
Abstract
Background:
Unstable fractures of the base of the middle phalanx are notorious for causing chronic loss of proximal interphalangeal (PIP) joint function, and they remain a challenge for the hand surgeon. We report on a temporary intraoperatively constructed internal joint stabilizer for unstable PIP joint injuries.
Methods:
Across 2 institutions, a retrospective chart review was performed for cases with acute presentation of pilon fracture or fracture-dislocation of the base of the middle phalanx which were surgically treated with an internal joint stabilizer. Information collected included time from injury to surgical intervention, time from implantation to device removal, complications, and preoperative and postoperative range of motion.
Results:
Seven patients met the inclusion criteria with a mean age of 51 (range: 24-72) years and a mean follow-up of 29 (range: 11-72) months. After removal of the fixator, the mean arc of PIP joint motion was 8° to 88° (range: 0°-100°). There were no infections, no hardware loosening or failures, and no revision procedures.
Conclusion:
The current findings are comparable to the results for dynamic external fixators. An internal joint stabilizer for unstable injuries to the base of the middle phalanx provides satisfactory functional outcomes, allows early postoperative motion, and mitigates the routine complications which may arise with external fixation.
Introduction
The proximal interphalangeal (PIP) joint is critical for hand function. A dysfunctional PIP joint can severely diminish the function of adjacent digits and occasionally the whole hand. 1 Unstable fractures of the base of the middle phalanx (P2) are notorious for causing chronic loss of PIP function, and they remain a challenge for the hand surgeon.
Many treatment methods are available, and there is no consensus on which is optimal. These methods include static or dynamic external fixation, open reduction internal fixation, closed reduction and pinning, volar plate arthroplasty, and hemi-hamate arthroplasty.2 -6 The central tenant for treatment of these injuries is to restore joint congruency. Failure to do so results in pathologic joint kinematics and often post-traumatic arthritis. 7
From the 1980s to the early 2000s, several techniques were developed for compact motion-allowing external dynamic fixators for PIP joint injuries. 8 Some of these were complex miniature variants of similar devices that had been developed for injuries of the elbow, ankle, and other medium-sized joints. Other devices were created by the surgeon in the operating room using Kirschner wires (K-wires), with or without rubber bands.9 -12 Limitations of these devices are their external placement and the use of transcutaneous pins which frequently loosen, become infected, or can be painful and inhibit active motion. Further, external devices can interfere with adjacent finger motion. 13
We introduce a technique using a temporary intraoperatively constructed internal joint stabilizer for unstable base of P2 PIP joint injuries. This method provides the benefits of articulating external fixators without a bulky apparatus and removes the potential for pin tract complications.
Methods
A retrospective chart review from 2010 to 2020 (IRB 1-1504538-1) was performed at 2 institutions for cases with acute presentation of dorsal fracture-dislocations of P2 with intact dorsal cortex and disrupted volar articular surface, and pilon fractures of P2 with complete disruption of the articular surface from the shaft which were surgically treated with an internal joint stabilizer. Chronic presentation and acute injuries that were surgically treated with other fixation constructs were not included. Range of motion (ROM) at the PIP joint was collected for each patient. Complications were compiled including infection, device loosening, or failure and secondary procedures including revision surgery and device removal.
Fixation Concept
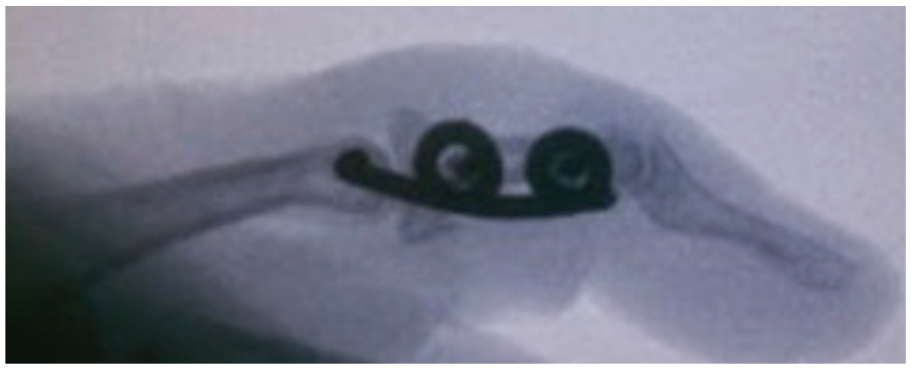
The concept of an internal joint stabilizer has been previously described for elbow instability.14 -16 When it is constructed for the treatment of an unstable P2 PIP injury, a rotating pin is placed along the axis of PIP motion to maintain joint reduction and guide proper joint kinematics (Figure 1). It is affixed to the lateral aspect of P2 by a longitudinal section capable of accepting screws. The surgeon creates the device intraoperatively by shaping an appropriately sized K-wire. The wire is bent close to a right angle at its proximal aspect to allow the axis pin to be inserted along the anatomical PIP rotational axis. The distal longitudinal section requires the creation of 2 loops to accept screw fixation to P2.
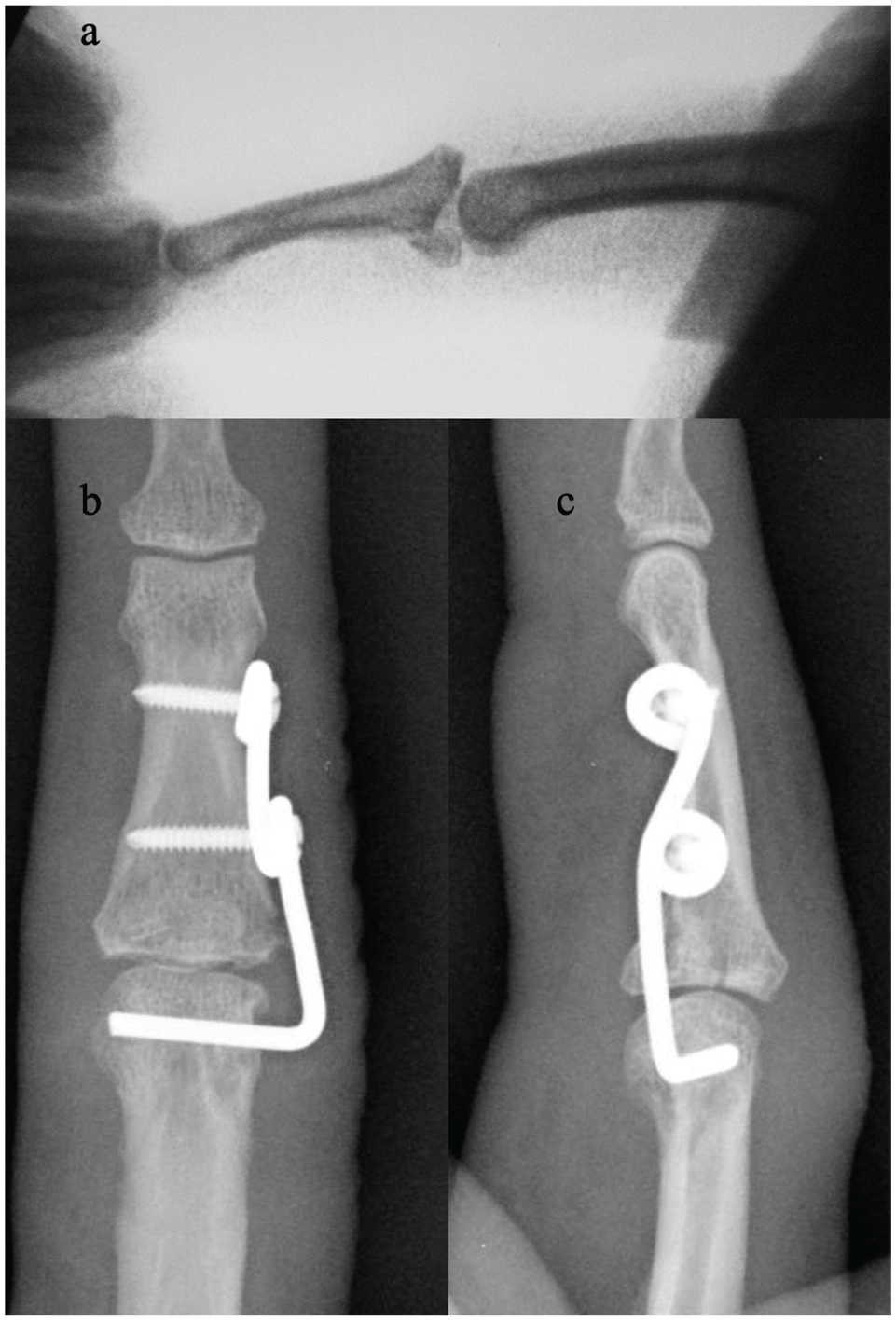
(a) Lateral fluoroscopy demonstrating unstable fracture-dislocation of the base of the middle phalanx. (b) Anteroposterior and (c) lateral radiographs of the internal joint stabilizer applied to the proximal interphalangeal joint.
Technique
Once this method has been selected, the surgeon decides whether the device will go on the radial or the ulnar side of the digit. Placing the incision on the external aspect of a border digit is both technically easier and avoids wound irritation against the adjacent finger during rehabilitation. Conversely, there is the possibility of developing an undesired or dysesthetic scar on the exposed border of the index finger or small finger.
The injured joint is anatomically reduced (Figure 2). Reduction can be achieved in either a closed or an open fashion. Temporarily fixation is applied with a small K-wire—usually 0.028 inch. This wire is typically placed through the dorsum of P2 and into the condyles of the proximal phalanx (Figure 3a). In the proximal phalanx, the desired K-wire position is either slightly dorsal or slightly volar to the PIP axis to prevent interference with the axis pin.
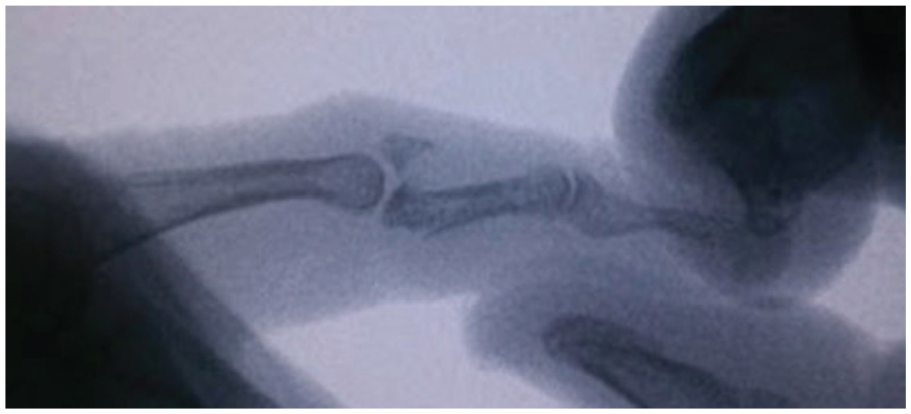
Lateral fluoroscopy of a comminuted unstable fracture of the base of the middle phalanx, with applied longitudinal traction.
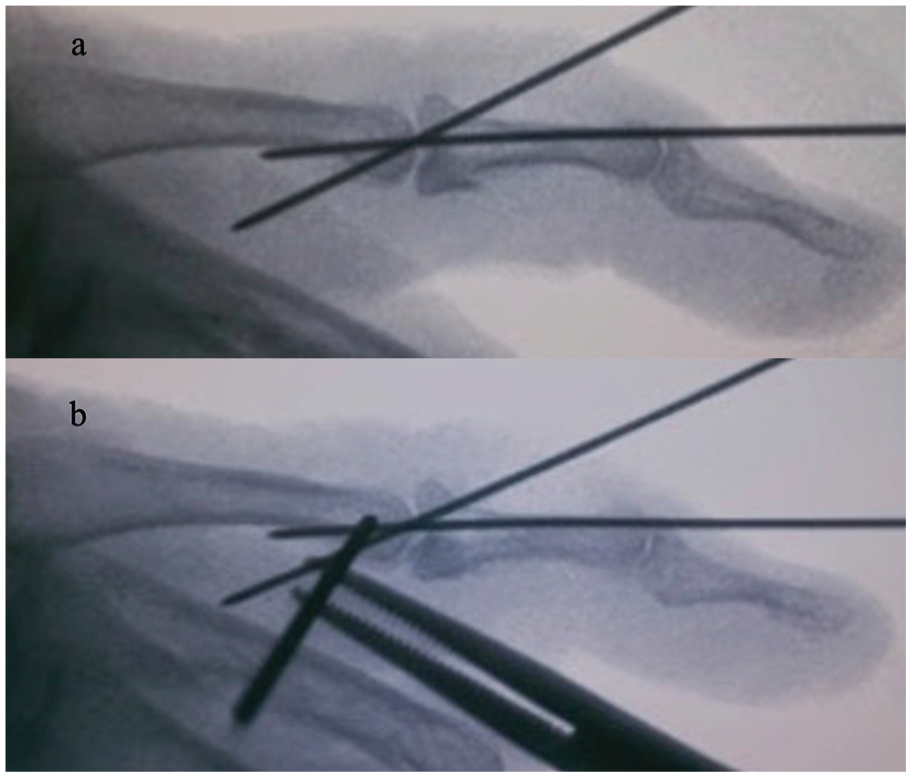
Lateral fluoroscopy of (a) provisional fixation with Kirschner wires following closed reduction and (b) insertion of the axis pin through the condylar section of the proximal phalanx.
Before or after obtaining reduction, a mid-axial incision is made spanning the length of P2 and the distal third of the proximal phalanx. After dissection and retraction of the volar and dorsal skin flaps, the dorsal branch of the digital nerve must be mobilized and should be preserved. Access to both the fracture and the PIP joint is attained by releasing the transverse retinacular fibers and mobilizing the lateral band and extensor hood.
The stabilizer is created by bending a 0.062- or 0.045-mm K-wire around a 2.0-mm Steinmann pin or K-wire to create the holes for the screws. The size of the loops is such that the screw shaft can easily pass through the loop, but the screw head cannot. These should be spaced far enough apart to provide ample working length with respect to the length of P2. Now, the transcondylar width of the proximal phalanx is assessed. The pilot hole is created under fluoroscopic guidance along the PIP axis of rotation. The drill is aligned with the center of curvature of both the medial and lateral PIP condyles (Figure 3b). The wire is then driven through the far cortex. Now the K-wire is bent to 90° to place the 2 screw holes at the proper level with respect to the distal part of P2. The length of the axis pin is measured with a depth gauge, and the wire is cut to this length. The axis pin is inserted into the proximal phalanx, and the alignment of the stabilizer with respect to P2 is evaluated. A final shaping of the stabilizer is needed to provide optimal reduction and alignment of P2. Finally, 2.0-mm screws are applied to the distal part of the stabilizer after drilling their pilot holes (Figure 4).
Lateral fluoroscopy of the insertion of screw through the internal joint stabilizer.
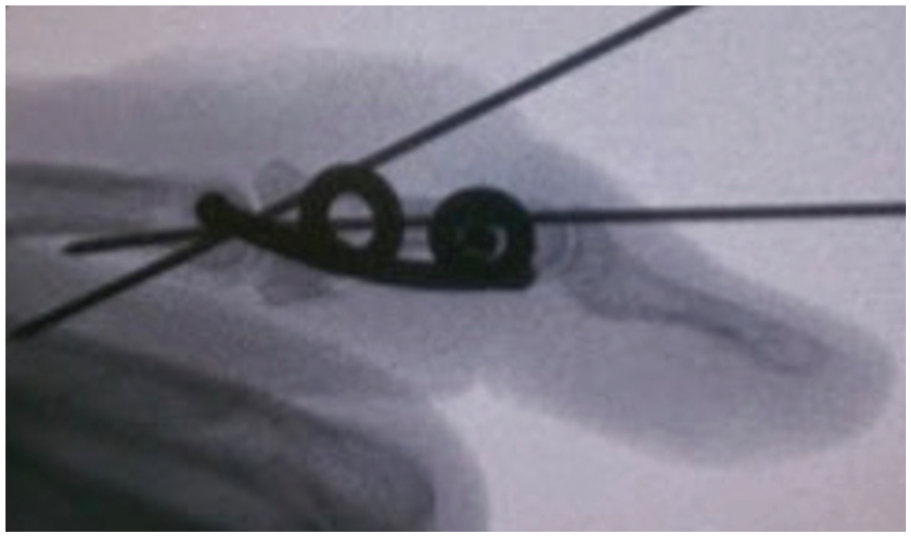
At this time, fluoroscopy is used to confirm that the implant appropriately fits the joint and the proximal and middle phalanx (Figure 5). The temporary fixation 0.028 wires are removed. Stability is tested, and sagittal plane views are taken in flexion and extension to ensure congruent joint motion. The skin is closed, and a sterile dressing is applied.
Lateral fluoroscopy of the internal joint stabilizer after removal of Kirschner wire provisional fixation.
We encourage early active and passive ROM of the injured digit with a goal of 90 or more degrees of motion. We will frequently buddy strap the injured digit to the adjacent digit. Removal of the stabilizer is scheduled no sooner than 3 months postoperatively but can be delayed until the patient returns to a near-normal ROM. Hand therapy is often an integral component of the recovery course.
Removal is scheduled as an outpatient surgery under local anesthesia. The operative incision is reused (Figure 6). The stabilizer is removed, often by cutting it into segments to preserve the dorsal sensory nerve branch.

Intraoperative image of the internal joint stabilizer at the time of device removal.
Results
Seven patients (5 men, 2 women) met the inclusion criteria. The mean age of the patients was 51 (range: 24-72) years. All patients were enrolled in early postoperative hand therapy. Individual patient results are displayed in Table 1. The mean follow-up was 29 (range: 11-72) months. The mean time from injury to surgery was 27 days. The mean preoperative PIP ROM was 0°. At the final follow-up after the removal of the stabilizer, the mean PIP joint ROM was 81° with a mean lower arc of 8° and a mean upper arc of 88°. The device was removed at a mean of 3 months after implantation. There were no reported infections, hardware failure/loosening, and no unplanned returns to the operating room. To our knowledge, no patients underwent reconstruction or other salvage procedures at later dates for their injured PIP joints.
Individual Patient Data for an Internal Joint Stabilizer Used for Unstable Fractures of the Base of the Middle Phalanx.
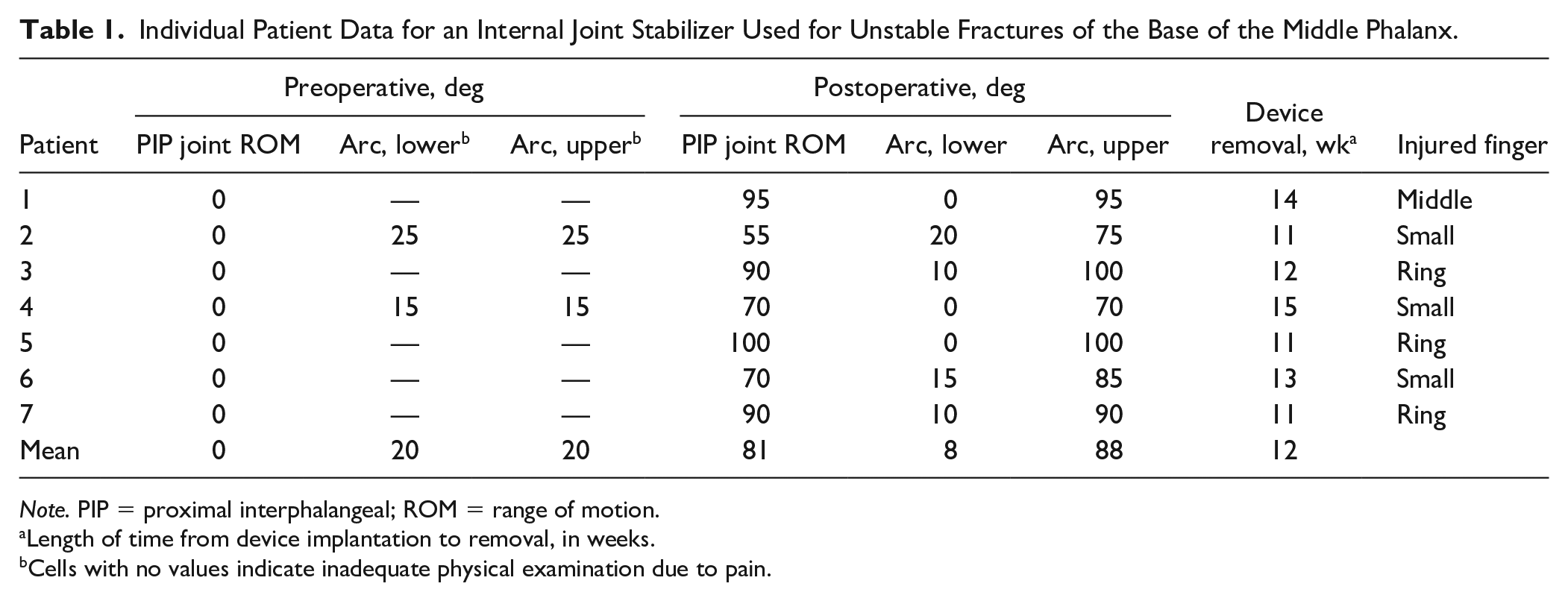
Note. PIP = proximal interphalangeal; ROM = range of motion.
Length of time from device implantation to removal, in weeks.
Cells with no values indicate inadequate physical examination due to pain.
Discussion
Despite the wide variety of techniques and devices, complex unstable fractures of the base of P2 remain a challenge for hand surgeons. The goals of surgical treament are to restore joint congruity which allows return of native kinematics and to provide stability in order to withstand the forces of early mobilization.17,18 Fracture comminution is often associated with these injuries and may preclude stable internal fixation. In addition, there is a reduced risk of infection and other forms of pin tract complications that are common with external fixation. The internal joint stabilizer provides stability and allows immediate ROM, which is a crucial component for a successful outcome. This treatment options has utility across a wide spectrum of injury patterns involving the PIP joint. Contraindications for this method include tenuous soft tissue envelope and infection.
The results of this study are comparable to results reported for external fixation in PIP fracture-dislocations. Badia et al reported a series of six patients who were treated with a dynamic external fixator. 17 The PIP ROM was 5° to 89° at a mean follow-up of 24 months. There were two early pin tract infections. Sastravaha et al presented an alternative external fixator that used a syringe to maintain distraction force. 19 Across 13 patients, the mean PIP ROM of 89° (range: 70°-104°) at a mean follow-up of six months. One patient developed a pin tract infection and underwent debridement with removal of the fixator. Inanami et al treated four patients with a small dynamic external finger fixator following acute unstable fracture-dislocation. 20 At a mean follow-up of 21 months, the mean PIP ROM was 88°.
A limitation of our study is the retrospective design with short-term follow-up and no case-control. It is reasonable to suggest that patients with less satisfactory outcomes may have been lost to follow-up. The internal joint stabilizer requires a subsequent procedure for device removal which has economic cost and the potential for morbidity. These factors should be discussed with the patient. In addition, the learning curve for this novel device may lengthen the procedure time of early cases due to device construction and placement.
We present an internal joint stabilizer as a novel treatment method for unstable base of P2 fractures that provides restoration of joint congruity and allows early postoperative motion while avoiding some of the complications associated with other means of treatment.
Footnotes
Acknowledgements
We appreciate the support of Saffet Guleryuz, MD.
Ethical Approval
This study was approved by our institutional review board (IRB 1-1504538-1).
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.L.O. discloses patents 8506606 and 8608741 issued to Skeletal Dynamics, LLC. The other authors declare no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.