
Abstract
Background:
Despite intensive research into the epidemiology of adult distal forearm fractures, the literature is limited. This study aimed to provide a full overview of adult distal forearm fracture epidemiology, including incidence, fracture classification, mode of injury, and trauma mechanism in patients sustaining a distal forearm fracture, based on an accurate at-risk population with manually validated data leading to a high quality in data.
Methods:
This was a population-based cohort study with a manual review of X-rays and charts. The primary outcome measure was the incidence of adult distal forearm fractures. The study was based on an average at-risk population of 522 607 citizens. A total of 5426 adult distal forearm fractures were included during the study period. Females accounted for 4199 (77%) and males accounted for 1227 (23%) of fractures.
Results:
The overall incidence of adult distal forearm fractures was 207.7/100 000/year. Female incidence was 323.4/100 000/year, and male incidence was 93.3/100 000/year. A marked increase in incidence with increasing age was observed for females after 50 years of age. The incidence of distal radius fractures was 203.0/100 000/year, and the incidence of isolated ulna fractures was 3.8/100 000/year. The most common fracture type was an extra-articular AO type 2R3A (69%), and the most common mode of injury was a fall from own height (76%). A small non-trending year-to-year variation was observed during the 5-year study period.
Conclusion:
Results show that adult distal forearm fractures are very common in women after the postmenopausal period. The overall incidence of adult distal forearm fractures was 207.8/100 000/year. Female incidence was 323.4/100 000/year.
Keywords
Introduction
Worldwide, a fracture of the distal forearm is one of the most common adult orthopedic injuries in the trauma department, with distal radius fractures (DRFs) accounting for an overall 17% of all fractures. 1 Adult DRFs are reported with a bimodal distribution, with peaks in younger males and older females and with the majority of DRFs presenting among females (78%).2-4 Isolated ulna fractures are very rarely reported. 5
The incidence of adult DRF has been investigated in several studies, including both selected and non-selected patient groups.1-4,6-14 In a Scandinavian population, the incidence has recently (2016) been reported as 220/100 000/year in southern Sweden. 6 To the authors’ knowledge, the incidence of adult isolated distal ulna fractures is not reported. Furthermore, recent reports of adult forearm fracture in a Danish setting are lacking.
The distribution of distal forearm fractures according to the AO classification 15 has been investigated by several authors.3,4,16,17 Extra-articular DRFs AO type A have commonly been reported as the most prevalent fracture type, followed by type C and type B fractures.3,4 High-energy trauma is reported to increase the risk of type C complex fractures.4,16
The most common mechanism of injury is reported as fall from standing height and participating in sports, representing 49% to 68% and 16% to 23% of fractures each.3,16 High-energy trauma is most frequent in younger men and low-energy trauma in elderly women.2-4
Despite intensive research of the epidemiology of adult fractures of the distal forearm, existing literature concerning epidemiology lacks a complete overview regarding incidence, trauma mechanism, and fracture classification investigated within a non-selected patient group and manually validated data of high quality. Moreover, recent studies including an accurate at-risk population are limited.
Based on an accurate at-risk population with manually validated data, this study aimed to provide an exhaustive overview of adult epidemiology, including incidence, fracture classification, mode of injury, and trauma mechanism in patients sustaining a distal forearm fracture.
Patients and Methods
In this retrospective population-based epidemiological cohort study, adult distal forearm fractures between January 1, 2013 and December 31, 2017 were examined. All hospitals in the Northern Region of Denmark participated, including 4 regional hospitals and one University Hospital. The region has an average population of 522 607 citizens in the study period (Figure 1).
At-risk population of Northern Region of Denmark (number of citizens).
The present study was based on data from The Danish National Patient Registry (DNPR), 18 which is one of the oldest nationwide health registries in the world and is used extensively for research.18,19 Danish health regulations require that all contacts with health care providers be registered in the DNPR. 18 At birth, a unique Civil Registration Number (CPR) is given to all residents and digitally registered in the DNPR. 18 All information concerning health care contacts throughout life is registered with reference to the CPR. The registry provides researchers with an accurate registry of all health-related contacts on population- and individual-based levels.
Identification of adult patients with a distal forearm fracture was undertaken in the DNPR. 18 Included were all patients diagnosed with a fracture in the distal forearm International Classification of Diseases (ICD-10; DS525, DS525A, DS525B, DS525B, DS525 C, DS528 C, DS529) in the study period. Patients above 10 years of age with closed epiphysial plates were included. Throughout this manuscript, we have defined adults as patients with closed epiphysial plates. All patients’ medical and radiological records were reviewed manually. Patients who were misclassified or did not have a Danish CPR were excluded. Patients not residing in the Northern Denmark region were also excluded.
Data Retrieval
Information regarding the date of injury, age, sex, and trauma mechanism was obtained from the registry and patient charts. The trauma mechanism was divided into low- and high-energy and mode of injury. High-energy trauma includes the following: high-speed accident (>65 km/h), estimated vehicle deformation of more than 0.5 m, hit by vehicle, pedestrian/bicyclist/motorcycle/car colliding, pedestrian/bicyclist collision with motorized vehicle >50 km/h, and fall >4 m. Any other trauma mechanisms were considered low-energy. Mode of injury was divided into 8 categories: fall from <1 m, fall from >1 m, bicycle-accident, sport, motor vehicle operator or passenger, pedestrian/cyclist collision with motor vehicle, hit by object, and other. If any mechanism besides bicycle accident coincides with sport, the mechanism was considered sport. Fractures identified on X-rays (posterior/anterior and lateral X-rays) were used to classify fractures according to the AO classification. 15 Computed tomography and/or magnetic resonance imaging were used when available.
This study was conducted in accordance with the ethical principles of the 1975 Declaration of Helsinki. 20 The Danish Data Protection Agency approved the study (J nr: 2020-158). The reporting of the study complies with the Strengthening of the Reporting of Observational Studies in Epidemiology (STROBE) statement. 21
Statistics
Percentages and frequencies are given for categorial data. Incidences were calculated by age and gender and by year-to-year. Prevalence of fractures is given for fracture classification and trauma mechanism. The statistical analysis was performed by STATA 16, (StataCorp, College Station, Texas). Microsoft Excel 365, version 16.56, was used to prepare figures.
Results
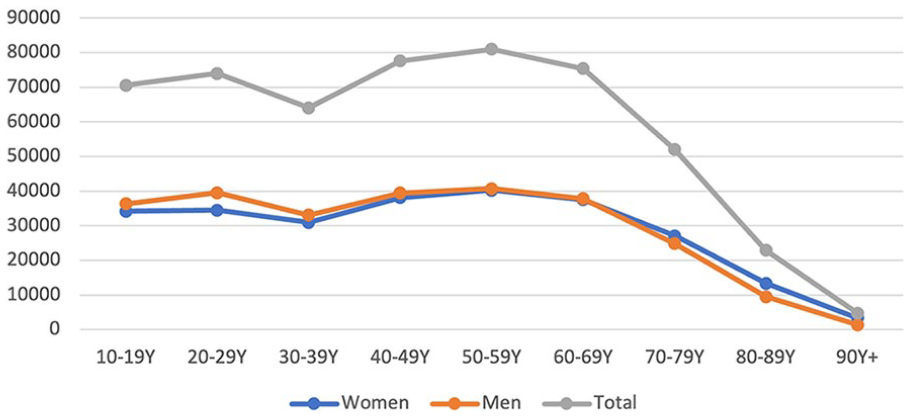
A total of 5426 adult distal forearm fractures were included in the study period. Females accounted for 4199 (77%), and males accounted for 1227 (23%) of the fractures (Table 1). Left-sided fractures accounted for 57% of patients, and 43% had a right-sided fracture. The mean age at the time of fracture was 63.0 years (62.5-63.5). A total of 5305 patients presented with a DRF and 100 patients with an isolated distal ulna fracture. The X-rays of 21 patients were excluded as foreign object rendered classification impossible.
Patients Divided by Age-Group and Gender.

Primary Outcome
The overall incidence of adult distal forearm fractures was 207.7/100 000/year. Female incidence was 323.4/100 000/year, and male incidence was 93.3/100 000/year. A marked increase in incidence with increasing age was observed for females after the age of 50 (Figure 2). The incidence of DRF was 203.0/100 000/year, and the incidence of isolated ulna fractures was 3.8/100 000/year. Isolated ulna fractures were uncommon, representing about 2% of all adult distal forearm fractures.
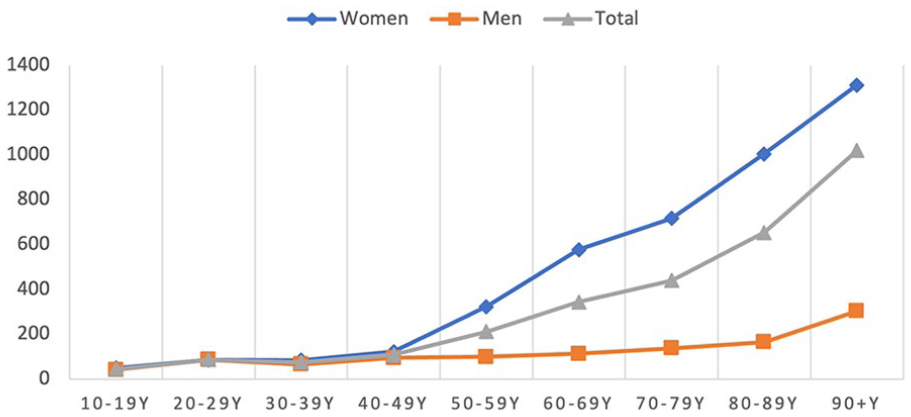
Incidence (10000/year) by age group and sex.
Secondary Outcomes
Gender-specific fracture classifications of all adult distal forearm fractures are shown in Table 2. The most common fracture type was a DRF AO type 2R2-A (68%), followed by type 2R3-C (22%) and 2R3-B (8%). The most common isolated distal ulna fracture was an AO-2U3A1 (1.1%).
Gender-Specific Fracture Classification.

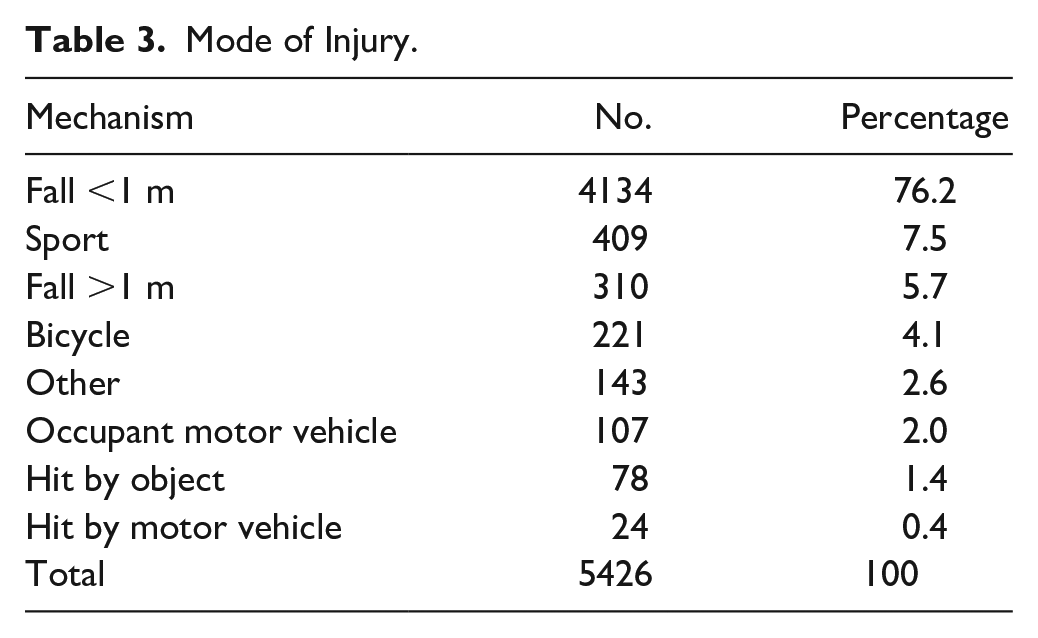
Modes of injury are shown in Table 3. The most common modes of injury were falling from <1 m representing as much as 76%, followed by sport, representing 8% of all cases. Mode of injury was observed comparable between patients presenting with DRFs and distal isolated ulna fractures.
Mode of Injury.
During the 5-year study period, a year-to-year variation <13% in the incidence of adult distal forearm fractures was observed with no apparent trend (Figure 3). The highest incidence of 223.3/100 000/year was observed in 2017, and the lowest incidence of 198.4/100 000/year was observed in 2016.
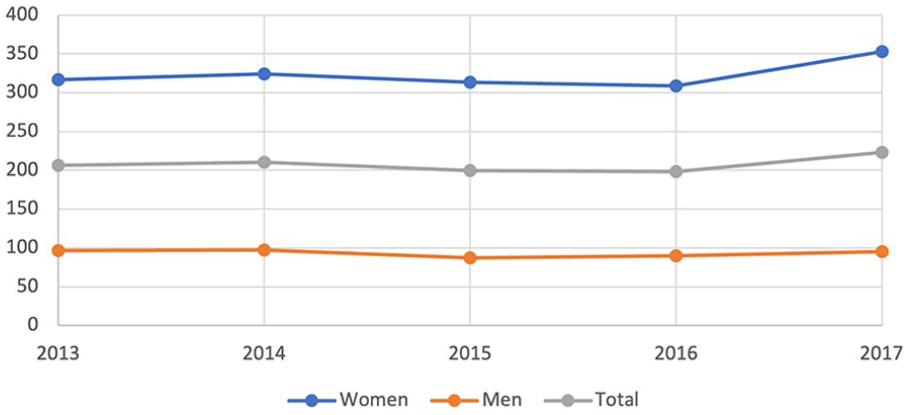
Incidence (100 000/year) by year and sex.
Discussion
The main finding in the present study is the overall incidence of adult distal forearm fractures of 207.7/100 000/year. Distal radius fractures were observed with an incidence of 203.0/100 000/year and isolated distal ulna fractures with an incidence of 3.8/100 000/year. Female incidence increased with age from the perimenopausal period, while in the male population, the increase in incidence with age is moderate.
Results from the present study are consistent with recent studies from the Scandinavian countries reporting an incidence of DRFs between 197 and 220/100 000/year.3,5,6 To the authors’ knowledge, recent studies investigating the incidence of adult isolated distal ulna fractures are not available. However, comparison to the existing literature is difficult due to widespread methodological differences between the studies known to affect the reported incidence rates. The present study includes an accurate adult population with distal forearm fractures based on manually validated X-rays evaluating bone maturity. Although a high incidence of pediatric distal forearm fractures is reported, the incidence is reported to decrease after the age of 15 years. 22 The present study showed a generally small number of fractures in the younger age groups, decreasing the total incidences reported compared to studies reporting incidence including only age groups with a higher likelihood of DRFs. Furthermore, existing literature detailing a full overview of adult distal forearm fractures is limited, as most studies only report specific fracture types and select age groups.
This 5-year retrospective study showed no apparent trend in the year-to-year variation of incidence in adult distal forearm fractures. Compared to a single Danish study by Abrahamsen et al 10 reporting the incidence of forearm fractures in patients age 20+ in 2010, results from the present study are lower. However, Abrahamsen included all forearm fractures (ICD10 code DS52X), and the present study included only distal forearm fractures. The existing literature is vast and report both increases7,11 and decreases9,23 in incidence when comparing different time periods. However, comparison between studies is very difficult due to substantial differences in periods, demographics, study methods, and included age groups.
The distribution of DRFs according to the AO classification 15 showed that the most common fracture type was an extra-articular AO type 2R3A fracture, followed by type 2R3 C and type 2R3B. These results are supported by several previous studies reporting AO type 2R3A as the most common fracture of the distal forearm in adults, followed by type 2R3 C and type 2R3B fractures.3,4 In the present study, 69% of patients presenting with an AO type 2R3A fracture is comparable to Solvang et al 3 reporting 52% and Rundgren et al 4 reporting 65% extra-articular AO type 2R3A in comparable studies. However, some difference in fracture classifications is present among existing literature. 17 Differences in population demographics, periods, study methods, and included age groups may play a key role. Furthermore, the low interobserver validity of the AO classification may be an important component in the differences observed. 24 However, prior to data extraction, all physicians participating in this study attended a kick-off seminar including hands-on training in the radiological classifications used and an introduction to a coding manual to increase the validity and reliability of data.
The majority of adult distal forearm fractures in the present study occurred in women older than 50 years of age due to low energy trauma. The mode of injury was commonly a fall from own height representing as much as 76%. These results are in accordance with results from recent Scandinavian studies.3,4 The high incidence of distal forearm fractures in postmenopausal women is well-known.1,3,4,11 The association between a decrease in bone mineral density in postmenopausal women and DRFs is also previously reported.8,25
Data Validity
This study used data from The DNPR, reported with a high quality of data.18,19 In Denmark, health reporting to the DNPR is mandatory by law. The positive predictive value of orthopedic diseases in the DNPR is reported to be 89% to 91%. 19 A further strength is the inclusion of all adult age groups with manually validated X-rays detailing bone maturity and classification of the fracture. By reviewing patient charts and X-rays, all fractures in the present study have been confirmed, and accurate classification has been validated. Furthermore, based on the CPR allocated to all residents in Denmark, this study included an accurate at-risk population used for the calculation of incidence 18 It is difficult to estimate the completeness of data, as no complete registry exists for comparison. All contacts with hospitals require reporting to the DNPR, and all minor and major trauma are treated in local public hospitals, as these are the only facilities equipped to examine and treat minor and major trauma, indicating high completeness of data.
Limitations
A limitation of our study is that medical charts and X-rays were manually reviewed by several physicians. Some differences in coding may be present due to intra- and interobserver variations. However, prior to data extraction, all physicians participating in this study attended a kick-off seminar including hands-on training in the radiological classifications used and an introduction to a predefined coding manual to increase the validity and reliability of data. Incidence in the age group 10 to 20 years should be interpreted as fracture incidence among patients with mature bone (closed epiphysial plates) related to the total population in the age group, entailing a reduced incidence of mature bone fractures in this age group compared to other studies not distinguishing between open and closed epiphyseal plates.
In conclusion, the overall incidence of adult distal forearm fractures was 207.8/100 000/year. Distal radius fractures were observed with an incidence of 203.0/100 000/year and isolated distal ulna fractures with an incidence of 3.8/100 000/year. Female incidence increased significantly with age from the perimenopausal period. The mode of injury was commonly a fall from own height representing as much as 76%.
Footnotes
Acknowledgements
Hanne Dalsgaard, MD, Head of hand surgery, Aalborg University Hospital, was acknowledged for supporting the study idea, study process, and comments to the final manuscript.
Author Contributions
Conceptualization: L.R.K., S.S., P.L., R.E., and K.P.W.; Data curation: S.S., P.L., L.R.K., A.A.C., M.B.L., J.T.F., K.P.W., and R.E.; Analysis: L.R.K., S.S., P.L., R.E., and K.P.W.; Methodology: S.S., P.L., L.R.K., A.A.C., M.B.L., J.T.F., K.P.W., and R.E.; Validation: S.S., P.L., L.R.K., and R.E.; Writing: S.S., P.L., K.P.W., and R.E.; and Review and editing: S.S., P.L., L.R.K., A.A.C., M.B.L., J.T.F., K.P.W., and R.E.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Not relevant—no contact to any patients, register study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.