
Abstract
Trigger digit, Dupuytren’s disease, and ganglion cysts are 3 common disorders treated by hand surgeons. Despite the varying nature of their pathology, these 3 entities can all present as a mass at the flexor crease in the distal palm. The regional similarity of these presentations can make diagnosis more difficult. In this paper, we describe a simple clinical exam method that can assist in distinguishing between trigger digit, Dupuytren’s disease, and flexor sheath ganglion cysts.
Trigger digit, Dupuytren’s disease, and ganglion cysts are 3 common disorders treated by hand surgeons. All 3 entities can present with a mass at the flexor crease in the distal palm. Trigger digit is caused by pathological inflammatory changes in the retinacular tendon sheath and on the peritendinous tissue it encloses.1-3 This ultimately leads to hypertrophy of one or both these structures, which progressively restricts the motion of the flexor tendon in its sheath. 4 Clinically, this is manifested by symptoms of locking and clicking, most commonly occurring at the A1 pulley of the ring finger.1,4 Lack of full motion due to painful triggering or locking can lead to secondary contracture of the proximal interphalangeal (PIP) joint. 1
The finding of a flexion contracture of the digit is not unique to a locked trigger digit, but is often the clinical presentation of Dupuytren’s disease.4 -7 Pathologically, Dupuytren’s is a disease of the palmar fascia presenting as a formation of fibromatous nodules and cords that can result in flexion contracture and decreased hand function.8 -12
The most common lumps encountered in the hand and wrist region are ganglion cysts. 13 Although the pathology is not completely clear, they are thought to represent outpouching of synovial membranes of joints and tendon sheaths. At the palmar aspect of the metacarpophalangeal (MCP) joint, the flexor sheath ganglion is the third most common location for a ganglion cyst in the hand, comprising 7% to 12% of hand and wrist ganglions.13,14 They generally arise from the A1 or A2 pulley of the flexor tendon sheath and present as a small, firm, minimally mobile mass near the proximal digital crease or MCP joint.13,15 As these 3 entities tend to arise in similar locations on the distal palm (as shown in Figure 1), we have described typical physical findings unique to each pathology that will help the clinician distinguish between these 3 regionally similar but distinctly different clinical entities.
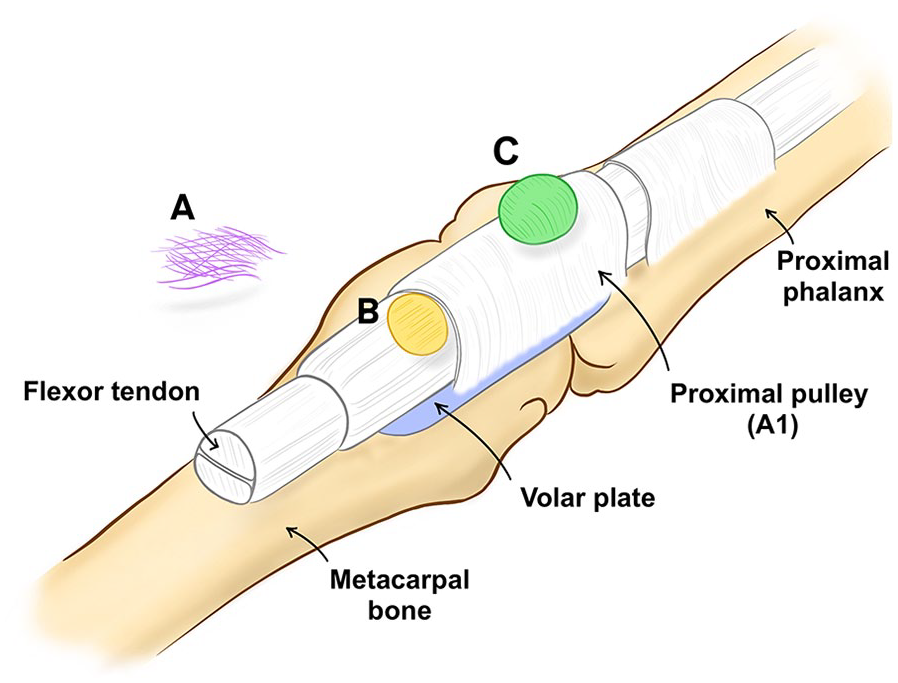
Illustrative depiction of the flexor pulley system overlying the metacarpal bone and proximal phalanx. 16
Clues to the diagnosis can be gleaned by history and the physical examination, and these should all be considered. This report describes an additional specific physical examination test that can help differentiate the 3 entities.
The clinician palpates the mass in the A1 pulley region with one hand while passively flexing and extending the patient’s MCP joint or the PIP joint in a sequential manner while holding the other joint without motion. The motion of the palmar mass is compared when passively flexing and extending the PIP joint, to the motion of the mass when moving the MCP joint. Ganglion cysts will move proximally and distally with passive flexion of the MCP joint; however, they will not move with excursion of the flexor tendon (ie, PIP motion alone). This is because the A1 pulley—the typical site of the origin of the ganglion—has its origin on the palmar plate which moves proximally and distally with MCP joint motion.
The thickening or nodule in the flexor tendon causing trigger finger will move with PIP motion, but not with MCP motion, when the PIP is held in extension. Palpable nodules from Dupuytren’s disease will not move during passive excursion of the PIP or MCP joint. In addition, the clinician may not be able to fully passively extend the patient’s MCP or PIP joint if a flexion contracture is present, but enough flexion is usually present to complete this test.
In summary, distinguishing between a flexor sheath ganglion, trigger digit, and Dupyutren’s may be accomplished with a detailed physical examination of the MCP region of the affected digit. Differential motion of the mass with PIP or MCP motion can be informative. A proper diagnosis will facilitate proper treatment and minimize patient morbidity. Advanced imaging is typically not required for proper diagnosis.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This article does not contain any studies with human or animal subjects.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.