
Abstract
Background:
Between 2014 and 2020, candidates for scaphoid non-union (SNU) surgery were enrolled in a prospective randomized trial (Scaphoid Nonunion and Low Intensity Pulsed Ultrasound [SNAPU] trial) evaluating the effect of low-intensity pulsed ultrasound on postoperative scaphoid healing. At trial completion, 114/134 (85%) of these patients went on to union, and 20/134 (15%) went on to persistent SNU (PSNU). The purpose of this study was to use this prospectively gathered data to identify patient-, fracture-, and surgery-specific risk factors that may be predictive of PSNU in patients who undergo surgery for SNU.
Methods:
Data were extracted from the SNAPU trial database. The inclusion and exclusion criteria of this study were the same as that of the SNAPU trial. Nineteen patient-, fracture-, and surgery-specific risk factors were determined a priori. A stepwise multivariable logistic regression model was used to identify independent risk factors for PSNU.
Results:
Three risk factors were found to be independently significant predictors of PSNU: age at the time of surgery, dominant hand injury, and previous surgery on the affected scaphoid. With every decade of a patient’s life, dominant hand injury, and previous scaphoid surgery, the odds of union are reduced by 1.72 times, 7.35 times, and 4.24 times, respectively.
Conclusion:
We identified three independent risk factors for PSNU: age at SNU surgery, dominant hand injury, and previous surgery on the affected scaphoid. The findings of this study are significant and may contribute to shared decision-making and prognostication between the patient, surgeon, and affiliated members of their care team.
Introduction
The scaphoid is the most commonly fractured of the 8 carpal bones found in the wrist. It is unique in its retrograde blood supply and curving structure, deriving its name from skaphos, the Greek word for “boat.” 1 Scaphoid fractures predominantly occur in active males aged 10 to 19 years.2-4 They typically occur following a blow to the wrist via a fall on an outstretched hand, motor vehicle accident, injury in contact sports, or when an individual punches with a neutral or slightly flexed wrist.5,6 The scaphoid is commonly fractured at the waist (65%), followed by the proximal third (25%), and the distal third (5%-10%). 7 Its blood supply is mostly derived from the dorsal carpal branch of the radial artery, making proximal pole and displaced fractures vulnerable to avascular necrosis.2,3
Despite a myriad of treatment options including electrical stimulation, cast immobilization, and surgical fixation, scaphoid fractures have an established non-union rate ranging between 5% and 15%.8,9 Although its cause is not always known, scaphoid non-union (SNU) is a concerning outcome that can cause ongoing pain, altered wrist kinematics, diminished range of motion, and degenerative changes including SNU advanced collapse.2,10-13 The most cited risk factors for SNU include degree of fracture displacement and comminution, female sex, smoking/nicotine use, regular manual labor, proximal pole fracture, presence of avascular necrosis, delayed diagnosis, and delayed time to treatment.10,12-17 This significant morbidity following SNU is of concern, particularly when we consider the young demographic who may experience high-cost implications associated with early disability.
Although many scaphoid fractures are treated non-operatively with immobilization, operative treatment is often warranted for displaced fractures and provides the benefit of shorter immobilization time and a faster return to work. 12 There is a general trend to using screws rather than Kirschner wires for fixation of scaphoid fractures, with some studies reporting higher union rates with screw use.18,19 In addition, debridement of fibrous tissue and non-viable bones creates bone defects which are often filled with bone grafts. 18 Vascularized bone grafts (VBGs) have been reported to shorten immobilization time, and citing the scaphoid’s tenuous blood supply, many surgeons prefer VBG over non-vascularized structural grafts (NVSGs).3,20,21 However, evidence supporting VBG over NVSG to increase union rates is conflicted.19,20,22
Scaphoid non-unions are well-studied, and risk factors for their occurrence have been documented. Those who incur an SNU are recommended to undergo operative management.9,23 However, union rates following surgery for SNU are variable, ranging from 27% to 100%, depending on the fixation method. 19 Aside from experiencing the same ongoing risks of degenerative changes, physical disability, and mental health struggles that accompany SNU, 13 those who experience persistent SNU (PSNU) will need to undergo yet another surgery and accept its associated risks. There remains a paucity of studies determining risk factors for PSNU, and those that do exist are limited by retrospective nature and a small sample size. The purpose of this study was to identify risk factors predictive of PSNU from a large prospectively collected data set.
Materials and Methods
The Scaphoid Nonunion and Low Intensity Pulsed Ultrasound (SNAPU) multi-centered prospective randomized controlled trial was conducted through the South Campus Research Unit for Bone and Soft Tissue (SCRUBS) at the University of Calgary (Calgary, Alberta, Canada). This trial enrolled and randomized 151 surgical patients between 2014 and 2020 to determine the effectiveness of pulsed ultrasound postoperatively to improve healing rates and time to union in patients who have undergone surgery for an established SNU. Low-intensity pulsed ultrasound (LIPUS) was self-administered by patients for 20 minutes daily via visually identical active or sham Exogen 4000 (Bioventus, Durham, North Carolina, United States) LIPUS units. Treatment began at the subjects’ 2-week postoperative follow-up appointment. The LIPUS device was applied directly over the fracture site through a window in the cast. Treatment ceased once the fracture was deemed to be united on computed tomography (CT) with multiplanar reconstruction (>50% total trabecular bridging) or a persistent non-union after a minimum of 4 months of treatment. If union was not determined on CT with multiplanar reconstruction, non-union status was ultimately determined by the treating surgeon based on symptoms in combination with imaging. All non-unions were critically assessed over time for the purposes of this study. If the non-union status was not clear, these patients were considered unknown and excluded from this study. Following treatment end, the LIPUS devices were returned to Bioventus for data extraction, which included compliance. At trial close, 134 patients had completed data sets and known union status. Twenty (15%) of these patients went on to have PSNU. Using the prospectively collected data from these same patients, there was an opportunity to determine risk factors for PSNU in those who have undergone a surgery for an SNU.
Data were extracted from the SNAPU trial in the University of Calgary’s REDCap database. Ethics approval for this trial was granted by the University of Calgary’s Conjoint Health Research Ethics Board (CHREB) (REB13-0849). As these data were from the prospectively collected SNAPU data, the inclusion and exclusion criteria of this study were the same as those of SNAPU (Table 1). Nineteen a priori risk factors were determined from a literature review in combination with the expertise of all co-authors (Table 2). A total of 293 patients were screened for eligibility, and 173 were found to be eligible and were enrolled in the trial. Twenty-two patients withdrew before randomization, leaving 151 to be randomized. A further 9 patients withdrew from the trial, resulting in a total of 142 patients included in the final analysis. At the trial’s end, union status of 8 patients (6%) was unknown, 114 (80%) were found to be united, and 20 (14%) experienced a PSNU (Figure 1). The average age of the patients at the time of surgery was 27 years.
Inclusion and Exclusion Criteria for the SNAPU Trial.
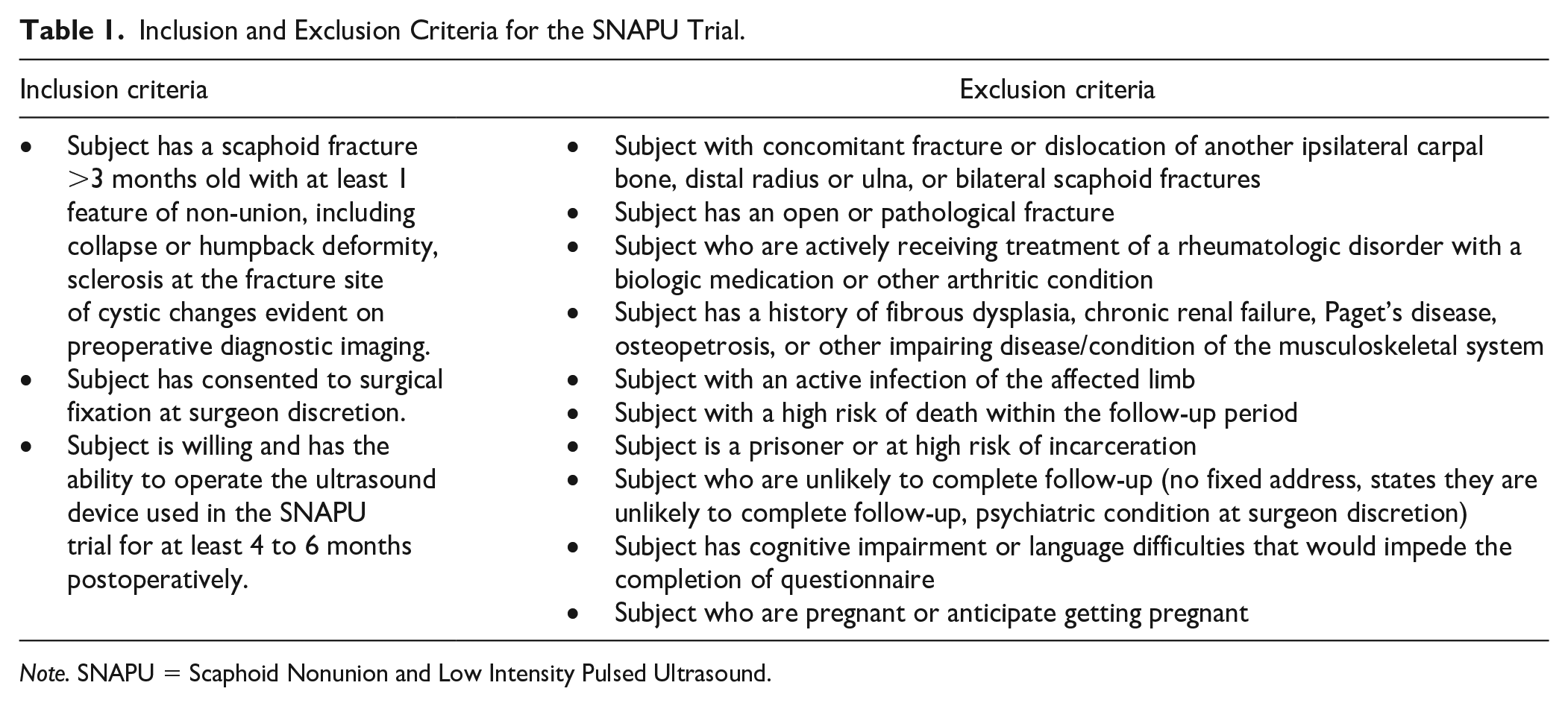
Note. SNAPU = Scaphoid Nonunion and Low Intensity Pulsed Ultrasound.
A Priori Risk Factors Analyzed.
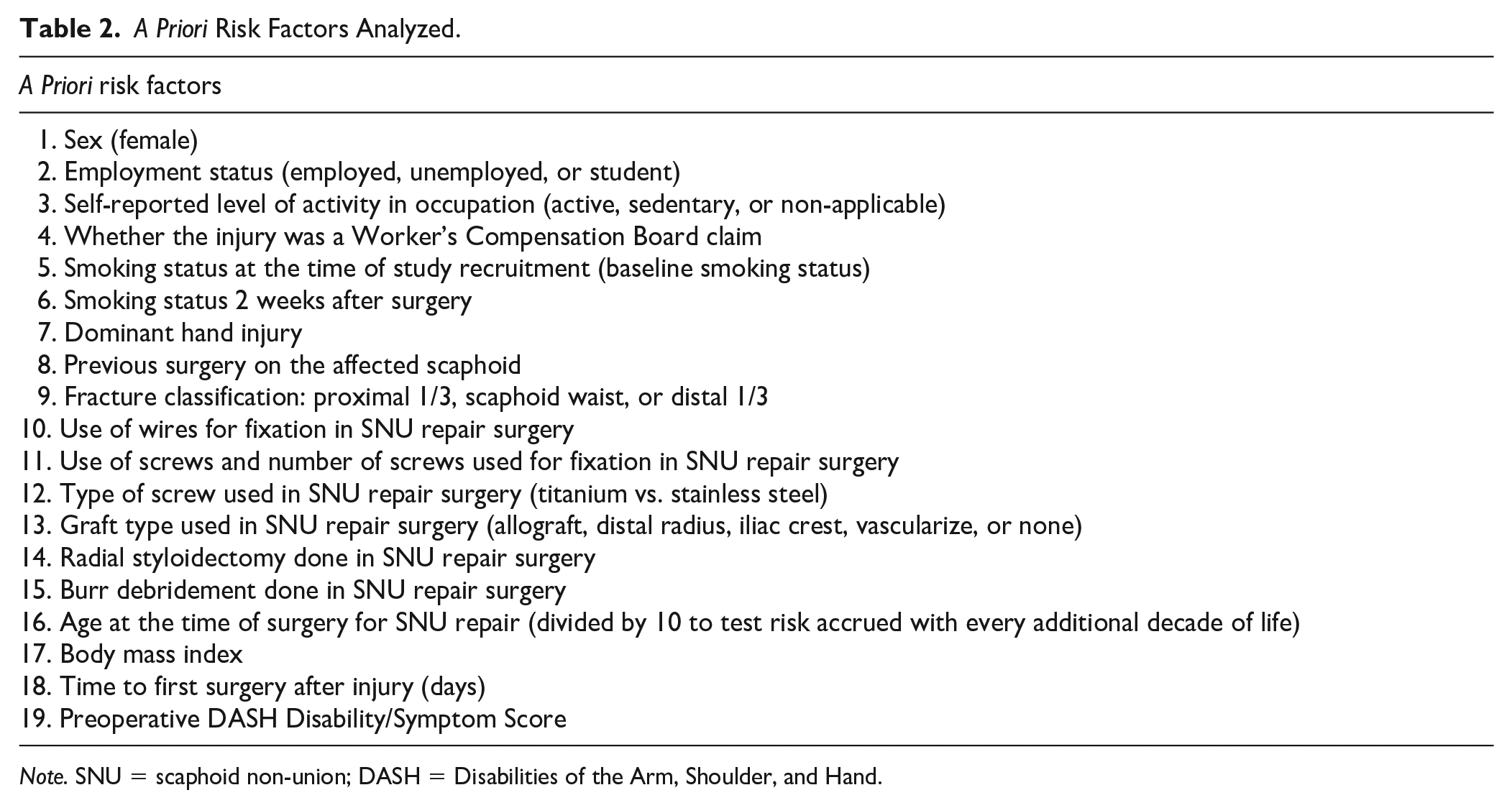
Note. SNU = scaphoid non-union; DASH = Disabilities of the Arm, Shoulder, and Hand.
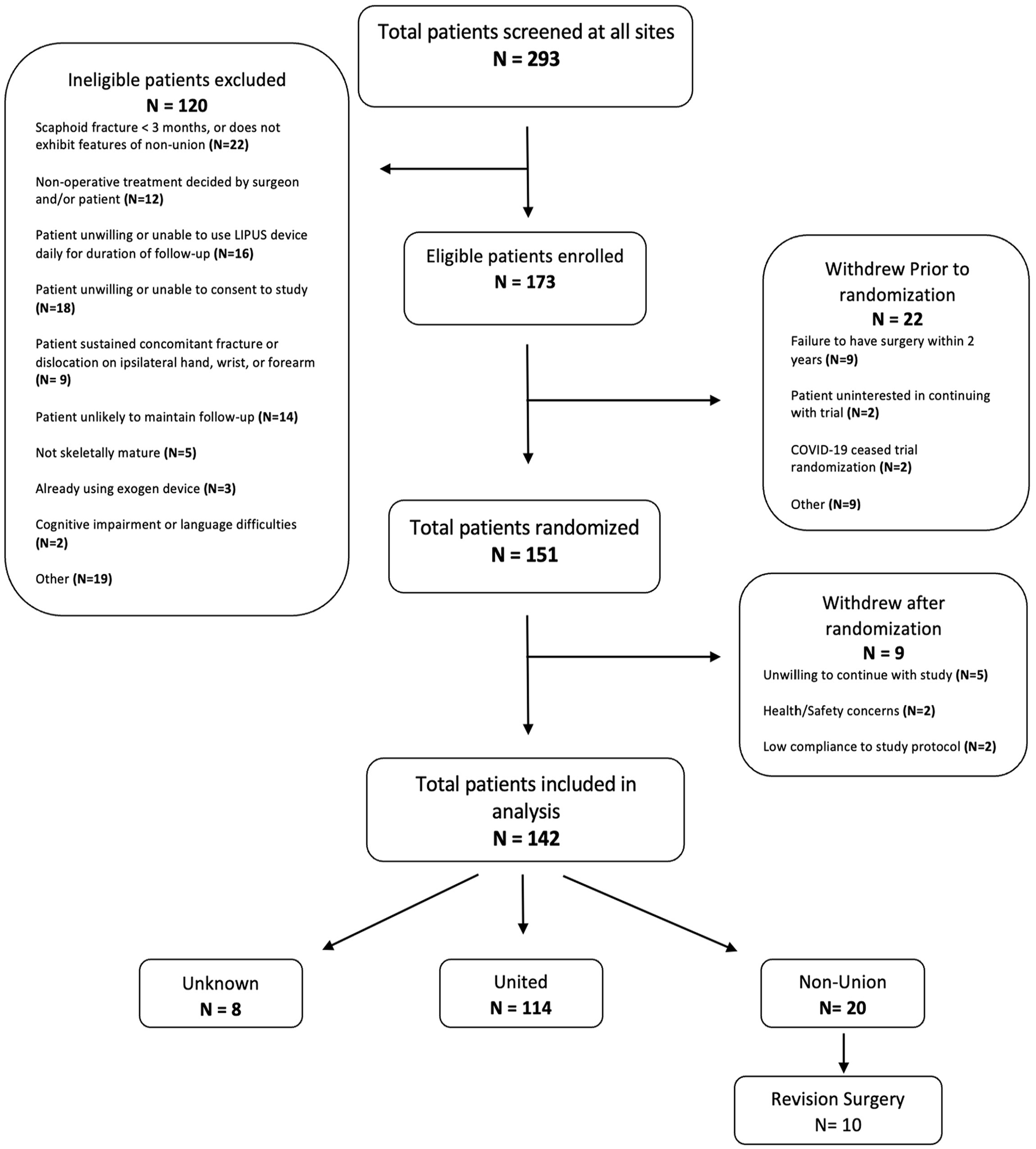
Patient recruitment for the Scaphoid Nonunion and Low Intensity Pulsed Ultrasound (SNAPU) trial.
Diagnosis and Classification of Scaphoid Fractures
Established SNUs were diagnosed by fellowshipped hand surgeons using radiograph and CT scans. Fractures were classified into: distal one-third, proximal one-third, or scaphoid waist. Following enrollment into the SNAPU trial and surgical treatment, both an orthopedic surgeon and a musculoskeletal (MSK) radiologist separately diagnosed the union status on serial CT scans. If the two physicians’ diagnoses were incongruent, a discrepancy was declared. The discrepant cases were sent for evaluation to an independent adjudication committee consisting of 3 members: 2 MSK radiologists and 1 orthopedic surgeon. None of the investigators in this process had any direct involvement in the trial. To reduce bias and improve accuracy, the committee was blind to the previous incongruent interpretation made by both the radiologist and treating surgeon.
Data Analysis
After extraction from the SNAPU trial database, risk factors were analyzed for significant differences between union/nonunion groups using χ2 tests for categorical variables, which included employment status, active or sedentary employment, Worker’s Compensation Board claim, baseline smoking status, smoking status at the time of surgery, dominant hand injury, previous scaphoid surgery, fracture location, use of wires, use of screws, type of screws (if they were used), graft type, intraoperative radial styloidectomy, and intraoperative burr debridement. When determining smoking status at the time of surgery, we used data from a survey completed at the subject’s 2-week postoperative visit. If a patient declared that they continued to smoke cigarettes, they were identified as an active smoker at the time of surgery. Wilcoxon rank-sum tests were used to test for group-wise differences in continuous variables, including age at the time of surgery, body mass index (BMI), days between date of injury and date of surgery, and preoperative Disabilities of Arm, Shoulder, and Hand (DASH) score. We were unable to calculate a preoperative DASH score for 2 (10%) of those in the non-union group and 7 (6%) of those in the union group.
After determining the significance of each individual variable in univariable analyses, those with P < .10 were included in a further stepwise-selected multivariable logistic model to select, at alpha = 0.05, a parsimonious model containing variables independently predictive of non-union (Tables 3 and 4). Subsequently, those variables that emerged from the stepwise model with P < .05 were considered significant and deemed independent risk factors for PSNU (Table 5).
Categorical Variable Risk Factors After Univariable Analysis.
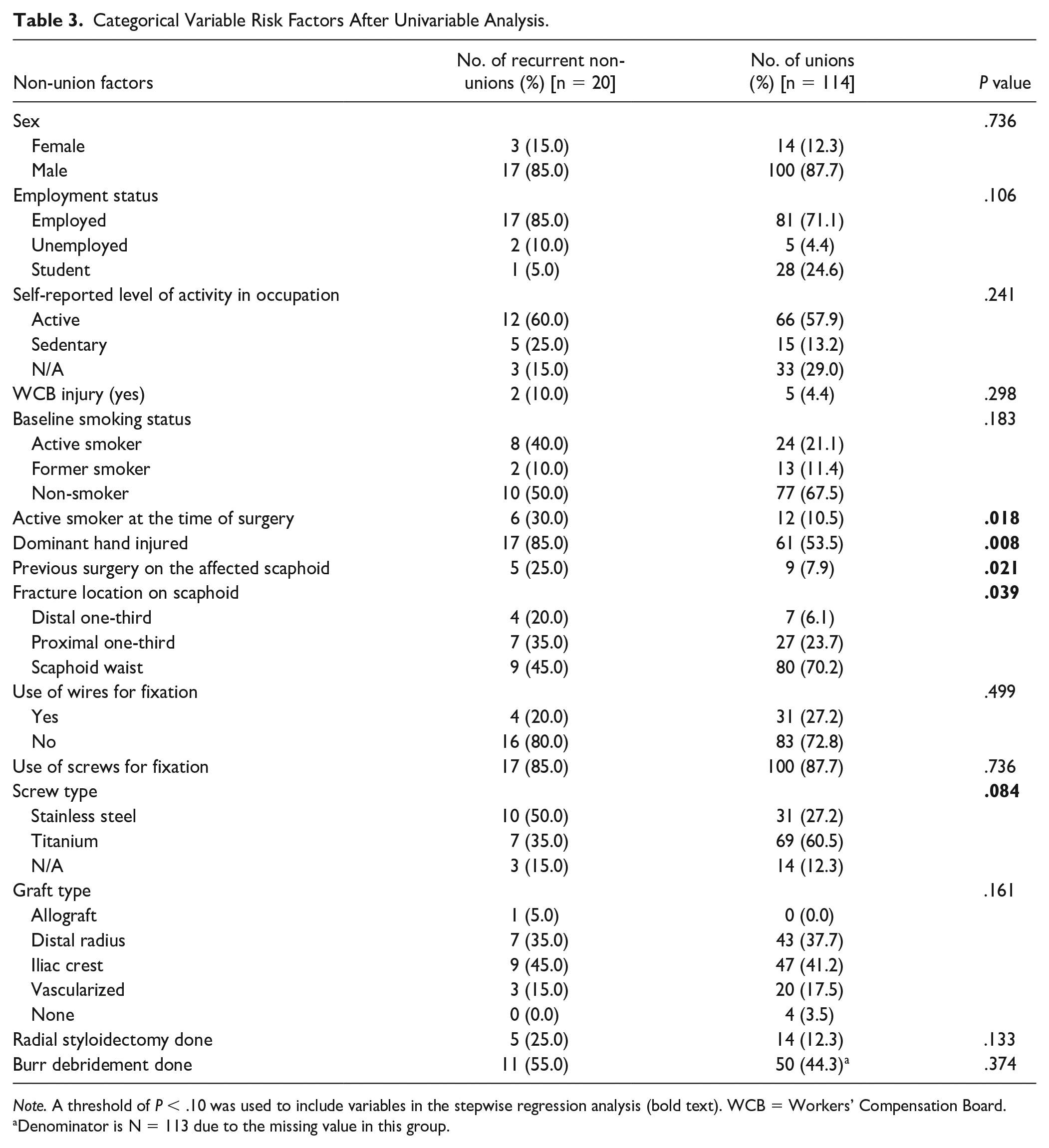
Note. A threshold of P < .10 was used to include variables in the stepwise regression analysis (bold text). WCB = Workers’ Compensation Board.
Denominator is N = 113 due to the missing value in this group.
Continuous Variable Risk Factors After Univariable Analysis.
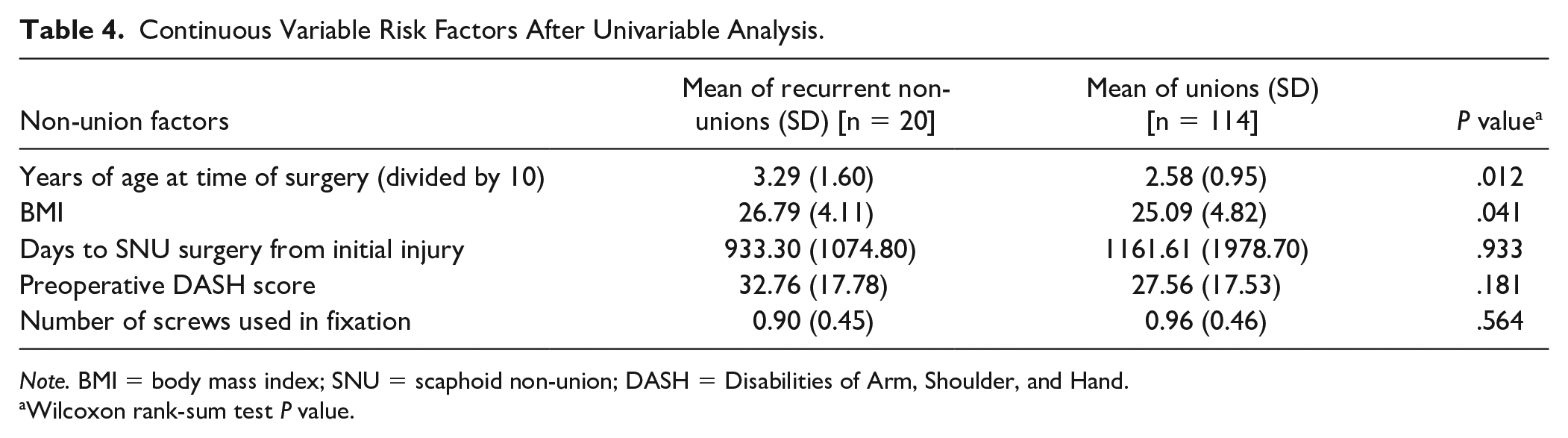
Note. BMI = body mass index; SNU = scaphoid non-union; DASH = Disabilities of Arm, Shoulder, and Hand.
Wilcoxon rank-sum test P value.
Significant Risk Factors After Regression Analysis.
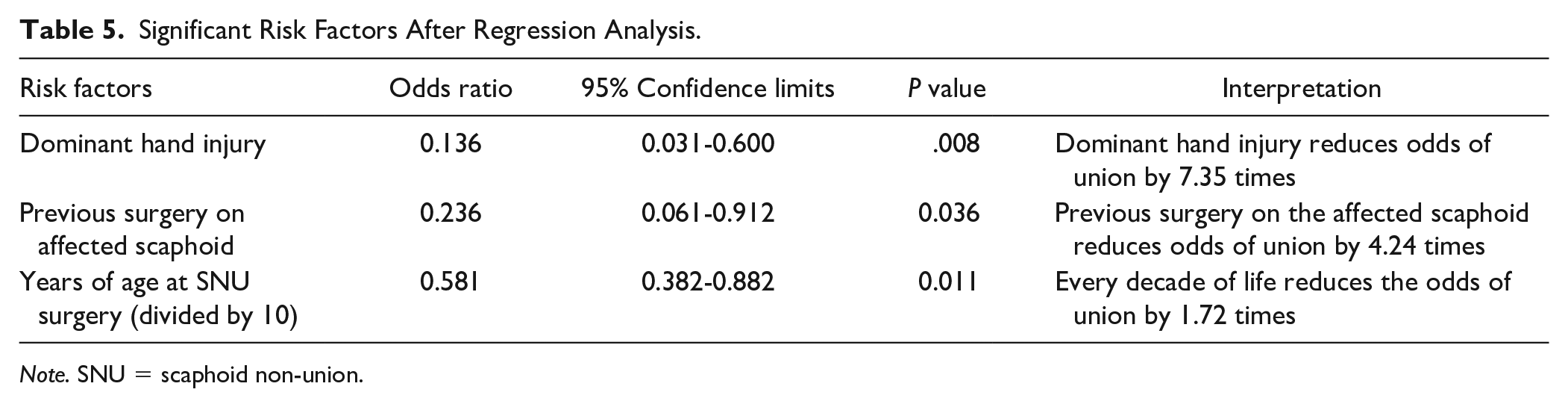
Note. SNU = scaphoid non-union.
Results
The study population (N = 134) included 117 males and 17 females. The average age at the time of surgery was 27 years. Twenty (15%) patients went on to a persistent non-union, while 114 (85%) patients united following surgery for established SNU. After an analysis of the 19 a priori risk factors, 7 (37%) were included in the multivariable regression analysis using a cutoff of P < .10 (Tables 3 and 4). These included smoking at the time of surgery (P = .02), dominant hand injury (P = .008), previous surgery on the affected scaphoid (P = .02), fracture location (P = .04), screw type (P = .08), age at time of surgery (P = .01), and BMI (P = .04). These variables were then inputted in a stepwise logistic regression analysis model at alpha = 0.05, which found that 3/7 variables were independently significant predictors of PSNU (Table 5). These three risk factors were dominant hand injury (P = .008), previous surgery on the affected scaphoid (P = .04), and increasing age (P = .01).
Discussion
This study analyzed prospectively collected data on 134 individuals from a large randomized controlled trial to identify risk factors predictive of PSNU following operative management of an established SNU. After we determined 19 a priori risk factors, our multivariable regression analysis showed that dominant hand injury reduced odds of union by 7 times, every additional decade of life reduced odds of union by 1.72 times, and previous surgery reduced the odds of union more than 4 times.
Although there is evidence to suggest older age may reduce chances of bone healing,24,25 the current literature is conflicted on age as a specific risk factor for fracture non-union. Many studies, although not focused on the scaphoid specifically, show that increased age is not an independent risk factor for fracture non-unions,26-28 while others have found the opposite, even in pediatric populations.29,30 There may be confounding variables associated with age, such as time from injury to surgery, as those who are older may have waited longer to undergo operative treatment since their initial scaphoid injury. We found that time from injury to surgery was not significant in our univariable analysis, which suggests this likely is not the case. This study also excluded other confounding variables often associated with fractures and aging, such as osteoporosis, thus making them unlikely explanations. This being said, fracture healing is a multifaceted process that can be complicated by numerous conditions and medications. Aging impairs a bone’s regenerative potential through an associated decrease in mesenchymal stem cells and impaired osteoblast differentiation. 31 Unlike most literature that compares 2 vastly different age groups’ potential for fracture healing, our study suggests that age gaps as little as 10 years can significantly alter relative union rates in scaphoid fractures.
Our finding of previous surgery increasing risk of PSNU is in direct contrast to a very recent study published by Diehm et al 32 which showed that previous surgery had no impact on the union rates following an SNU surgery. However, our study differed from theirs in a few ways. First, their study was retrospective in nature with a comparatively smaller sample size (95), which they acknowledge as a limitation of their investigation. We reviewed prospectively collected data from a 6-year period, which we believe increases the strength of our study and the generalizability of our work. Finally, the authors of the previous study acknowledge that their groups were not balanced in graft type and smoking status. In our study, of those who had a previous surgery on their scaphoid, 3/14 (21%) were smokers at the time of surgery, while 15/120 (13%) of those who had not had previous surgery on their scaphoid were smokers at the time of surgery, making the number of active smokers in our study more balanced. Overall, we believe our study complements theirs by providing a good rebuttal that encourages further research on this topic.
Dominant hand injury was the most significant risk factor for PSNU. To our knowledge, this has not been assessed in studies that have investigated risk factors for PSNU.33,34 We believe that the functional limitations imposed by injury to one’s dominant hand may explain this sevenfold increase in non-union risk. Dominant hand injuries may be at risk of overuse in the postoperative period. Considering right-handed individuals’ reliance on their dominant hand, that tasks are completed faster when using the dominant hand in both left- and right-handed individuals, and that 90% of the population is right-hand dominant, it is safe to assume that the majority of patients with a dominant hand injury will experience significant difficulty in completing activities of daily living (ADLs).35-38 If somebody lives a relatively independent life, or is eager to return to work, they may feel obligated to use their dominant hand to complete physically demanding ADLs despite pain and instructions to immobilize this hand. In addition, even if they intend to adhere to postoperative protocols including immobilization and limited activity, instinctively, a patient may be inclined to use their injured hand, for example, quick reactions such as using their hand for support when they lose their balance or are operating motorized vehicles. These factors may contribute to dominant hand injuries being at higher risk of PSNU. Conversely, injuries to non-dominant hands may be protective and encourage union following a scaphoid surgery, as patients may find minimal disruption in their daily functioning. This finding may be used to re-evaluate postoperative immobilization methods, educate patients, and recommend they modify ADLs to favor their non-dominant hand. Further studies are required in this area.
Smoking at time of surgery was significant in the univariable analysis (P = .02) but did not hold up in the final multivariable analysis; however, the results from the smoking analysis do present an interesting finding. In the initial univariable analysis, we found that being an active smoker at the time of surgery was significant (P = .02) yet being an active smoker at the time of recruitment to the trial was not (P = .18). At the time of recruitment to the trial, which is an average of 54 days before the surgery, 32 patients identified as active smokers. All patients were counseled on the perils of smoking. By the time of surgery, 14 patients had quit smoking. Interestingly, only 2 (14%) of those who quit went on to experience PSNU, while 12 (86%) went on to achieve union following SNU surgery. Few studies have investigated the impact of smoking on non-union surgery for scaphoid fractures, but after reviewing the findings of a 2006 study by Little et al, 39 we anticipated it would be a significant risk factor for causing PSNU in our study population. Although we cannot draw definitive conclusions from these results and recommend further study on the topic, these findings suggest that quitting smoking before surgery may improve patients’ odds of union to those of a non-smoker, and smoking cessation counseling should remain a vital component of SNU management.
Limitations
There are limitations to our study. One limitation of our study is that despite our large sample size of 134, our persistent non-union sample size is small, at just 20 patients. Furthermore, although the prospective nature of SNAPU has increased the power of this data set, there may be selection bias involved in the original trial. As those who consent to participation in the study commit to 20 minutes per day of using an ultrasound device on their wrists, they could also be those who are more motivated to follow postoperative instructions to maximize their chances of healing. This may mean that in clinical practice, the rate of SNU could be higher as some patients may disregard postoperative instructions. In addition, the patients from the SNAPU trial all underwent LIPUS or placebo exogen treatment to determine its effects on union rates and time to union. The SNAPU trial found that LIPUS treatment did not impact union rates or time to union, and therefore, we believe that our results were not affected by the LIPUS treatment itself. In addition, committing to 20 minutes per day of self-administering ultrasound may seem like an insignificant amount of time to some, but it is possible that this reflects a population whose occupation or daily routine has more predictability. For this reason, and because information on income was not recorded, further study needs to be done assessing more standard postoperative care and considering patients’ socioeconomic status to improve generalizability. In addition, most patients were male, and the average age at the time of first surgery was 27 years. Although this does reflect much of the population who experiences scaphoid fractures, if clinicians are attempting to determine a female and/or elderly patient’s risk for SNU, this should be taken into consideration. Despite these limitations, we believe that this study has revealed 3 clinically relevant and reliable risk factors to predict the odds of a postoperative PSNU.
Footnotes
Acknowledgements
This article and the research behind it would not be possible without the help of the staff at multiple facilities who assisted in recruiting patients and gathering data for the SNAPU trial. These sites include South Health Campus and the Peter Lougheed Center (Calgary, Alberta, Canada), St. Paul’s Hospital (Vancouver, British Columbia, Canada), The Ottawa Hospital (Civic Campus) (Ottawa, Ontario, Canada), and Hôpital du Sacré-Coeur de Montreal (Montréal, Quebec, Canada). We would also like to thank SCRUBS and WECAN for their contributions as co-investigators in the original SNAPU trial.
Authors’ Note
Research for this study was done at the South Campus Research Unit for Bone and Soft Tisue (SCRUBS) lab.
Author Contributions
Statistical analyses were completed by E.C.S. The parent trial and idea for this study was conceived by N.J.W, who encouraged and supervised E.D.P. and C.E. while they carried out investigations and collation of the data. E.D.P. wrote the manuscript in consultation with N.J.W. and G.D. All authors had input on, and approved, the final version of the manuscript.
Ethical Approval
Ethics approval for this trial was granted by the University of Calgary’s Conjoint Health Research Ethics Board (CHREB) (REB13-0849).
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the trial from which this study’s data were repurposed from. There is no participant-identifying information in this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: For previous work on the SNAPU trial from which this study’s data were repurposed from, N.J.W. received a grant from Bioventus LLC. The authors otherwise declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible by funding provided by SCRUBS and the University of Calgary. In addition, E.D.P. was awarded a summer studentship grant by the Queen’s University School of Medicine that supported this research. In addition, N.J.W. received a grant from Bioventus LLC (Durham, North Carolina, United States) for the randomized controlled trial from which this study’s data were repurposed from.