
Abstract
Acquired arteriovenous fistula (AVF) in the hand can occur after trauma, fracture, or surgery. It is a rare condition, and only a few cases have been reported in the literature. Clinically they appear as palpable or painful lesions that persist long after the local hematoma has resolved. We report a case of a young patient presenting with long-standing and invalidating pain of the hand caused by a post-traumatic AVF, treated with percutaneous endovascular laser ablation.
Keywords
Introduction
Post-traumatic arteriovenous fistula (AVF) is a rare condition. It is usually caused by vessel injury from sharp and penetrating objects or after bone fracture. Iatrogenic fistulas are also described after surgery, finger transplantation, or catheterization.1 -3 They are associated with an inexplicable pain lasting long after resolution of the local injury, and often irradiating proximally because of venous pressure overload. We report here the case of a young patient with post-traumatic AVF who was referred to our department because of a persistent and invalidating pain in the upper limb.
Case Report
A 14-year-old left-handed female patient presented with a hematoma on the palmar side of her dominant hand after playing handball at school. After 2 weeks, the bruise completely disappeared leaving a persistent pain localized at the mid-metacarpal and radiating into the third and fourth fingers as well as back up to the elbow. Clinically there was no edema, no palpable mass, no pulsatility, but a small vascular superficial network 3-cm wide at the center of the mid-metacarpal and an asymmetrical enlargement of hand dorsal veins (Figure 1).
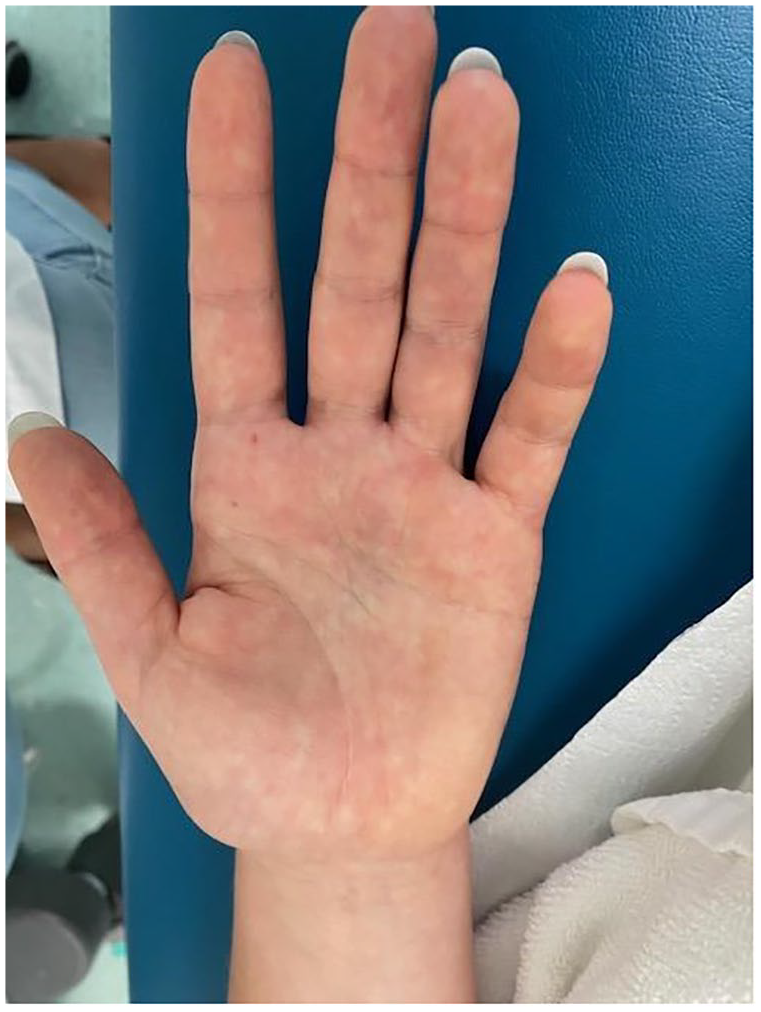
Slightly visible bluish discoloration of the palmar side of the distal carpus.
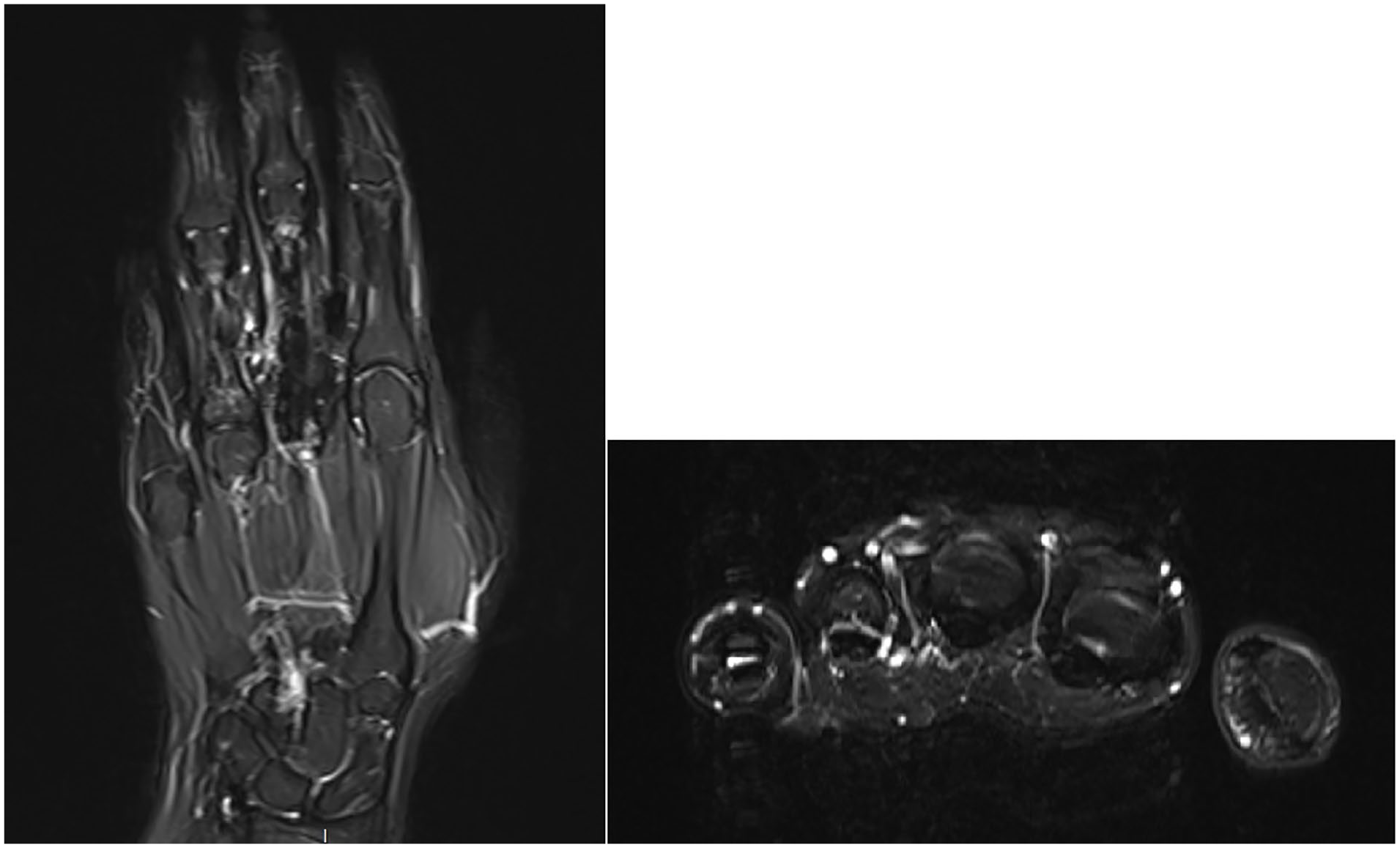
After 1 month of clinical follow-up, she reported worsening of symptoms. Magnetic resonance imaging (MRI) showed an enlarged aspect of both palmar and dorsal venous systems, with a fast venous network enhancement in the arterial phase, consistent with an AVF (Figure 2).
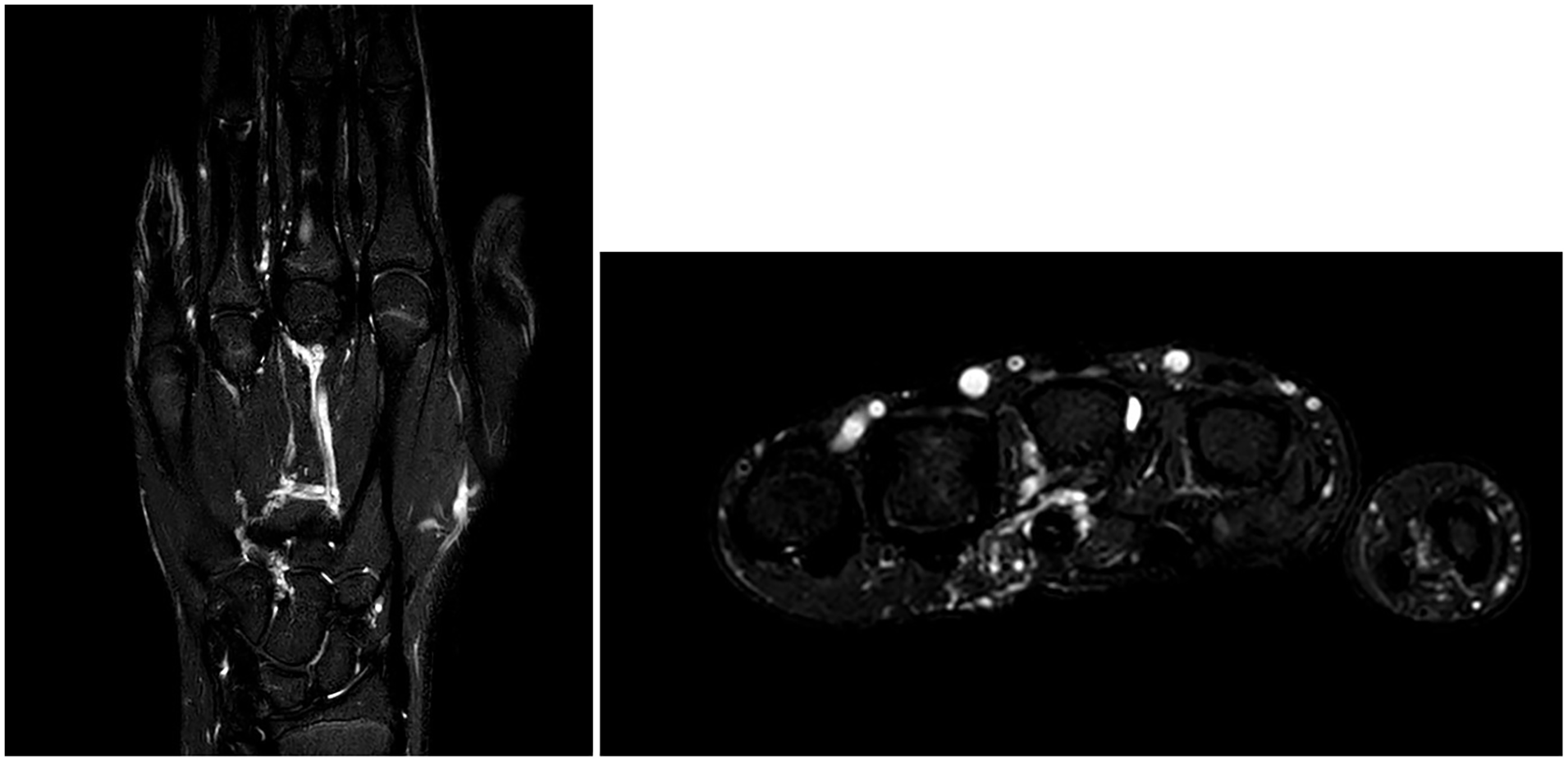
Preoperative T2-phase magnetic resonance imaging, showing simultaneous enhancement of the common digital artery and vein and enlargement of a deep and superficial venous network.
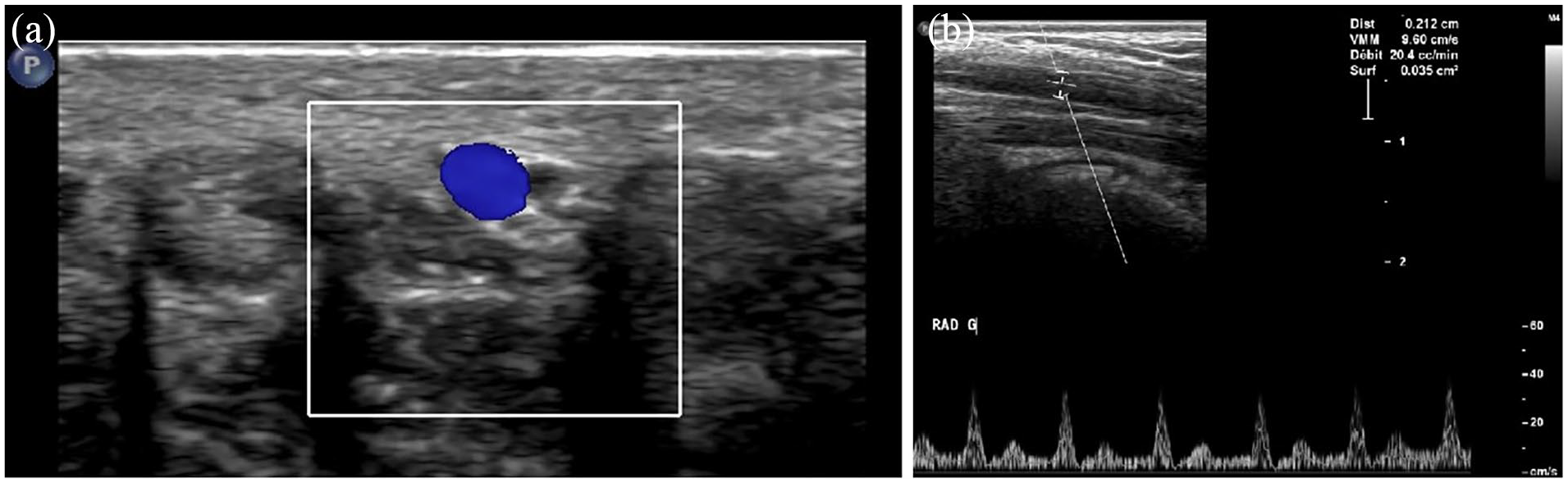
An accurate Doppler ultrasound revealed a typical anatomy of the arterial system and a small AVF connecting the third common digital artery with one of its satellite veins, thus nourishing a pulsatile and enlarged venous network in the carpus. At the site of the fistula, the artery was measuring 2.00 mm in diameter, the vein 1.20 mm, and the connection was only visible by the color Doppler aliasing phenomenon, but too small to be measurable in size. Arterial inflow to the hand, calculated as the sum of the radial plus the ulnar flow, was 82 mL/min compared with 65 mL/min on the right hand (Figure 3).
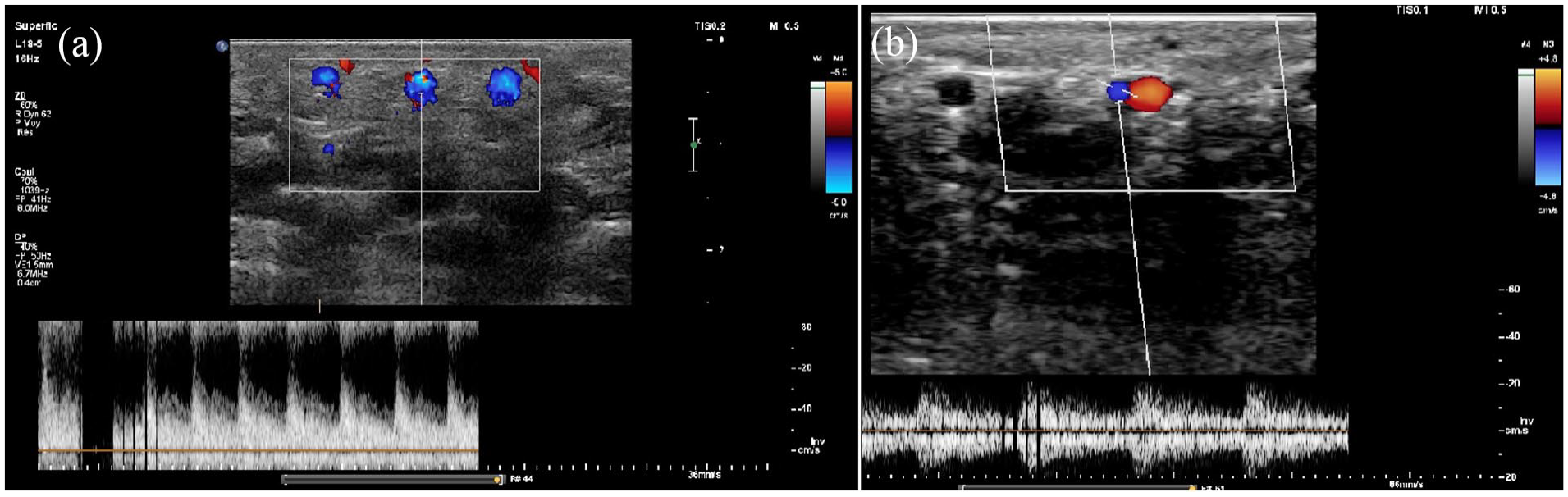
Color Doppler ultrasound assessment of the fistula: (a) low-resistance flow pattern in the involved digital artery and (b) fistula with a pulsatile flow into the common digital satellite vein.
Due to the small entity of the AV connection, we first opted for a conservative approach, prescribing a compressive custom-made glove that offered some pain relief at first, but soon became ineffective.
After 2 months, despite the compression glove, the pain was invalidating, present day and night, nonresponsive to systemic painkillers, and the arterial inflow to the hand increased to 176 mL/min.
After a multidisciplinary discussion involving angiologists, interventional radiologists, and hand surgeons, a minimally invasive approach with a thermal endovascular laser ablation was proposed to the patient and her parents, keeping the surgical option as a second-line strategy. Endovascular embolization was considered not feasible due to the small AV connection and the risk for the terminal vascularization of the third and fourth fingers.
Under loco-regional anesthesia, a ultrasound-guided percutaneous puncture of the digital vein approximately 1 cm distally to the fistula was performed with a 16G catheter (BD Venflon Pro), thus obtaining a venous drawback. A 1940-nm wavelength laser delivered by a 400-nm radial fiber (LSO Medical, Loos, France) was inserted through the catheter into the vein up to 1 cm proximally to the fistula (Figure 4).
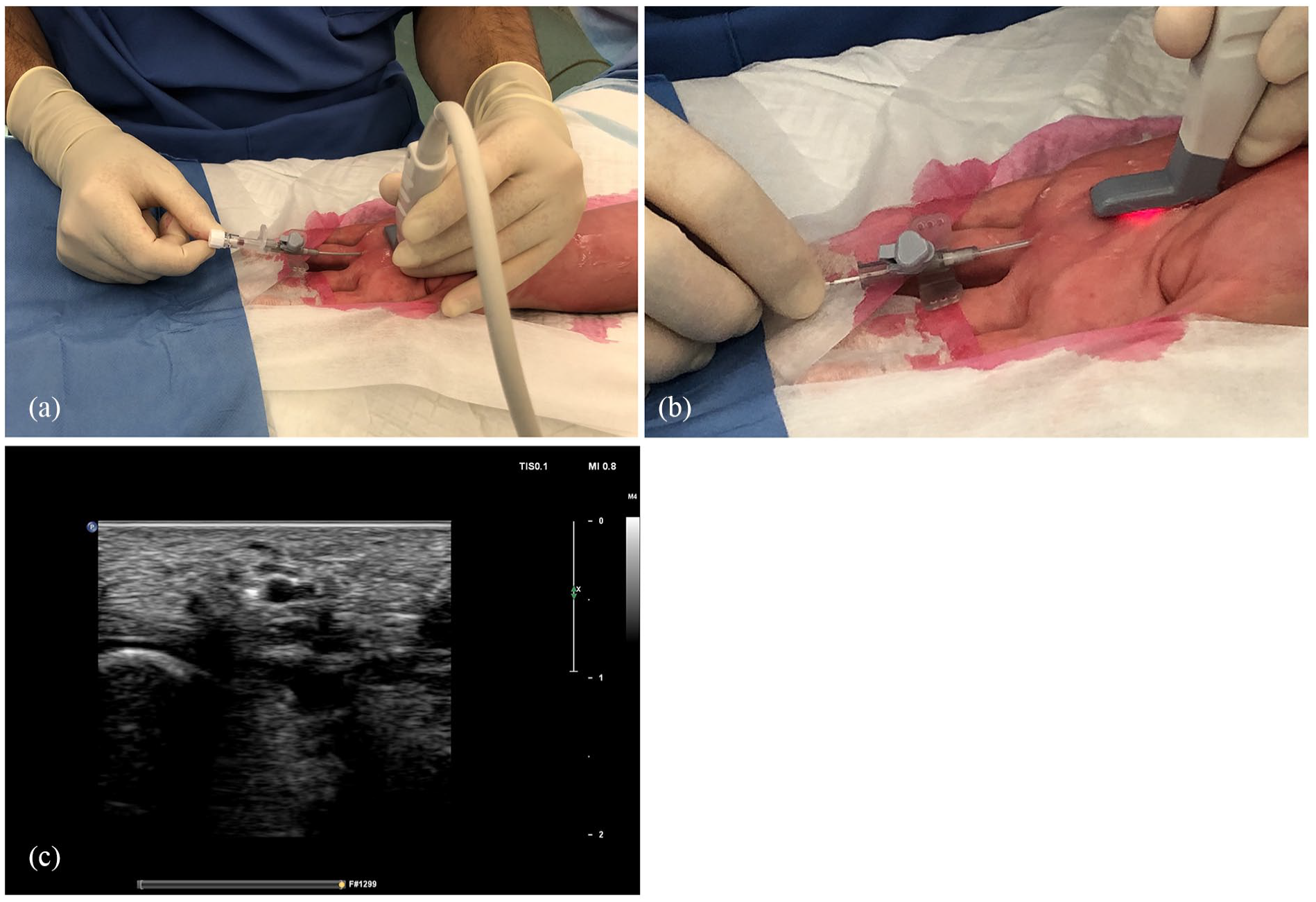
(a) Percutaneous ultrasound-guided cannulation of the common digital vein, obtaining a drawback and (b) insertion of the optic fiber, (c) whose advancement and position are confirmed under ultrasonography.
A total of 3 mL of tumescent anesthesia (100 mL of 0.9% NaCl with 8 mL lidocaine 1%/epinephrine 10 μg/mL and 1 mL of sodium bicarbonate 8.4%) was then injected around the vein to obtain a sufficient separation from the digital artery and create a venous spasm around the laser fiber.
To adjust the power in such a small vessel, the thermal ablation was performed under continuous ultrasound guidance with a power of 1.5 W, with a total energy of 65 J delivered over 2 cm.
Immediate result was satisfying, with a patent artery and a normal vascularization of the finger. The procedure lasted 45 minutes.
At days 1 and 7 postoperatively, we found no neurological complication, no hematoma, and no finger flow impairment. The patient reported complete resolution of symptoms within 3 days. Ultrasound showed a sclerosis of the treated vein, disappearance of the AVF, and a patent common digital artery, with a normalization of the flow pattern and of the cumulated radial and cubital flow that came back to a normal value of 40 mL/min, symmetrical to the right side (Figure 5).
Ultrasound showing (a) disappearance of the treated vein, and patency of the artery, (b) with normalization of the flow pattern.
The MRI at 3 months showed a normal vascularization of the hand, with no sign of AVF (Figure 6). During the next 24 months of clinical follow-up, the patient remained asymptomatic.
Three-month magnetic resonance imaging control that shows a normal vascularization of the hand, without early venous enhancement or enlargement.
Discussion
Blunt or penetrating trauma of the upper limb can result in vascular injuries. Diagnosis is made by clinical evaluation, color Doppler ultrasound, and MRI.1 -6 Clinical presentation varies from asymptomatic and self-resolving lesions to more severe conditions. These include the development of an AVF of the injured vessel that can be responsible of pain, venous insufficiency, and dilatation of the feeding artery or the surrounding veins and potentially evolve in heart failure.
If the AVF is small enough, it can disappear spontaneously over time. 4 There are only few reports of such acquired AVFs in the literature. The rationale of treatment lies in the interruption on the connection between the artery and the vein. Surgery is the oldest described technique.7 -10 The challenge of an open surgical approach resides in the difficulty of a precise location of the AV connection, resulting in wide dissection of deep tissues and scarring sequelae. The endovascular approach aims to occlude the AV connection or the feeding artery using embolic agents or devices. 11 In the hand, this approach clashes with anatomical limitations in terms of sacrifice of distal terminal arteries.
Laser treatment techniques are routinely used in the vascular field, especially for varicose veins, vascular tumors, and malformations.12,13 An optic fiber is inserted percutaneously in the vessel and delivers an amplified light energy which is absorbed by the vascular wall, cauterizing it. Its limitation consists in the diameter of the fiber that has to be inserted in the target vessel through a catheter of at least 1.63 mm of diameter, rendering technically challenging a cannulation of a smaller vessel. This technique requires a trained vascular specialist and a proficient use of the ultrasound. We found a similar case of employment of this technique in the foot, 14 but no previous report in the upper limb exists.
A case-by-case meticulous analysis of the vascular anatomy is essential.15,16 We planned a thermal ablation of the digital vein in the mid-metacarpal, at the level of the arterial connection, presuming that cauterizing the vein would be sufficient to resolve the AVF, sparing the artery.
In fact, the vein measured 1.20 mm, without dilatation under loco-regional anesthesia nor under proximal tourniquet, but an ultrasound-guided cannulation with a 16G Venflon (Becton Dickinson, Franklin Lakes, New Jersey, United States) was achieved and inserting the laser fiber was not difficult. The ultrasound-guided injected tumescent anesthesia separates the fiber from the artery and other surrounding tissues, thus absorbing the laser energy and avoiding thermal injury beyond the vein wall.
Apart from technical aspects discussed above, there are no clear inclusion or exclusion criteria for this technique, but an accurate damage risk analysis of the arterial circulation must be assessed. Potential risks could be digital ischemia, hematoma, skin burn, and neurological impairment.
Conclusion
The diagnosis and follow-up of post-traumatic AVF should be done in experienced vascular centers. Most of these conditions are self-resolving. The color Doppler ultrasound is the cornerstone technique of imaging, offering the possibility of a precise monitoring of the blood flow rate over time.
Multiple considerations as the location of the AVF, the vascular anatomy, the size of the AV connection, and the flow rate should guide the choice of treatment, that is, mostly surgical or endovascular. Percutaneous laser ablation, however, is a minimally invasive technique that offers precision and may represent an option in selected cases.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from the patient included in the study and her family.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.