
Abstract
Background:
Dupuytren disease is a common fibroproliferative disease that affects the palmar fascia of the hands. Currently, there is limited consensus regarding the optimal therapy for this condition, with treatment decisions based largely on surgeon preference. Therefore, the aim of this study was to determine which treatments are the most effective for Dupuytren disease.
Method:
A systematic review and network meta-analyses were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines. Medline, EMBASE, and Web of Science were searched for randomized trials comparing treatments for Dupuytren disease in adults. Eligible treatments included open limited fasciectomy, collagenase injection, and percutaneous needle fasciotomy. Study selection, data extraction, and quality appraisal were performed in duplicate. The methodological quality was evaluated with the Cochrane risk-of-bias critical appraisal tool.
Results:
Eleven randomized clinical trials were included in this study. At short-term (1-12 weeks) and long-term (2-5 years) time points, fasciectomy improved contracture release more than collagenase and needle fasciotomy as inferred by a lower total passive extension deficit. However, there was no difference between the groups regarding the best possible outcome at any time point. Fasciectomy was also superior in terms of recurrence and patient satisfaction compared with collagenase and needle fasciotomy, but only at later time points. There was no difference in skin damage–related and nerve damage–related complications following fasciectomy compared with other modalities. Risk of bias was generally moderate.
Conclusions:
Fasciectomy provides superior long-term advantages in terms of patient outcomes when compared with collagenase and needle fasciotomy. Larger trials with better blinding of outcome assessors are needed in the future.
Keywords
Introduction
Dupuytren disease is a common condition affecting the palmar aponeurosis of the upper limb. The disease progressively impairs hand function and can limit the ability to perform daily activities (such as personal care and feeding) as well as quality of life. .1,2 Patients typically present with an enlarging palmar nodule, and in advanced stages, they present with flexion contracture of the affected fingers. In most instances, the little finger and the ring finger are affected, followed by the first web space. 3 There are many different types of cords that vary based on anatomical consideration and include pretendinous, spiral, lateral, and central cords. Pretendinous and spiral cords tend to result in flexion contracture at the metacarpophalangeal joint (MCPJ), whereas lateral and central cords more commonly affect the proximal interphalangeal joint (PIPJ). Other variants such as natatory and retrovascular cords also exist. 4
To date, there is no cure for Dupuytren disease. Most existing treatments aim to improve functionality by releasing the contracture. However, each treatment differs with respect to the mechanism of action, risks, side effects, and recovery courses. Collagenase clostridium histolyticum injection, percutaneous needle fasciotomy, and open limited fasciectomy are the most common treatments for Dupuytren disease, and all 3 show favorable short-term outcomes.5,6 Yet it is unclear which treatment is superior and whether it confers long-term benefits to the patient. The uncertainty is exacerbated by the lack of clinical guidelines directing care; thus, decision-making is often reflective of the surgeon’s preference. 7 Therefore, the aim of this study is to systematically evaluate the effectiveness and safety of fasciectomy, collagenase injection, and needle fasciotomy for Dupuytren disease in adults.
Materials and Methods
This study followed the Preferred Reporting Items for Systematic Review and Meta-Analyses for Network Meta-Analyses (PRISMA-NMA) 2020 statement. This systematic review was registered with PROSPERO on August 25, 2021 (CRD42021269463).
Eligibility Criteria
The population, intervention, comparator group, outcome structure was used to guide the inclusion and exclusion criteria for this review.
Population
Adults (at least 18 years of age) with a diagnosis of Dupuytren disease (irrespective of the disease stage) affecting the MCPJ and/or the PIPJ.
Intervention
Percutaneous needle fasciotomy is a minimally invasive technique that has been used since the 1970s to treat Dupuytren disease. Cords are carefully divided with a percutaneous syringe needle until the affected fingers can be extended. 8
Comparator
Collagenase injection is a nonoperative treatment for Dupuytren disease approved by the US Food and Drug Administration in February 2010. It is an injectable solution that contains 2 collegenases, AUX 1 (class I C histolyticum collagenase) and AUX 2 (class II C histolyticum collagenase). In vitro research suggested collagenase application to contracted cords and bands causes hydrolyzation of collagen, which in turn improves elasticity and mobility. 6
Open fasciectomy is the most invasive technique available. Carefully planned skin excisions are used to provide surgical exposure. Disease plantar fascia is then excised to allow straightening of the affected fingers.9,10
Outcomes
The primary outcomes related to the efficacy of the interventions and included disease recurrence rates (percentage of patients) and contracture change. Contracture change was measured by the total passive extension deficit (TPED) in degrees after treatment and the number of patients with <5° TPED post-treatment (termed optimal outcome). Secondary outcomes included adverse events and patient satisfaction scores. Adverse events were categorized into 3 groups: skin-related complications, nerve damage, and edema. Skin-related complications referred to issues with wound healing, such as infection and dehiscence. Nerve damage included individuals with postoperative loss of sensation to areas of the hand and direct injury to digital neural structures. Patient satisfaction was measured by Disabilities of the Arm, Shoulder, and Hand (DASH) and Unité Rhumatologique des Affections de la Main (URAM) questionnaires. These questionnaires evaluate the impacts of upper limb function on patient experience. A higher score indicated a greater functional impairment and therefore less patient satisfaction.
Study Design
Only randomized clinical trials (RCTs) were eligible for this review given the comparative nature of network meta-analyses. Randomized clinical trials had to include at least 2 of the following treatments: collagenase injection, needle fasciotomy, or fasciectomy.
Exclusion Criteria
Nonrandomized studies and trials that compared only a single intervention with a control group were excluded given the objective of this study. Other exclusion criteria included: letters, editorials, perspectives, reviews, and non-English publications and studies in children.
Search Strategy
Medline Ovid, EMBASE Ovid, and Web of Science platforms were searched on August 4, 2021, to identify relevant citations. The search strategy is included in the supplementary materials as Supplementary Figure 1. Targeted Google searches were used to identify further relevant trials.
Study Selection and Data Extraction
Title and abstract screening was performed independently by 2 reviewers (S.N. and J.K.) using Rayyan (Qatar Computing Research Institute, Ar-Rayyan, Qatar). 11 Eligible trials were then reviewed at full text by 2 reviewers (S.N. and J.K.). Disagreements were discussed until a consensus was achieved. Two reviewers (J.F. and J.H.) extracted data using COVIDENCE. 12 The following information was extracted: trial inclusion and exclusion criteria, number of participants included/excluded, total number randomized to each intervention, missing data, patient demographic data (age, sex, comorbidities, etc), efficacy data before and after the intervention (primary outcomes), and patient satisfaction and complications rates (secondary outcomes). The data subsequently were transferred to an Excel spreadsheet for analysis by a third author (S.N.).
Risk-of-Bias Appraisal
Two reviewers (S.N. and J.F.) independently performed a risk-of-bias analysis. All included studies were appraised using the Cochrane risk-of bias tool 2.0. 13 Any disagreements were resolved by discussion.
Statistical Analysis
Network meta-analysis was used for the following outcomes: TPED, optimal outcome rates, recurrence rates, DASH and URAM scores, and complications. The outcomes were delineated into 3 time points: 1-12 weeks, 6-12 months, and 2-5 years, representing short-term, mid-term, and long-term time points. Data were aggregated based on which time period the extracted study data fell into. Baseline results were also analyzed for TPED and patient-reported outcomes. Separate network meta-analyses were completed across the 3 treatment groups: fasciectomy, collagenase injection, and needle fasciotomy for each outcome. Results were presented as mean difference or odds ratio (OR) with 95% confidence intervals (CIs). Results were considered statistically significant when the P value was <.05.
Heterogeneity was considered accounted for through a random-effects model. A common heterogeneity variance was assumed across all pairwise comparisons. Inconsistency was assessed using χ2 testing. A P value of <.05 was used to determine that inconsistency was present. Statistical analyses were performed using Stata Statistical Software: Release 15.1 (StataCorp LP, College Station, Texas). 14
Results
Characteristics of the Included Studies
From the 938 identified citations, 11 studies were included in this review. The PRISMA study flow diagram is presented in Figure 1. 15 A detailed summary of each publication is presented in Supplementary Table 1. All of these were prospective RCTs with 2 parallel arms that compared treatments with needle fasciotomy, collagenase injection, or fasciectomy for Dupuytren disease. Ten trials were performed in Europe and 1 in Japan. Follow-up varied from 6 weeks to 5 years. On average, patients across all studies were in their 60s and had minimal comorbidities. A higher proportion of men was included, and this likely relates to the higher prevalence of disease in this group. Almost all authors only included patients with MCPJ and/or PIPJ contractures of >20°-30°. Two authors excluded patients with PIPJ contractures of >60°. In general, no comment was made regarding the reversibility of the contracture. The operative procedure for each treatment was generally similar across all trials. For example, collagenase injection was performed on day 1 of the study, followed by manipulation under anesthesia 24 to 72 hours later. In 2 of the trials, repeat injections were performed 1 month later if the treatment was initially unsuccessful. Needle fasciotomy was performed under local anesthesia with a needle that was inserted percutaneously. One trial also used lipofilling following this procedure. During fasciectomy procedures, surgeons aimed to excise the diseased tissue completely and then close skin primarily. However, there was more variability in how this treatment was performed compared with needle fasciotomy and collagenase injection. Differences were often reflective of the surgeon preference with respect to the type of skin incision and surgical method, although most authors preferred a Bruner incision. Skin grafts were mentioned by one author and used in that trial when clinically indicated. Outcomes were measured similarly across most studies. Most studies measured TPED and the proportion of patients with the best possible outcome. Patient satisfaction was also frequently reported using DASH and URAM scoring systems.
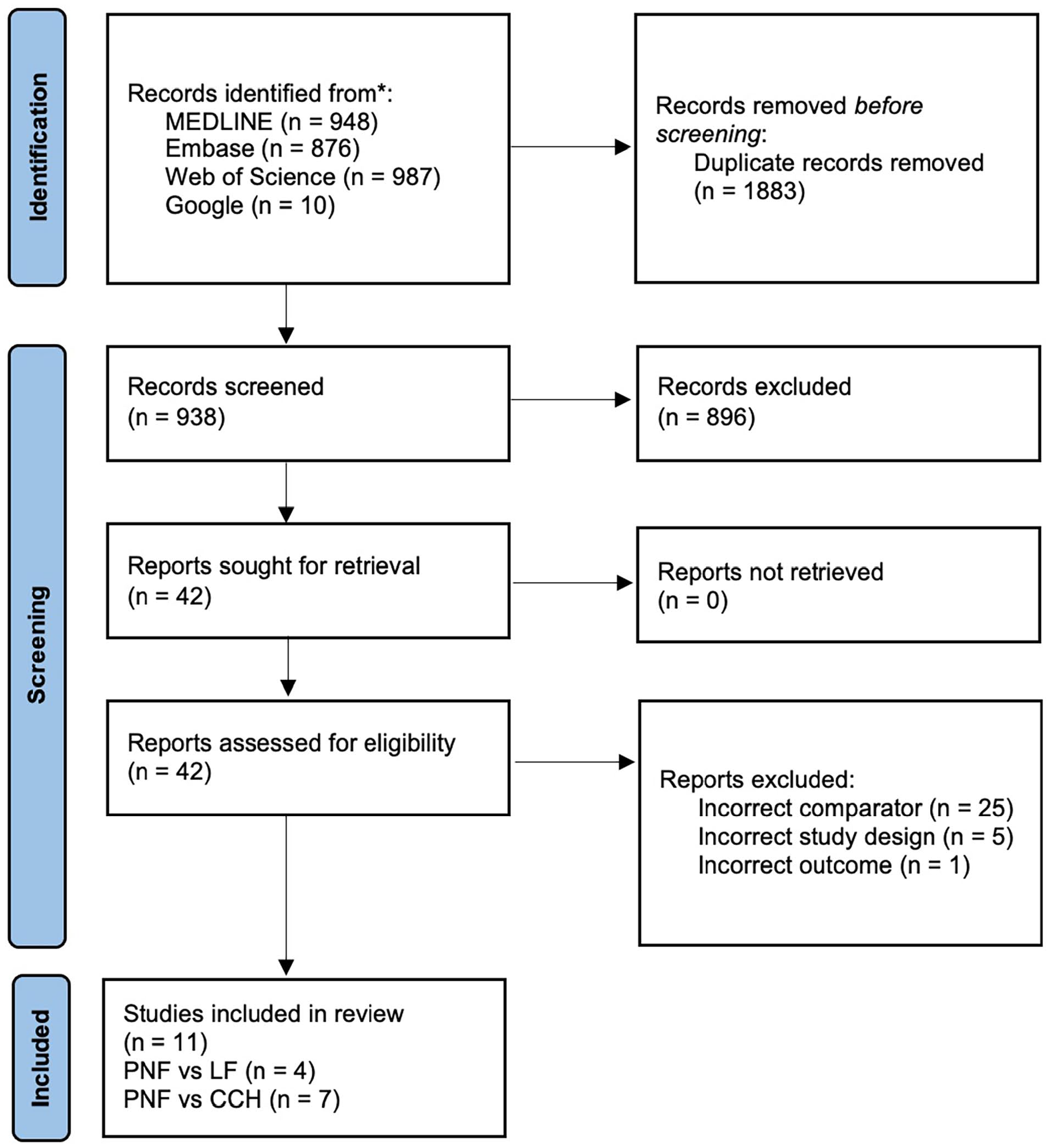
Preferred Reporting Items for Systematic Review and Meta-Analyses study flow diagram.
Findings
Total passive extension deficit
Total passive extension deficit was assessed at 1-12 weeks, 6-12 months, and 2-5 years post-surgery. Needle fasciotomy was directly compared with collagenase in 7 and to fasciectomy in 3 studies.16 -25 Results from the interval plots for TPED per time period are given in Table 1. The interval plot for the 2- to 5-year analysis is also presented in Supplementary Figure 2.
Change in TPED Score From 1-12 Weeks to 2-5 Years Post-Surgery.
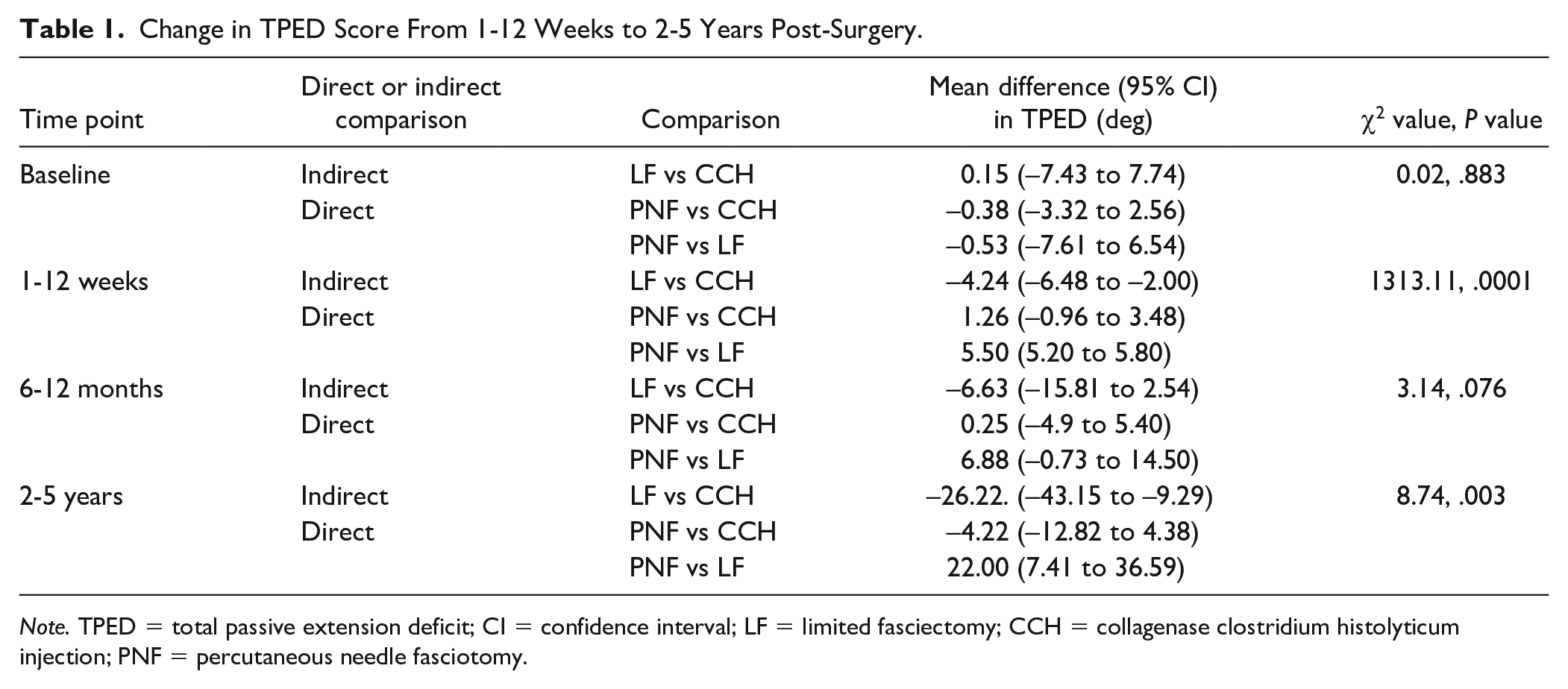
Note. TPED = total passive extension deficit; CI = confidence interval; LF = limited fasciectomy; CCH = collagenase clostridium histolyticum injection; PNF = percutaneous needle fasciotomy.
There was no difference in baseline TPED scores between all treatment groups (P > .05). Fasciectomy significantly differed from collagenase and needle fasciotomy in TPED at 1-12 weeks and 2-5 years post-surgery (P < .05). The mean difference between fasciectomy and collagenase was −4.24° (95% CI: −6.48° to −2.00°) and −5.50° (95% CI: −5.20° to −5.80°) for needle fasciotomy at 1-12 weeks. This difference was even greater after 2-5 years, with 26.22° less TPED than collagenase patients on average (95% CI: −43.15° to −9.29°) and 22.00° less TPED than needle fasciotomy patients (95% CI: 7.4°1-36.59°). No statistical differences were found between treatment groups for any analysis at 6-12 months. There were no significant differences between collagenase and needle fasciotomy at all time points.
Best possible outcome
The number of patients with optimal outcome was assessed at 1-12 weeks, 6-12 months, and 2-5 years post-surgery. Needle fasciotomy was directly compared with collagenase in 5 trials and with fasciectomy in 1 trial.16,17,22 -24,26 Results from the interval plots are presented in Table 2. The interval plot for the 1- to 12-month analysis is presented in Supplementary Figure 3.
Odds of Achieving the Best Possible Outcome From 1-12 Weeks to 2-5 Years Post-Procedure.
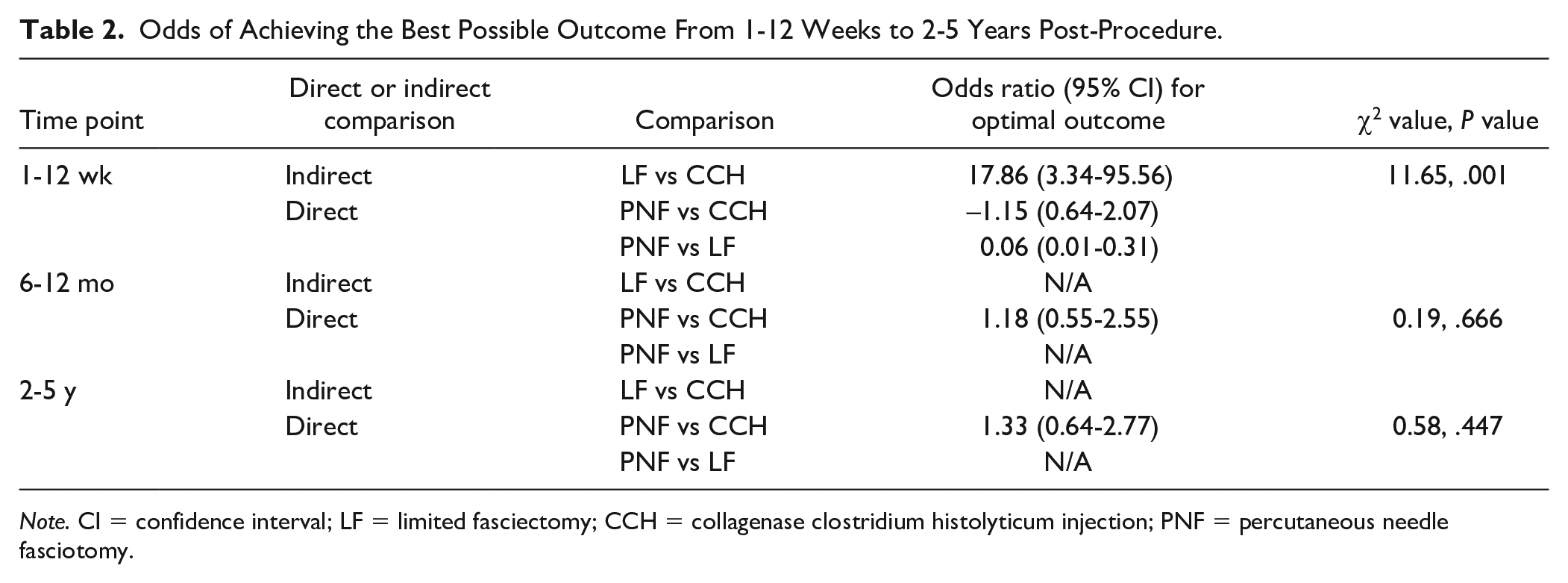
Note. CI = confidence interval; LF = limited fasciectomy; CCH = collagenase clostridium histolyticum injection; PNF = percutaneous needle fasciotomy.
There were significant differences in the number of patients reporting optimal outcome at 1-12 weeks post-surgery. Compared with needle fasciotomy and collagenase, fasciectomy had significantly greater odds of patients reporting the best possible outcome (OR: 0.06, 95% CI: 0.01-0.31 and OR: 17.86, 95%CI: 3.34, 95.56, respectively) at 1-12 weeks post-surgery. This translates to a 94% and 16.86-fold greater odds of reporting the best possible outcomes for those treated with fasciectomy compared with needle fasciotomy and collagenase, respectively. There was no difference in the number of patients reporting optimal outcome following needle fasciotomy or collagenase (OR: −1.15. 95% CI: 0.64-2.07) 1-12 weeks post-surgery. There were no statistical differences for any comparison at 6-12 months or 2-5 years post-surgery.
Recurrence rate
Recurrence rates were assessed at 1-12 weeks, 6-12 months, and 2-5 years post-surgery. Needle fasciotomy was directly compared with collagenase in 5 trials and with fasciectomy in 2 trials.16,19,21 -24,26 In these studies, recurrence is defined as a loss of extension of 20° or greater in the affected joint compared with the initial result by all authors other than one, who used 30° as the “clinically significant” value. 26 Results from interval plots for each recurrence rate are given in Table 3. The interval plot graph after 2-5 years is presented in Supplementary Figure 4.
Odds of Disease Recurrence From 1-12 Weeks to 2-5 Years Post-Procedure.
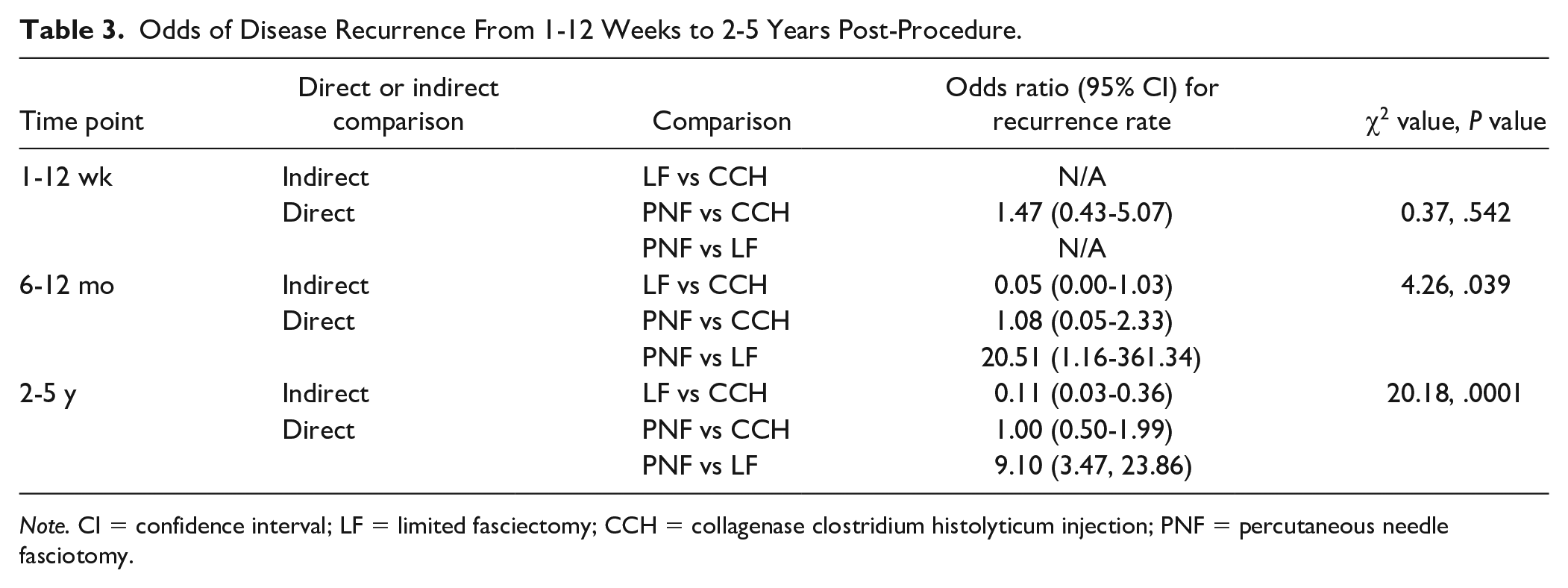
Note. CI = confidence interval; LF = limited fasciectomy; CCH = collagenase clostridium histolyticum injection; PNF = percutaneous needle fasciotomy.
Fasciectomy significantly differed from collagenase and needle fasciotomy in recurrence rates at 6-12 months and 2-5 years post-surgery (P < .05). The mean difference between fasciectomy and needle fasciotomy was OR = 20.51 (95% CI: 1.16-361.34) at 6-12 months. This translates to a 20.51-fold greater risk of recurrence for patients undergoing needle fasciotomy. At long-term time points, the mean difference between fasciectomy and collagenase was OR = 0.11 (95% CI: 0.03, 0.36) and OR = 9.10 (95% CI: 3.47-23.86) for needle fasciotomy. This translates to an 89% and 9.10-fold reduction in recurrence, respectively. There were no significant differences between collagenase and needle fasciotomy at all time points and no difference between treatments in the first 3 months.
Patient-reported satisfaction
Patient DASH and URAM scores were assessed at 1-12 weeks, 6-12 months, and 2-5 years post-surgery. Needle fasciotomy was directly compared with collagenase in 3 trials and with fasciectomy in 3 trials.16 -18,20,21,25 Results from interval plots for the DASH score at each time period are given in Table 4. The interval plot for DASH scores after 2- to 5-year analysis is also presented in Supplementary Figure 5.
Patient Satisfaction (DASH) From 1-12 Weeks to 2-5 Years Post-Surgery.
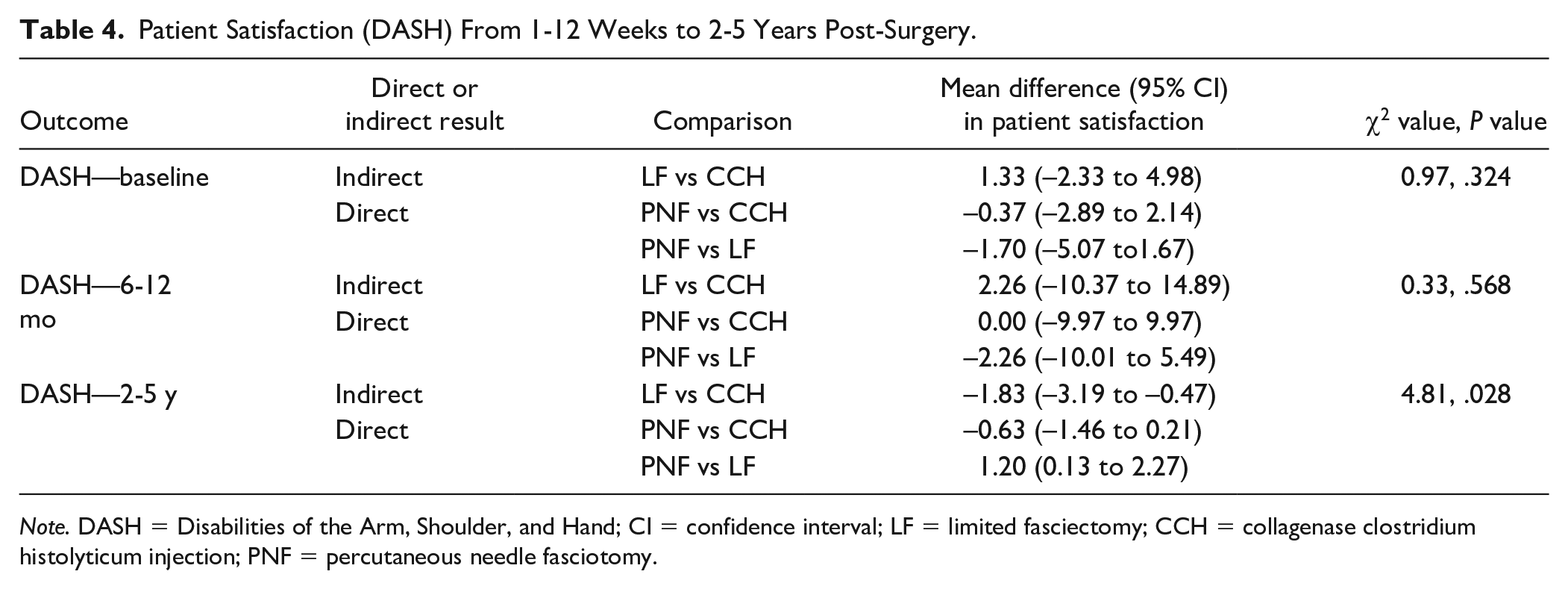
Note. DASH = Disabilities of the Arm, Shoulder, and Hand; CI = confidence interval; LF = limited fasciectomy; CCH = collagenase clostridium histolyticum injection; PNF = percutaneous needle fasciotomy.
There was no difference in baseline DASH scores between the treatments (P > .05). Significant differences were found following fasciectomy compared with collagenase and needle fasciotomy 2-5 years post-surgery. For example, patients who underwent fasciectomy had a DASH score of 1.20 points less (95% CI: 0.13-2.27) than needle fasciotomy patients and 1.83 points less (95% CI: −3.19 to −0.47) than collagenase patients. There were no significant differences 1-12 weeks or 6-12 months post-surgery or for comparisons involving collagenase and needle fasciotomy.
Furthermore, there were no significant differences between any treatment with respect to change in URAM score at any time period.
Adverse events
Adverse events data and reports up to 5 years post-surgery were aggregated. Needle fasciotomy was directly compared with collagenase in 5 trials and with fasciectomy in 2 trials.17,18,20,22 -25 Results from interval plots for each complication are given in Table 5.
Adverse Events Reported Throughout the Study Period (Up To 5 Years).
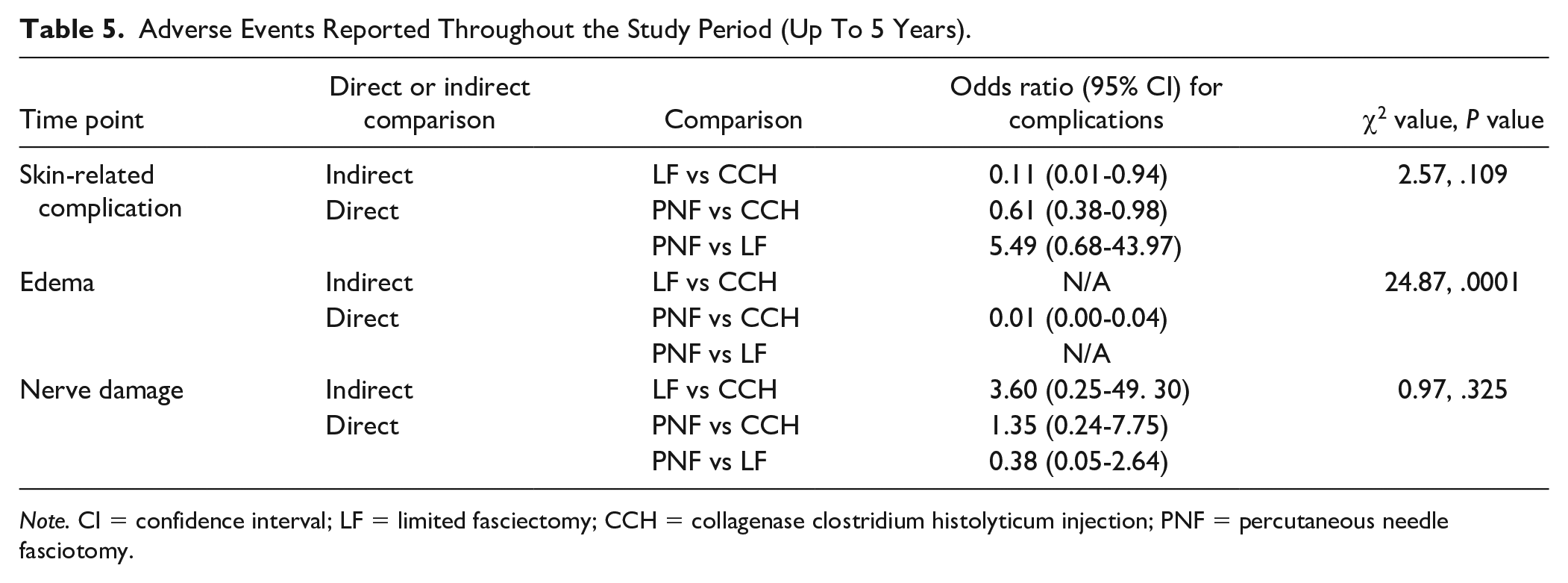
Note. CI = confidence interval; LF = limited fasciectomy; CCH = collagenase clostridium histolyticum injection; PNF = percutaneous needle fasciotomy.
Collagenase injection significantly differed from fasciectomy and needle fasciotomy in adverse event rates related to skin and edema (P < .05). Skin complications were mostly related to skin tears/rupture, as well as infection. Edema when reported was not clearly defined by authors in terms of clinical severity or timeframe.
The mean difference between collagenase and fasciectomy was OR = 0.11 (95% CI: 0.01-0.94) and OR = 0.61 (95% CI: 0.38-0.98) for needle fasciotomy when analyzing skin-related complications. This translates to an 89% and a 39% reduction in adverse skin events, respectively. In terms of edema affecting function, the mean difference between needle fasciotomy and collagenase was OR = 0.01 (95% CI: 0.00-0.04). This translates to a 99% reduction in postoperative rates of edema. No differences were found between groups when analyzing the rates of nerve damage. From the included studies, there were no reported serious adverse events, such a loss of a finger or damage to tendons, nor were there any reports of complex regional pain syndrome (CRPS).
Risk of Bias
Most of the included studies were considered to have a moderate risk of bias (Figure 2 and Supplementary Figure 6). All publications underwent a suitable randomization process. This generally involved using envelopes or computer codes. Most trials concealed allocations appropriately. As all 3 treatment modalities (collagenase, needle fasciotomy, and fasciectomy) are distinctive in their delivery, blinding of surgeons was unachievable across all studies. However, participants were adequately blinded across all studies. It is theoretically possible to blind outcome assessors (eg, examination with the treated hand hidden by a plastic glove); however, this was only implemented in selected studies. Despite appropriate outcome measures being used for all studies, knowledge of the treatment provided may have influenced assessor judgment and thereby created a potential for some detection bias. All publications described an appropriate estimation of study effect and a degree of statistical significance, minimizing the effects of reporting bias. Almost all authors declared that they have no financial interest related to the contents of the articles. Only public funding was used for studies that declared the source of funding.
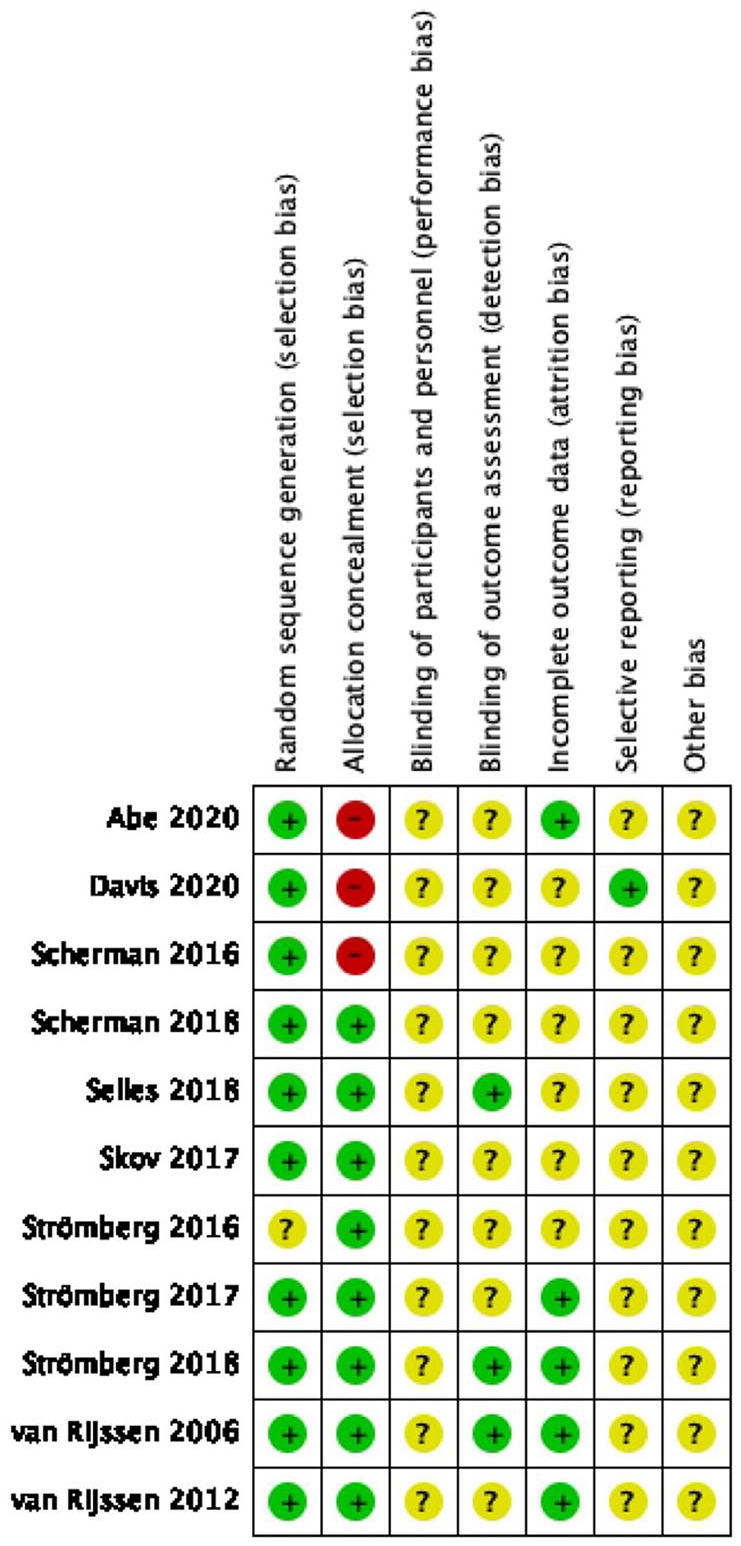
Quality appraisal of the included studies using the Cochrane risk-of-bias 2.0 tool.
Discussion
Currently, there is no consensus regarding the optimal treatment for Dupuytren disease. Usually, surgeons determine management plans based on personal experience and institutional preferences. 7 Previous systematic reviews suggest that open limited fasciectomy has the lowest recurrence rates, yet also lower patient satisfaction and higher adverse events rates than needle fasciotomy. 27 The aim of this network meta-analyses was to determine the relative safety and effectiveness of collagenase, needle fasciotomy, and fasciectomy for Dupuytren disease thereby informing evidence-based practice and clinical guidance.
Total passive extension deficit is frequently used to determine the success of the surgery given it is an objective measure of hand flexibility. The network meta-analyses indicated that, shortly after surgery, fasciectomy yields slightly better TPED scores compared with collagenase and needle fasciotomy. While there is an initial short-term benefit following fasciectomy compared with collagenase and needle fasciotomy, it is unclear whether this is outweighed by the severity of the side effects. After 2-5 years of surgery, patients who underwent a fasciectomy continued to exhibit significant greater flexibility compared with other treatments (as inferred by the TPED score). Extension improved by 22.0° and 26.22° compared with collagenase and needle fasciotomy, respectively. The greater flexibility following fasciectomy may reflect that a greater amount of disease tissue is removed compared with needle fasciotomy and collagenase, which in turn allows the hand to move more. Importantly, it is currently unclear to what extent TPED correlates with quality-of-life measures and what the clinical significance of short-term changes in TPED is given the patient’s hand function is impaired owing to the recovery/wound-healing process. Future research needs to correlate TPED to quality-of-life scores and determine how much extension is needed to improve patients’ lives.
The best possible outcome implies that the function of the hand in terms of passive extension is comparable to a nondiseased state (ie, almost complete reversal of the contracture). It was found that rates of patients with TPED of <5% are only statistically significant during the first 3 months, where fasciectomy patients are much more likely to present with the best possible results than any other treatment modality. This has been suggested by other authors who have reported complete contracture release in 61% to 97% of patients.9,10 Again, the significance of this is unclear because these patients underwent the most substantial surgical intervention with associated longer recovery courses and more extensive follow-up postoperatively. In the long term, rates of patients with TPED of <5° appear to be similar between groups. Therefore, although recurrence is less likely and TPED is improved on average with fasciectomy, the rates of patients with complete contracture release in the long term are not statistically different.
The removal of affected tissue does not prevent recurrence of disease as the underlying genetic defect will continue to express abnormal protein, and consequently, no cure exists to date for Dupuytren disease. Therefore, it is important to consider how likely it is for the disease to return following treatment. Fasciectomy seems to have distinct benefits compared with collagenase and needle fasciotomy when considering recurrence rates. After 12 months, the patients who underwent needle fasciotomy are 20.51 times more likely to present with contracture recurrence of 20° or more. This is a substantial difference, especially because the baseline characteristics of patients (eg, disease severity, comorbidities) were similar for all included studies. The lower rates of recurrence persisted at later time points, reinforcing the superiority of fasciectomy. It should be noted that recurrence was only defined in degrees, rather than need for further procedures that must be considered by clinicians. There were no statistical differences for any collagenase versus needle fasciotomy comparisons.
Although fasciectomy is more invasive than other techniques, patient satisfaction is not affected in the short term or the long term. No statistical difference in DASH or URAM scores was found in the first year after operation. After 2-5 years, fasciectomy patients reported a minor improvement in DASH scores compared with needle fasciotomy and collagenase. On average, with the open technique, scores are 1.20 and 1.83 points better, respectively. This difference is unlikely of clinical relevance as the minimum clinically important difference for this scoring system has been estimated to be 10.83 points. 28 Regardless, this minor statistical improvement in DASH scores highlights that fasciectomy has similar patient satisfaction outcomes at all time points.
Adverse events were also analyzed in this network meta-analysis. Across the 11 included RCTs, there were no reported serious adverse events, such as tendon damage or loss of digits, nor any cases of CRPS. Interestingly, collagenase is the most prone to cause skin-related complications. It also most probably results in clinically relevant edema, and hence, collagenase seems to have more associated complications than any other technique, likely related to the chemical properties of the injected solution. Fasciectomy is not more likely to result in adverse events than needle fasciotomy or collagenase, including neurological and skin complications. All techniques appear to be safe with low number of serious adverse outcomes.
Overall, fasciectomy is better than other techniques across multiple measured long-term parameters, with no differences in patient satisfaction at all time points. Surgeons should take this into consideration when counseling patients regarding treatment options. Needle fasciotomy will always be better tolerated than open surgery due to being a minimally invasive technique and should be considered as an option to defer fasciectomy in patients with mild disease and in the aged infirm where the time of recurrence is less important than achieving some functional improvement with minimal morbidity. It may be particularly useful in disease of the MCPJ. Significant deformity of the PIPJ is more suitable to be treated with open surgery because of the increased risk of injury to neurovascular structures. 29 Although needle fasciotomy is certainly useful in select circumstances, the risk of recurrence is significantly higher compared with fasciectomy.
It should be noted that for the outcomes related to TPED, recurrence rates, and patient satisfaction, no statistical differences were found for any comparison between needle fasciotomy and collagenase. This indicates that there is no measurable benefit with either technique. The cost of collagenase injection is substantially higher as 2 visits with surgical input are required, compared to 1 visit. 16 This technique also appears to have more minor adverse events associated, in particular, local skin complications. For these reasons, the collagenase product is no longer available in some jurisdictions, including Australia.
This review is subject to several limitations. High-quality data in this field are still limited. Included studies are mostly small in terms of number of participants. Selection of adverse events reported in these RCTs does not capture all the possible complications in a relevant manner. All trials have either moderate or high risk of bias when analyzing the design. A particular area of concern was lack of blinding in most studies. Because this was difficult to achieve given the type of intervention, most publications feature data collectors and outcome assessors that were unblinded. This may have resulted in detection biases. The collected data were aggregated in 3 blocks of time after operation and hence were potentially affected by publication bias. Although heterogeneity was low in general, inconsistencies between trials may have affected the network meta-analysis to some degree, which may limit the applicability of results. Particularly, indirect comparisons between collagenase and fasciectomy are subject to uncertainty, and it is unclear to what extent this mirrors real-world data. Furthermore, this is a condition where patient-reported functional improvement is more important than changes in angulation of the contracture; however, data are much more limited for this outcome, and therefore, the conclusion is less robust. Another limitation in the current reporting is the incapacity to control for the degree of postoperative hand therapy input. It is likely that studies the incorporate aggressive hand therapy will have better outcomes, particularly among the more severely affected patient groups.30,31 Future research should focus more on patient-reported outcomes than other measurable variables, as well as evaluating the role of hand therapy during the recovery period. Trials directly comparing collagenase with fasciectomy would further improve the quality of data in this field.
Conclusion
Fasciectomy results in superior long-term outcomes. Compared with needle fasciotomy and collagenase injection, fasciectomy improved long-term TPED significantly more on average and is less likely to result in recurrent disease. Patient satisfaction is equivocal in early stages of recovery and improved following fasciectomy in the long term, although this is unlikely to reflect a minimum clinically important difference. The selection of adverse events reported by these RCTs does not capture all the possible complications; however, in this analysis, adverse events are not more likely to occur with fasciectomy. Collagenase injection was more likely to cause skin and edema complications and was not superior compared with needle fasciotomy for any measured outcome.
Supplemental Material
sj-docx-1-han-10.1177_15589447231174175 – Supplemental material for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses
Supplemental material, sj-docx-1-han-10.1177_15589447231174175 for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses by Silas Nann, Joshua Kovoor, James Fowler, James Kieu, Aashray Gupta, Joseph Hewitt, Christopher Ovenden, Suzanne Edwards, Stephen Bacchi, Jonathan Henry W. Jacobsen, Richard Harries and Guy Maddern in HAND
Supplemental Material
sj-jpeg-2-han-10.1177_15589447231174175 – Supplemental material for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses
Supplemental material, sj-jpeg-2-han-10.1177_15589447231174175 for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses by Silas Nann, Joshua Kovoor, James Fowler, James Kieu, Aashray Gupta, Joseph Hewitt, Christopher Ovenden, Suzanne Edwards, Stephen Bacchi, Jonathan Henry W. Jacobsen, Richard Harries and Guy Maddern in HAND
Supplemental Material
sj-jpeg-3-han-10.1177_15589447231174175 – Supplemental material for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses
Supplemental material, sj-jpeg-3-han-10.1177_15589447231174175 for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses by Silas Nann, Joshua Kovoor, James Fowler, James Kieu, Aashray Gupta, Joseph Hewitt, Christopher Ovenden, Suzanne Edwards, Stephen Bacchi, Jonathan Henry W. Jacobsen, Richard Harries and Guy Maddern in HAND
Supplemental Material
sj-jpeg-4-han-10.1177_15589447231174175 – Supplemental material for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses
Supplemental material, sj-jpeg-4-han-10.1177_15589447231174175 for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses by Silas Nann, Joshua Kovoor, James Fowler, James Kieu, Aashray Gupta, Joseph Hewitt, Christopher Ovenden, Suzanne Edwards, Stephen Bacchi, Jonathan Henry W. Jacobsen, Richard Harries and Guy Maddern in HAND
Supplemental Material
sj-jpeg-5-han-10.1177_15589447231174175 – Supplemental material for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses
Supplemental material, sj-jpeg-5-han-10.1177_15589447231174175 for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses by Silas Nann, Joshua Kovoor, James Fowler, James Kieu, Aashray Gupta, Joseph Hewitt, Christopher Ovenden, Suzanne Edwards, Stephen Bacchi, Jonathan Henry W. Jacobsen, Richard Harries and Guy Maddern in HAND
Supplemental Material
sj-jpeg-6-han-10.1177_15589447231174175 – Supplemental material for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses
Supplemental material, sj-jpeg-6-han-10.1177_15589447231174175 for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses by Silas Nann, Joshua Kovoor, James Fowler, James Kieu, Aashray Gupta, Joseph Hewitt, Christopher Ovenden, Suzanne Edwards, Stephen Bacchi, Jonathan Henry W. Jacobsen, Richard Harries and Guy Maddern in HAND
Supplemental Material
sj-jpeg-7-han-10.1177_15589447231174175 – Supplemental material for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses
Supplemental material, sj-jpeg-7-han-10.1177_15589447231174175 for Surgical Management of Dupuytren Disease: A Systematic Review and Network Meta-analyses by Silas Nann, Joshua Kovoor, James Fowler, James Kieu, Aashray Gupta, Joseph Hewitt, Christopher Ovenden, Suzanne Edwards, Stephen Bacchi, Jonathan Henry W. Jacobsen, Richard Harries and Guy Maddern in HAND
Footnotes
Ethical Approval
Formal ethics approval is not required for this type of study.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects
Statement of Informed Consent
The research was performed in accordance with relevant guidelines and regulations. Patient data were stored and managed in accordance with the Australian Code for the Responsible Conduct of Research. Informed consent was not required for this type of study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.M. was the authorizer of a health technology assessment of the collagenase product for South Australia; however, this does not represent a conflict of interest with regard to this publication. The authors have no other conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.