
Abstract
Background:
Revision of radial head arthroplasty (RHA) may be indicated in cases of prosthesis loosening and malposition. Inherent difficulties in revision surgery include poor bone stock and disrupted soft tissue envelope. Although cases of RHA used for revision of failed RHA are rare, there is reasonable expectation for increasing frequency of these cases due to the increasing incidence of primary RHA. Furthermore, there is an increasing demand for postoperative recovery of function; thus, surgeons may consider revising a failed RHA to a new RHA. We report on series of failed RHA which were revised to a new radial head prosthesis.
Methods:
A retrospective review was performed at multiple institutions for a single radial head prosthesis used for revision of a failed radial head prosthesis. Clinical and radiographic outcomes were collected with a minimum of 1 year of follow-up.
Results:
Across 11 patients at a mean follow-up of 45.1 months, the mean Mayo Elbow Performance Score was 81.7; mean Disabilities of the Arm, Shoulder, and Hand scores were 24.4; and mean Visual Analog Scale for pain was 0.6. Radiographic analysis yielded no evidence of capitellar wear or stem loosening.
Conclusion:
A radial head prosthesis can produce satisfactory results when used for revision of a failed prosthesis. Inherent difficulties in revision surgery include the potential for reduced bone stock and a disrupted soft tissue envelope. Elements of prosthesis design which may contribute to effectively managing revision surgery include a long stem with in-growth surface and prosthetic head alignment to the axis of forearm rotation.
Keywords
Introduction
The utilization of primary radial head arthroplasty (RHA) is increasing due in part to further understanding of forearm kinematics and improved clinical outcomes.1 -3 Implant innovation and standardization of surgical technique have contributed to the recent success in primary RHA. However, with increasing rates of RHA procedures comes the eventual need to address prosthesis failure with revision surgery.
Options for treating a failed radial head prosthesis include removal of the prosthesis, implantation of a new radial head prosthesis, or interposition arthroplasty. There is increasing evidence for the narrowed indications of radial head excision. 4 Common complications include instability,5,6 malposition and loosening,7,8 degenerative disease of the ulnohumeral joint,9,10 and distal radioulnar joint pathology. 11 Interposition arthroplasty may provide short-term pain relief but has limited application due to lack of durability.12,13
Revision of radial head prostheses may be indicated in cases of prosthesis loosening and malposition, including overstuffing which may lead to stiffness and pain.7,8,14 Inherent difficulties in revision surgery include poor bone stock and disrupted soft tissue envelope.
Although cases of RHA used for revision of failed RHA are rare, there is reasonable expectation for increasing frequency of these cases due to the increasing incidence of primary RHA. Furthermore, there is an increasing demand for postoperative recovery of function; thus, surgeons may consider revising a failed RHA to a new RHA. We report on series of failed radial head prostheses that were revised to a new radial head prosthesis.
Material and Methods
A retrospective review was performed at multiple institutions for cases of failed RHA revised to a new RHA. Inclusion criteria specified a single radial head prosthesis design (Skeletal Dynamics, Miami, Florida) implanted following removal of a failed radial head prosthesis with a minimum of one year of follow up. Cases of primary arthroplasty and cases of revision RHA for failed radial head osteosynthesis were excluded. Additional exclusion criteria were patients younger than 18 years and patients with less than 1 year of follow-up. Data collected included patient age and gender, length of time from the index RHA, and the term of follow-up. Outcome metrics collected include the Mayo Elbow Performance Score (MEPS); Disabilities of the Arm, Shoulder, and Hand (DASH) score; and a Visual Analog Scale for pain at rest (VASr) and during activity (VASa). Radiographs were evaluated for excessive prosthetic length - overstuffing of the joint - evidence of stem loosening, and evidence of capitellar wear.
Surgical Technique
Before incision, the ulnar fovea was identified and marked. If necessary, additional radial neck cuts were performed until anatomical prosthetic length was restored. The trial prosthesis was inserted and evaluated with fluoroscopy to confirm appropriate length, ensuring the joint was not overstuffed. Overstuffing was defined as the prosthetic radial head being proximal to the corner formed by the lesser and greater sigmoid notch on a true anteroposterior view (Figure 1). Proper radial head diameter was confirmed by ensuring that the apex of the capitellum was aligned with the center of the prosthetic radial head. An alignment tool was secured to the radial head proximally and placed on the previously marked ulnar fovea distally. With the forearm in neutral rotation, the prosthetic radial head was aligned to the axis of forearm rotation (Figure 2). The head was then permanently secured to the prosthetic stem, restoring alignment of the axis of forearm rotation.
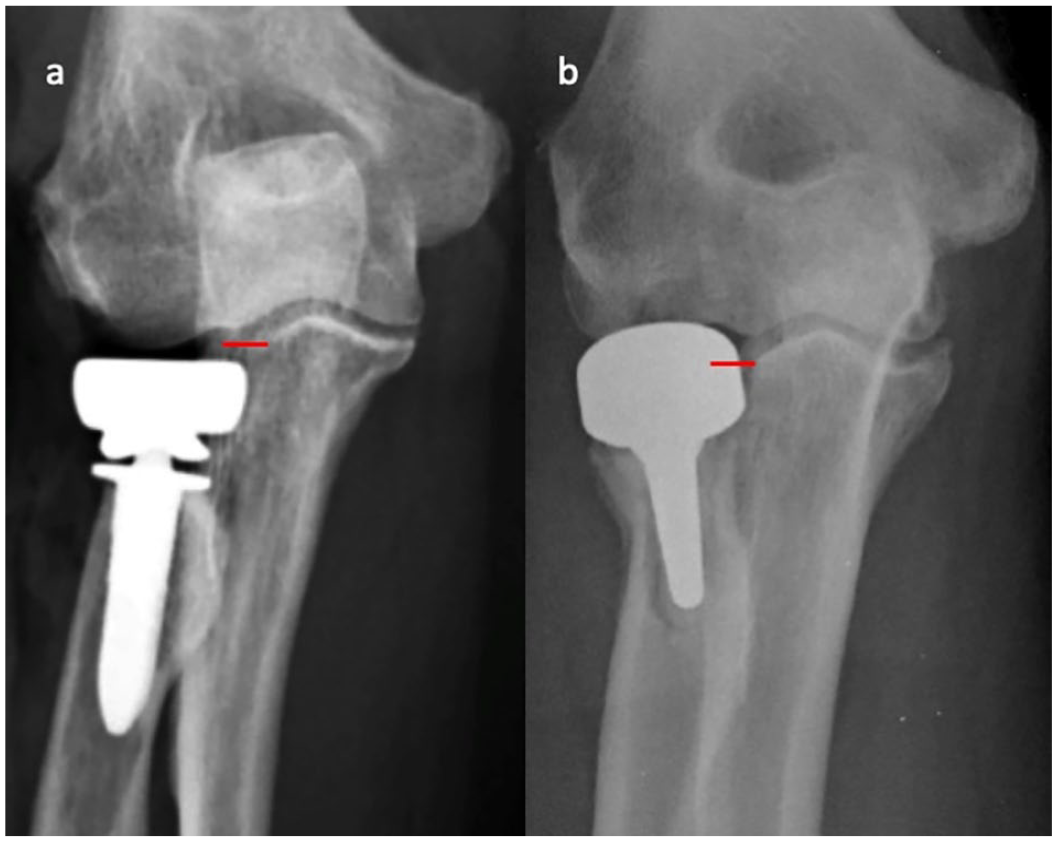
(a) Anteroposterior radiograph of the recommended prosthesis position with the proximal aspect of the head being at or distal to the corner formed by the lesser and greater sigmoid notches (red line). (b) Anteroposterior radiograph of an overstuffed prosthesis with the proximal aspect of the head being proximal to the corner formed by the lesser and greater sigmoid notches (red line).

Intraoperative photograph of the instrument used to align the radial head prosthesis to the anatomical axis of forearm rotation.
Radiographic Measures
Postoperative radiographs were evaluated for capitellar wear, osteolysis, radiolucent lines, and prosthesis loosening. Each radiographic variable was independently graded by 2 fellowship-trained upper extremity surgeons. Stages describing the qualitative appearance of the capitellum were used to evaluate the presence of wear. Stage I showed increased subchondral density. Stage II showed early erosion. Stage III showed substantial, readily apparent erosion. 15 The presence of osteolysis was described based on its position in proximity to the stem. 16 Radiolucent lines were quantitatively described using the method developed by Fehringer et al. 17 A prosthesis was defined as loose when there was a change in position from prior imaging with associated bony effects. 18
Results
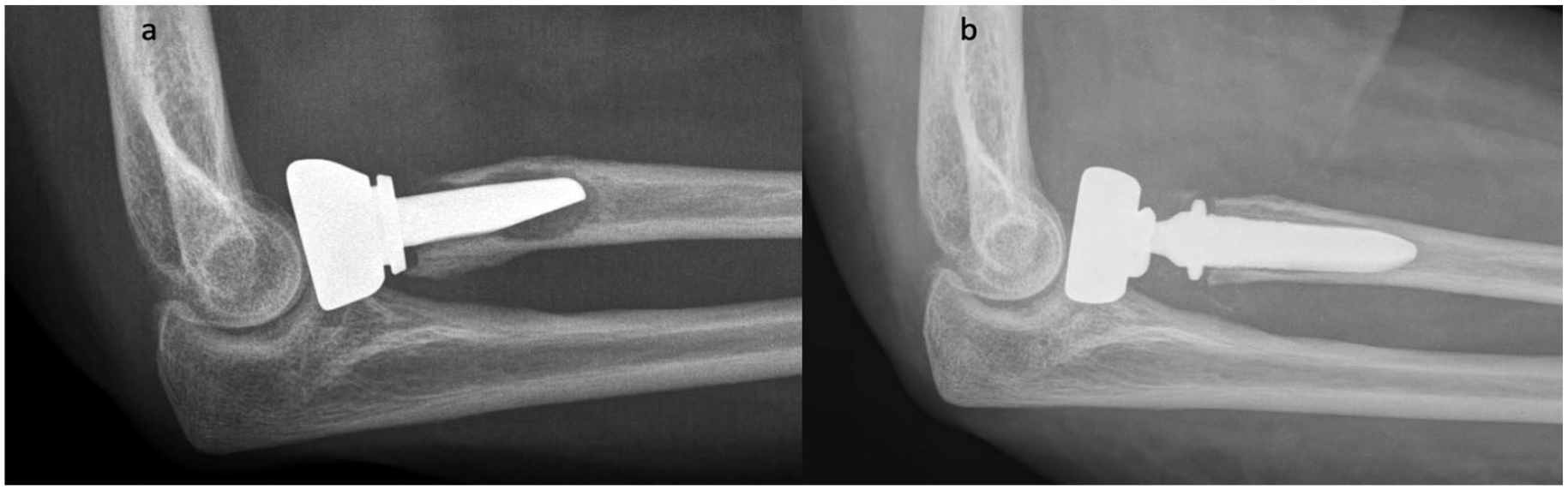
A total of 11 patients were included in this series. Patient variables are detailed in Table 1. Mean follow-up was 45.1 (±29.1) months after the revision procedure. All patients had a minimum of one year of follow-up, three patients (27%) had less than two years, and six patients (55%) had more than 37 months. Revision surgery was performed at a mean of 40.0 (±43.3) months from the index RHA procedure. Five (45%) of the failed prostheses were smooth stems and six (55%) were press-fit stems. Mean MEPS was 81.7 (±14.2), with 88% (7/8) achieving a good score (75-90) per the categorical score values. One patient (9%) was scored as poor (<60). This patient had two prior surgeries for prosthesis overstuffing following the index arthroplasty. Mean DASH scores were 24.4 (±21.6). Mean VASr was 0.6 (±1.1), and mean VASa was 2.8 (±2.4).
Patient Characteristics and Outcome Data for 11 Cases of Failed Radial Head Arthroplasty Which Were Revised to a Single Radial Head Prosthesis.
Note. DASH = Disabilities of the Arm, Shoulder, and Hand score; MEPS = Mayo Elbow Performance Score; VAS = Visual Analog Scale for pain; deg = degrees.
Follow-up term in months.
Radiographic analysis yielded no evidence of capitellar wear and no evidence of stem loosening (Figures 3 and 4). All prostheses were deemed to be appropriately sized and positioned relative to the proximal radioulnar joint. Limited proximal stress shielding was identified in 5 cases (45%) at a mean follow-up of 61.2 (±30.9) months.
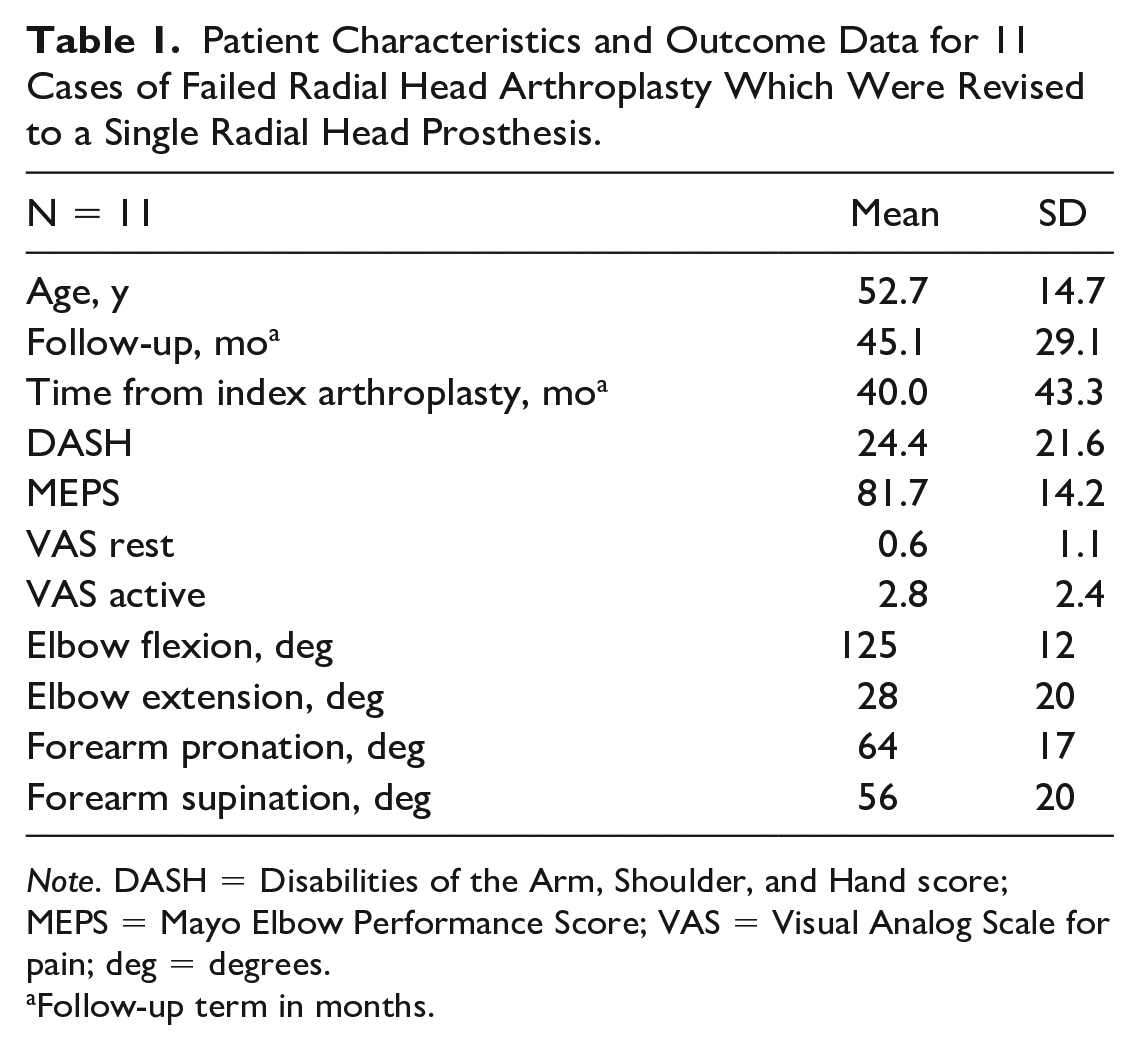
(a) Lateral radiograph of a 46-year-old woman with a failed radial head prosthesis at 9 years after the index arthroplasty, (b) revised with a new radial head prosthesis.
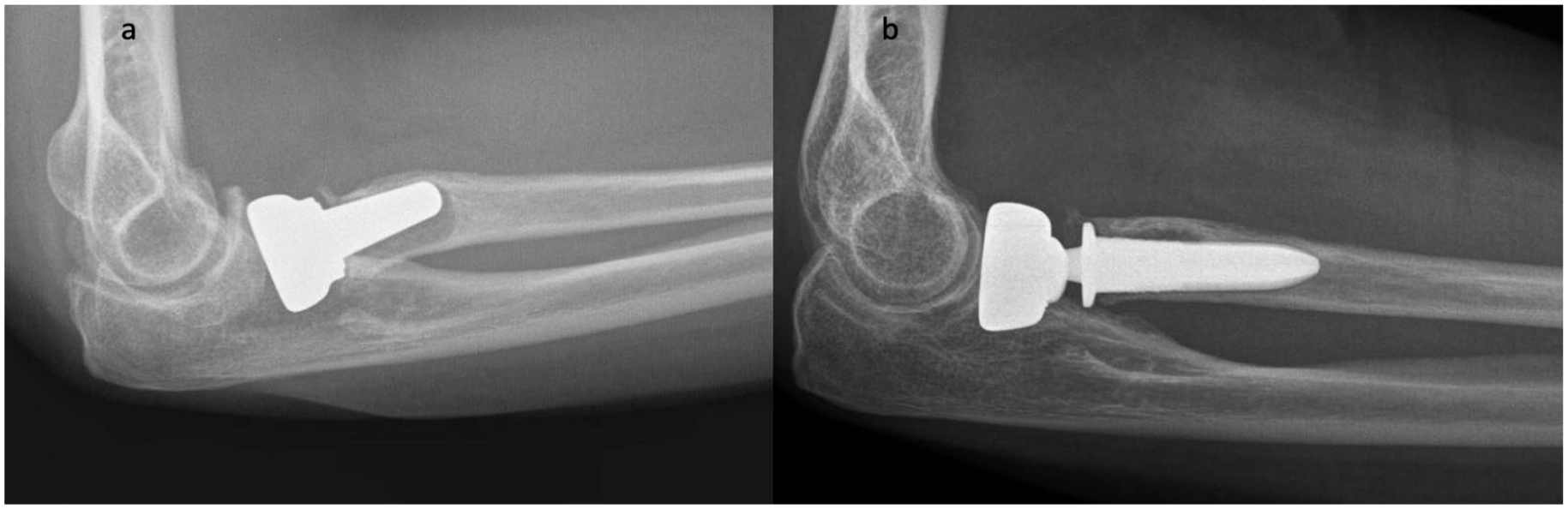
(a) Lateral radiograph of a 54-year-old woman with a failed radial head prosthesis at 4 months after the index arthroplasty, (b) revised with a new radial head prosthesis.
Discussion
Although performed infrequently, revision surgery for failed RHA can be expected to increase with the recent rise in primary RHA.1,19 Improved outcomes in contemporary primary RHA have been attributed to standardization of surgical techniques such as more appropriate prosthesis positioning and sizing.20 -23 Further, improvements in prosthetic design have been indicated as important components in achieving favorable outcomes in primary RHA.14,15,20,24 -26 These variables also have the potential to contribute to improved outcomes after revision RHA.
Across our 11 patients, clinical outcomes were satisfactory for revision of failed RHA with a new RHA. The mean MEPS is comparable to the value reported in a prior study on RHA used for revision, and VAS scores for pain during rest and activity were low. 27 There were no construct failures which were attributed to the implant.
Characteristics of this implant design may contribute favorably to revision arthroplasty. These include a long stem that purchases distal to the bicipital tuberosity, an in-growth surface restricted to the collar and proximal aspect of the stem to mitigate stress shielding, and the ability to align the radial head with the forearm axis of rotation. Reports describe stem loosening as the most common reason for RHA failure. 14 Reduced bone stock is frequently encountered in revision surgery. This may be due to the prior surgical intervention or implant removal. This implant design provides multiple neck length options that allow reconstruction up to 23 mm of proximal bone loss. Compared to a shorter stem, the increased working length of a long stem provides a more robust initial three-point fixation strength and a wider distribution of bone contact. This initial fixation is important to stabilize the stem and allow osseous ingrowth. 28 The value of a long press-fit stem may be more pronounced in the presence of proximal bone loss. 29 Further, long stems are less likely to loosen and develop osteolysis than short stems, 30 and are more stable to transverse forces helping prevent valgus collapse and altered pronosupination mechanics. 31 Finally, well-fixed long stems are more suitable to be used in conjunction with impaction bone grafting techniques. Owing to inherent lack of stability, smooth rotating stems are more likely to result in graft resorption and failure.
The forearm axis of rotation extends from the radial head through the ulna fovea.32,33 When the prosthetic radial head is aligned with this axis, a more native radiocapitellar tracking occurs throughout pronosupination. This reduces capitellar contact stresses and therefore reduces wear on the capitellar surface. Furthermore, stability of the prosthesis is maintained in conjunction with this alignment capability. In revision surgery where stiffness is a common complication, a more physiologic radiocapitellar relationship may afford the opportunity to maximize pain-free range of motion.
Radiographic evidence of proximal radial stress shielding is indicative of robust stem fixation.16,34 -36 Across this small series, 45% of cases demonstrated stress shielding at a mean follow-up of more than 5 years. These changes are emblematic of Wolff’s law that describes bony adaptations due to imposed demands. A well-fixed stem results in reduced loading of the proximal metaphyseal bone resulting in nonprogressive stress shielding. This radiographic finding has been shown to stabilize with time and result in no negative clinical impact.27,36
Avoidable complications still plague radial head surgery.14,26 Although stiffness is a common result of elbow trauma, it may also be a consequence of inappropriate prosthesis position.14,20 Overstuffing refers to prosthetic lengthening of the proximal radius. Additional length can increase radiocapitellar contact pressure, which contributes to accelerated capitellar wear.9,24 Alterations in radiocapitellar tracking can also affect ulnohumeral pressures, which can lead to degenerative pathology.20,37 These avoidable complications may be addressed with improved prosthesis design and standardization of surgical technique.
As our understanding of forearm kinematics has improved, excision of the radial head is performed within more narrowed indications. When compared with primary excision, radial head excision performed as a secondary procedure has demonstrated inferior results with low satisfaction and continued pain. 38 Radial head excision substantially increases tension on the central band of the forearm interosseous ligament which may lead to attritional failure and subsequent proximal migration of the radius. This can result in ulnocarpal abutment at the wrist and dysfunctional forearm kinematics. 39 Additionally, radial head excision eliminates the support against transverse forearm forces, which can result in impingement of the proximal radial stump onto the ulna. 40
Limitations of our work include its retrospective nature and the small sample size due in part to the infrequency of revision RHA. The follow-up term was highly variable, with three patients having less than two years of follow-up. Additionally without baseline scores, we were unable to demonstrate the magnitude of the clinical improvement after revision arthroplasty. Strengths of this work include the aggregation of data across multiple institutions and surgeons. Multiple surgeons represent a broad spectrum of experience and skill. These characteristics improve the generalizability of the findings. The results of a single implant improves our understanding of this design but may not be transferable to other designs.
In conclusion, a radial head prosthesis can produce satisfactory results when used for revision of a failed prosthesis. Inherent difficulties in revision surgery include the potential for reduced bone stock and a disrupted soft tissue envelope. Elements of radial head prosthesis design which may contribute to effectively managing revision surgery include a long stem with in-growth surface and prosthetic head alignment to the axis of forearm rotation.
Footnotes
Acknowledgements
The authors thank Amy Heifner for her valued contributions to the process.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.P.K. declares consulting relationship with Axogen, Trice Medical, and OrthoCircle and is a shareholder in Oxos Medical. D.M.M. declares speakers bureau relationship with Skeletal Dynamics and Axogen. J.J.H., L.E.B., P.A.S., and G.A.G. have nothing to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.