
Abstract
Background:
Nonunion rates following ulnar shortening osteotomy (USO) are reported up to 18% with few known risk factors. While resection length is variable in practice, little is known about the prognostic implications on healing. The purpose of this study was to evaluate whether longer resection lengths increased the odds of nonunion.
Methods:
A retrospective review was performed on patients who underwent an elective USO at a single institution over a 6-year period. Demographic, social, comorbidity, and surgical data were reviewed. Ulnar resection length was obtained from operative notes and dichotomized into smaller (<5.5 mm) and larger (≥5.5 mm) groups. The primary outcome was the rate of nonunion. Univariate analyses and a multivariable logistic regression model were used to assess for significant predictors of nonunion.
Results:
A total of 87 patients were included with a mean age of 45 years. Patient comorbidities included 12.6% with diabetes, 29.9% with an American Society of Anesthesiologists score of ≥ 3, 5.8% reporting current tobacco use, and 29.9% reporting former tobacco use. There were 55 patients (63.2%) with resection lengths < 5.5 mm and 32 patients (36.8%) with ≥ 5.5 mm resections. Multivariable analysis identified longer resection length (≥5.5 mm) and current tobacco use as independent risk factors for nonunion. Patients with a resection length of ≥ 5.5 mm had 20.2 times greater odds of nonunion compared with patients with smaller resections, and current smokers had 72.2 times greater odds of nonunion compared with nonsmokers.
Conclusion:
Longer ulnar resection length (≥5.5 mm) significantly increases the risk of nonunion following USO.
Introduction
Ulnar shortening osteotomy (USO) is a widely accepted surgical procedure for multiple conditions resulting in ulnar-sided wrist pain, including ulnar impaction syndrome, triangular fibrocartilage (TFCC) tears, lunotriquetral ligament tears, and malunited distal radius fractures.1 -6 These conditions may result from static or dynamic positive ulnar variance, which creates distal ulnar abutment through the TFCC and carpus.4,5,7 Biomechanical studies have shown that even with neutral ulnar variance, the ulnocarpal articulation transfers a considerable amount of stress over a relatively small area.7,8 By shortening the ulna, the USO eliminates bony abutment, decreases stress through the ulnocarpal joint, and relieves pain.3 -5,9,10
Outcome studies on USO have been favorable with wide adoption for refractory ulnar-sided wrist pain.2,3,6,9,10 The reported rates of complications such as nonunion, delayed union, and removal of hardware have varied considerably in the literature. Nonunion, a serious complication typically requiring reoperation, has reported rates ranging from 0% to 18% following USO. 1 ,11 -16 However, a recent systematic review by Owens et al 5 revealed a composite nonunion rate of 4.0%. As with any osteotomy procedure, factors influencing bony union are multifactorial. To date, the 3 primary risk factors for USO nonunion evidenced by the literature are smoking, diabetes, and use of a freehand osteotomy.4,11,17 Additional risk factors for nonunion such as thyroid disease, age, body mass index (BMI), and alcohol use have not been shown to have a significant association with USO nonunion. 4 Besides use of a freehand osteotomy, little is known about intraoperative risk factors for nonunion after USO.
The length of ulnar resection ranges widely in the literature.9,18,19 There is no commonly accepted or recommended length of resection for USOs, and it is generally left to the discretion of the surgeon on a case-by-case basis.
The primary purpose of this study was to examine the association of ulnar resection length for USOs with the rate of subsequent nonunion. We hypothesized that larger resection lengths would have an increased risk of nonunion.
Materials and Methods
Data Collection and Outcomes
A retrospective review was performed including all patients who underwent USO by 1 of 5 fellowship-trained hand surgeons at a single academic institution. Patients who underwent surgery from the initiation of the electronic medical record of the institution on January 1, 2014, to January 1, 2020, were included. The electronic medical record was queried for CPT codes 25390 (osteoplasty, radius or ulna; shortening) and 25360 (USO) to ensure all patients were captured. Exclusion criteria included patients with immune compromising conditions, chronic steroid therapy, proximal ulna or olecranon osteotomies, radius osteotomies, patients with less than 3 months of clinical follow-up, and patients who were lost to follow-up prior to confirmed union or nonunion. This retrospective study was approved by the institutional review board of the center.
Postoperatively, the patients’ charts were reviewed through the last clinic follow-up and the last recorded radiograph. Demographic, social, and comorbidity data were collected for each patient including age, sex, BMI, tobacco use, and American Society of Anesthesiologists (ASA) score. Surgical data such as ulnar resection length and the plating system used were collected for each patient. The primary outcome was the rate of nonunion. Nonunion was defined as lack of congruence of 3 of the 4 cortices at the osteotomy site at an interval of ≥ 6 months from the time of surgery (Figure 1) or lack of radiographic change for 3 consecutive months in the setting of consistent clinical findings.4,20 Delayed union was defined as ≥ 6 months to bony union as measured radiographically and confirmed with clinical examination.4,20 Radiographs were reviewed by a blinded, fellowship-trained hand surgeon to assess cortical bridging across the osteotomy site on orthogonal views. Secondary outcomes collected were complications, including symptomatic hardware, surgical site infection, and revision surgeries.

(a) Anterior-posterior (AP) and (b) lateral preoperative radiograph of a patient with ulnar impaction syndrome after a malunited distal radius fracture. (c) AP and (d) lateral postoperative radiograph 1 month after an ulnar shortening osteotomy with a 7-mm ulnar resection. (e) AP and (f) lateral postoperative radiograph 7 months after ulnar shortening osteotomy without cortical bridging indicative of nonunion.
Perioperative Protocol
Three plating systems were used: Tri Med Ulnar Osteotomy Compression Plate (TriMed, Santa Clarita, CA); Acumed LCP-based Ulna Osteotomy System (Acumed LLC, Hillsboro, OR); and TriLock titanium APTUS plate (Medartis, Basel, Switzerland). The amount of ulna to be resected was determined by preoperative templating on a posteroanterior (PA) clenched fist radiograph. While there were 5 surgeons in this cohort, the goal in most cases was to achieve 2 mm of ulnar negative variance. All surgeons used an oblique osteotomy created by a jig-based guide. The surgical technique was similar to that previously described using the extensor carpi ulnaris and flexor carpi ulnaris interval to approach the ulna, using the guide of the manufacturer to make an oblique osteotomy in the distal one-third of the ulnar shaft, and placing the plate in the most anatomical location as determined by the treating surgeon. 4 The maximum allowable resection length for the Acumed cutting guide is 10 mm. For the 2 cases with greater than 10 mm resections, the first cut was made with the Acumed resection guide. The maximal resection length (10 mm) was then marked, and the guide was translated the additional templated distance which was confirmed with a ruler before the second cut was made. All surgeons instituted similar postoperative protocols with splinting or bracing for 6 weeks followed by mobilization exercises.
Length of clinical follow-up was variable, but the routine postoperative protocol for these patients was follow-up at 2 weeks, 6 weeks, and 3 months. Patients lost to follow-up less than 3 months post-op were excluded from the study. If the patient showed radiographic union, full range of motion, and minimal pain at 3 months, the patient was either allowed to return to clinic as needed thereafter or was followed-up based on surgeon preference. If these conditions were not met, the patient returned to clinic for further evaluation at 6 months. If radiographic union was not observed at the 6-month visit, patients were prescribed a low-intensity pulsed ultrasound bone stimulator to increase chances of achieving delayed union. Those patients with persistent nonunion after bone stimulation and/or with catastrophic failures of fixation as a result of their nonunion underwent revision fixation with bone grafting.
Sample Size and Statistical Analysis
A priori power analysis performed using G*Power version 3.1.9.3 to determine the sample size needed to detect a difference in time to union rates between patients with a smaller and larger resection length assuming a 2:1 ratio. Nonunion rates were extrapolated from data from a systematic review by Owen et al. 5 The sample size calculation was performed using the z family of tests with the statistical test for proportions: difference between 2 independent proportions. In the literature, nonunion rates following ulnar shortening osteotomies are reported from 0% 7 to 18%.1,2 Assuming a 2-sided test, alpha of 0.05, power of 0.8, nonunion rate of 1% in the smaller resection group, and nonunion rate of 20% in the larger resection group, it was determined that a total of 78 patients would be needed to detect a significant difference (P < .05) in bony union between groups. Thus, a minimum of 52 patients would be needed for the smaller resection group and a minimum of 26 patients in the larger resection group. The Youden index was then employed to determine the optimal resection cutoff point for the receiver operator characteristic curve in a univariable model for predicting nonunion rates. This index value represents the level at which both sensitivity and specificity are maximized.
All variables were summarized with means and standard deviations for continuous variables or frequencies and percentages for categorical variables. The distributions of continuous variables were assessed using histograms, box plots, and the Kolmogorov-Smirnov test for normality and homogeneity of variance using the Levene test. The resection length data are positively skewed with an average resection length of 5.6 mm (SD = 2.3; range, 3-16 mm) and median of 5.0. According to analysis with the Youden function, the optimal cutoff value that maximized sensitivity and specificity in predicting nonunion was found to be 5.4 mm, although discrimination was limited (concordance statistic: 0.69). Resections are made in 0.5 mm increments. Based on these considerations, 2 subgroups were created and analyzed: smaller resection length (resection length < 5.5 mm) and larger resection length (resection length ≥ 5.5 mm). Bivariate analyses were performed comparing these 2 cohorts of patients. Continuous variables were compared between the resection groups using independent 2-sample t-tests, and categorical variables were compared using χ2 or a Fisher exact test in the presence of small cell counts (<5). Univariate logistic regression models were constructed to identify risk factors for nonunion. Variables determined to be statistically associated (P < .10) with the occurrence of nonunion in univariate testing were used in a multivariable logistic regression model using the Firth bias-correction to control for potential confounding and to identify independent risk factors for nonunion. Odds ratios with 95% confidence intervals were reported for all significant predictors, and model fit was confirmed using the Hosmer-Lemeshow test. All statistical tests were 2-sided, and a probability of .05 or less was considered significant for all statistical analyses. Statistical analyses were performed using SAS, version 9.2 (SAS Institute, Cary, North Carolina).
Results
Demographic and Clinical Data
Of the 110 patients initially identified, 87 patients who underwent an USO met the inclusion criteria and were included in this study. Demographic information can be found in Table 1. The mean patient age was 45.0 years (SD = 14.4; range, 15-75 years). Most patients were women (n = 53, 60.9%). The average BMI was 29.8. (SD = 7.5). Patient comorbidities included 11 (12.6%) with diabetes and 26 (29.9%) with an ASA score of 3 or greater. A total of 5 (5.8%) patients reported current tobacco use and 26 (29.9%) reported former tobacco use.
Preoperative Demographic and Clinical Data.
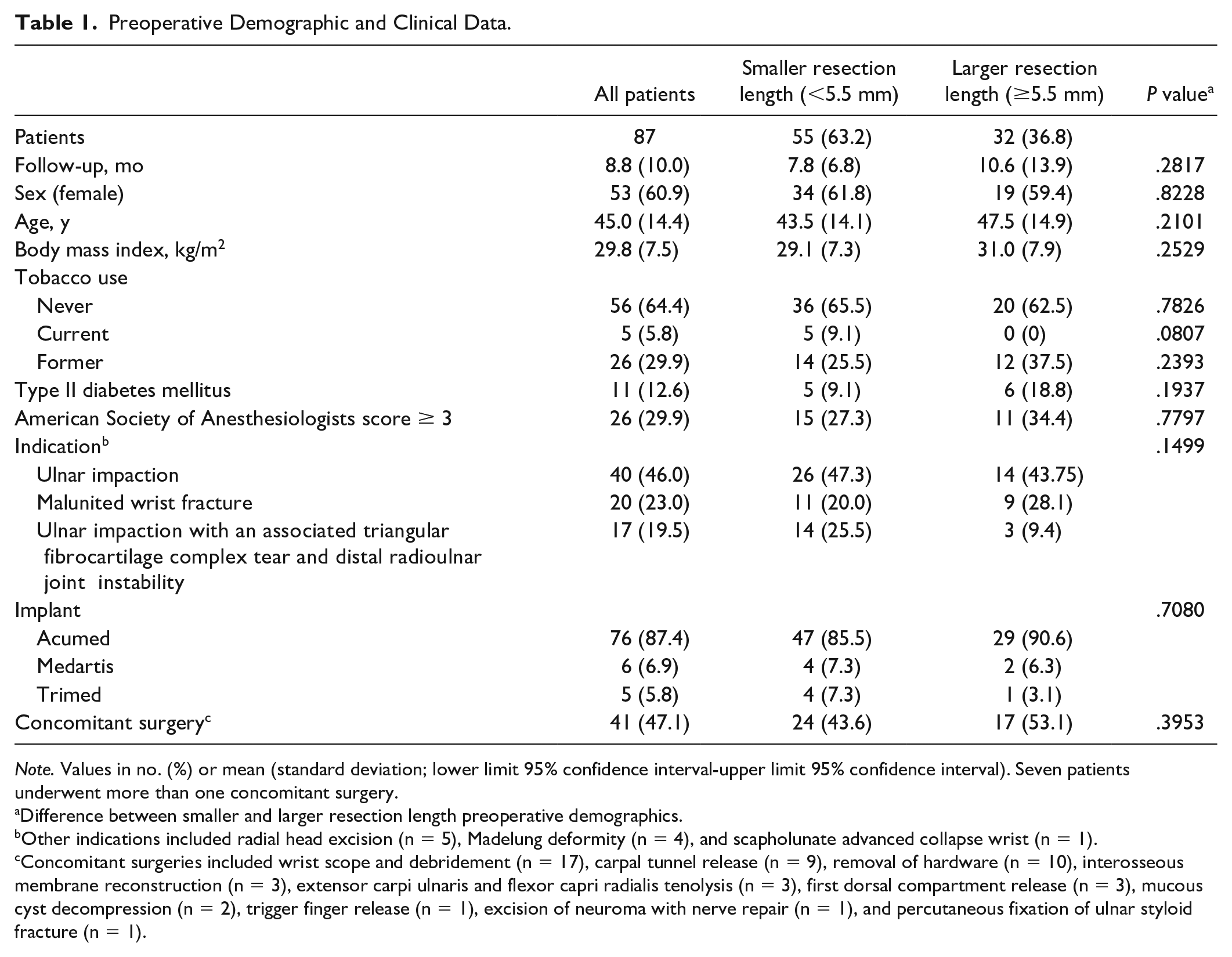
Note. Values in no. (%) or mean (standard deviation; lower limit 95% confidence interval-upper limit 95% confidence interval). Seven patients underwent more than one concomitant surgery.
Difference between smaller and larger resection length preoperative demographics.
Other indications included radial head excision (n = 5), Madelung deformity (n = 4), and scapholunate advanced collapse wrist (n = 1).
Concomitant surgeries included wrist scope and debridement (n = 17), carpal tunnel release (n = 9), removal of hardware (n = 10), interosseous membrane reconstruction (n = 3), extensor carpi ulnaris and flexor capri radialis tenolysis (n = 3), first dorsal compartment release (n = 3), mucous cyst decompression (n = 2), trigger finger release (n = 1), excision of neuroma with nerve repair (n = 1), and percutaneous fixation of ulnar styloid fracture (n = 1).
The surgical indications most commonly identified were ulnar impaction (n = 40, 46.0%), malunited wrist fracture (n = 20, 23.0%), and ulnar impaction with an associated TFCC tear and distal radioulnar joint (DRUJ) instability (n = 17, 19.5%). The implant most commonly used was the Acumed ulnar shortening plate (n = 76, 87.4%). A total of 41 (47.1%) patients underwent a concomitant surgical procedure at the same time as their USO. This most commonly involved a wrist scope and debridement (n = 17), carpal tunnel release (n = 9), and removal of hardware (n = 10). Seven patients underwent more than one concomitant procedure. The average resection length was 5.6 mm (SD = 2.3; range, 3-16 mm). The demographics and clinical data were similar between the 2 cohorts without any significant, between-group differences (Table 1).
Complications
Postoperative complications are outlined in Table 2. One patient (1.2%) had a deep surgical site infection requiring irrigation and debridement with removal of hardware at 14 days postoperative for a methicillin-resistant stapholococcus aureus (MRSA) infection. There were 13 patients (14.9%) that experienced delayed union. Seven patients (8.1%) had a nonunion. Of these radiographic nonunions, 5 were atrophic, 1 was oligotrophic, and 1 was hypertrophic. Of the 7 patients with nonunion, 3 underwent revision USO with removal of hardware and repeat internal fixation, 2 refused further intervention despite recommendation for revision USO, 1 patient died, and 1 patient continued metabolic optimization with endocrinology in anticipation of revision USO. A total of 20 patients (23.0%) reported symptomatic hardware. There were 17 patients (19.5%) who underwent a repeat surgery. This included 9 (10.3%) patients who underwent isolated removal of hardware; 3 patients (3.6%) who underwent revision USO with removal of hardware and repeat internal fixation; 1 patient (1.1%) who had an irrigation and debridement with removal of hardware for infection; and 3 patients with other indications.
Complications and Repeat Surgery.

Note. Values in no. (%).
Repeat surgeries included 9 (10.3%) patients who underwent isolated removal of hardware; 3 patients (3.6%) who underwent revision ulnar shortening osteotomy with removal of hardware and repeat internal fixation; 1 patient (1.1%) who had an irrigation and debridement with removal of hardware for infection; 1 patient (1.1%) with a wrist scope and triangular fibrocartilage complex debridement; 1 patient (1.1%) with a posterior interosseous nerve neurectomy, anterior interosseous nerve neurectomy, and dorsal capsule release; and 1 patient (1.1%) with a segmental resection of the ulna and distal radioulnar joint arthrodesis.
Includes all patients with at least 1 of the above complications.
Risks Factors for Nonunion
Resection length had a significant impact on the incidence of nonunion. A total of 15.6% (95% confidence interval [CI], 5.3%-32.8%, n = 5/32) patients with a large (≥5.5 mm) resection experienced a nonunion (Figure 1) compared with 3.5% (95% CI, 0%-8.6%, n = 2/55) patients that had a smaller (<5.5 mm) resection (OR, 4.9; 95% CI, 1.89-27.0; P < .05). See Table 1 for a demographic comparison of the small and large resection length cohorts. Current smoking was also found to be a risk factor for nonunion. Nonunion resulted in 40% of patients who were current smokers (n = 2/5) compared with only 6.1% (n = 5/82) of patients who were not currently smoking (P ≤ .05). Diabetes did not reach statistical significance as a risk factor for nonunion (18.2% vs 6.6%, P = .19). No other predictor variables were found to be statistically associated (P < .10) with the incidence of nonunion (Table 3).
Categorical Predictor Variables Predicting Union Versus Nonunion After Elective Ulnar Shortening Osteotomy.
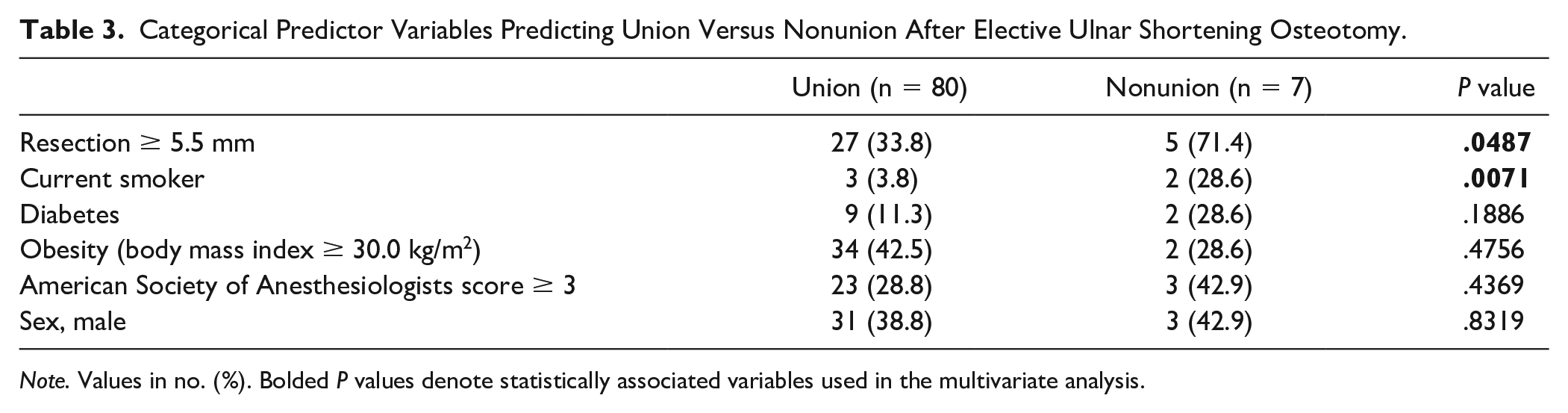
Note. Values in no. (%). Bolded P values denote statistically associated variables used in the multivariate analysis.
Based on these univariate findings, resection length and current smoking status were incorporated into a multivariable logistic regression model. Both a resection of ≥ 5.5 mm (OR, 20.2, 95% CI, 1.04-390.9, P ≤ .05) and a history of current tobacco use (OR, 72.2, 95% CI, 2.6-999, P < .05) were found to be significant independent predictors for nonunion. When controlling for smoking status, patients with a resection length of ≥ 5.5 mm had 20.2 times increased odds of developing a nonunion following elective USO compared with patients with a smaller resection length. The final logistic model was found to be significant (P < .05) and correctly predicted 84.7% (concordance statistic: 0.85) of the nonunions.
Discussion
Ulnar shortening osteotomy is an established and effective treatment for refractory ulnar-sided wrist pain. Of the common complications of this procedure, ulna nonunion is among the most severe. Intraoperative ulnar resection length is a key variable that must be considered preoperatively, although there are no established guidelines on the amount that is safe to resect. This study sought to evaluate an association between increased ulnar resection length and the development of subsequent nonunion. By dichotomizing the ulnar resection length into < 5.5 mm and ≥ 5.5 mm cohorts, we found that the odds of developing a nonunion were 20.2 times greater in the larger resection group.
While nonunion is a known and severe complication of USO, few risk factors have been identified in the literature. Much of the difficulty in identifying risk factors stems from the relative rarity of this procedure and the small, retrospective series which result. The reported rate of nonunion in this study (8.1%) falls well within the range of prior studies—0% 7 to 18%.1,2 In spite of the variable reported rates of nonunion and small, retrospective series, smoking and diabetes have been identified as the most commonly and well-supported risk factors for nonunion following USO, similar to in long-bone fracture healing.4,7,11,21 -23 While glycemic optimization and smoking cessation should be strongly encouraged during preoperative counseling, there is little known about further measures the orthopedic surgeon may take to decrease risk for nonunion. Sunil et al 17 identified freehand osteotomy as an intraoperative risk factor associated with higher rates of nonunion following USO. To avoid freehand osteotomy, the resection guide was used in every case in this series. In cases that require resection lengths greater than the maximum allowable resection length of the cutting guide, the aforementioned double cut technique, using translation of the guide should be employed to avoid freehanded cuts. The current study identified ulnar resection length ≥ 5.5 mm to be an additional intraoperative and surgeon-controlled risk factor for the development of subsequent nonunion. This knowledge should be taken into consideration during preoperative templating, especially in patients with other known risk factors such as active smoking and diabetes. In cases where ulnar resection length ≥ 5.5 mm lengths are necessary, rigorous preoperative metabolic optimization with smoking cessation and glycemic control are likely to improve the odds of union. In the authors’ practice, shorter lengths (≤5.5 mm) of ulnar resection have now been employed in most cases. In patients with longer planned (≥5.5 mm) resections, preoperative evaluation with serum calcium, 25-hydroxy-vitamin D, thyroid-stimulating hormone, alkaline phosphatase, and albumin are now being employed in the authors’ practice to ensure optimized metabolic conditions for bony union. Intraoperatively, in cases with longer ulnar resections, consideration of orthogonal fixation has been employed in authors’ practice, although the decision is made on a case-by-case basis.
The mean ulnar resection length in this study was 5.6 mm which falls well within the reported range of 1 to 13 mm.3,9,17 While reported lengths of resection and rate of nonunion vary widely, little is known about an association between these 2 variables. A study by Mirza et al 6 and Cha et al 7 reported a 0% nonunion rate with a mean ulnar resection length of 2.5 and 4.65 mm, respectively, while a study by Fulton et al 2 reported an 18% nonunion rate with a mean ulnar resection of 3.11 mm. Series such as these have no discernible pattern between ulnar resection length and subsequent rate of nonunion and were underpowered to do so. This study, although still relatively small, was powered to identify the association between large resection lengths (≥5.5 mm) and subsequent nonunion. While a 5.5 mm resection is certainly higher than in many other series,2,6,7 the knowledge that resecting greater than 5.5 mm increases the odds of nonunion remains clinically relevant, especially when using the Acumed and Medartis systems which have cutting guides with an allowable resection length of 10 and 8 mm, respectively.
Ulnar resection decreases bony abutment and stress through the ulnocarpal joint and simultaneously provides stability to the DRUJ.5,7,8 A prior cadaveric study by Nishiwaki et al 8 found that after performing ulnar resections of 3 to 6 mm, the greatest DRUJ stability was conferred with 6 mm resections, when the radioulnar ligaments were attached or partially attached to the fovea. In isolation, this finding could lead to the conclusion that larger resections may be favorable. One possible explanation for the higher rate of nonunion in large resections is that the tension created in the distal oblique bundle of the interosseous membrane which confers stability to the DRUJ also pulls against the osteotomy site. The current study shows that these large resection lengths of ≥ 5.5 mm have the inadvertent effect of increasing the odds of subsequent nonunion. While this finding does not provide a guideline for the optimal length of resection, it does provide a key consideration for integration into decision making preoperatively, taking into account risk of nonunion, templated postoperative ulnar variance, and aspects of DRUJ stability.
Despite the focus on nonunion, the most frequent cause for a subsequent surgical procedure in patients was symptomatic hardware. In this cohort, all plates were placed on the volar surface of the ulna and the rate of subsequent hardware removal indicated for symptomatic hardware after USO was 10.3%. The literature reports rates of hardware removal up to 55% following USO.11,24,25 This finding further supports the notion that all patients undergoing USO should be counseled on the possibility of needing a subsequent surgery.
There are several limitations to this study including biases inherent to retrospective studies. This includes the potential for information bias and selection bias from retrospectively reviewing data. While demographic data in the electronic health record were compared among the 2 groups, there was no way to know whether the groups had similar preoperative calcium, Vitamin D, and other serum markers that favor subsequent bony union. An additional limitation is the limited sample size given the relative infrequency of the procedure as well as the infrequency of the primary outcome, nonunion. However, all patients who underwent a USO since the implementation of the electronic medical record within the orthopedic hand department of a large-volume, academic hospital were included in this study. Despite this, the current study was powered appropriately to answer the proposed hypothesis predicated on resection size and nonunion rate. However, the data are possibly underpowered to detect other significant predictors such as diabetes, which did not reach statistical significance in the current study, but have been found to be significant risk factors in previous studies.4,11 The literature on nonunion following USOs is fraught with small samples, with a recent systematic review by Owen et al 5 identifying 37 prior studies with an average of 38 participants each. In these small studies, the range of ulnar resection lengths is quite variable. The 5.5 mm resection cutoff is certainly higher than in many other series2,6,7,26 and may be larger than the norm in general practice which is a limitation of this study. When reporting the actual length of ulnar resection in the operative notes, all surgeons in the cohort measured resection length to the nearest 0.5 mm based on preoperative templating and confirmatory intraoperative measurements. There is inevitably a small margin of error with measurements this precise which is a limitation of the study. It should be noted that prior studies measured ulnar resection length to the nearest 0.16 or 0.012, 7 mm. Another limitation was the short follow-up length with a minimum of 3 months. Based on individual surgeon preference, some included patients were allowed follow-up as needed if they showed radiographic union and were otherwise doing well at 3 months postoperatively. However, no patients were included if they did not have a confirmed union or nonunion at the last follow-up timepoint.
In conclusion, longer ulnar resection length (≥5.5 mm) was found to significantly increase the risk of nonunion following USO. This knowledge should be considered in preoperative patient counseling and radiographic templating, especially in the setting of other known risk factors for nonunion.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was not obtained as this was a de-identified database study that is open to use by participating institutions.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two of the authors, M.J.R. and D.S.R., report being paid consultants for Acumed LLC and Medartis, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.