
Abstract
Background:
To review the available literature on Darrach and Sauvé-Kapandji (SK) procedures and perform a systematic review to identify differences in clinical outcomes. We hypothesized that SK would have a higher complication rate without significant clinical benefit.
Methods:
A literature search was conducted using PubMed, EMBASE, Cochrane Library, and SCOPUS (from inception to January 2020) to identify studies evaluating outcomes of Darrach and SK procedures. Primary outcome measures included the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) score, range of motion, grip strength, complications, and overall satisfaction.
Results:
A total of 103 articles were identified and screened, and of these, 44 full-text articles were used for data extraction and qualitative analysis. Outcomes were similar for QuickDASH scores, grip strength, and range of motion, as was overall satisfaction. Specifically, satisfaction rates for stabilized SK and Darrach procedures in patients without rheumatoid arthritis were comparable at 70.2% and 72.6%, respectively. Average QuickDASH scores were similar (21 for Darrach and 29 for SK). Mechanical symptoms due to stump instability occur with either procedure but were higher with the Darrach procedure (12.5% compared with 6.8%). The SK had more surgery-related complications such as nonunions (2.3%), symptomatic hardware, and reoperations (6.8% compared with 3.2%).
Conclusions:
Both Darrach and SK procedures provide comparable satisfaction rates regardless of the underlying pathology. Improvement in range of motion, strength, and overall function is similar for both procedures; however, the reoperation rate is higher with SK.
Introduction
Ulnar-sided wrist pain due to distal radioulnar joint (DRUJ) arthritis continues to present a clinical challenge for hand surgeons. Distal radioulnar joint arthritis can be due to underlying inflammatory diseases such as rheumatoid arthritis (RA), primary osteoarthritis (OA), post-traumatic arthritis including sequelae of distal radius malunions, or congenital deformities. Symptoms are characterized by pain over the ulnar aspect of the wrist, typically worse with pronation and supination. Forearm rotation can be associated with crepitus and is often decreased or associated with instability of the distal ulna. Initial management includes activity modification and bracing although no conservative management has been shown to be superior. After conservative treatment modalities have been exhausted, surgical treatment can be considered to alleviate pain and increase function. Two commonly performed procedures are the Darrach resection, in which the ulnar head is removed, and the Sauvé-Kapandji (SK) procedure, which involves arthrodesis of the DRUJ with a more proximal ulnar osteotomy to create a mobile pseudoarthrosis.1,2 The goals of surgical treatment are to decrease pain, maintain forearm rotation, increase grip strength, and restore overall function.
Resection of the distal ulna, first mentioned by Malgaine in 1855 for an irreducible DRUJ dislocation and later described for more broad indications of DRUJ pathology by Moore in 1880, was ultimately popularized by William Darrach in 1912. 3 Noted complications included instability of the ulnar stump, radioulnar convergence, and subluxation of the extensor carpi ulnaris tendon. With loss of the ulnar-sided structural restraint provided by the ulnar head, ulnar translation of the carpus can occur in the setting of inflammatory arthritis and associated soft tissue compromise.
Owing to the historically unpredictable results and frequency of complications with the Darrach procedure, Sauvé and Kapandji described an alternative procedure in 1936 that combined a fusion of the DRUJ with a more proximal osteotomy of the ulna to create a mobile pseudoarthrosis permitting forearm rotation. 2 The goal was to create a more stable wrist, prevent carpal migration, and decrease ulnar stump instability. This procedure, however, is technically more demanding, requires sufficient bone stock and quality, and has its own set of complications, including nonunion of the arthrodesis site, hardware prominence or irritation, and even fractures of the distal radius.4-7
Various soft tissue modifications have been developed to address stump instability for both procedures, and complication rates in general vary widely in the literature, depending on patient factors, underlying etiology of the DRUJ pathology, and the outcomes measured. 5 In addition, some argue that complications do not necessarily correlate with ultimate satisfaction rates. 8
Conventionally, Darrach resection has been recommended for elderly or low-demand patients and the SK procedure for younger, more active patients. 9 However, there is very little evidence that substantiates this algorithm. The goal of this review was to analyze the current literature on Darrach and SK procedures to delineate clinical outcomes, satisfaction, and complication rates and to better define indications.
Materials and Methods
A literature search was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines using PubMed, EMBASE, Cochrane Library, and SCOPUS (from inception to January 2020) databases. Key words used in the search were related to Darrach and SK procedures (“Darrach,” “Sauvé-Kapandji,” “Ulnar head resection,” “Resection of distal ulna,” “DRUJ arthritis,” “ulnar instability,” “ulnar abutment,” and “ulnar impingement”). The titles and abstracts of all citations were screened for potential relevance by 2 reviewers, and disagreements at any stage were resolved by a third reviewer prior to full-text evaluation.
Studies were included if they had at least 6 months of follow-up, were in English, peer-reviewed, included a minimum of 3 cases, and reported the outcomes of Darrach or SK procedure performed for DRUJ pathology. Articles describing treatment of acute trauma, congenital anomalies, or tumor resections/reconstruction were excluded. Data were extracted from the text, tables, and figures of all eligible studies and included baseline demographic data, the primary outcome measures of pain and mechanical symptoms, as well as secondary outcome measures: range of motion, grip strength, radiographic measurements, and patient-reported outcomes such as the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) score, overall satisfaction, and complications. Range of motion (ROM) and grip strength were only included if they were reported in degrees and in pounds/kilograms, respectively, before and after the procedure.
Data Analysis
Few studies included standard deviations, preventing effect size calculations for each operation in the individual studies. Percentages for mechanical symptoms, reoperations, and other complications were recorded based on reports of instability, complaints indicative of instability (ie, clicking), and radiographs indicative of instability or impingement. We calculated weighted means and ranges of means for final ROM.
A semiqualitative satisfaction rating scale classified patient outcomes into 1 of 3 categories. Based on verbiage from each individual paper using outcome measures such as Mayo wrist scores, visual analogue scales (VAS), and satisfaction surveys, a patient categorized as excellent or good and without pain was then categorized as “Satisfied.” A patient without change in any of the outcome measures and fair or mild pain was categorized as “Unchanged.” Documentation of worse symptoms, severe pain or dissatisfaction with the procedure, was categorized as “Dissatisfied.”
Results
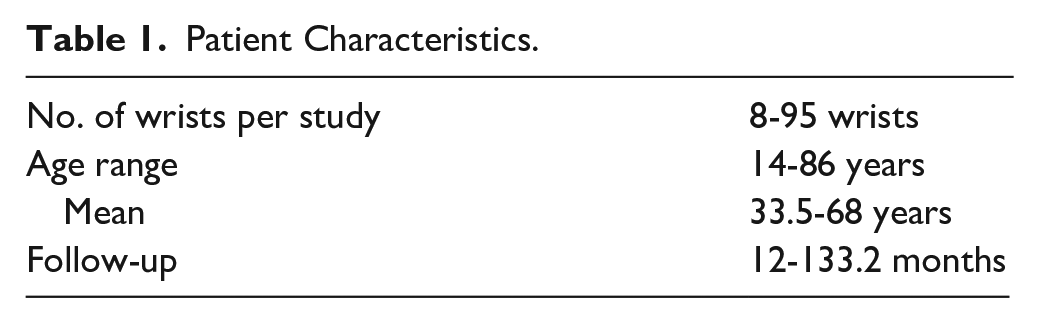
After the review process (Figure 1), 44 articles were used for analysis.8-52 Patient characteristics were recorded from articles in which this information was available (Table 1). Although a minimum of 6-month follow-up was required to meet inclusion criteria, the shortest follow-up in the studies included was 12 months.
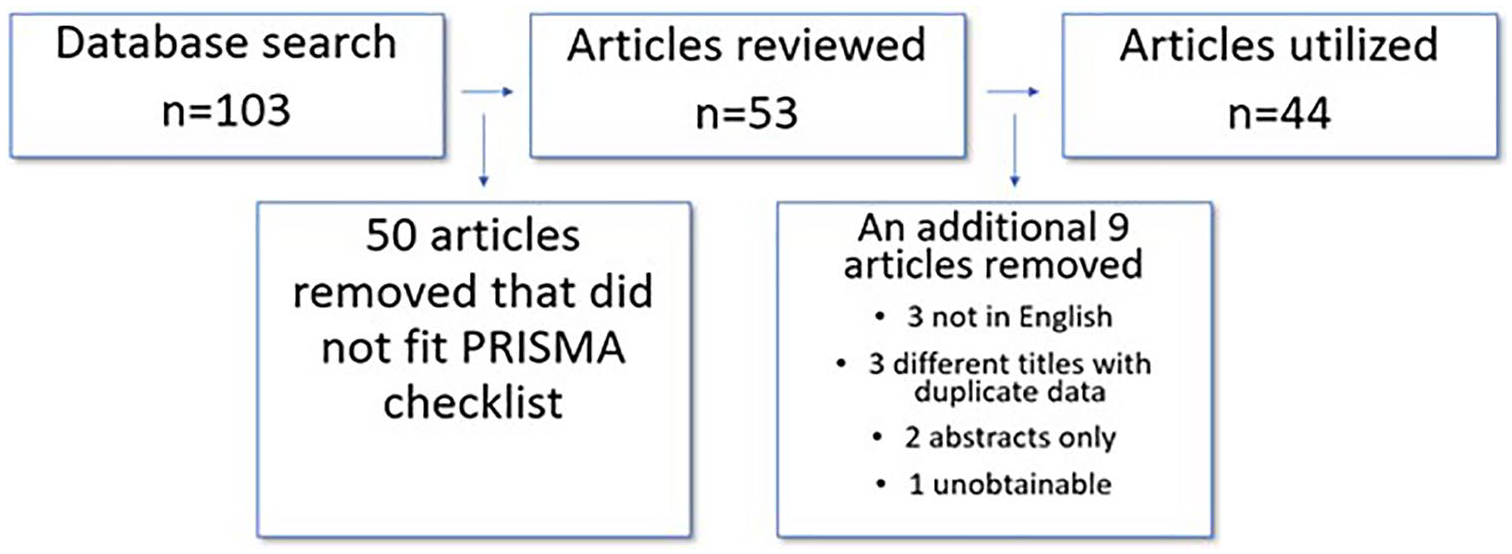
Article inclusion process for systematic review.
Patient Characteristics.
Five of 44 studies reported QuickDASH scores (Table 2). The average postoperative scores were 29 and 21 (SK and Darrach, respectively). There were no reported QuickDASH scores for Darrach patients with RA. Eight studies reported grip strength, which was converted to kilograms (Table 3) and subdivided based on arthritis type. The average postoperative strength for patients without RA was 23 kg for SK and 23 kg for Darrach. The final postoperative motion was collected from 25 articles, and average means for the SK and Darrach procedures were 78 and 78 for pronation, 82 and 78 for supination, 35 and 43 for flexion, and finally 41 and 49 for extension, respectively, reflected in the forest plot shown in Figure 2.
QuickDASH Final.

Note. QuickDASH = Quick Disabilities of the Arm, Shoulder, and Hand; SK = Sauvé-Kapandji; RA = rheumatoid arthritis.
Grip Strength.
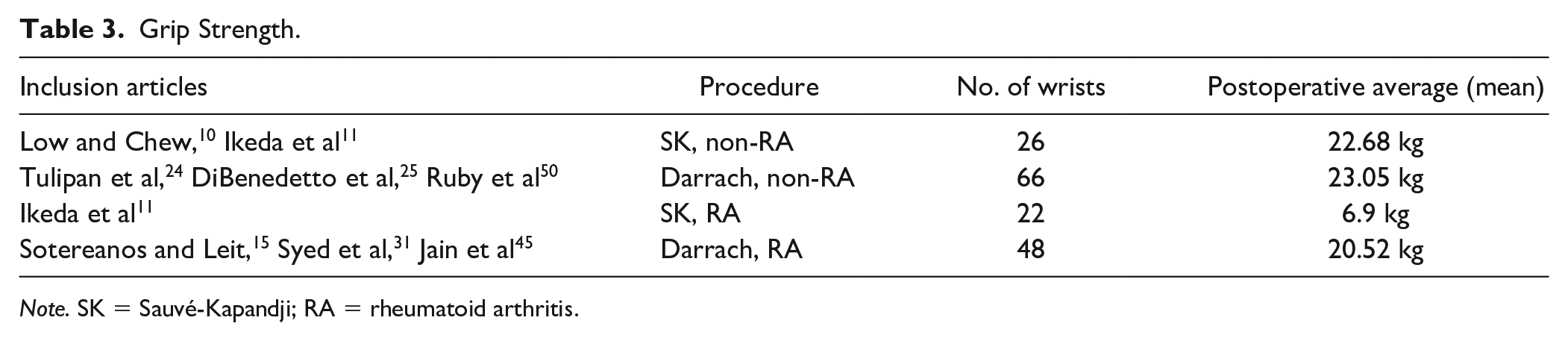
Note. SK = Sauvé-Kapandji; RA = rheumatoid arthritis.
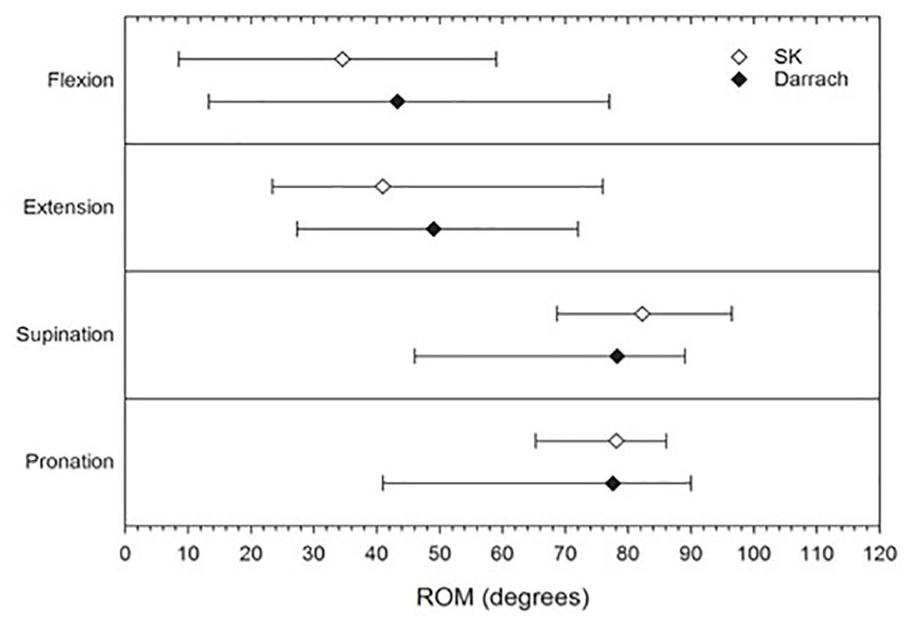
Final range of motion averages between SK and Darrach procedures.
Mechanical symptoms were reported in 39 articles involving a total of 1258 wrists. Whether painful or not, the rate was 13% with Darrach and 7% with SK (Table 4). Unique to the SK group, the nonunion rate was 2%, and the reoperation rate was higher than with the Darrach procedure (7% compared with 3%) (Table 4). The dorsal cutaneous branch of the ulnar nerve injury was also noted in 9 patients post-Darrach compared with 11 patients post-SK (Table 4).
Complications.
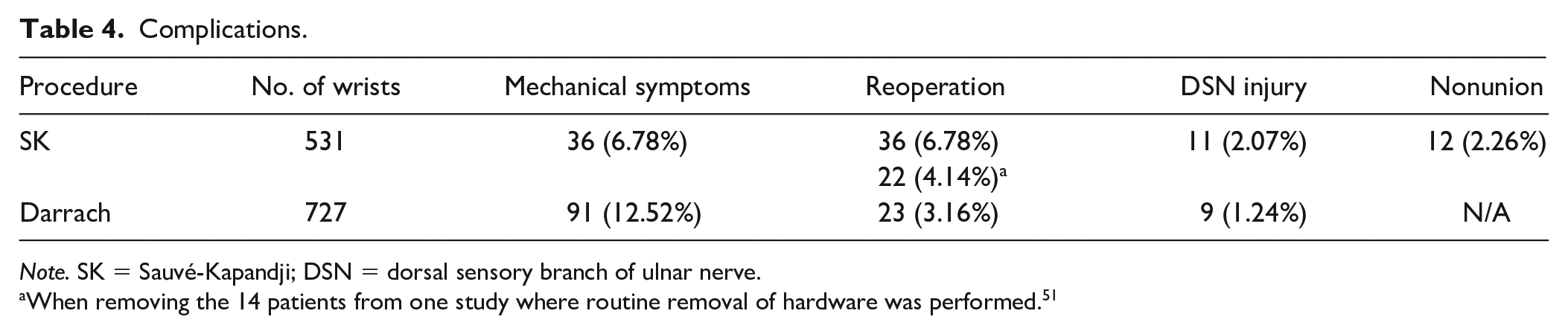
Note. SK = Sauvé-Kapandji; DSN = dorsal sensory branch of ulnar nerve.
When removing the 14 patients from one study where routine removal of hardware was performed. 51
Twenty-nine articles reported patient satisfaction, which was subcategorized for soft tissue stabilization and arthritis type (Table 5). Stabilized SK and Darrach procedures in patients without RA were comparable at 70% and 73%, respectively. The highest satisfaction group consisted of patients with RA stabilized after Darrach (93%), and the least satisfied groups were those nonstabilized after SK in patients without RA (25%) and those nonstabilized after Darrach in those with RA (15%).
Patient Overall Satisfaction.
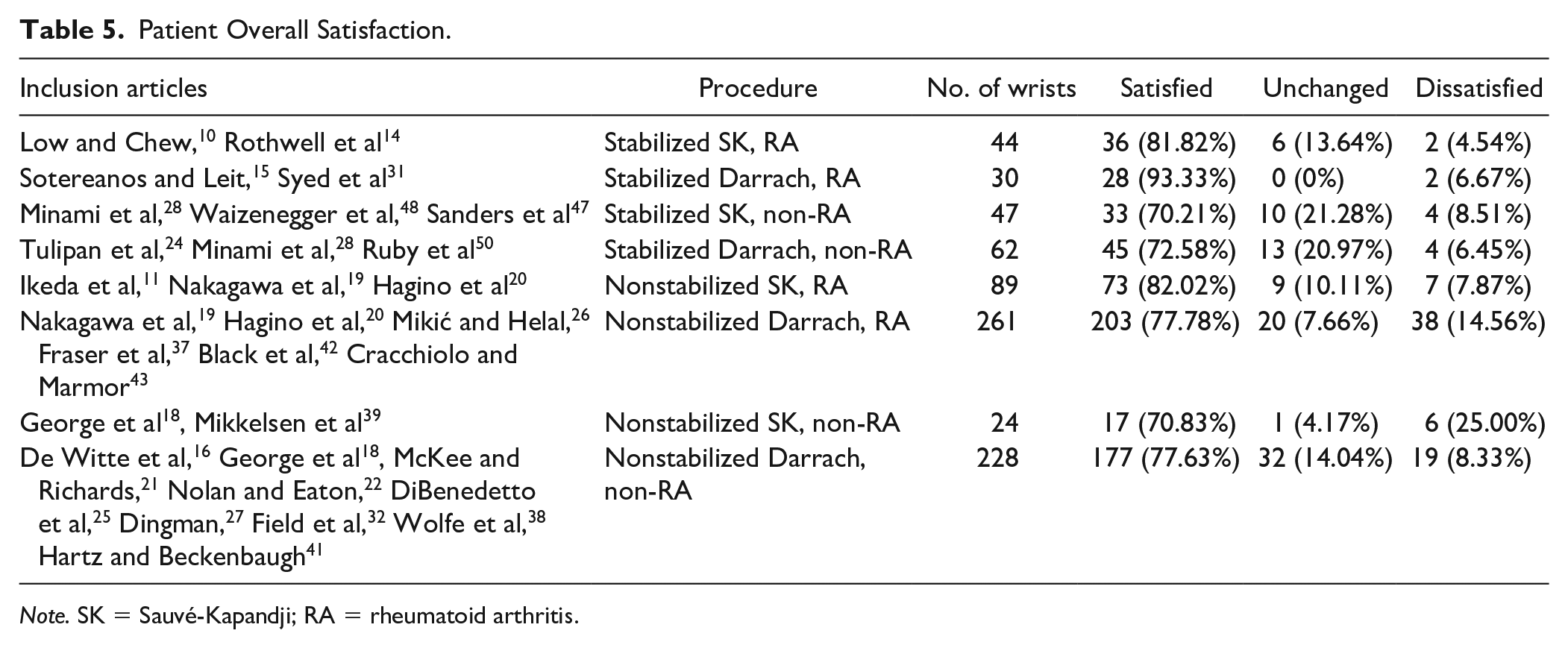
Note. SK = Sauvé-Kapandji; RA = rheumatoid arthritis.
We purposefully did not include P values, as the data from the various studies included in our analysis have inconsistent and variable methods and outcome measures, and therefore running a statistical analysis violates the assumptions these tests are based on. For that reason, we thought it best to use a qualitative approach to interpret the data.
Discussion
The Darrach resection and SK procedures were designed to reduce pain and increase function for patients with recalcitrant DRUJ arthritis. In this review, more than 70% of patients achieved satisfactory outcomes regardless of which procedure was performed. QuickDASH scores were similar (or below the threshold of clinical importance), and ROM and grip strength for patients without RA were near equal for both procedures. 53
Despite the intent of Sauvé and Kapandji, impingement was still a problem for both procedures, and while our report indicates that this complication was more likely following a Darrach resection, statistical analysis was not possible. In addition, impingement or stump instability did not necessarily correlate with patient satisfaction, and the inclusion of a variety of additional soft tissue stabilization procedures in many of the reports made definitive conclusions regarding the clinical importance of this observation difficult. These stabilization efforts did seem to improve patient satisfaction rates, although the data were too heterogeneous or nonspecific to provide more insightful analysis. Nonunion and reoperation rates were complications unique to the SK procedure and skewed overall complication rates and may have affected patient satisfaction. One author removed all SK screws regardless of the clinical symptoms, which artificially increased the number of reoperations in the SK group but does not reflect common clinical practice. 51 Furthermore, techniques have evolved and hardware and instrumentation have improved, so some of the complications historically known to be common may be less frequent in the more recent literature.
Like many of the other outcome measures, reporting of radiographic arthritis/degenerative changes, ulnar impingement/radioulnar convergence, ulnocarpal distance ratio, carpal radial distance ratio, and carpal height ratio were too inconsistent to allow specific meaningful comparisons. Other limitations of this review include the potential for publication bias. 54 There is also a lack of information regarding disease (RA) severity or treatment and changes in relative complication risk related to the dramatic evolution of medical management of RA that has occurred over the spectrum of years included in our analysis.
Unfortunately, we were unable to fully analyze various subgroups and their outcomes in more detail due to the heterogeneity of patients included in the individual studies available for review, as can be a limitation of systematic reviews such as this one. We purposefully did not pursue a quantitative statistical analysis in this context of trying to synthesize data from the studies that had varying methods or reporting their outcome measures, and instead chose to use a qualitative approach in interpreting the data.
This review does not support the conventional wisdom that the SK procedure restores better function or has less complications despite the increased technical effort necessary. Sauvé-Kapandji patients report mechanical symptoms at about half the rate of Darrach patients, but overall they are quite low across both groups. Sauvé-Kapandji patients are more likely to undergo a reoperation and have a small rate of nonunions, consistent with rates of fracture or other nonunions reported more broadly. Higher mechanical symptoms with Darrach must be weighed against the higher reoperation rate associated with SK although both surgeries provide high percentages of satisfactory results.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article is a review and did not study new human or animal subjects.
Statement of Informed Consent
Informed consent was not required for this study as it does not contain any identifying patient information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.