
Abstract
Background:
Intramedullary screw fixation of phalangeal and metacarpal fractures has gained popularity as a method of providing rigid internal fixation with minimum tendon disturbance, allowing early mobilization and rehabilitation. Despite this, the literature on outcomes using this technique is limited. Thus, the aim of this study was to assess the short-term to medium-term outcomes of intramedullary screw fixation for proximal phalangeal fracture fixation in an Australian setting.
Methods:
A retrospective analysis of consecutive patients with a fracture(s) of the proximal phalanx fixated using intramedullary screws between January 2020 and March 2023 was conducted via telehealth.
Results:
Forty-six phalangeal fractures from 37 patients were included in this study. Mean Quick Disabilities of the Arm, Shoulder, and Hand score of 6.2 (range: 0-61.4, median: 0), mean pain visual analogue scale score of 1.8 (range: 1-7, median: 1), and mean total active motion of 231° (range: 132-282) were noted. A total of 4.4% of fractures sustained a major complication, and 94.6% of patients reported willingness to undergo intramedullary screw fixation again.
Conclusion:
This study concurs with the prior literature that intramedullary screw fixation is a safe and effective method of stabilizing extra-articular proximal phalangeal fractures in the short to medium term. Superior clinical outcomes, as well as cost-effectiveness and time-effectiveness, render it a viable alternative to plate fixation in this setting.
Introduction
Hand fractures are common and account for up to a third of all fractures presenting to emergency departments, with phalangeal fractures occurring more commonly than those involving the metacarpals.1 -3 Injury to the proximal phalanx comprises 39% of all phalangeal fractures and poses a significant financial and health burden to both the individual and the community.4 -6 Thus, optimal management is key.
The treatment objective once the proximal phalanx is fractured is to ensure sufficient stability in a satisfactorily reduced position to allow early mobilization, thus preventing the formation of adhesions that may limit range of motion and function. 4 Many of these fractures are stable and can be treated nonoperatively.7,8 However, fracture pattern and mechanism, as well as patient characteristics and functional requirements, may necessitate surgical intervention.1,7 Rigid fixation constructs are generally preferred to nonrigid fixation, as they facilitate precise alignment and earlier mobilization. However, stable fixation is only one determinant of outcome, with invasiveness, degree of soft tissue dissection, and cost also important considerations. 9
Intramedullary screw fixation of phalangeal and metacarpal fractures has gained popularity as a method of providing rigid internal fixation with minimum tendon disturbance, allowing early mobilization and rehabilitation, with novel methods of instrumentation broadening the indications.10,11 Screws may be inserted via retrograde intra-articular, antegrade intra-articular, and antegrade transarticular routes, with choice determined via fracture pattern, patient characteristics, and surgical preference.
Despite the increasing popularity and adoption of the use of intramedullary screw fixation, the literature on outcomes using this technique is limited. Thus, the aim of this study was to assess the short-term to medium-term outcomes of intramedullary screw fixation for proximal phalangeal fracture fixation in an Australian setting.
Methods
This study was performed as a retrospective review of a series of consecutive patients with proximal phalangeal fractures stabilized by intramedullary screws by 2 fellowship-trained orthopedic hand surgeons in Sydney and the Gold Coast, Australia. The intramedullary screws were inserted via either antegrade or retrograde routes. Following provisional fracture reduction, a guidewire was inserted through the proximal interphalangeal joint (for retrograde insertion), or through the metacarpal head or the metacarpophalangeal joint (for antegrade intra-articular and antegrade transarticular insertion, respectively). For extremely basal fractures, the technique of reverse instrumentation and stabilization of the fracture followed by antegrade intra-articular insertion, as described by Sivakumar and Graham, was used. 11 A small skin incision was then performed, and screw length measured. The diameter of the screw was determined by the phalangeal anatomy, aiming for an isthmic fit—in the vast majority of patients, a 2.2-mm cannulated compression screw (Medartis AG, Basel, Switzerland) was used. The screw was inserted with care taken to hold the digits in relaxed flexion, to maintain a normal cascade and prevent any malrotation. Patients commenced active range of motion within 1 week of the operation, with buddy strapping to the adjacent digits to control rotation, within a hand-based thermoplastic splint. Radiographs were taken at a standardized timepoint of 6 weeks after the operation, with a return to normal activities in a graded fashion if union or progression to union was noted.
For this study, following procurement of institutional ethics approval, records of all patients who had received intramedullary screw fixation of proximal phalangeal fractures under the care of the 2 surgeons in the 38-month period between January 2020 and March 2023 were obtained from a prospectively maintained database. Patient details were identified via the computerized medical records systems of both public and private institutions.
Patients were eligible for inclusion if they received intramedullary fixation of at least 1 proximal phalanx fracture; were at least 6 months after the operation at follow-up; and consented to receiving telehealth surveys and providing clinical photographs for measurement.
Demographic information, fracture characteristics, and fixation approach were collated from the medical records. Union was determined by the treating surgeon based on crossing trabeculations at the fracture site on radiographs, and a lack of pain or crepitus on clinical examination. A telehealth interview was conducted to assess patient satisfaction, the presence of complications, return to normal function and work, and outcome measures in the form of a Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) and a pain visual analogue scale (VAS). Patients also provided clinical photos of the sagittal profile of the affected digit in full flexion and extension, from which total active motion (TAM) of that digit was calculated (Angles in Photo, Kubilay Erdogan, Munich, Germany). Total active motion is used as defined by the American Society for Surgery of the Hand as the sum of active motion of the metacarpophalangeal and interphalangeal joints of a digit and can be compared with a norm of 260°. 12 Simple statistical analysis was performed where appropriate. 13 T tests (2 variables) and analysis of variance (3 variables) were used to determine P values.
Results
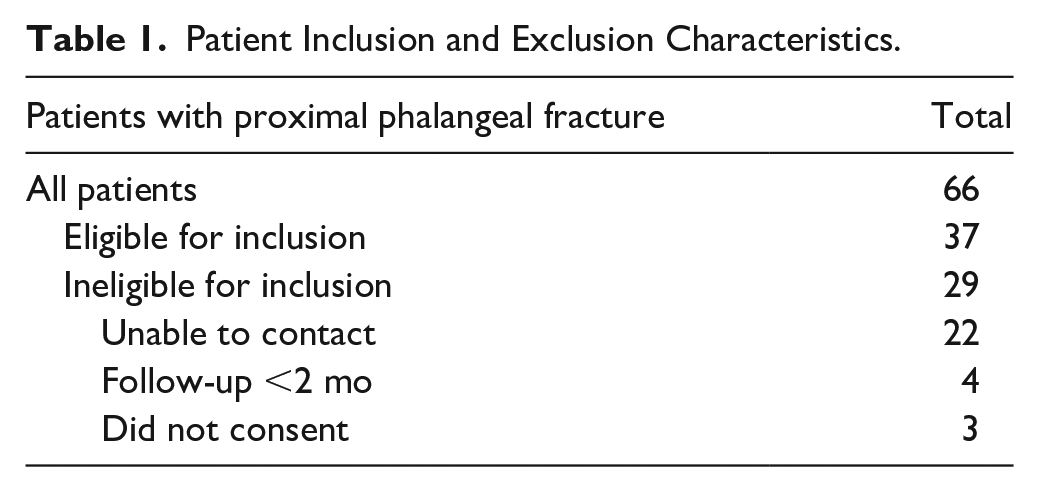
Sixty-six patients were identified from the database, with 37 eligible for inclusion (refer Table 1). Thirty-one patients sustained a single fracture; the remainder had involvements of multiple digits, resulting in a cohort of 46 digits (refer Table 2).
Patient Inclusion and Exclusion Characteristics.
Patient and Fracture Demographics.
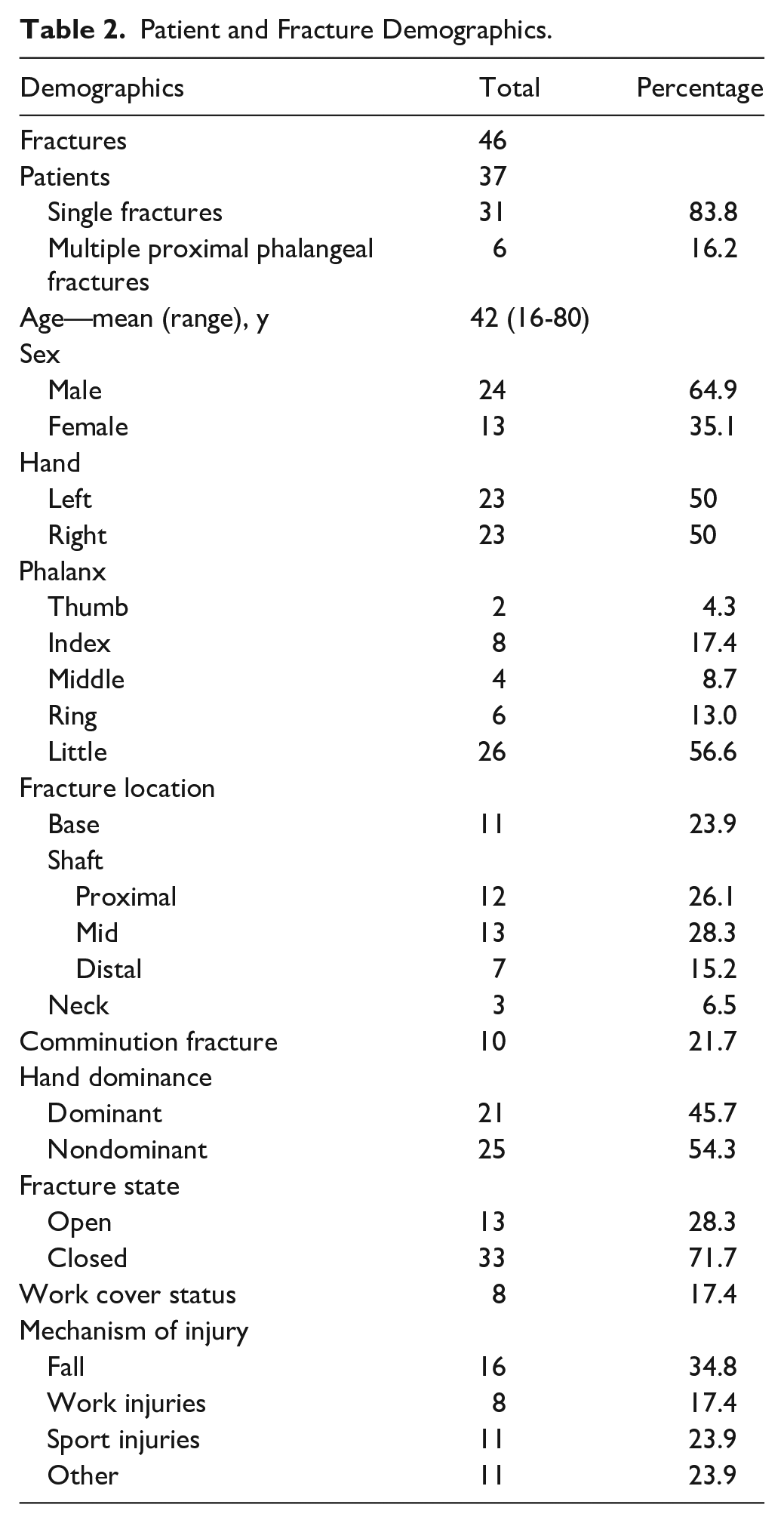
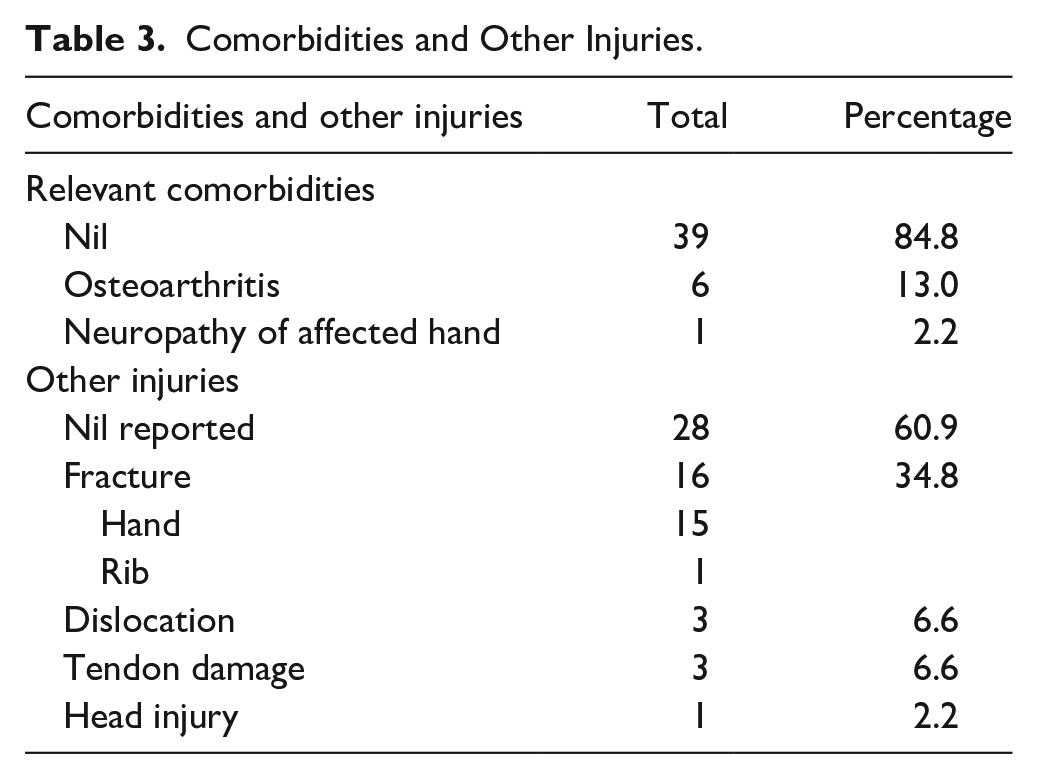
Most patients were men, with a mean age of 42 years (16-80) at the time of injury. Sixteen fractures occurred following a fall from standing height; 6 fractures were sustained during work and were covered by workers’ compensation insurance. The most frequently involved digit was the little (57%), followed by the index (17%) (refer Table 2). Roughly three-quarters of the cohort were closed injuries, and although most fractures were isolated in nature, some patients had tendon or neurovascular damage, or concomitant fractures (refer Table 3). Thirty-two fractures were stabilized through intramedullary screws inserted retrograde; the remainder were inserted antegrade transarticular (3) or intra-articular (11) (refer Figure 1).
Comorbidities and Other Injuries.

Approaches: retrograde intra-articular (32/46; 69.6%), antegrade intra-articular (11/46; 23.9%), and antegrade transarticular (3/46; 6.5%).
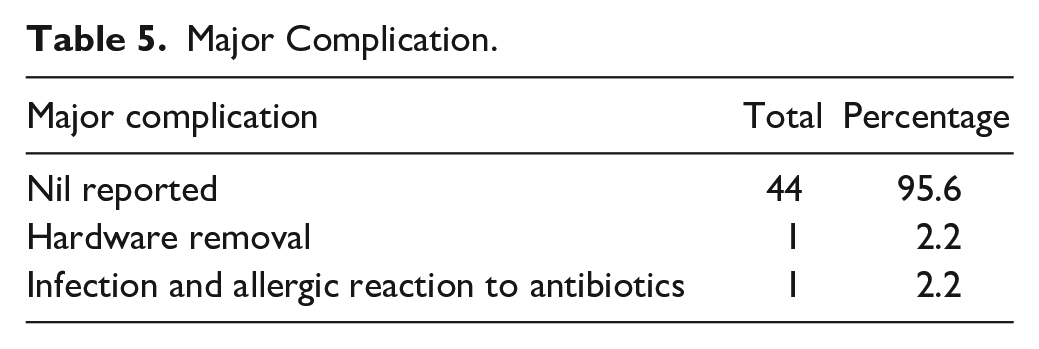
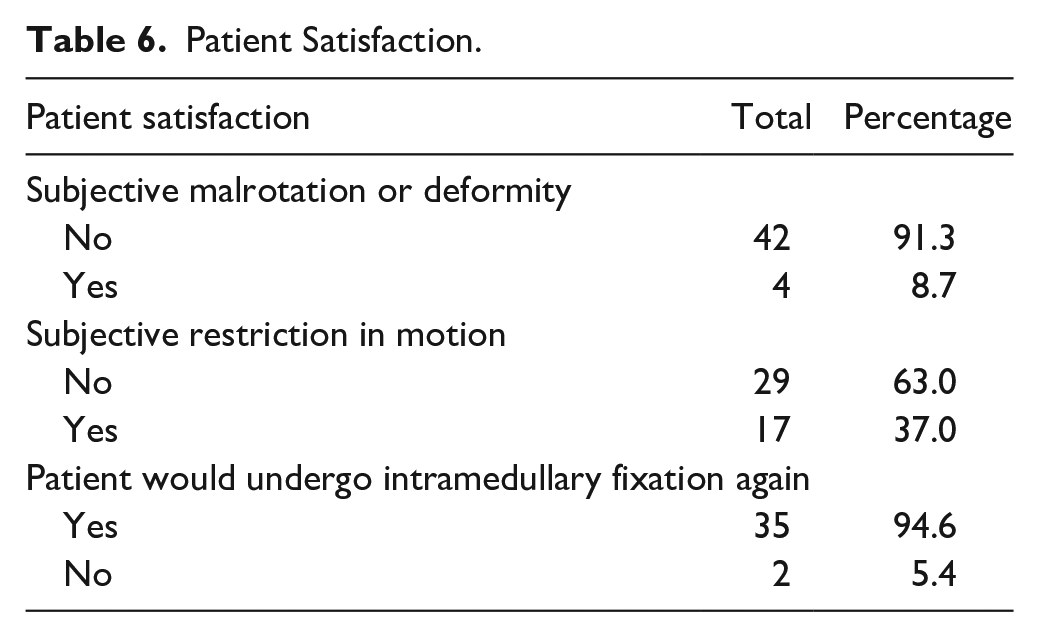
Mean follow-up was 79 weeks (28-183). All patients were noted to have united or progressing toward union (as evidenced by crossing trabeculation at the fracture site) on the 6-week postoperative radiograph. Patients returned to work at an average of 7 weeks (0-26), and full function at 14 weeks (2-46). At follow-up, mean QuickDASH was 6.2 (0-61.4; median: 0), while mean pain VAS score was 1.8 (1-7; median: 1) (refer Table 4). One patient developed an infection requiring debridement, whilst another required hardware removal, yielding a complication rate of 4.4% (refer Table 5). Thirty-five patients reported willingness to undergo intramedullary screw fixation again, resulting in a 94.6% patient satisfaction rate (refer Table 6).
Outcomes.

Note. QuickDASH = Quick Disabilities of the Arm, Shoulder, and Hand; VAS = visual analogue scale.
Major Complication.
Patient Satisfaction.
Twenty-nine patients provided clinical photographs of 33 phalanges for TAM assessment. Mean TAM in the lesser digits was 233° (132-282), while TAM for the thumb was 105° (81-129) (refer Supplemental Table 1).
One patient had a particularly poor outcome—after sustaining 2 open proximal phalangeal fractures with tendon damage in a workplace injury, he developed an infection requiring debridement and endured an allergic reaction to his antibiotic therapy. This patient reported a QuickDASH of 61.4, with calculated TAM of 145° and 166° for each digit—when excluded, the mean QuickDASH for the remainder of the cohort was 3.8 (0-29.6), mean pain VAS was 1.69 (1-7), and the mean TAM was 236° (132-282).
Subanalysis revealed that closed fractures had significantly improved outcomes when compared with open fractures in mean return to work (6 cf 11 weeks, P = .009), return to full function (12 cf 22 weeks, P = .006), QuickDASH (3.49 cf 13.44, P = .023), and TAM (241° cf 206°, P = .017). Similarly, patients sustaining single fractures reported superior outcomes than those suffering from multiple proximal phalangeal injuries, for return to work (5 cf 12 weeks, P = .001), QuickDASH (3.5 cf 12.1, P = .043), pain VAS (1.35 cf 2.87, P = .006), and TAM (238° cf 211°, P = .070). Mean QuickDASH was significantly poorer in patients whose injuries were covered by workers’ compensation insurance than those that were not (15.91 cf 4.28, P = .026). No difference was noted between alternate insertion routes for the intramedullary screws (refer Supplemental Table 2).
Discussion
Proximal phalangeal fractures are common, posing significant health and financial burdens to individuals and the community.2 -6 Thus, optimal management is key. Recently, operative intervention for hand fractures has increased, with Kirschner wire (K-wire) and plate fixation traditionally being the main operative modalities. 1
Kirschner wire fixation is rapid and cost-effective, requiring minimal soft tissue dissection. However, it often yields decreased construct rigidity and rotational control, and lacks compression at the fracture site. Protruding wires may cause pin site infections; those buried require another operation for removal. These limitations necessitate immobilization prior to rehabilitation, which when combined with potential extensor apparatus tethering on insertion, can cause significant stiffness. 14
Biomechanical studies and operative trends indicate that rigid fixation constructs such as plates are favorable to nonrigid alternatives.15 -17 However, technique invasiveness and soft tissue damage also influence outcomes.18,19 Although newer generation plating systems are of lower profile, limited cross-sectional area available for implant placement (due to the intimate relationship between soft tissue and bone in the proximal phalanx), and degree of soft tissue dissection required in the traditional dorsal tendon splitting approach, often causes increased scarring and diminished TAM. 9 Various approaches and plate positions have been suggested to minimize invasiveness and extensor tendon impediment, with a meta-analysis by Sivakumar finding that tendon-sparing approaches resulted in significantly greater TAM (8.5°; 95% confidence interval, 0.8-16.4, P = .03) than a tendon-splitting approach. 9
Recently, intramedullary screw fixation has been advocated to address concerns of tendon disturbance minimization while providing sufficient stability to facilitate early mobilization. 20 Intramedullary screws can be inserted via retrograde (through a flexed proximal interphalangeal joint into the head of the proximal phalanx); intra-articular antegrade (where the proximal phalanx base is subluxated at the metacarpophalangeal joint to facilitate direct entry); and transarticular (where the screw is inserted through the metacarpal head into the base of the proximal phalanx) routes. 21
Various biomechanical and cadaveric studies have alleviated concerns surrounding this technique. Ibanez found that intramedullary screw fixation provides greater construct stability and load to failure than lateral plating. 22 Vegas found that insertion of 2.8-mm screws via retrograde insertion damaged 6.2% of the articular surface of the head of cadaveric proximal phalanges, while a 4.1-mm screw affected 13.4%. 23 Retrograde insertion also preserved the central slip, with the tendon lesion an average of 2.7 mm wide and 4.9 mm proximal to its insertion unto the middle phalanx. 23
del Piñal assessed articular surface involvement following retrograde insertion, finding that the smallest joints had less than 18% and 25% damage with 2.5- and 3.0-mm screws, respectively. 24 Proximal articular surface lesions of the proximal phalanx (via antegrade techniques) are markedly smaller, with Borbas reporting 4.5% and 8.5% disruption when using a 2.2- or 3.0-mm screw, respectively. 25 Notably, the screws used in these studies are of relatively large diameter, while this study routinely used 2.2-mm cannulated screws.
Stern warned that the “push-up” technique for antegrade intra-articular screw insertion is technically challenging, as dorsal translation usually occurs at the fracture site and not through the joint. 26 Sivakumar recommended retrograde K-wire insertion and fracture stabilization through the proximal interphalangeal joint, prior to dorsal translation, followed by antegrade intramedullary screw insertion. 11 This facilitates screw stabilization of fairly proximal fractures without the need for transarticular insertion, broadening the indications for use of intramedullary screws.
Despite increasing popularity and adoption of this technique, outcome data are limited, particularly when considering proximal phalangeal fractures alone. del Pinal noted that intramedullary screw fixation was an effective and technically uncomplicated procedure with few drawbacks and excellent postoperative range of motion in a cohort of 19 unstable transverse proximal phalangeal fractures, as did Giesen in a larger group of 24 proximal phalanges.21,24 Aita reported a DASH score of 3.6 and VAS of 1.5 at 1 year after operation in a cohort of 41 patients with 48 fractures. 27 A systematic review by Sivakumar in 2020 found a pooled average TAM of 248° in a cohort of 77 fractures, with a 6% complication rate, mean QuickDASH of 3.6, and return to work of 9.3 weeks after an average 70.5-week follow-up. 10 More recently, Triwidodo described excellent functional and patient-reported outcomes in a small cohort of 3 fractures, while Silins reported significantly shorter durations for return to work and greatly improved postoperative range of motion in a larger cohort (29 patients with 31 fractures).28,29 Silins also observed that antegrade screw insertion from the radial or ulnar corner allowed treatment of complex juxta-articular basal fractures without violation of the articular surface. 29
This study contributes to the limited literature on intramedullary screw fixation in proximal phalangeal fractures. It finds a mean TAM of 231°, QuickDASH of 6.2, and pain VAS of 1.8 at a mean follow-up time of 79 weeks. One patient’s results were significant outliers (QuickDASH of 61.4, VAS of 6, TAM of 145° and 166°), and removing these drastically improves results of the remaining cohort. Despite this, the cohort results align with previous publications following intramedullary screw fixation in proximal phalangeal fractures and outperform most results following plate fixation, particularly via tendon splitting approaches.9,29,30 As expected, patients with multiple fractures, open injuries, and injuries covered by workers’ compensation insurance demonstrated poorer outcomes.
Although clinical outcome is the main determinant, various factors influence optimal surgical modality, such as cost-effectiveness and time-effectiveness. Sivakumar reported greater surgical durations, hardware costs, follow-up requirements, and subsequent hardware removal with plate fixation compared with intramedullary screw insertion in the Australian health care system, resulting in increased expenditure of AUD $1519.41 and AUD $1698.59 in the public and private sectors, respectively. 6 Wage losses were approximately AUD $1973.35 more when fractures were fixated by a plate, as opposed to an intramedullary screw. 6 Brewer found that despite lower hardware-associated costs, K-wire stabilization carried significantly increased outpatient follow-up costs (AUD $1826 ± $285 vs AUD $1490 ± $274) and a trend toward higher health care–related costs when compared with uncomplicated intramedullary screw fixation. 31
Sivakumar further assessed practice variation in proximal phalangeal fracture management by surveying members of the Australian Hand Surgery Society, finding that clinician experience, base specialty training, practice location, and practice volume affected decision-making. Orthopedic surgeons and less experienced surgeons were more likely to feel comfortable with, and attempt, intramedullary screw fixation. 32
This study has several limitations, including its retrospective nature, small sample size, and reliance on the initial documentation accuracy to assess demographic, injury, and surgical data. Operations from multiple surgeons, across the surgical learning curve, with varying methods of screw insertion, lead to potential confounding. Total active motion was not compared with the normal contralateral side, nor was grip strength measured. Quick Disabilities of the Arm, Shoulder, and Hand, although allowing comparison with other studies, may be affected by hand dominance. 33 Postoperative rehabilitation protocols were not detailed and may have varied between patients.
However, this study concurs with the prior literature that intramedullary screw fixation is a safe and effective method of stabilizing extra-articular proximal phalangeal fractures in the short to medium term, due to excellent clinical outcomes, and cost-effectiveness and time-effectiveness. Further long-term studies, and randomized controlled trials, are required.
Supplemental Material
sj-docx-1-han-10.1177_15589447241235339 – Supplemental material for Intramedullary Screw Fixation of Proximal Phalangeal Fractures: Short- to Medium-term Outcomes
Supplemental material, sj-docx-1-han-10.1177_15589447241235339 for Intramedullary Screw Fixation of Proximal Phalangeal Fractures: Short- to Medium-term Outcomes by Hagen Abbot, Adam R. George, Luke McCarron, David J. Graham and Brahman Sivakumar in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447241235339 – Supplemental material for Intramedullary Screw Fixation of Proximal Phalangeal Fractures: Short- to Medium-term Outcomes
Supplemental material, sj-docx-2-han-10.1177_15589447241235339 for Intramedullary Screw Fixation of Proximal Phalangeal Fractures: Short- to Medium-term Outcomes by Hagen Abbot, Adam R. George, Luke McCarron, David J. Graham and Brahman Sivakumar in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5).
Statement of Informed Consent
Informed consent was obtained from all patients for being included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.