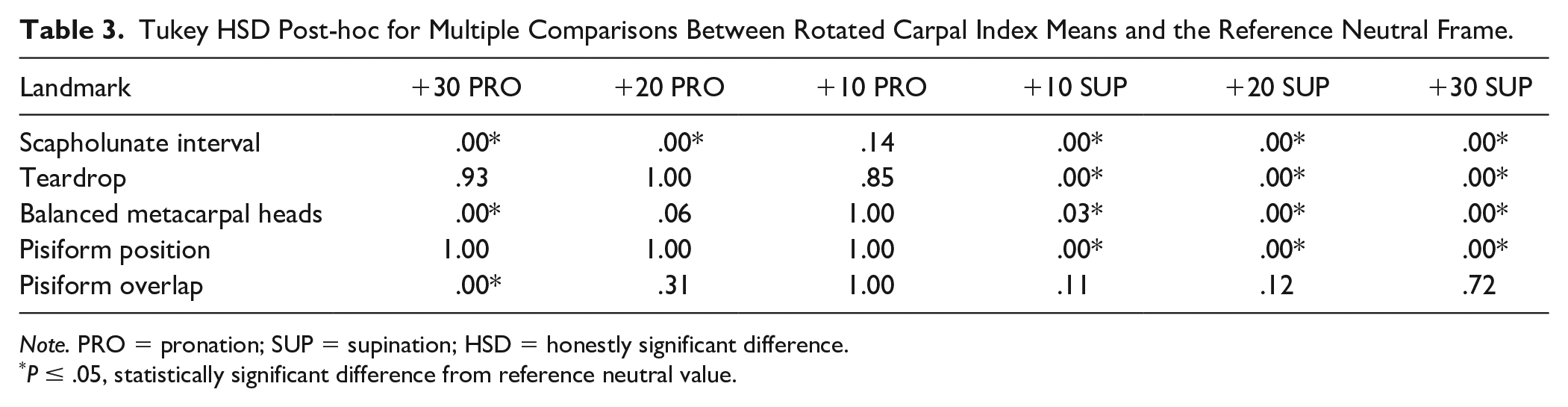
Note. PRO = pronation; SUP = supination; HSD = honestly significant difference.
P ≤ .05, statistically significant difference from reference neutral value.
The distribution of the third metacarpal head was shown to vary linearly as a function of wrist rotation. The distribution of the area peripheral to the dorsal nonarticular contour was shown to transition from ulnarly distributed at extreme pronation to radially distributed at extreme supination at an average rate of 14% per every 10° of rotation (Figure 4b). This linear relationship was demonstrated by an R2 value of 0.94 with statistically different mean measurements compared to the expert neutral position across the entire rotation sequence (Table 3).
The distribution in area of the pisiform about the ulnar axis remained consistent in pronation, with the distribution shifting radially when the wrist was placed into supination (Figure 4c). There was no statistical significance between means in pronation and that of the expert neutral position (Table 3). As the wrist is supinated away from the expert neutral position, the distribution of the total pisiform area linearly shifts ulnarly to radially at an average rate of 24% for every 10° of pronation (R2 = 0.92).
The pisiform and triquetral overlap showed the reverse trend; supination did not affect the apparent measurement, and pronation decreased the apparent measurement (Figure 4d). The overlapping area was found to decrease by 7% every 10° of pronation away from the expert neutral position. The linear relationship was confirmed an R2 = 0.94. Statistical significance was only found between the +30° pronation and the expert neutral frame (Table 3).
Discussion
This study aimed to evaluate the effect of wrist pronation and supination on the SL interval and 4 proposed radiographic landmarks. The measured SL interval was significantly affected by both wrist pronation and supination, with as little as 10° of wrist pronation changing the measurement by 27% compared to that of the expert neutral position (Figure 3, Table 2). Linear modeling of our results shows that the apparent SL interval decreases by 35% for every 10° of pronation and decreases rapidly by 86% at the first 10° of supination. This result is clinically relevant as unrecognized rotation positioning errors between 10° and 20° regularly occur in the clinical environment. 10 These data suggest that wrist positioning is of critical importance when assessing the SL interval, especially given the years of pain, disability, and loss of hours on the job that result from failure to detect SLI. Due to the relatively small size and marked complexity of the carpus, slight pronated or supinated rotation of the wrist reduces the accuracy of SL interval measurements, potentially leading to missed SLI and error in the treatment of SL wrist injuries.
Robertson et al 11 investigated the relationship between wrist internal and external rotation on multiple carpal indices in lateral and PA radiographs using digitally reconstructed radiographs from 5 healthy volunteers. The digitally reconstructed radiographs were rotated from a predefined neutral position to 15° internal and external rotation in 5° increments, and simulated radiographs were taken from each rotation interval and printed off to be measured by 5 blinded observers. Bonferroni’s correction was used to compare sample means of rotated frames to that of the neutral frame, showing no correlation between simulated rotational malpositioning and the 13 carpal indices, including SL interval, measured in the PA radiograph. Our results differed from those reported by Robertson et al, 11 with significant change noted in measured SL interval with pronated and supinated rotation (Figure 3). These variations between results may be accounted for due to different rotation and carpal measurement protocols used between our study and that of Robertson et al 11 and our use of radiographs rather than digitally reconstructed radiographs. In our study, the axis of wrist rotation followed the long axis of the ulna, with the radius rotating about the stationary ulna through pronation and supination. This more accurately replicates the physiologic axis of forearm rotation, which follows the line connecting the center of the radial head proximally to the fovea of the distal ulna distally. 18 Robertson et al 11 simulated wrist rotation by rotating the digitally reconstructed radiographs about the radial long axis, keeping the radius stationary and rotating the ulna about the radius. Due to the projective nature of plain radiography, rotating the carpus about the radial long axis may have no visible effect on the relative position of carpal landmarks in relation to one another, especially for landmarks near the axis of rotation, such as the SL interval. Robertson et al 11 followed the SL distance measurement protocol presented by Cautilli and Wehbé, 15 wherein the distance is measured from the proximal ulnar-most corner of the scaphoid to the proximal radial-most corner of the lunate. Said et al 13 indicate the optimal location to measure the SL interval is at the midpoint of the SL joint, as this is the point with the least variability in measurement and is supported by MRI findings reported by Schimmerl-Metz et al. 19 Measuring the SL interval at the midpoint of the joint may reduce the variability in our results, better representing the effects wrist pronation and supination have on the measured SL interval in the PA radiograph.
The landmarks that were most sensitive to wrist supination were the visible perimeter of the hook of the hamate, the distribution of the distal dorsal third metacarpal head, and the distribution of the pisiform about the ulnar long axis. Only the distribution of the metacarpal heads was shown to respond to both supination and pronation. It was also shown that the overlap of the pisiform over the triquetrum did not vary significantly with wrist pronation or supination (Table 3). Interobserver and intraobserver reliability showed moderate to strong results, particularly with mild rotation compared to the neutral position. The extremes of rotation considered in our study are unlikely to occur in clinical settings; hence, we feel lower reliability at these extremes may not be significant.
Our study suggests that radiographers can potentially use the assessment of the hook of the hamate, third metacarpal head, and pisiform position with respect to the ulnar long axis to determine whether repeat radiographs are required and to hone their positioning skills over time. Radiologists and clinicians can potentially use these landmarks to help determine whether wrist radiographic series need to be redone due to poor positioning. Clinicians can use these landmarks to help guide clinical decisions when determining whether to request further medical imaging to investigate the SL joint or to proceed with the current treatment plan.
Our results support the expert neutral position used for PA wrist radiographs at our center. The expert neutral represents the “true” PA in our study and is defined as the amount of pronation required to compensate for the subject’s thenar eminence, placing the coronal carpal plane perpendicular to the incident x-ray beam (Figure 1d). Our results confirm that in this position, the largest SL interval was measured, and therefore, the standard position in which the SL interval should be measured for the greatest clinical relevancy.
Limitations of our study are that the sample only included cadaveric specimens and possible unknown inconsistencies in the positioning of the x-ray beam central ray. Cadaveric specimens, the majority of which were amputated at the midhumerus, may not accurately represent the rotational positioning errors that would occur with human participants. Without centering the central ray precisely through the same point across all the series of rotation, there may be unrecognized magnification caused by beam divergence. However, the protocol used more accurately replicated the clinical environment, and given the proximity of the anatomy measured, the effect of magnification on our measurements is likely negligible. Another limitation was that all measurements were performed in specimens with normal wrist bony anatomy. Expanding the study to include volunteer healthy and injured participants is required for further validation.
Conclusions
Our study illustrates the sensitivity of the SL interval to wrist rotation in a healthy cadaveric cohort, emphasizing the importance of proper anatomical positioning in wrist PA radiographs. Our results indicate that the landmark most sensitive to wrist rotation is the distribution of the third metacarpal head, with the perimeter of the hook of the hamate and the position of the pisiform being sensitive to pronation. The overlap of the pisiform was not found to be sensitive to wrist rotation. Clinicians can use these landmarks to confirm positioning within the PA radiograph to potentially reduce the error in measurement of the SL interval.
Footnotes
Acknowledgements
We would first like to thank the Arthritis Society of Canada for generously funding this research, and others like it, in their mission to fight and extinguish arthritis. We would like to acknowledge and thank the individuals and their families who have selflessly donated their bodies for use within scientific research. Lastly, we would also like to thank John Henry and Jamie Kueneman for their expertise and input over the course of this project.
Contributorship
MC, NS, and EL completed the research design. MC, EL, and GS completed data acquisition. Data and statistical analyses were completed by MC and EL. MC, EL, and NS completed data interpretation. MC wrote the manuscript. NS, EL, and GG critically analyzed the article. All authors have read and agreed upon the final version of the manuscript.
Ethical Approval
Ethical approval for this study was obtained from the Western Research Ethics Board (120285).
Statement of Human and Animal Rights
The authors declare that the procedures followed in this study were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 and 2008.
Statement of Informed Consent
Informed consent was not required for this study due to the nature of the research and the use of cadaveric specimens.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through an Innovation Grant from the Arthritis Society of Canada (IG-21-0000000017).