
Abstract
Background:
Unconscious bias of the clinician favors the diagnosis of carpal tunnel syndrome (CTS) in patients with median paresthesia. We hypothesized that more patients in this cohort would be diagnosed with proximal median nerve entrapment (PMNE) by strengthening our cognitive awareness of this alternative diagnosis. We also hypothesized that patients with PMNE may be successfully treated with surgical release of the lacertus fibrosus (LF).
Methods:
In this retrospective study, cases of median nerve decompression at the carpal tunnel and in the proximal forearm for the 2-year periods before and after adopting strategies to mitigate cognitive bias for CTS were enumerated. Patients diagnosed with PMNE and treated by LF release under local anesthesia were evaluated to determine surgical outcome at minimum 2-year follow-up. Primary outcome measures were changes in preoperative median paresthesia and proximal median-innervated muscle strength.
Results:
There was a statistically significant increase in PMNE cases identified after our heightened surveillance was initiated (z = 3.433, P < .001). In 10 of 12 cases, the patient had previous ipsilateral open carpal tunnel release (CTR) but experienced recurrent median paresthesia. In 8 cases evaluated an average of 5 years after LF release, there was improvement in median paresthesia and resolution of median-innervated muscle weakness.
Conclusions:
Owing to cognitive bias, some patients with PMNE may be misdiagnosed with CTS. All patients with median paresthesia, particularly those with persistent or recurrent symptoms after CTR, should be assessed for PMNE. Surgical release limited to the LF may be an effective treatment for PMNE.
Keywords
Introduction
The lacertus fibrosus (LF) has long been considered one of several potential anatomic sites of proximal median nerve entrapment (PMNE). Since the first report by Laha et al in 1978, 1 other single cases2,3 and case series4,5 have implicated the LF as the cause of nerve compression in the documented cases. However, 2 other common sites of PMNE are between the heads of the pronator teres and at the fibrous arch of the flexor digitorum superficialis (FDS), 6 while anatomic anomalies such as Struthers ligament 7 or the Gantzer muscle 8 may also be impinging structures. As it may be difficult to identify the exact location of compression preoperatively, many authors9 -12 prefer comprehensive nerve release at all potential entrapment sites when surgical decompression for PMNE is indicated.
This common wisdom was challenged in 2013 when Hagert 13 showed consistently favorable outcomes in a prospective study of 44 patients with PMNE who were treated with division of the LF alone. The report implied that nerve compression at the LF is the essential lesion in PMNE and that nerve release at other potential sites of compression may not be necessary. Moreover, as this patient cohort was identified during a 1-year period, the paper suggested that the prevalence of PMNE may be underestimated. The cognitive bias of hand surgeons evaluating patients with median paresthesia favors diagnosis of the more prevalent carpal tunnel syndrome (CTS) rather than PMNE, particularly if examination is limited to confirmatory tests for CTS. 14
The primary objectives of this study were to describe our recent experience with PMNE and to report patient outcomes after median nerve decompression limited to release of the LF. We hypothesized that an increased cognitive awareness during diagnostic formulation would improve recognition of PMNE among patients presenting with median paresthesia, including those with persistent or recurrent symptoms after carpal tunnel release (CTR). We also hypothesized that symptomatic median neuropathy in this patient cohort would improve after lacertus release.
Materials and Methods
This was a retrospective therapeutic outcomes study in the community-based practice of a fellowship-trained orthopedic upper extremity specialist. The research proposal was approved by the governing institutional review board. All patients who enrolled in the study provided written informed consent before outcome data were collected.
Clinical Diagnosis
On October 1, 2015, we modified our diagnostic approach to patients presenting with median nerve paresthesia to mitigate cognitive bias for CTS. Debiasing strategies 14 included keeping alternative diagnoses in mind, performing proximal median nerve provocations, and assessing median-innervated muscle strength during the evaluation. The heightened scrutiny was applied not only to those with primary paresthesia, but also to patients with recurrent median paresthesia after previous CTR.
The diagnosis of PMNE at the LF was based on the following clinical triad: (1) median paresthesia associated with hand or forearm weakness; (2) positive lacertus compression test at the elbow flexion crease which reproduced the patient’s median paresthesia and subjective complaints of extremity pain and/or weakness; and (3) demonstrable weakness of the median-innervated flexor carpi radialis (FCR), index flexor digitorum profundus (FDP), and/or flexor pollicis longus (FPL). Patients may also have numbness of the thenar eminence innervated by the palmar cutaneous branch of the median nerve, also helping to distinguish PMNE from CTS. The scratch collapse test 15 and electrodiagnostic evaluations were not used to establish the diagnosis.
Patient Selection
The practice database of the senior author was screened to determine the number and site of median nerve decompressions for the 2-year periods before and after heightened surveillance for PMNE was started. Thus, the 4-year period from October 2013 to September 2017 was studied. The pertinent International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes for CTS and PMNE were 354.0 and 354.1, respectively, whereas the ICD-10 codes were G56.0x and G56.1x, respectively. The Current Procedural Terminology codes for CTR and proximal median nerve decompression were 64721 and 64708, respectively.
Inclusion in our study required the diagnosis of PMNE at the LF, treatment with lacertus release under wide awake local anesthesia no tourniquet (WALANT) technique, and a minimum 2-year follow-up. We chose to recommend only proximal median nerve decompression even in patients with double crush syndrome, 16 so that clinical improvement could be attributed solely to nerve decompression at the LF. Patients who had concomitant lacertus release and CTR were excluded from the study.
Anesthetic and Surgical Technique
The procedure is accomplished using WALANT technique as previously described by Hagert.13,17 Local anesthesia without IV sedation is sufficient for this minimally invasive surgery. Furthermore, with the patient fully awake and alert and with uninterrupted blood flow to the tourniquet-free extremity, the surgeon may confirm return of FCR, index FDP, and FPL strength after division of the LF during or immediately following the procedure.
While lying supine in the preoperative holding venue, the patient’s anteromedial arm is anesthetized using 15 to 20 mL of standard 1% lidocaine (10 mg/mL) with 1:100 000 epinephrine (10 mcg/mL), staying well below the maximum lidocaine dose of 7 mg/kg body weight. Injection through a long 27-gauge needle by tumescent technique begins at the medial elbow flexion crease and advances centrally and proximally toward the biceps and distally over the LF. The anesthetic is administered a minimum of 25 minutes before making the surgical incision to permit vasoconstriction sufficient to minimize intraoperative bleeding. 18
After the anesthetic has set up, the patient is taken to the procedure room and placed supine on the operating table. The affected extremity is prepped and draped and supported on an adjacent hand table with the forearm fully supinated. The surgeon is seated on the medial side of the extremity and uses loupe magnification for the procedure.
A 3 to 4 cm transverse skin incision is made in the medial elbow flexion crease. The subcutaneous layer is dissected with care, preserving branches of the medial antebrachial cutaneous nerve. The distal biceps tendon and lateral-to-medial extent of the LF are identified. An 18-gauge IV catheter sans needle is positioned beneath the medial border of the LF to introduce 5 mL of 1% lidocaine with epinephrine to desensitize the median nerve. A Freer elevator is placed deep to the LF which is then divided transversely using a 69 Beaver blade with care taken to avoid injury to the distal biceps, brachial artery, or median nerve. After releasing the LF, the median nerve is palpated to confirm the absence of distal compression sites.
The wound is closed with 4-0 or 5-0 absorbable subcutaneous suture, and a soft compression dressing is applied. Immediate elbow motion is permitted, but heavy lifting and sports activities are restricted for 4 to 6 weeks.
Outcome Measures
Demographic and disease-specific clinical data were extracted from the electronic medical records of all patients eligible for study. Primary outcome parameters were improvement in preoperative median paresthesia and median-innervated muscle strength. Secondary outcome assessments included patient satisfaction and scores on validated patient-reported outcome measures. Postoperative complications and the need for secondary surgery after the lacertus release were also documented.
Eligible patients were contacted by telephone and recruited to participate in the study. Volunteers provided informed consent and were compensated for their time and travel expenses with a modest stipend. Questionnaires were administered to quantify median paresthesia and extremity pain on a 0 to 10 visual analog scale (VAS) where 0 was asymptomatic. Patient satisfaction with surgical outcome and willingness to recommend the procedure was also assessed on a 0 to 10 VAS where 10 was the most favorable response. Physical examination of both upper extremities focused on static 2-point discrimination in the median nerve distribution, median nerve compression provocations at the wrist and elbow, and median-innervated muscle strength, 19 including FCR strength on resisted wrist flexion, index FDP strength on resisted distal interphalangeal joint flexion, and FPL strength on resisted thumb interphalangeal joint flexion. The short-version Disabilities of the Arm, Shoulder, and Hand (QuickDASH) 20 and Patient-Rated Elbow Evaluation (PREE) 21 were also administered to the study participants.
Statistical Analysis
Data were compiled and analyzed in an electronic database system. Standard descriptive statistics were calculated and used to characterize the study cohort. The 2-proportion z test was used to determine if there was a statistically significant difference in the number of PMNEs identified before and after implementing CTS debiasing strategies. The level of statistical significance was set at P < .05 for a 2-tailed test.
Results
During the 2-year period after adopting CTS debiasing strategies, there were 189 median nerve decompressions, including 176 CTRs, 12 lacertus releases, and 1 two-level decompression (Table 1). During the preceding 2-year period, there were 165 median nerve procedures, all of which were CTRs. Applying the z test, this difference in case type was statistically significant (z = 3.433, P < .001). Thus, it appears that increased awareness of cognitive bias regarding CTS improves recognition of PMNE.
Median Nerve Decompressions Before and After Heightened Surveillance.
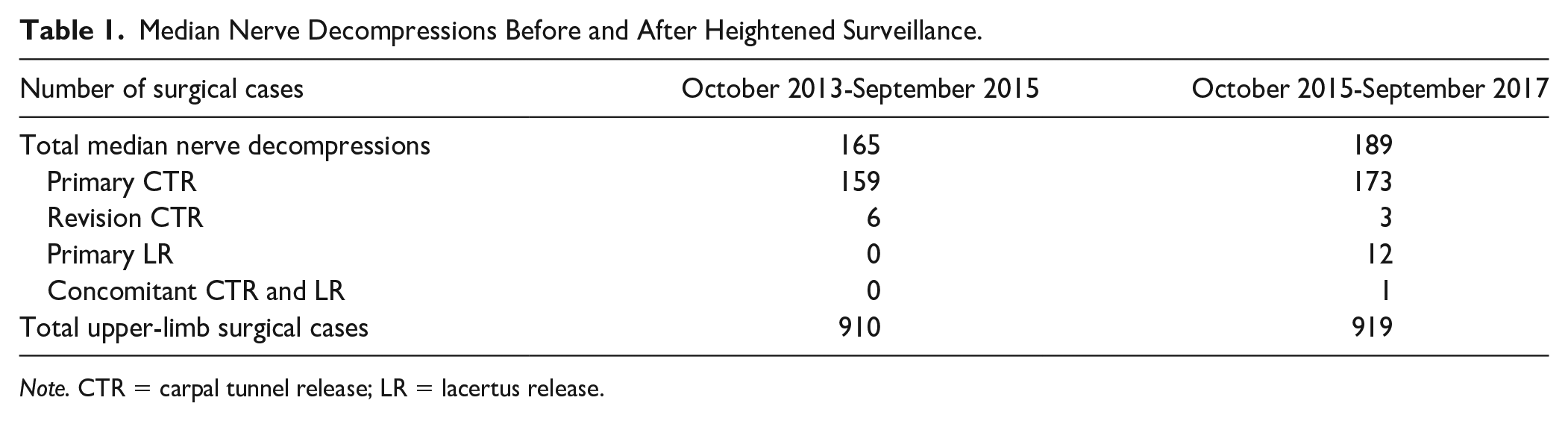
Note. CTR = carpal tunnel release; LR = lacertus release.
Demographics, clinical presentation, and operative data derived from the medical records of the 10 patients (12 limbs) meeting study inclusion criteria are summarized in Table 2. Details for each case are provided in Supplemental Table S1. The cohort had mean age of 53 years and was comprised of 4 men and 6 women. Two of the women had bilateral PMNE at the LF for which they underwent staged lacertus releases. Seven patients (8 limbs) were enrolled in the study, 2 were unable to participate, and 1 was lost to follow-up. One patient with double crush syndrome underwent concomitant lacertus release and CTR (Table 1) and was excluded from the study.
Patient Demographics, Clinical Presentation, and Operative Findings (10 Patients, 12 Limbs).
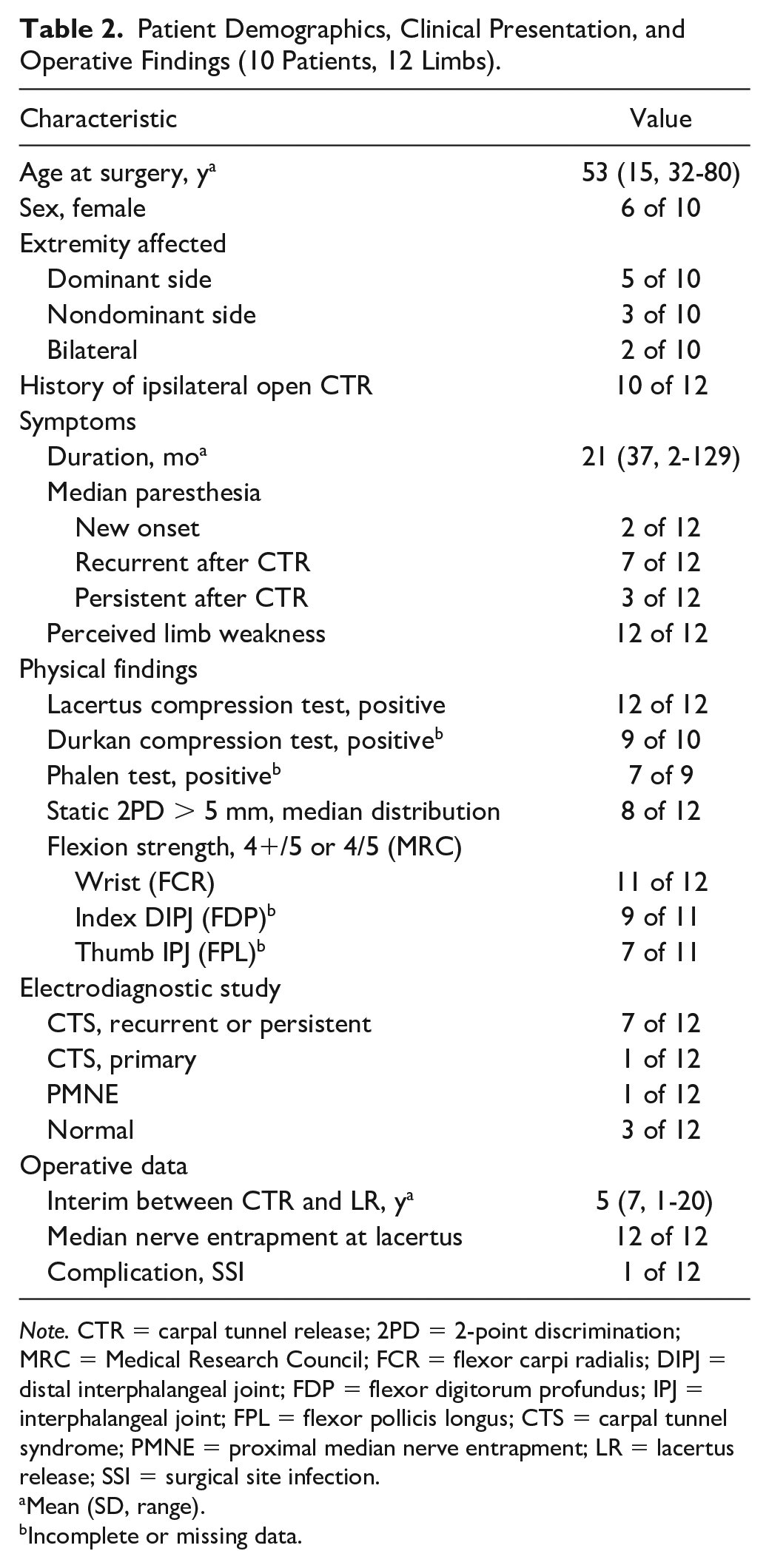
Note. CTR = carpal tunnel release; 2PD = 2-point discrimination; MRC = Medical Research Council; FCR = flexor carpi radialis; DIPJ = distal interphalangeal joint; FDP = flexor digitorum profundus; IPJ = interphalangeal joint; FPL = flexor pollicis longus; CTS = carpal tunnel syndrome; PMNE = proximal median nerve entrapment; LR = lacertus release; SSI = surgical site infection.
Mean (SD, range).
Incomplete or missing data.
At presentation, all patients complained of median paresthesia associated with weakness of the hand and/or forearm, and some reported extremity pain. On physical examination, all patients demonstrated a positive proximal median nerve compression test at the elbow flexion crease over the LF which reproduced their symptoms (Figure 1). Also, all patients except 1 had weakness of median-innervated muscles on manual resistive testing. These clinical features suggested PMNE at the LF as the primary diagnosis, although some with positive provocative signs at the wrist may have had primary or recurrent CTS as a secondary diagnosis. Patients understood that open CTR would be offered to those still symptomatic after lacertus release. As only 1 patient in the study cohort had electrodiagnostic findings consistent with PMNE (Supplemental Table S1), electrodiagnostic tests were not helpful confirming this clinical diagnosis.

Proximal median nerve compression test, right elbow. With the elbow flexed 70°, the examiner’s right thumb compresses the median nerve beneath the leading edge of the lacertus fibrosus at the elbow flexion crease.
Among the 12 limbs treated, there were only 2 cases of primary PMNE. In 10 cases, the patient had previous ipsilateral open CTR, but experienced persistent symptoms (3 cases) or recurrent median paresthesia (7 cases) associated with extremity weakness from months to, in some cases, years after the index surgery. In this subgroup of patients, considered to have double crush syndrome of the median nerve, the average time between the CTR and lacertus release was 5 (range = 1-20) years. In all 12 limbs under study, tight entrapment of the median nerve at the LF was found at the time of nerve decompression. In 7 of 12 cases, the LF was also noted to be thickened. No other anatomic site of PMNE was identified in the study cohort.
The surgical outcome evaluations of 7 patients (8 limbs), completed an average of 5 years after lacertus release, are summarized in Table 3 and detailed in Supplemental Table S2. Focusing on our primary outcome measures, median paresthesia was better in all cases, being resolved in 4, greatly improved in 3, and somewhat improved in 1. Similarly, weakness of the median-innervated muscles observed preoperatively was resolved at the follow-up examination in all cases. Regarding our secondary outcome measures, VAS scores for patient satisfaction and willingness to recommend the procedure to others were favorably high, while the 0 to 100 disability scale QuickDASH and PREE scores were favorably low. Taken together, these results suggest that PMNE improves with surgical release of the LF.
Outcome Data (7 Patients, 8 Limbs).
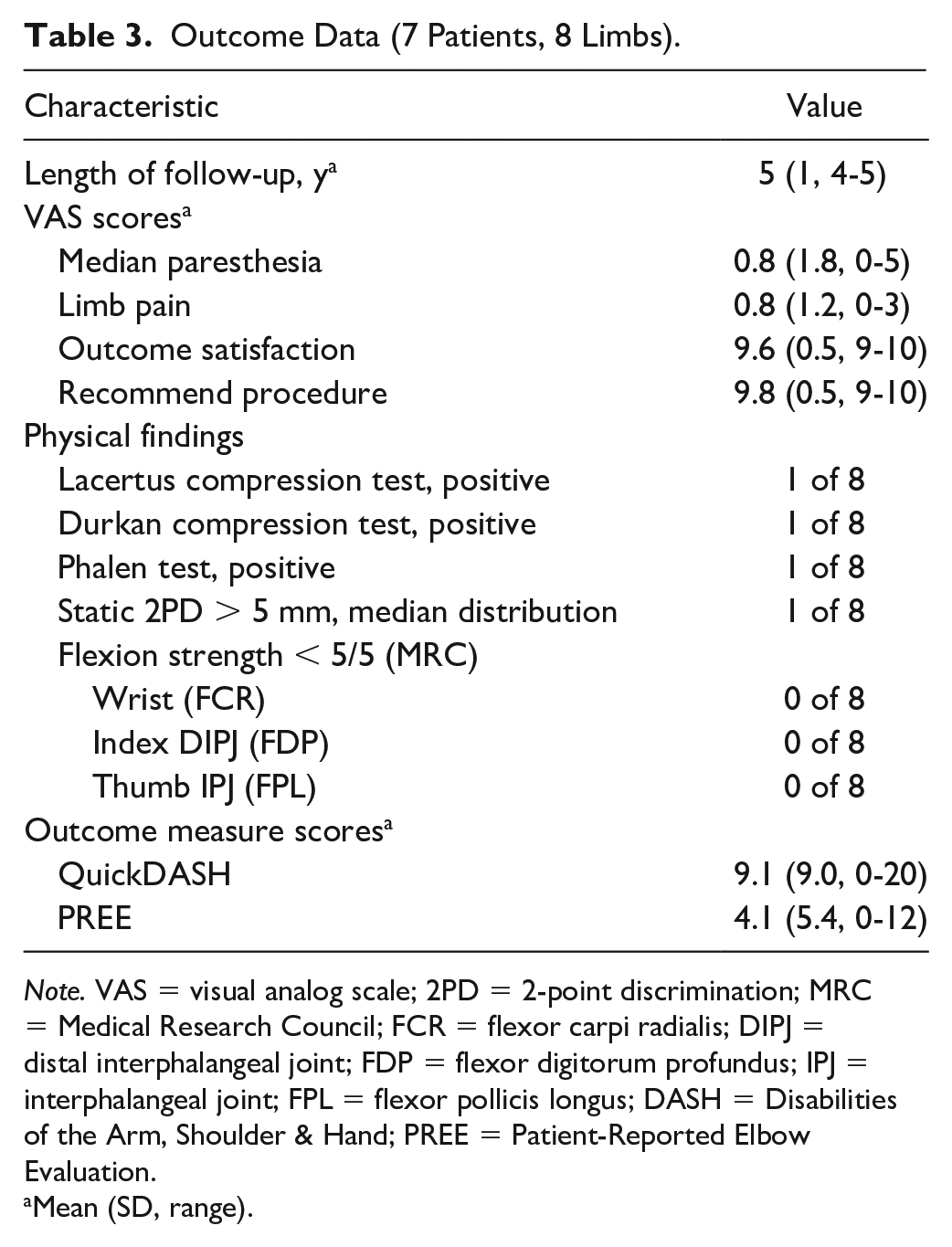
Note. VAS = visual analog scale; 2PD = 2-point discrimination; MRC = Medical Research Council; FCR = flexor carpi radialis; DIPJ = distal interphalangeal joint; FDP = flexor digitorum profundus; IPJ = interphalangeal joint; FPL = flexor pollicis longus; DASH = Disabilities of the Arm, Shoulder & Hand; PREE = Patient-Reported Elbow Evaluation.
Mean (SD, range).
Surgical site infection in 1 patient resolved after wound debridement and oral antibiotics. There were no other complications related to lacertus release. During the study, 1 patient diagnosed with double crush syndrome experienced partial symptomatic relief after lacertus release. In accordance with our surgical plan, she underwent staged CTR 3 weeks after the index procedure with complete resolution of symptoms. Two patients with symptomatic improvement after lacertus release subsequently experienced recurrent median paresthesia and were treated elsewhere with revision CTR, one with partial improvement and the other without relief of symptoms.
Discussion
For years, our experience with PMNE was similar to others10,22 because we infrequently made the diagnosis and rarely indicated patients for nerve decompression. Thus, we were surprised to find numerous cases of PMNE during the 2-year period after heightened surveillance in the present study. An explanation for this finding requires understanding medical heuristics or subconscious short-cuts in diagnostic reasoning and how they may predispose to diagnostic error.
When evaluating a patient with median paresthesia, the examiner promptly formulates the diagnostic hypothesis of CTS, the most prevalent cause of the symptom. However, rather than considering alternative diagnoses at this point, the clinician may commit the most common cognitive error in data synthesis by prematurely concluding (premature closure) 23 that CTS is the correct diagnosis. Notably, experienced practitioners are as vulnerable to premature closure as are their junior colleagues. 24 Further increasing the likelihood of diagnostic error, the physician may then exhibit confirmation bias14,25 by seeking additional data (physical findings or electrodiagnostic studies) which confirm the diagnostic hypothesis, while excluding disconfirming data (such as proximal median nerve provocations). Most cognitive errors occur in cases when clinicians are confident of the diagnosis, such as CTS, rather than in more challenging cases when the diagnosis is uncertain. 25 Thus, surgeons are cautioned to avoid the pitfalls of premature closure and confirmation bias and should routinely include disconfirming examination maneuvers when evaluating patients with median paresthesia.
Our study also found that lacertus release using the WALANT technique was an effective treatment for PMNE, improving median paresthesia and median-innervated muscle strength in the cohort studied. We agree with Hagert 13 who opined that the LF is the most prominent and consistent structure compressing the median nerve at the elbow. To the contrary, others9,11,26 have reported that PMNE may occur not only at the LF but also at the pronator teres or the FDS arch. Nerve compression at more than 1 location in the proximal forearm has also been observed. However, in another case series, Olehnik et al 27 attributed none of their PMNE cases to the LF.
Also known as the bicipital aponeurosis, the LF is a 3-layer fixed-length fibroaponeurotic expansion originating from both long and short heads of the biceps proximal to the distal biceps tendon. 28 The aponeurosis extends distally across the antecubital fossa passing superficial to the median nerve and brachial artery, inserting onto radial and ulnar aspects of the proximal ulna after encircling the forearm flexors. When these forearm muscles contract, tension develops in the aponeurosis pulling the forearm flexors proximally and the biceps medially. If resisted elbow flexion with the forearm supinated reproduces median paresthesia and forearm weakness, PMNE beneath the taut LF should be suspected. 26 Lacertus release has not only been reported to relieve neurologic symptoms,1 -5,13 but also activity-related forearm claudication due to brachial artery impingement at the thick leading edge of the aponeurosis. 29
Two recent cadaver studies also implicated the LF in PMNE. One study of 36 upper-limb specimens 30 found that the bicipital aponeurosis crossed the median nerve at mean 1.5 ± 0.6 cm distal to the humeral bi-epicondylar line, thereby localizing the leading edge to the elbow flexion crease. In 15 of the 36 cadaver arms (42%), the nerve was in direct contact with the LF. Dissecting 55 cadavers, Caetano et al 31 reported the length of the bicipital aponeurosis from origin to insertion ranged from 4.5 to 6.2 cm and the width varied from 0.5 to 2.6 cm. In 42 of 55 limbs (76%), the aponeurosis was thickened, while in 27 cases (49%), the nonyielding fascial band was resting directly on the nerve. Thus, from an anatomic standpoint, the LF may impinge on the median nerve near the elbow flexion crease, particularly in the elbow-flexed position. Anatomic anomalies of the bicipital aponeurosis32,33 may also contribute to proximal median neuropathy.
As in the Hagert study, 13 we localized PMNE in our cohort to the LF primarily by demonstrating weakness of median-innervated muscles preoperatively. Early median compression neuropathy at the elbow which may be subclinical involves the superficial anteromedial fascicules, which provide motor innervation of FCR, index FDP, and FPL. With disease progression, the deeper sensory fascicules are compressed giving rise to clinically significant median paresthesia typically associated with CTS, but in addition, thenar eminence numbness owing to involvement of the palmar cutaneous branch fibers. Our secondary indicator of entrapment at the LF was a positive lacertus compression test which reproduced the patient’s median paresthesia and subjective complaints of extremity pain and/or weakness. In our hands, nerve compression at the elbow flexion crease medial to the distal biceps is a reliable provocative test for PMNE by the LF (Figure 1). Like other investigators,6,10,34 we have not found electrodiagnostic evaluation to be a useful diagnostic tool for PMNE.
Our study demonstrated a high prevalence of CTS in this small cohort of patients with PMNE. There was previous CTR in 10 of 12 cases and primary or revision CTR in 3 patients after the lacertus release in our study. In the context of recent literature, these findings are not surprising. For instance, El-Haj et al 12 reported CTS in 23 of 27 patients with PMNE, and Binder et al 35 observed new-onset CTS in 3 of 12 patients within 2 years of proximal median nerve decompression. Also, the prevalence of PMNE in patients with median paresthesia presumed to be CTS may be underestimated. In a retrospective review of median nerve compression, Hsiao et al 36 found double crush of the median nerve at the carpal tunnel and proximal forearm in 21 of 343 cases (6%). Taken together, these data suggest that PMNE should always be considered in patients with median paresthesia, particularly in those with persistent or recurrent paresthesia after CTR.
When clinical findings suggest median nerve entrapment at both the wrist and elbow, most authors12,36 -38 recommend concomitant CTR and proximal median nerve decompression. Both procedures may be completed at the same operative setting using WALANT technique 38 to minimize recovery time and morbidity.
Limitations of this study include small cohort size and incomplete clinical database, as preoperative QuickDASH and PREE scores were not available for comparison and only 7 of 10 patients were available for follow-up evaluation. Furthermore, as these encounters were not blinded, examiner bias may have influenced the outcomes data. There was also no control group for comparison. Last, owing to the possibility of double crush syndrome, the observed clinical improvement may not be entirely attributable to lacertus release in all cases.
Conclusions
Appreciating the cognitive bias influencing diagnostic reasoning permitted us to identify significantly more cases of PMNE in patients with median paresthesia. Our study confirmed previous reports12,36 that PMNE may occur in isolation or may coexist with CTS. All patients with median neuropathy, but particularly those with persistent or recurrent symptoms after CTR, should be evaluated for PMNE.
In our study cohort, the diagnosis of PMNE was based on clinical grounds which included demonstrable weakness of the FCR, index FDP, and/or FPL and a positive proximal median nerve compression test at the elbow flexion crease over the LF. Patients were treated with isolated lacertus release using the WALANT technique. At mean 5-year follow-up, patient outcomes showed improvement in median paresthesia, resolution of median-innervated motor weakness, high patient satisfaction, and favorable mean QuickDASH and PREE scores suggesting that lacertus release may be effective treatment for PMNE.
Supplemental Material
sj-docx-1-han-10.1177_15589447231153233 – Supplemental material for Experience With Proximal Median Nerve Entrapment by the Lacertus Fibrosus
Supplemental material, sj-docx-1-han-10.1177_15589447231153233 for Experience With Proximal Median Nerve Entrapment by the Lacertus Fibrosus by Justin A. Cline, Lisa M. Frantz, Jessica M. Adams and Bernard F. Hearon in HAND
Supplemental Material
sj-docx-2-han-10.1177_15589447231153233 – Supplemental material for Experience With Proximal Median Nerve Entrapment by the Lacertus Fibrosus
Supplemental material, sj-docx-2-han-10.1177_15589447231153233 for Experience With Proximal Median Nerve Entrapment by the Lacertus Fibrosus by Justin A. Cline, Lisa M. Frantz, Jessica M. Adams and Bernard F. Hearon in HAND
Footnotes
Acknowledgements
The authors gratefully acknowledge Rosalee E. Zackula, MA, research statistician at the University of Kansas School of Medicine Wichita, for her assistance with statistical analysis.
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by the institutional review board overseeing all human subjects research at our university.
Statement of Human and Animal Rights
Compilation and analysis of all subject-protected health information was done in accordance with the guidelines published in the Health Insurance Portability and Accountability Act of 1996.
Statement of Informed Consent
Before participating in this study, all subjects provided written informed consent as approved by our university institutional review board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.