
Abstract
Background:
This study reports the clinical results following primary repair of distal biceps tendon ruptures more 6 weeks after injury.
Methods:
A retrospective review of distal biceps tendon repairs performed by 8 different hand surgeons from January 1, 2015 to October 15, 2020 was performed. Patients with complete tears surgically treated ≥6 weeks after injury without tendon graft were included. Thirty patients qualified and underwent chart review for complication and range of motion (ROM) data. They were contacted for final patient-reported outcome measures (PROMs) using Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) and Patient Reported Elbow Evaluation (PREE) scores. Final PROMs were obtained from 21 patients with an average follow-up of 31.3 months (range: 4-71 months).
Results:
Average time from injury to repair was 71 days (range: 42-204). The average QuickDASH score was 6.6 (±6.2) and PREE score was 7.8 (±8.0). The amount of elbow flexion necessary to complete the repair was documented in 21 patients and averaged 64º (±10º). Postoperatively, patients achieved an average extension/flexion of 1º (±1º) to 138º (±2º) and pronation/supination of 76º (±4º) to 77º (±3º). Complications were reported in 14 patients (47%) and included 2 re-ruptures, 1 adhesive scar formation, 1 superficial infection, 1 intraoperative lateral antebrachial cutaneous nerve laceration, 12 neuropraxias, and 1 case of heterotopic ossification (HO).
Conclusions:
Primary repair of chronic distal biceps tendon tears greater than 6 weeks from injury demonstrated excellent PROMs and elbow ROM. However, the complication rate may be higher than early repair.
Introduction
While repair of distal biceps injuries commonly leads to good functional results, repair of chronic injuries has also been associated with increased complication rates.1,2 Additionally, chronic tears of the distal biceps commonly result in tendon retraction, and primary repair may be impossible without significant flexion of the elbow to establish contact between the tendon and bone. Concern that high-flexion tendon repairs would result in re-rupture or chronic elbow flexion contractures has led some to advocate grafting to extend the length of the distal biceps tendon. However, grafting of chronic distal biceps tears has been associated with worse patient-reported outcomes than primary repair, and prior literature demonstrates equivalent results between a high-flexion repair group and a control group.3,4
Despite the increased difficulty and complication rates of chronic distal bicep repairs, several authors have published promising results.5,6 The aim of this paper is to report the results of a cohort of patients with chronic (≥6 weeks) distal bicep tears who were treated by multiple surgeons with primary repair through an anterior approach to the radial tuberosity. Our hypothesis was that these patients would achieve excellent long-term outcomes and final range of motion (ROM) with an acceptable complication rate.
Methods
Patients
This study is a retrospective case series which includes prospectively collected patient-reported outcome data. With institutional review board approval, we queried all distal bicep repairs done at our center from January 1, 2015 to November 1, 2020 using a surgical database by Current Procedural Terminology (CPT) code 24342. There were 288 patients initially identified within the database. Inclusion criteria included primary repair of a complete distal biceps rupture ≥6 weeks after the day of injury without graft augmentation. After initial screening chart review, 104 patients underwent repair in less than 6 weeks after injury; 99 patients underwent surgical repair of a partial tear of the biceps tendon; 32 patients were treated for tear of the distal triceps, which has the same CPT code; 14 patients underwent distal biceps repair with tendon grafting; 5 patients had a distal biceps revision repair; 1 patient was excluded due to a planned staged repair; and 3 patients did not have sufficient documentation for evaluation. Thus, 30 patients were deemed eligible for inclusion in the present study.
Patient demographic data were collected including age, gender, body mass index (BMI), smoking status, and work status. Preoperative Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) scores were available for 19 patients and were collected during chart review. Surgical details such as fixation method and time from injury to repair were noted. The amount of elbow flexion required to complete the repair was noted if specified in the operative report.
Surgical Technique
All surgeries were performed by 8 separate fellowship-trained hand surgeons within the same practice. The surgical repair technique was at the discretion of the treating surgeon. All surgeons used a single, anterior incision for their initial approach to the radial tuberosity. An accessory incision was made proximally in 11 (37%) cases to aid in the identification and release of the biceps tendon due to retraction or scarring. Once the biceps tendon had been retrieved, any remaining pseudotendon was trimmed proximally to healthy-appearing tendon. The tendon was then secured and reduced to bone. Elbow flexion was used to facilitate opposition of the tendon to bone when necessary, but fractional lengthening of the tendon was not performed in any cases.
A cortical button was used for fixation in all cases. Depending on surgeon preference, either the Endobutton® (Smith and Nephew, Andover, Massachussetts) or the Ziploop® (Biomet, Warsaw, Indiana) systems were used. The amount of elbow flexion required to repair the tendon to bone was documented in 21 cases.
Outcomes
Patients were contacted by phone to obtain final patient-reported outcome measures (PROMs) including the Patient Reported Elbow Evaluation (PREE) and the QuickDASH which have been previously validated and used for the assessment of distal biceps repair outcomes.7-10 At the time of the phone call, informed consent was obtained from the patients for inclusion in the study. Patients were determined to be lost to follow-up if they did not answer the phone or return the call after 3 attempts were made. Of the patients eligible for the study, 21 agreed to participate in providing outcome scores including 14 patients who were documented to require elbow flexion to complete the repair intraoperatively. Postoperative ROM was assessed through review of the motion documented at each therapy visit. Twenty-eight patients completed a prescribed course of therapy as directed by the treating surgeon and therapists with ROM data available (Figure 1). All patients were placed in a long arm splint postoperatively and transitioned to a Bledsoe brace 1 to 2 weeks after surgery to allow motion while limiting extension. Timing of therapy visits and the progression of terminal extension occurred at the discretion of the treating surgeon. On average, all ROM restrictions were removed 6.8 (±0.7) weeks after surgery. No static or dynamic bracing was used to assist in the recovery of elbow motion postoperatively.
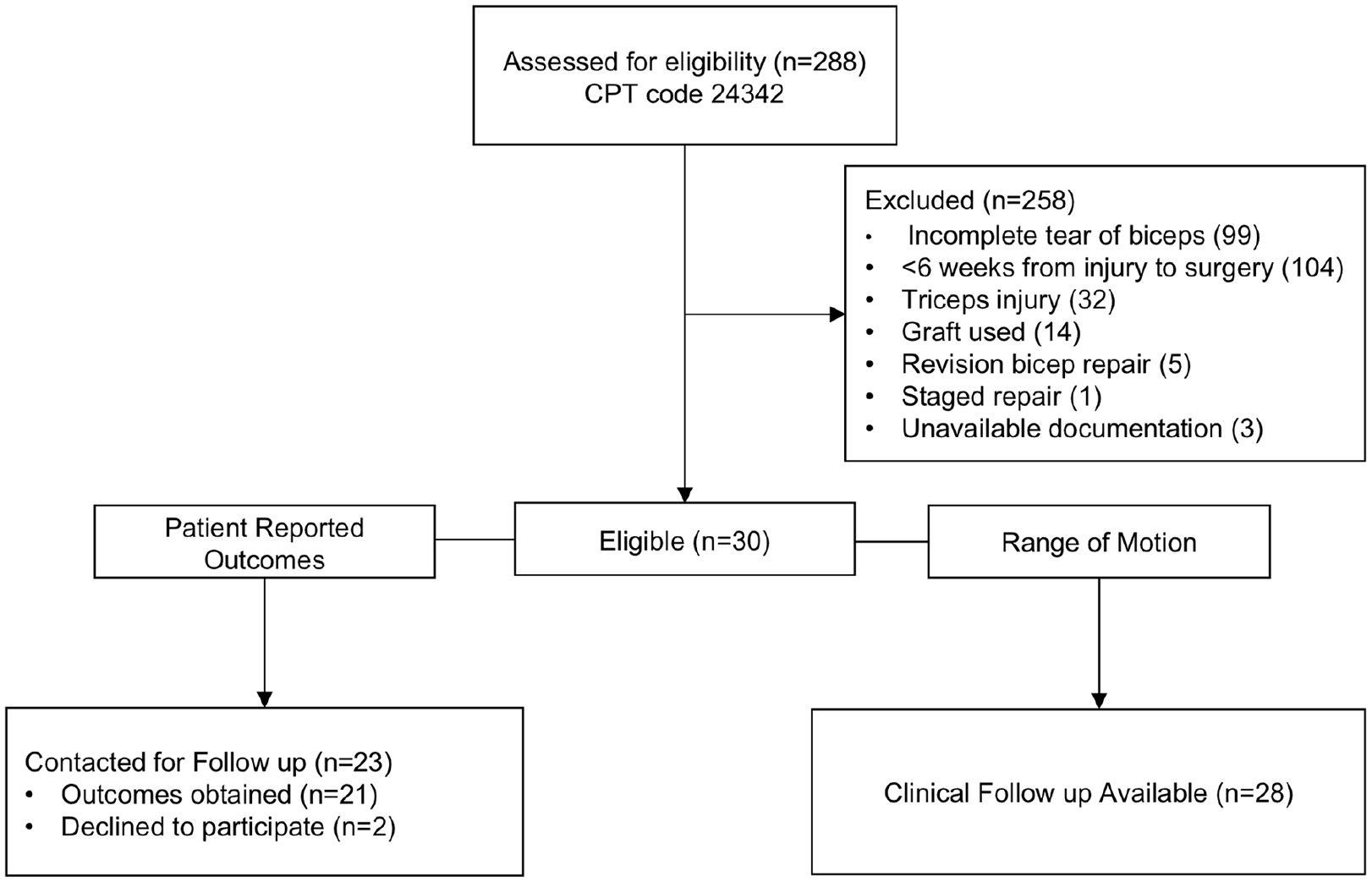
Diagram demonstrating the progression of patients through the study.
Postoperative complications were noted through review of the patients’ postoperative records. Patients who underwent additional surgery at our center were recorded as reoperations if the additional surgery pertained to the original distal biceps repair.
Statistical Considerations
In all, 95% confidence intervals for all measurement values are presented using a Student’s T distribution.
Results
Demographics
All eligible patients for the study were male with an average age of 52.7 (range: 38-80). The average BMI was 32.6, and 5 patients (17%) were active smokers. Two (7%) patients had a preoperative diagnosis of diabetes. Twenty-eight (93%) patients were actively employed at the time of surgery, and 13 (43%) presented with the injury as part of a Worker’s Compensation claim. The average time from injury date to surgical repair averaged 71 days (range: 42-204 days), and the median time to surgery was 58 days (interquartile range: 45-88 days) (Table 1).
Characteristics of Patients Included in Study.
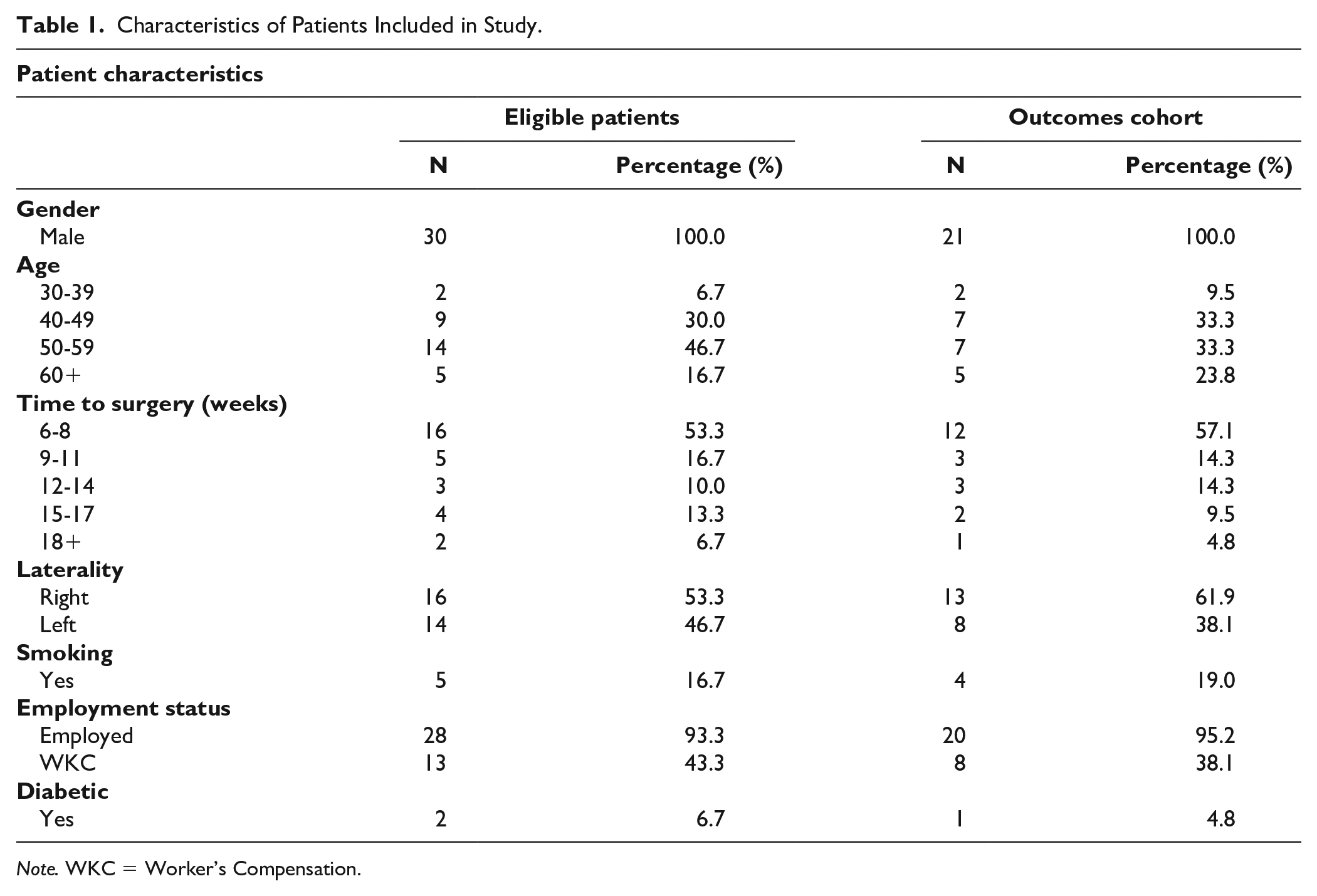
Note. WKC = Worker’s Compensation.
Delayed presentation after injury contributed to the need for late repair in 19 patients (63%). A delayed diagnosis or referral from the initial evaluating provider contributed to delayed repair in 8 (27%) patients. Two (7%) patients had a greater than 3-week interval from diagnosis by the treating surgeon to surgical repair contributing to a delayed repair. Finally, 1 patient who ultimately underwent repair 204 days after injury was significantly delayed in undergoing surgery while awaiting insurance approval. Of all patients, only 1 was observed for a period of 1 month for improvement before undergoing surgery.
Outcomes
Final outcome scores were obtained with an average follow-up of 31.3 months (range: 4-71 months). The average QuickDASH score at final follow-up was 6.6 (±6.2), and the average PREE score at final follow-up was 7.8 (±8.0). Pre-operative QuickDASH scores were obtained a median of 2.6 weeks before surgery and averaged 46.1 (±12.0). Twenty-one patients were documented to require elbow flexion to complete the repair intraoperatively, which averaged 64º (±10º) and ranged from 20º to 95º.
Postoperatively, patients achieved an average extension/flexion of 1º (±1º) to 138º (±2º) and pronation/supination of 76º (±4º) to 77º (±3º). On average, patients regained their final amount of extension at 10 (±2) weeks postoperatively. Three patients failed to achieve extension to at least 0º postoperatively. Of those patients, 1 had a 5º flexion contracture at the completion of their therapy course which finished 18 weeks postoperatively. Another patient’s postoperative course was complicated by re-rupture, and he had a 5º flexion contracture 18 weeks after his primary surgery and 8 weeks after his revision surgery. The other patient had a 15º extension deficit, which was equal to his contralateral elbow extension.
Complications
Postoperative complications occurred in 14 patients (47%) and included 2 re-ruptures, 1 adhesive scar formation, 1 superficial infection, 1 intraoperative lateral antebrachial cutaneous nerve (LABCN) laceration, 9 LABCN neuropraxias, 3 radial sensory nerve (RSN) neuropraxias, and 1 case of radiographic heterotopic ossification (HO) (Table 2).
Postoperative Complications Within Study Cohort.
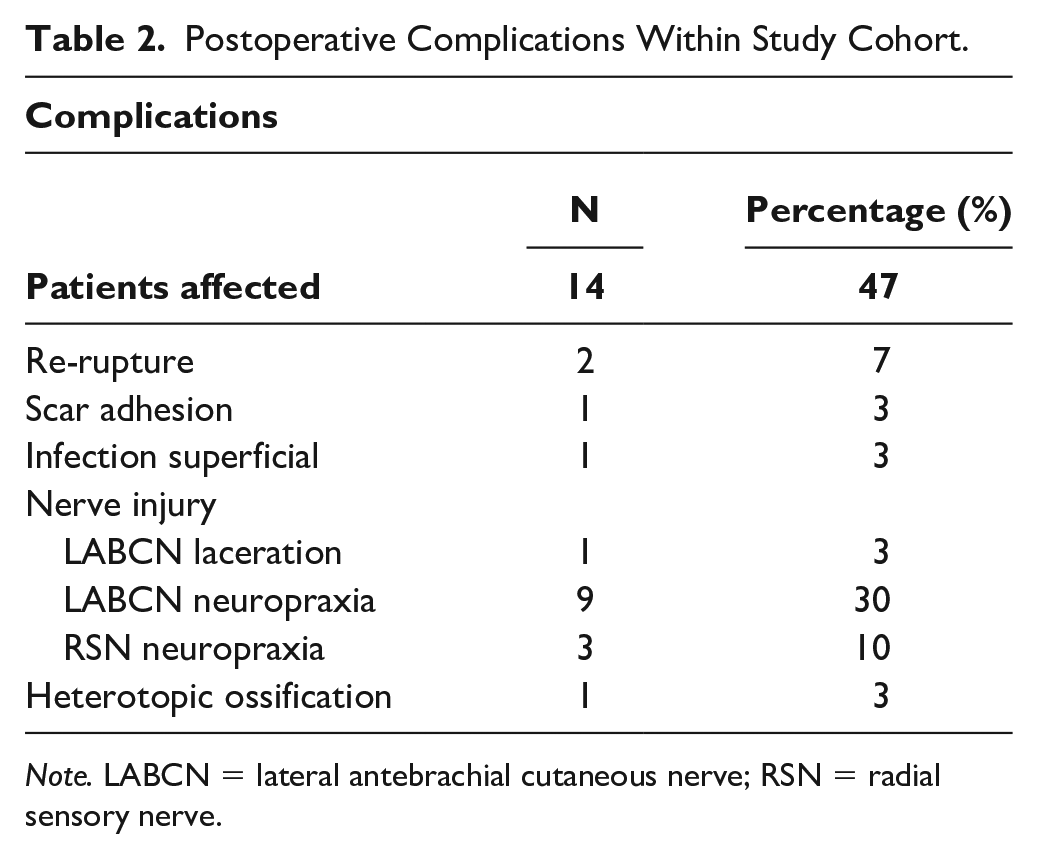
Note. LABCN = lateral antebrachial cutaneous nerve; RSN = radial sensory nerve.
The 2 patients who experienced re-rupture were treated with revision primary distal biceps repair without graft augmentation. One patient re-ruptured 2 weeks after his initial repair, which was performed 43 days after the initial injury. This patient regained flexion to 140º but had a flexion contracture of 5º following a course of therapy after his revision surgery. When contacted 14 months after primary repair and subsequent revision, the patient noted continued disability with a QuickDASH of 54.5 and PREE of 71. The other patient, who had surgery 56 days after the initial injury, fell on an outstretched arm, and re-ruptured 1 month after the initial repair. He was able to regain flexion/extension of 0º/140º postoperatively. This patient was contacted 12 months after his primary surgery and 10 months after his revision repair and demonstrated a good final result with a QuickDASH of 2.3 and PREE of 2.3. No other patients were noted to have abnormal biceps contour postoperatively.
One patient was diagnosed with scar adhesions at the site of an accessory incision which dimpled and caused pain with biceps contraction. This patient was taken back to the operating room and treated with scar excision alleviating the symptoms.
There was 1 superficial postoperative infection in the cohort which resolved with a course of oral antibiotics. One laceration of the LABCN was noted intraoperatively. It was repaired during the original surgery, but the patient was noted to have continued loss of sensation in the distribution of the LABCN 1 year postoperatively.
One patient was diagnosed with radiographic HO postoperatively. This was clinically insignificant as the patient did not require reoperation or have any limitations to his ROM at the completion of his therapy course. Twelve (40%) patients were diagnosed with neuropraxias of the LABCN or RSN postoperatively, all of which resolved in the early postoperative period with no permanent nerve symptoms.
Discussion
This study indicates primary repair of chronic distal biceps tears is a viable treatment option 6 weeks or greater from the time of injury. The final QuickDASH and PREE scores demonstrate excellent patient-reported outcomes postoperatively. Additionally, patients were consistently able to achieve at least 0º of extension postoperatively despite many patients requiring high flexion angles of the elbow to complete the repair.
Prior studies have provided evidence in support of primary repair of chronic distal biceps tears. Zemen et al 6 reported on a series of 20 patients who underwent primary repair of a distal biceps tear using a cortical button by a single surgeon at least 4 weeks after the day of injury with 35% of patients having surgery less than 6 weeks after injury and an average time to repair of 10 weeks. The authors reported significantly improved Mayo Elbow Performance Score (MEPS) and Oxford Elbow Scores (OES) postoperatively at an average follow-up of 26 months and an average final MEP of 100 and OES of 48. They also reported no re-ruptures of the repairs and only a 14% incidence of postoperative neuropathy. Haverstock et al 5 reviewed the results of 16 patients who were treated with distal biceps repair using a 1- or 2-incision technique using suture anchors or bone tunnels greater than 3 weeks after injury (mean = 37 days). The authors compared them to a matched cohort of patients who were treated less than 3 weeks (mean = 10 days) after injury, and they showed no significant differences in PREE, DASH, or American Shoulder and Elbow Surgeons elbow questionnaire at final follow-up. The delayed repair group did show a higher rate of complications than the acute repair group (63% vs. 29%). However, 90% of the reported complications in the delayed repair group were self-limited neuropraxias and no re-ruptures were reported.
This study showed reliable return of motion despite the average elbow flexion of 64.1º at the time of repair. These findings reinforce the previously published findings of Morrey et al 4 who reviewed 23 patients who required ≥60º or more elbow flexion to complete the repair. The authors found reliable return of motion and no difference in pain, MEPS, or return to work when compared to a “low-flexion” repair control group. Frank et al 3 compared the outcomes of 19 patients who were treated with semitendinosus distal biceps reconstruction ≥3 weeks after injury with 16 patients used for the delayed repair group in the Haverstock et al 5 paper. While the patients treated with tendon reconstruction had a significantly longer delay from injury to surgery (266 vs. 37 days, P < .001), the authors found significantly improved outcomes in PREE and Mayo Elbow Performance Index in the primary repair group indicating a potential benefit of primary repair.
The overall complication rate in this study was 47%, which supports prior reports of increased complication rates with repairs of chronic distal biceps ruptures. 2 It is important to note that most of the complications were self-limiting, and they did not have a lasting effect on outcomes. Cain et al 2 showed an increased rate of complications (46% vs. 30%) with distal biceps repair ≥4 weeks after injury. However, when assessing for “major” complications, which included posterior interosseous nerve palsy, HO, and re-rupture, the authors reported a rate of 11%. Similarly, this study shows a much higher rate of “minor” complications than “major” complications. Using the criteria described in Cain et al, 2 there was a major complication rate of 11% (3 of 28). Two patients (7%) did undergo revision repair after re-rupture of the tendon, which is a higher rate of re-rupture than many other previous reports of chronic distal biceps repair.2,5,6,11,12 Overall, the results of this study show reliably good outcomes and return of motion after primary repair of distal biceps ruptures ≥6 weeks after injury.
This study has several strengths and provides additional support for attempting primary repair of chronic distal biceps tendon ruptures. To our knowledge, no other study has evaluated a cohort of patients with such chronic injuries. While the patients evaluated by Zemen et al 6 underwent repair at an average of 10 weeks after injury, more than one-third of the included patients were less than 6 weeks out from injury. Additionally, the high duration of average follow-up in this decreases the chances of missing late complications or unknown reoperations outside of the study center. Finally, the inclusion of multiple surgeons in the study may increase the external validity of the results, as they are less representative of 1 surgical technique, 1 implant, and 1 rehabilitation protocol.
Of course, there are several limitations as well. One is the retrospective nature of the study, which likely contributed to the inability to collect postoperative PROMs from all patients. There is significant variability in the duration of follow-up within the cohort ranging from 4 to 71 months which may introduce bias in the results. However, all noted complications occurred within 5 weeks of surgery limiting the risk of missed complications, and PROMs would be expected to continue to improve as time after surgery increases following distal biceps repair. The inclusion of patients treated by multiple surgeons introduces variability in the surgical technique, fixation used, and postoperative treatment protocol; this may be viewed as both a weakness and a strength. While no patients had postoperative ROM deficits which required further intervention, the ROM measurements were obtained retrospectively from previously documented measurements potentially increasing the risk of measurement error as compared to prospectively obtained data. Additionally, complications were determined based on the postoperative evaluations of the treating surgeons which is a possible source of bias.
Importantly, this report does not provide an answer to the question of when a distal biceps tendon rupture is “too chronic” for primary repair. However, the data presented in this study and prior studies support the treatment of many chronic distal biceps tendon ruptures, which may have been previously treated with graft reconstruction, with primary repair. Currently, it is the standard practice of the senior authors (J.A.G. and R.W.H.) to perform primary repair of all chronic distal biceps injuries, with graft reconstruction limited to a rarely used bail-out option, an option not employed by either for more than 5 years.
Footnotes
Ethical Approval
This study was approved by our Institutional Review Board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) with the Helsinki Declaration of 1875, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.