
Abstract
Background:
Swelling and edema of the hand and forearm may occur in various traumatic and degenerative diseases. So far, no precise measurement protocol exists. The objective of this study was to evaluate an examination protocol with relevant regions of interest (ROIs) measured by a 3-dimensional (3D) scanner to achieve precise, reproducible, and objective measurements for an optimized detection of volumes of the hand and forearm.
Methods:
A 3D scan protocol was developed using an Artec, 3D scanner EVA to measure discrete hand volumes of healthy volunteers. Five areas were defined as ROIs, representing volumes of the finger, metacarpus, wrist, hand, and distal forearm. Contralateral limbs were used for volume comparisons and calculation of volume differences.
Results:
For this study, 12 individuals (58.3% women, 24 hands and forearms) with a mean age of 27.1 ± 3 years were included. Mean volume values for left and right ROIs correlated with each other, with slightly higher volumes for the right upper extremity. Volume differences showed statistically significant results for the finger region (ROI I; P = .009), the metacarpal region (ROI II; P < .001), hand region (ROI IV; P = .001), and forearm region (ROI V; P = .006), with the exception of the wrist region (ROI III; P = .722).
Conclusions:
Our results demonstrate that this 3D volumetric approach is a reliable and objective tool for measuring volumes and circumferences in hand and forearm. Based on our determined ROIs, further studies are needed to explore the significance for clinical applications.
Introduction
Swelling and edema of the hand and forearm are frequent symptoms with a broad variety of different causes in orthopedic and trauma surgery. Overload of tissue fluid and its deranged circulation lead to an increased circumference of this region. 1 Common reasons for this pathophysiologic imbalance are injuries of these regions, such as distal radius fractures; fractures of the carpus, metacarpus, or fingers; and infections of different origins.2 -4
These pathologies often require a surgical treatment. Definitive therapy is almost always recommended after at least significant reduction of swelling as soft tissue complications due to swelling and edema are generally named causal for serious complications within surgical treatment of these injuries. 5
Therefore, the extent of soft tissue swelling and its objective evaluation are indispensable for the determination of the optimal time point for definitive surgery. Moreover, inclusion of swelling conditions can be crucial in the process and progress of postsurgical evaluation and for hand therapy. An objective and early detection and evaluation of swelling could help with indications for potential revision surgeries, the initiation of necessary actions, and thereby avoid protracted courses and further complications, such as the complex region pain syndrome.
Currently, there is no consensus on the best measuring method. 6 The ideal method for circumferential measurements should be objective, noninvasive, fast, and inexpensive. Certain methods have been described for detecting and measuring the circumference and volume of several areas of the human body, including bioelectrical impedance and subjective tape measurements. To date, circumference tape measurements and water displacement are commonly the criterion standard method for the diagnosis and evaluation of swelling and edema in the clinical routine.
However, the abovementioned methods for detecting circumferences and volumes of different body regions, including tape measurement and water displacement, are mostly imprecise and have underlying subjective bias. 6
In the last decade, technological developments of 3-dimensional (3D) imaging techniques have led to the development of special 3D scanners that evolved to be precise, objective, and noninvasive. Such devices could serve as objective and accurate tools for volume assessments. 7
Koban et al showed in a recent work that in diagnostics and therapy of lymphedema, 3D volume measurements with a 3D imaging system served as a helpful tool for the acquisition of swelling conditions and volumes. In addition, measurements with a 3D scanner can be taken significantly faster than conventional tape measurements. Not least, results of water displacement, as the most reliable method, showed high accordance in comparison with 3D imaging measurements. 8
The aim of this study was to establish a 3D imaging protocol as an objective and reproducible tool to acquire and evaluate circumferences and volumes of the hand and forearm region. We conducted a prospective study in healthy volunteers and determined relevant regions of interest (ROIs) that could in particular serve as a framework for future investigations to evaluate swelling conditions in hand and forearm infections and be a helpful diagnostic tool in initiating an appropriate treatment for those patients.
Materials and Methods
Study Design and Population
The study protocol was approved by our hospital’s institutional review board (IRB#: 2019-475). Informed written consent was obtained from all participants, and the study was conducted according to the principles expressed in the Declaration of Helsinki.
Twelve healthy volunteers (24 hands and forearms) were included in this study. Inclusion criteria were individuals older than 18 years with a healthy medical history regarding the upper extremities. Participants who documented injuries or any other functional disorders regarding their fingers, hands, or wrist joints were excluded from the study. Each participant completed a standardized questionnaire, including demographics such as age, self-stated sex, height, weight, and dominant extremity.
Image Processing and 3D Analysis
Images were conducted with Artec EVA (Artec Group, Senningerberg, Luxembourg). Artec EVA is a structured light scanner with a superior data acquisition speed, accuracy, and resolution (acquisition speed of 2 mln points/s, resolution of 0.5 mm, and an accuracy of 0.1 mm). In addition, it is a portable device, allowing scanning in convenient environments.
During the scanning process, objects are illuminated by the scanner. The scanner recognizes and records the objects and ROI by 2 main cameras and by normal visible light, sparing harmful radiation. A third camera, which is located in the middle of the scanner, receives texture information. For an accurate processing of the 3D scans, patterns that mark and circumscribe the ROI have to be defined and set a priori. Up to sixteen 3D pictures per second are conducted and automatically integrated into Artec Studio 13 software for processing. After the scanning procedure, all images and texture information are merged together in real time, to create a color texturized 3D scan. Measurements were conducted by the Artec Studio 13 software (Version 13; Artec Group). Each scan took around 3.8 (SD ±2) minutes.
Study Protocol and Scanning Procedure
All scans were recorded by the same examiner and took place in the same environment and with the same scanner (Artec, Model EVA). Before scanning, circumferences were indicated with a marker. As a result of this, the Proc. styloid radius was established as a beginning point, and the circumferences were marked 20 cm proximal and 10 cm distal, subdivided into segments of 2.5 cm (12 volumes [V], Figure 1).
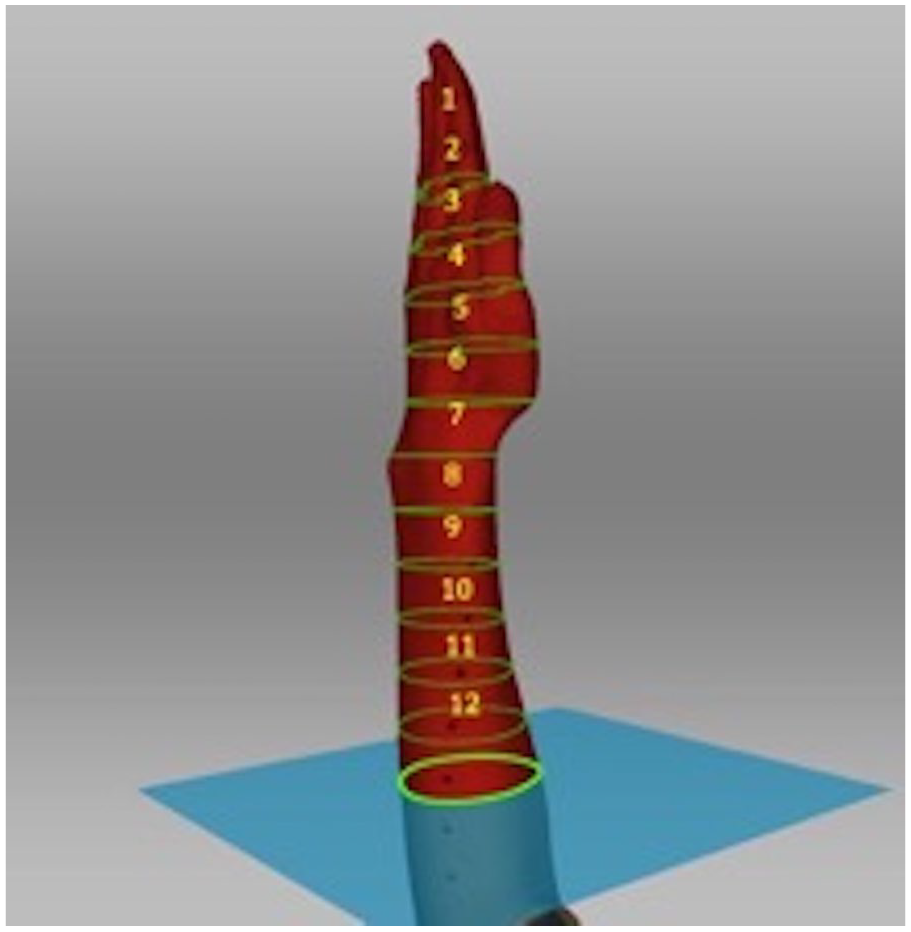
Three-dimensional scan of the upper extremity with indicated volume circumferences (volumes 1-12) extending from the distal finger region to the proximal forearm.
The volunteers were seated on a stretcher, and their elbow was perpendicularly placed on a table with an upright hand position, according to the neutral-zero position of the hand (wrist in 0°, elbow 90°). 9 To make a proper compartmentalization possible during the scanning procedure, before scanning, we marked the whole hand and forearm region at distances of 2.5 cm, starting from the finger tips up to the proximal forearm. After that, the scanning procedure was started, and the examiner moved the scanner around the volunteer until the hand and the distal forearm were completely recorded. The scanner would recognize every 2.5-cm mark and scan that area and measure a certain volume (yellow circles in our figures). Given that, we were able to calculate the volumes of the different ROIs in accordance with the anatomical segments (finger, metacarpal, wrist, hand, and forearm region) by adding up the separate volumes. All volunteers were instructed to keep the scanned extremity calm and to move as little as possible during the scans. The ideal distance to perform the best scan was determined by the distance adjustment indicator within the Artec Studio 13 Software.
ROIs and Volume Measurements
We defined areas as the ROIs (Figure 2): ROI I was compiled of 2 most distal volumes and represented the finger region (volumes 1 + 2), ROI II was defined as the metacarpal region (volumes 3-5), and ROI III as the wrist region (volumes 6 + 7). In addition, we looked at the overall hand volume that was defined as ROI IV and consisted of the finger, metacarpal, and wrist region (volumes 1-7) and ROI V as the forearm region (volumes 8-12) (Figure 2).
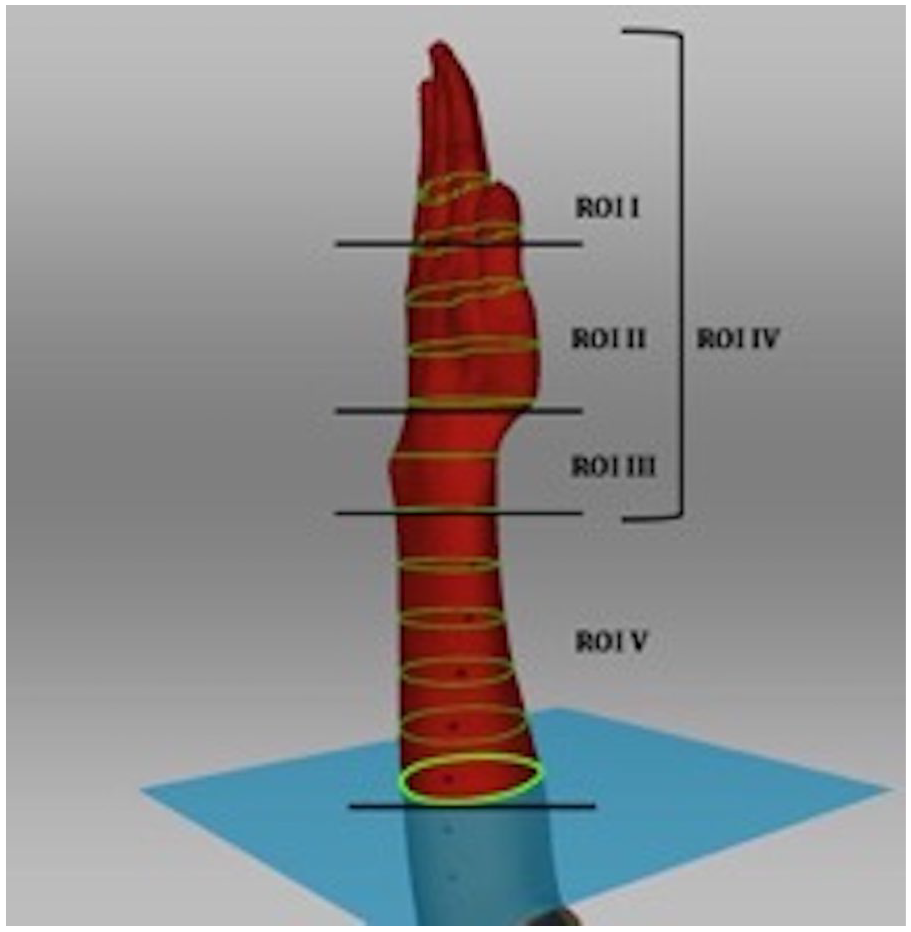
Determination of the 5 ROIs.
Statistical Analysis
The Shapiro-Wilk test was applied to check the normality of the data. For comparisons between volumes of both extremities, the paired t test was used. Data are presented as mean ± SD. Mean and SD were summarized for continuous variables depending on their distribution. Count and percentage were calculated for discrete variables. All analyses were performed using SPSS Statistics, version 23.0 (IBM Corp, Armonk, New York). The statistical significance was set as P ≤ .05.
Results
Baseline Data and Demographics
A total of 12 individuals (58.3% women) who were predominantly right-handed (91.7%) were included in the final analysis. The patient cohort showed a mean age of 27.1 ± 3 years and a mean body mass index of 24.0 ± 4.5 kg/m2. Scanning procedures with EVA Artec required an average of 6.8 ± 2 minutes for each upper extremity. Detailed mean volume values for all ROIs are presented in Table 1.
Mean Volumes of the Different ROIs With Accordingly Calculated Difference, Presented as P Values.
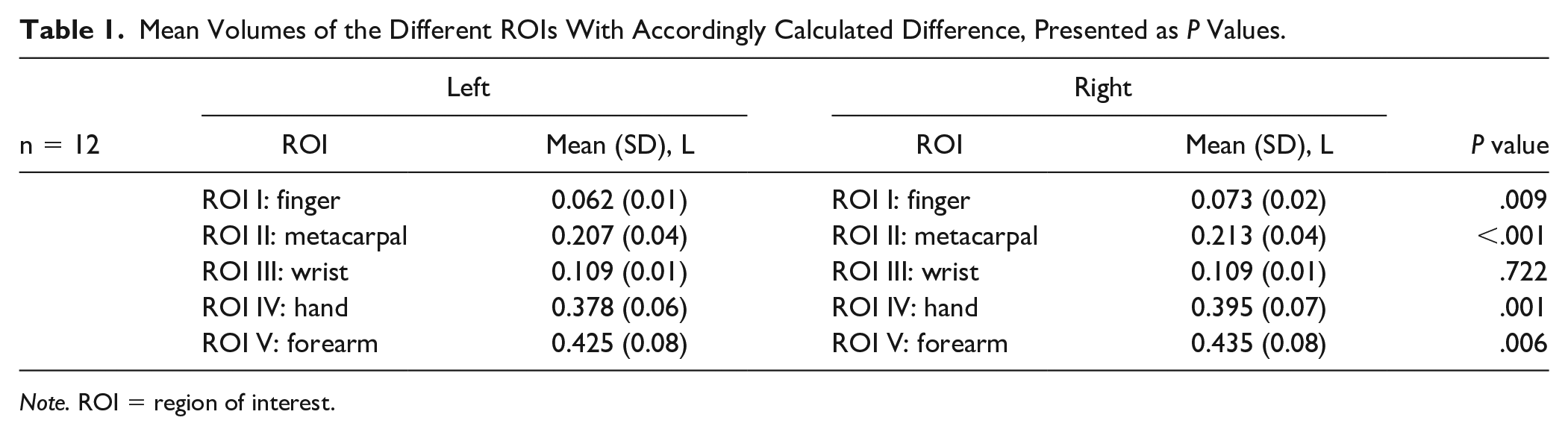
Note. ROI = region of interest.
Comparison of Left Versus Right ROIs
Comparison of left versus right ROI volumes showed a significant higher volume for the right side of the finger region (ROI I; P = .009), metacarpal region (ROI II; P < .001), hand region (ROI IV; P = .001), and forearm region (ROI V; P = .006).
Only the wrist region showed no significant results of mean volume difference (ROI III; P = .722). Detailed mean volume differences of the ROI between the left and right side are outlined in Table 1.
Detailed calculation of the volume differences between left and right ROIs is presented in Table 2.
Volume Differences Between Left and Right ROI.
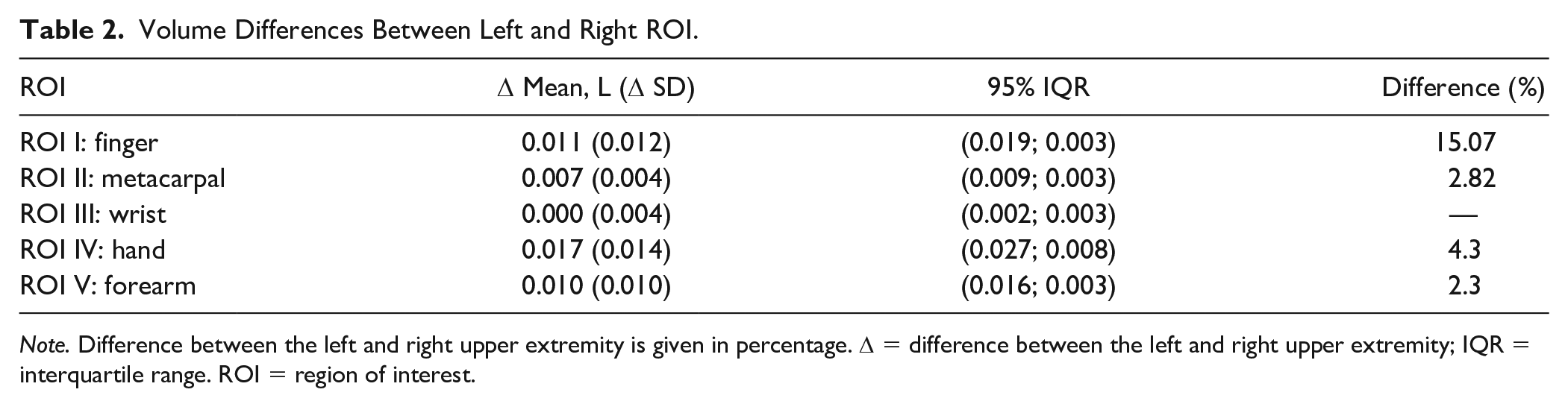
Note. Difference between the left and right upper extremity is given in percentage. Δ = difference between the left and right upper extremity; IQR = interquartile range. ROI = region of interest.
Discussion
Swelling of the hand and upper extremity occurs in various pathologic conditions such as fractures, dislocation, infections, and compartment syndrome. Moreover, implication of an objective evaluation tool to measure swelling conditions and influence subsequent therapy could serve as a helpful tool in several postoperative settings and during hand therapy sessions, not last to avoid complications.
We established a standardized 3D measurement protocol to scan hand volumes in a noninvasive, clinically applicable method.
A variety of methods for detecting circumferences and volumes of different body regions have been established over the last decades, including bioelectrical impedance, tape measurement as well as water displacement.10,11 Currently, the water displacement method is considered to be the gold standard for volume measurements. 2 Nonetheless, in some cases, it is inappropriate to perform, especially in wounded tissue, and does not offer the classification into specific ROIs, despite being time-consuming and inconvenient to handle.7,12
Portable 3D scanners have recently evolved as a valid, objective, reliable, noninvasive, and fast volume measurement tools, competing to the current criterion standard.3,4. Koban et al 8 tested the validity and reliability of the portable Artec EVA 3D scanner by capturing swelling conditions and volumes of the lower extremity and showed a significant correlation to the water displacement method and concluded the scanner to be a reliable mean for volume measurements. Another study identified a low mean error of 1.4%, when comparing the Artec EVA scanner with the most accurate methods presented in the literature, including the water displacement method. 13
Furthermore, Hameeteman et al 12 determined volumes in breast cancer patients with lymphedema and concluded that measurements with 3D imaging have a high reliability and significant lower variances in comparison with the water displacement method. In this study, a stereophotogrammetry system was used to assess volumes of the upper extremity.
Seminati et al 13 described it as a valid and reliable method for assessing residual limb volumes with a low mean percentage error of 1.4 % (validity) compared with the most accurate methods presented in the literature.
To date, we are the first to conduct measurements of the hand and upper extremity with the portable Artec EVA scanner that allows a less cumbersome use and a noninvasive technique. Volume and swelling comparison to the contralateral, healthy extremity is essential and commonly performed for a proper evaluation. Currently, there is a lack of knowledge in evidence-based volume variability between unilateral and contralateral hand and forearm. As the Artec EVA scanner provides the possibility to analyze high-resolution, specific ROIs, we established 5 different ROIs, in accordance with relevant and valid landmarks for volume assessment of the upper extremity in prior studies.14,15 We considered different attributes that are clinically relevant for daily evaluation of upper limb pathologies or injuries and chose anatomical landmarks that are also relevant for clinical examination and allowed a categorization in 5 autonomous areas that potentially display specific tissue impairment: finger for phalangeal fractures/infections, metacarpus and wrist for carpometacarpal dislocations/fractures/ infection, and hand and forearm for fractures/infections or compartment syndrome.
We could identify similar volume values for the different ROIs of the left and right upper extremity, however with significant volume differences for all ROIs for the left and right, with exception of ROI III (wrist region).
Our study revealed well-correlated volumes for both left and right limbs. Volume differences were significant between the left and right for all ROIs, with higher values for the right side, except for the wrist region (ROI III). An explanation could be the given volume difference between dominant and nondominant side and at the same time the majority of right-handed individuals in our study. The nonsignificant difference between the left and right wrist region underlies the influence of individual soft tissue and muscle expression and confirms the valid method of scanning, as the wrist region is dominantly shaped by its bony structures and does not consist of much surrounding tissue. Taking these measurement characteristics into account can be helpful for future investigations and the establishment of volume reference values for the upper extremity.
Here, also the development of volume differences in terms of conservative or preoperative/perioperative time courses and features can be of great interest and relevant for decision-making. Besides, in plastic and reconstructive surgery, 3D imaging of volumes and shapes has been already used for individual planning of plastic operations that can often become necessary in hand and forearm pathologies, in relation to the course and progression. 16
Lately, many approaches have been proposed to combine 3D scanning with pigmentation or thermal imaging to perceive color or temperature differences in tissue, next to shape and volume.17,18 This could imply an additional crucial potential in the evaluation and diagnosis of hand and forearm pathologies.
Our study presents several limitations. First is the relatively small sample size of 12 participants. However, previous studies showed, in similar small or even smaller sample sizes, a low mean percentage error using the same portable Artec 3D scanner.8,13,19
Second, our population presents mostly right-handed individuals, which could bias our results. Of note, a comparison between dominant and nondominant extremity was not feasible within our study population, although our results imply that a difference might be possible due to generally higher volume differences for ROIs of the right limb. Finally, our study population consists predominantly of healthy, white individuals. The fact that we only studied 1 single population was not by design or actively chosen but rather a matter of coincidence and circumstances. This fact does not only impede the generalizability of our results but also make them inapplicable to a nonwhite population or populations with diversity or ethnical background. Obviously, this could lead to the perception of racial and ethnic disparities. Several studies already addressed such conflicts in the past20,21 as clinical trials tend to offer far too little racial and ethnic diversity. These conflicts exist for a long time, and it should be the aim of every clinical trial/study to offer general results and therefore the opportunity to apply the results to any population, no matter what ethnical background or diversity.
Indeed, our technique should also be applied within populations of different ethnical backgrounds in future studies.
The implementation of Artec scanning in daily clinical practice offers great opportunities for evaluation and establishment of therapy regimes. The investigation of a wider range of population and specification of the variances between dominant and nondominant extremities are needed. Here, the examination of different patient populations such as athletes or professional musicians could further establish this method before using it in patients with acute pathologies and injuries.
Conclusion
We showed that portable 3D scanning volume measurements are an accurate and reliable mean to assess volume differences in the hand and forearm region.
The determined ROIs could in particular serve as indicators in the investigation and evaluation of several pathologies and could optimize their management. Moreover, our information could serve as a helpful tool in the postoperative setting and in the further course of hand therapy to avoid lengthy courses of disease or complications. Based on our results and our determined ROIs, further studies in broader populations with different ethnical backgrounds and diversity are needed to investigate the significance for clinical applications in patients with hand and forearm pathologies.
Footnotes
Acknowledgements
We thank Tobias Ruhrmann for excellent technical assistance and support. We also thank Pierre Koppetsch for supply of technical devices and Prof. emerit. Godehardt and Anja Schmitt (born: Bergermann) for their contribution in preliminary work.
Ethical Approval
The study protocol was approved by our hospital’s institutional review board (IRB#: 2019-475).
Statement of Human and Animal Rights
The study was conducted according to the principles expressed in the Declaration of Helsinki.
Statement of Informed Consent
Informed written consent was obtained from all participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.