
Abstract
Background:
Previous studies have suggested that proximal row carpectomy (PRC) results in increased contact pressures and decreased contact areas in the radiocarpal joint. Such experiments, however, used older technologies that may be associated with considerable measurement errors. The purpose of this study was to determine whether there was a significant difference in contact pressure and contact area before and after PRC using Tekscan, a newer pressure sensing technology.
Methods:
Ten nonpaired cadaveric specimens were dissected proximal to the carpal row and potted. An ultra-thin Tekscan sensor was secured in the lunate fossa of the radius. The wrists were loaded with 200 N of force for 60 seconds to simulate clenched-fist grip; contact pressure and area was assessed before and after PRC.
Results:
Performing a PRC did not significantly increase mean contact pressure at the lunate fossa compared to the native state (mean increase of 17.4 ± 43.2 N/cm2, P = .184). Similarly, the PRC did not significantly alter peak contact pressures at the lunate fossa (intact: 617.2 ± 233.46 N/cm2, median = 637.5 N/cm2; PRC: 707.8 ± 156.6 N/cm2, median = 728.5 N/cm2; P = .169). In addition, the PRC (0.46 ± 0.15 cm2, median = 0.48 cm2) and intact states (0.49 ± 0.25 cm2, median = 0.44 cm2) demonstrated similar contact areas (P = .681).
Conclusions:
In contrast to prior studies that demonstrated significant increases in contact pressure and decreases in contact area after PRC, our findings propose that performing a PRC does not significantly alter the contact pressures or area of the lunate fossa of the radiocarpal joint.
Introduction
The wrist is a complex joint, involving multiple ligamentous and bony articulations to maintain balanced motion. In the course of scapholunate advanced collapse and scapholunate nonunion advanced collapse, as well as Kienbock’s disease, alterations in ligamentous and bony structures result in modifications in forces across the wrist, producing painful, degenerative changes at the radiocarpal joint.1,2 One treatment option is a proximal row carpectomy (PRC), in which a new articulation is created through excision of the degenerated proximal row. This process, however, is believed to create a new pressure pattern across the radiocarpal joint; by removing 3 bones articulating with the radius and replacing them with one articulation, it would be expected that the reduction in surface area would cause an increase in pressure at the radiocarpal joint, and therefore increase the risk of pain and development of degenerative changes. 3 Patients undergoing PRC, however, typically report significant pain relief, improved grip strength, and improved motion, as compared to their preoperative baseline. 4 Additionally, as compared to the alternative procedure for radiocarpal arthrosis, 4 corner fusion, PRC typically results in improved motion and lower rates of reoperation and conversion to fusion.5-7 Conversion to wrist arthrodesis after PRC is believed to be, at least in part, due to the development of degenerative changes at lunate fossa secondary to an increase in contact pressures.
Pressure changes across the wrist following a PRC have been previously studied.3,8,9 Such experiments used FujiFilm to assess the biomechanical changes that occur with surgical intervention. While FujiFilm was an adequate tool for assessing contact pressure changes across the joint in the late 20th century, it has been shown to have measurement errors as large as 14% to 28%. 10
To our knowledge, no prior study has investigated the role of PRC on contact pressures using Tekscan, a newer technology that has a higher accuracy compared to FujiFilm. Tekscan allows for more specific pressure-sensing due to the presence of a greater number of calibration points, which improve accuracy and reduce error, and for dynamic rather than static measurement of pressure and force across a joint. In this study, we compare the mean contact pressures, peak contact pressures, and contact area at the lunate fossa before and after a PRC. Based on the existing literature, we hypothesized that PRC would increase mean and peak contact pressures of the lunate fossa and decrease contact area.
Materials and Methods
This study did not require institutional review board approval due to the use of deidentified cadaveric specimens. The entire study was performed at SUNY Downstate Medical Center. An a priori power analysis was performed in G*Power (v3.1.8.7) based on prior studies analyzing contact pressure before and after PRC. Due to the scant available literature, 2 papers were selected for our power analysis as they reported mean and standard deviations despite differences in methodology.3,8 Each power analysis was performed as a difference between matched pairs test, with 2 tails, alpha set to 0.05, and 80% power. Zhu et al 3 reported an intact mean contact pressure at the lunate fossa in a neutral position of 23.2 ± 3.2 N/cm2 compared to after the PRC, which resulted in a mean contact pressure 136.4 ± 30.7 N/cm2 (P < .001). This study suggested that 3 and 4 cadaveric specimens were needed to achieve 80% and 90% power, respectively. In contrast, a power analysis based on a study by Hogan et al, 8 which reported on the mean contact pressure in the lunate fossa at a neutral position (intact: 41.3 ± 15.4, PRC: 64.9 ± 23.5, P < .001), suggested 9 cadaveric specimens were needed to achieve 80% power. Based on these results, a sample size of 10 nonpaired frozen human cadaveric forearms was selected for this study.
Wrist Preparation
Each specimen was thawed at room temperature for 16 hours prior to testing. The wrists were cut using an oscillating saw approximately 5 inches from the carpal row. All soft tissue approximately 1 inch proximal to the carpal row was removed except for the interosseous membrane, which was left intact. The specimens were then potted in 4-inch cylinders using fiberglass resin.
The radiocarpal joint of each wrist was exposed to allow insertion of the ultra-thin Tekscan sensor (Model 4201, Tekscan Inc, Boston, Massachusetts). Each sensor is 0.178 mm thick and contains a total of 24 rows and 11 columns, creating a total of 264 sensels (or 27.8 sensel/cm2). The total pressure ranges are 5 to 2,000 psi and 34 to 13,790 kPa. A longitudinal incision was made approximately 0.5 cm radial to Lister’s tubercle, and superficial dissection was continued down to the extensor retinaculum. Next, the retinaculum over the third dorsal compartment was incised. The overlying extensor tendons were then retracted to allow exposure of the dorsal capsule. This capsule was then incised to allow exposure of the proximal carpal row and corresponding radiocarpal joint, to allow for insertion of Tekscan sensor. Once the Tekscan sensor was placed in the radiocarpal joint, the joint capsule was sutured closed.
Experimental Set Up
The wrist flexors and extensors were dissected off of the elbow and forearm to allow mounting of the extremities to the Instron device (Instron Model 8874, Instron Corp., Canton, Massachusetts). 11 The potted cadaveric arm was vertically mounted onto the Instron device, with the hand in a clenched-fist position (Figure 1). To secure the fist in a neutral position and prevent any flexion/extension, a metal box was placed around the fist, and filled with sand-filled balloons. The wrist was placed in 20 degrees of extension utilizing a goniometer. These balloons were molded to the fist to prevent movement with wrist loading and ensure even pressure distribution across the metacarpophalangeal joints. The K-scan pressure sensing system software (version 7.70-16I, Tekscan Inc) was calibrated under a series of loads in axial compression using the Instron device, prior to testing.

Experimental set-up. Each specimen was potted in fiberglass resin and inserted into the Instron. Sand-filled balloons were then added to secure the distal aspect of the specimen while a 200 N axial force was applied.
Each wrist was loaded with 200 N of axial force using the 5566 Instron device loadcell. A 200 N force was chosen to simulate a clenched-fist.12-16 This force was applied for 60 seconds, during which time contact pressures and contact areas across the joint were collected using the Tekscan pressure sensing system. These data points were recorded and saved for each specimen cycle on the K-scan software. The loading of the wrists was repeated for all 10 native wrists. A new Tekscan sensor was utilized for each wrist.
PRC Procedure
Following the loading of each native wrist, the dissection was continued to allow removal of the proximal carpal row. First, the sutures were removed from the dorsal capsule to allow removal of the Tekscan sensor and exposure of the proximal carpal row. Next, the scapholunate interosseous ligament was incised and sharp dissection of the soft tissue attachments around the scaphoid was performed to allow removal of the bone. This process was then repeated for the lunate and triquetrum. Care was taken to ensure that the radioscaphocapitate and dorsal radioulnar ligaments remained intact. 17 After the PRC was performed, the capitate articulated with the radius. A Tekscan sensor was again inserted between the radiocapitate articulation in the lunate fossa and the capsule was sutured closed to secure the Tekscan sensor in place.
Following the PRC, the wrists were again mounted onto the Instron device, and loaded with 200 N of force for 60 seconds. The mean and peak contact pressures (N/cm2) and contact areas (cm2) across the joint were collected using the Tekscan pressure sensing system at the lunate fossa and saved using the K-scan software. The I-scan software was used to analyze the measurements, which were then tabulated in Microsoft Excel (Microsoft, Redmond, Washington).
Statistical Analysis
Descriptive analysis was performed in Microsoft Excel and statistical analysis was performed using STATA (v13, STATACorp, College Station, Texas). Normality of the pressure data was evaluated with a Shapiro-Wilk test, which demonstrated the presence of nonnormally distributed data (P < .05) and thus a nonparametric paired analysis was employed. Due to presence of nonnormally distributed data, the results of the contact pressures are presented as both means and medians. A Wilcoxon-signed rank test was used to compare the pressure data for the intact and PRC states at the lunate fossa. The data for distances between peak pressures were normally distributed and were thus evaluated using a paired t-test. Significance was set at P < .05.
Results
A total of 10 nonpaired wrists were included in final analysis (mean specimen age = 74.50 ± 13.27, 4 males/6 females). In all specimens, the radiocarpal joint was grossly inspected. No specimens had any gross evidence of prior trauma or arthritis.
Mean Contact Pressure
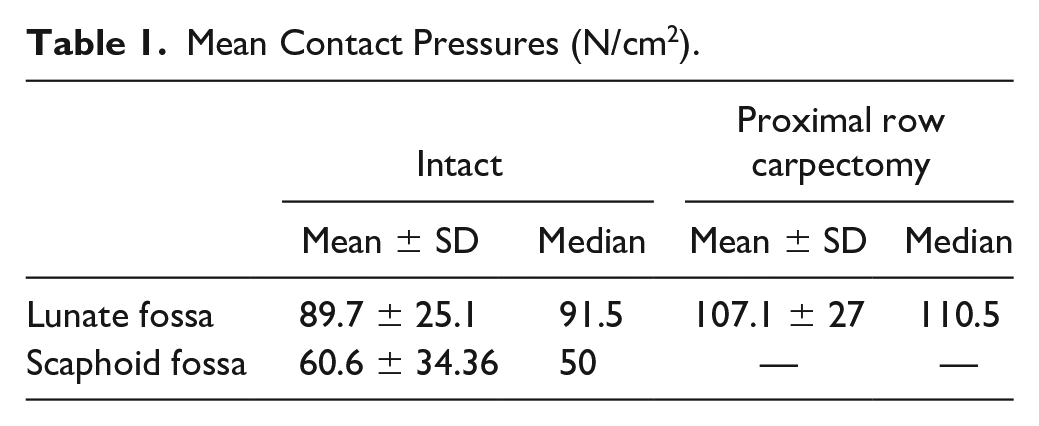
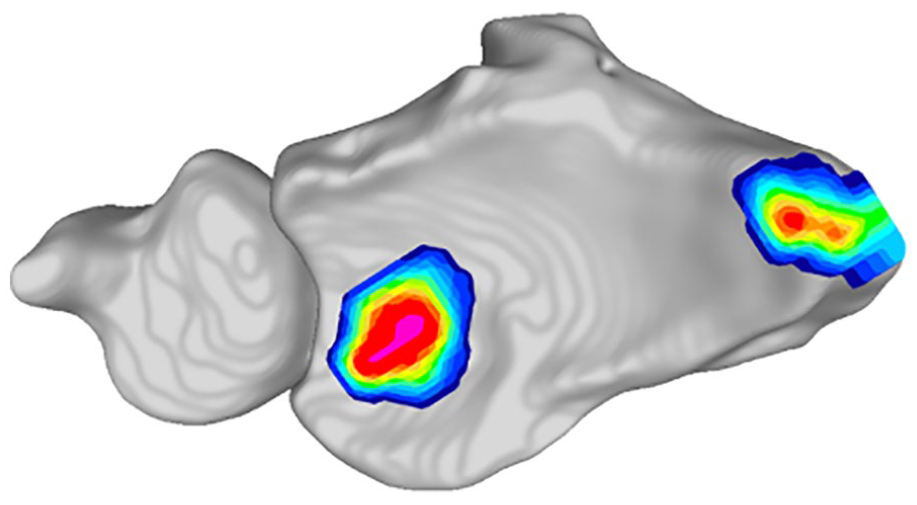
Mean contact pressures at the lunate fossa in the intact and PRC states are demonstrated in Table 1. Performing a PRC did not significantly increase the mean contact pressure compared to the intact group (mean increase of 17.4 ± 43.2 N/cm2, P = .184). Figure 2 demonstrates a representative overlay of the contact pressures on a 3D reconstructed computed tomography (CT) scan.
Mean Contact Pressures (N/cm2).
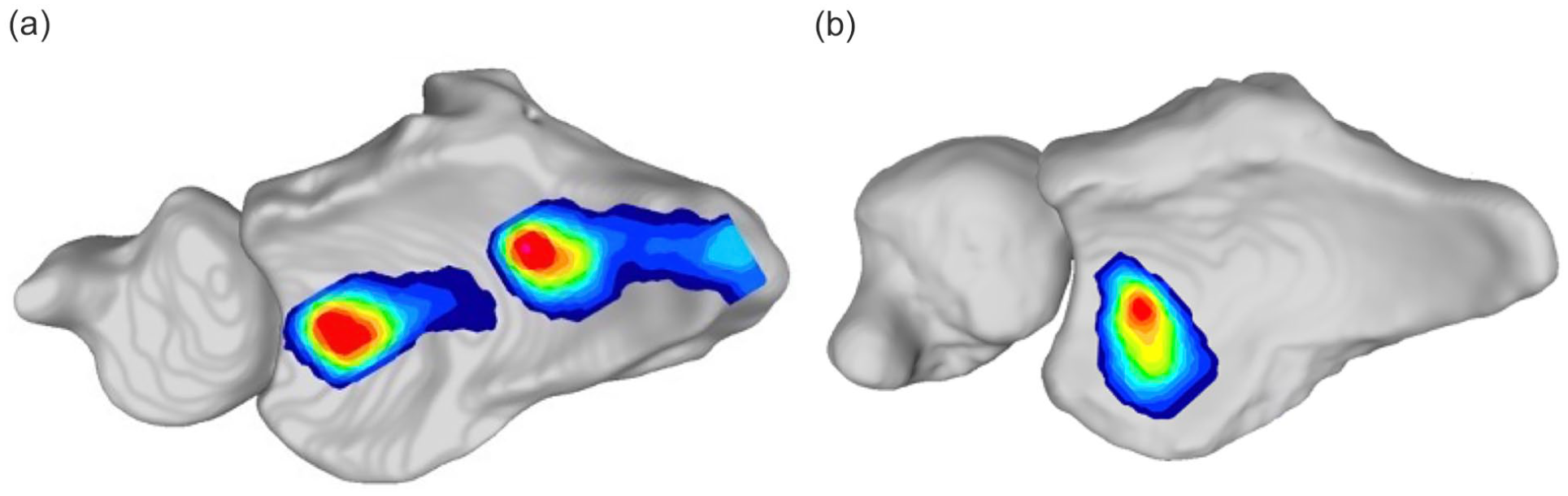
Representative Tekscan contact pressure map overlayed onto the associated specimen’s 3D reconstructed computed tomography, demonstrating the contact pressure in (a) the native state in the scaphoid and lunate fossa and (b) in the lunate fossa after proximal row carpectomy.
Peak Contact Pressure
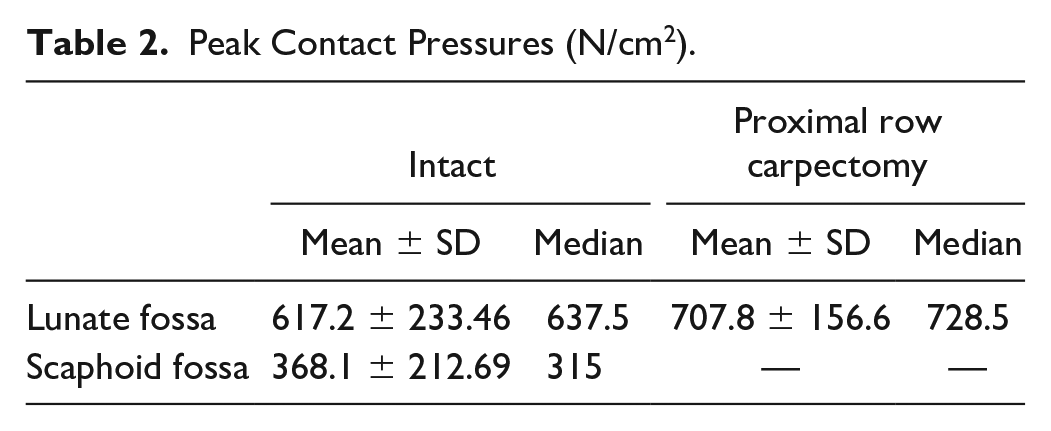
Peak contact pressures at the lunate fossa and scaphoid fossa are displayed in Table 2. There were no significant differences in peak contact pressure after PRC (intact: 617.2 ± 233.46 N/cm2, PRC: 707.8 ± 156.6 N/cm2, P = .169).
Peak Contact Pressures (N/cm2).
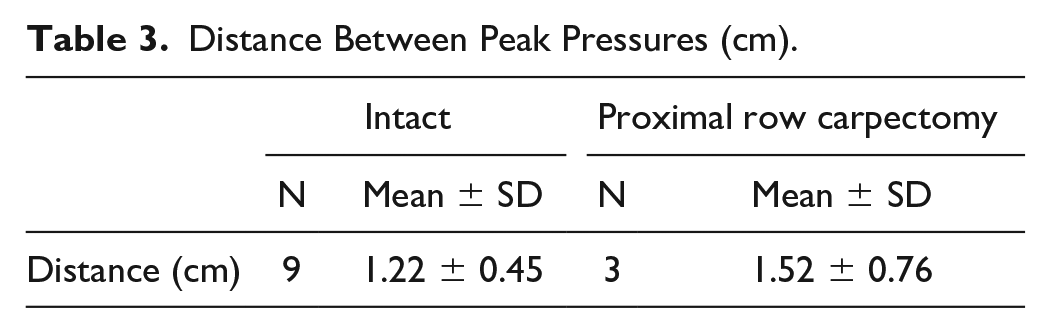
In the intact group, 9 wrists demonstrated 2 main areas of peak pressure in the lunate fossa and scaphoid fossa (mean of 1.22 ± 0.45 cm between peaks) with the remaining specimen only containing 1 pressure peak in the lunate fossa (Table 3). In the PRC group, 3 wrists demonstrated dual pressure peaks (between the lunate fossa and radial styloid) with a mean distance between peaks of 1.52 ± 0.76 cm (Figure 3). The mean peak pressure of the radial styloid in this subgroup was 328 ± 173.76 N/cm2 and was an average of 49% of the lunate fossa peak pressure. The remaining PRC specimen (n = 7) demonstrated a sole peak in the lunate fossa.
Distance Between Peak Pressures (cm).
Tekscan contact pressure map of a specimen after proximal row carpectomy with a contact pressure peak in the lunate fossa and radial styloid.
Contact Pressure Area
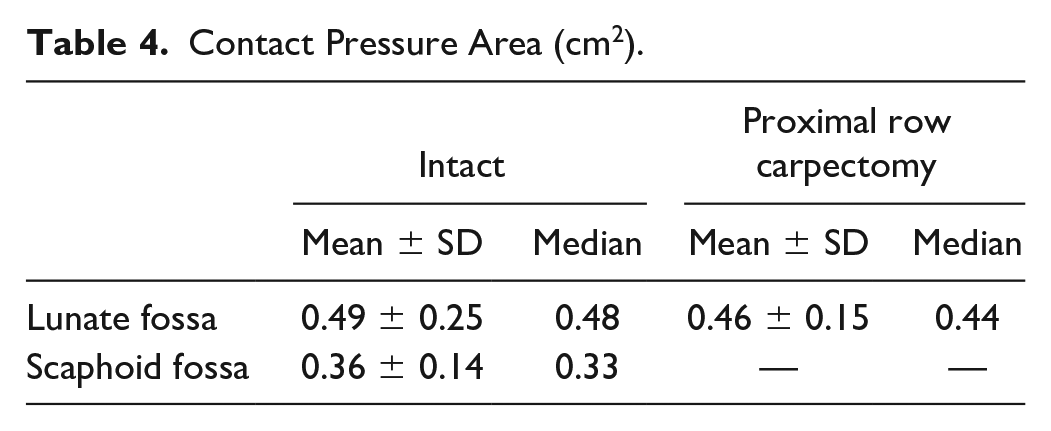
Mean contact areas for each group at the lunate and scaphoid fossa are shown in Table 4. At the lunate fossa, the intact state had a contact area of 0.49 ± 0.25 cm2. Similarly, after a PRC the contact area was 0.46 ± 0.15 cm2. No significant differences between the intact and PRC groups (P = .681) were observed.
Contact Pressure Area (cm2).
Discussion
The main finding of this study was that there were no significant differences in mean contact pressure, peak contact pressure, or contact area in the lunate fossa after PRC. These results vary compared to prior literature that suggests that a PRC significantly increases mean contact pressure while decreasing contact area. For example, Zhu et al 3 reported that the mean contact pressure in the lunate fossa with the wrist in a neutral position increased from 23.2 ± 3.2 to 136.4 ± 30.7 N/cm2 after a PRC with the contact area decreasing from 2.08 to 0.30 cm2. This study, however, is not directly comparable to ours due to methodologic differences; specifically, their study utilized a 100 N axial load instead of our 200 N load, which may explain why their intact contact pressure was much lower (approximately 20%) than ours. Similarly, Hogan et al 8 reported a decrease in contact area by 37% after PRC (from 4.5 ± 0.013% to 6.1 ± 0.017% of the available radiocarpal contact area) and an increase in contact pressure from 41.3 ± 15.4 N/cm2 to 64.9 ± 23.5 N/cm2 using a total axial load of 134 N. Tang et al 9 used the same amount of axial load as this study (200 N), but the authors reported a mean contact pressure increase in the lunate fossa from 1.3 MPa in the intact state to 4.9 MPa after PRC and a contact area decrease from 63.3 to 33.5 mm2. This may be because this study also used a significantly different methodologic approach: the authors applied the 200 N load across the flexor and extensor tendons of the wrist (each individual tendon was loaded, except the extensor carpi radialis longus and brevis which were loaded together) instead of applying a direct axial load. The vectors of this indirect load, despite being of the same magnitude, may explain the differing results as compared to our study. We decided to use a clenched-fist position as this has been shown to stress the SL joint and stress to the SL joint generally underlies the pathology that necessitates a PRC.18,19 In addition, the clenched-fist position has been used in prior studies when comparing SL reconstructions to axially load the wrist. 20 We hypothesized that providing axial loading in the clenched-fist position would most closely replicate clinical stress in patients undergoing PRC. However, the most accurate testing approach and clinical value of these varying methodologies is unclear.
In addition, all of these aforementioned studies utilized FujiFilm as their pressure sensing method. This technology has been shown to have measurement errors up to 14% to 28%, raising concern about the validity of the results reported in the prior literature. 10 Furthermore, when directly comparing Tekscan and FujiFilm technologies, Tekscan has been shown to deliver greater accuracy while providing high sensitivity and real-time measurements. 21 Due to the use of FujiFilm and differing methodologic approaches, it is challenging to directly compare our results to those in the current literature. The results from our study, however, contradict the prior literature and suggest that a PRC does not significantly alter the contact pressure or contact area within the radiocarpal joint.
However, it is important to note that 3 specimens demonstrated a second contact pressure peak at the radial styloid after PRC that was approximately 50% of the peak pressure observed in the lunate fossa. A statistical comparison of the peak pressure at the radial styloid prior to and after PRC could not be performed due to the small sample size of PRC specimen that demonstrated this pattern and because the contact pressure observed at the radial styloid in the intact group was not significant enough to be considered a peak. Our qualitative results suggest that a PRC can increase the peak contact pressure at the radial styloid in some cases, which we hypothesize is due to impingement of the radial styloid against the trapezium. 22 This change in contact pressure may suggest a role for radial styloidectomy as an adjunct procedure to PRC in some individuals. However, further research is needed to understand what anatomical risk factors may increase the risk of a patient developing increased contact pressures at the radial styloid after a PRC.
Our negative findings suggest that contact pressure and area changes are unlikely solely responsible for the pathogenesis of degenerative changes in the lunate fossa after PRC and that other contributing factors must be considered. Altered kinematics and a differing radius of curvature (ROC) of the capitate compared to the lunate are biomechanical factors that have been suggested to play a role in the failure of PRC. A cadaveric study by Sobczak et al, 11 for example, reported on the alterations in the mean pivot point, which was defined as the point where the sum of the squared distances to the helical axes is minimal, after PRC. The authors reported that the mean pivot point shifted 6.8 to 9.1 mm proximally after PRC (P < .05), and that the moment arms of all wrist muscles decreased, except for the flexor carpi ulnaris (FCU) (P < .01). Similarly, a study by Nichols et al demonstrated how PRC alters wrist kinematics. The authors reported significant alterations in moment arms of 4 primary muscles (flexor carpi radialis, extensor carpi radialis brevis [ECRB], extensor carpi radlis longus, and extensor carpi ulnaris [ECU]), while the FCU was not affected. 23 Specifically, after PRC there was a bias toward flexion in extended wrist postures due to a decrease in the ECRB and ECU extension moment arms. Changes in the flexion-extension axis after PRC were also reported by Blankenhorn et al. 24 In a 3D CT-based model, the authors reported that while overall wrist motion decreased, motion at the radiocarpal joint during flexion and extension increased by 135% to 136% after PRC. In addition, the capitate altered its direction of motion within the radiocarpal joint, moving along the flexion-extension axis instead of the radioulnar axis during radioulnar wrist motion. These biomechanical studies support the notion that PRC significantly alters the kinematics of the radiocarpal joint, which may contribute to the development of degenerative changes after PRC.
In addition to affecting kinematics, significant differences in ROCs between the capitate and lunate ROCs may contribute to the pathogenesis of degenerative changes after PRC. Hawkins-Rivers et al, 25 for example, demonstrated that the proximal lunate has a significantly larger ROC than the proximal capitate. They reported that the ROC of the proximal capitate to proximal lunate was 0.366 to 0.811 on coronal projections and 0.46 to 0.71 on sagittal projections based on magnetic resonance imaging data. Radius of curvature congruency may also affect outcomes after PRC. A clinical study by Lenoir et al 26 reported that a better radiocapitate congruency, defined as the ROC of the tip of the capitate divided by the mean ROC of the lunate fossa, in the frontal plane (r = -0.572, P = .045) was significantly associated with higher functional Disabilities of the Arm, Shoulder, and Hand questionnaire outcomes. This study suggests that ROC may play an important role in outcomes after PRC. Future studies are needed to investigate whether ROC incongruency is directly associated with failure or conversion to arthrodesis in setting of symptomatic radiocapitate degenerative changes after PRC.
While we hypothesize that the evolution of degenerative changes after PRC is multifactorial and may involve changes in kinematics and ROC, the long-term development of degenerative changes and conversion rate to wrist arthrodesis after PRC remain relatively low. Recent studies have reported the failure rate, defined as conversion of PRC to arthrodesis, to be between 2.7% and 35%. 6 ,27-29 It is important to note, however, that there are a variety of indications for converting a patient to wrist arthrodesis, often unrelated to degenerative changes, such as decreased strength or pain. In addition, not all patients who develop radiographic degenerative changes are symptomatic nor require an arthrodesis.29-31 Furthermore, functional outcomes, patient-reported outcomes, and pain level after PRC may not be related to radiologic degeneration.28,32 Because of this, the role of degenerative changes in the conversion to wrist arthrodesis remains poorly defined. In addition to investigating the role of biomechanical changes in the development of degenerative changes, future studies are needed to clarify the relationship between degenerative changes and failure after PRC.
Limitations
This study should be interpreted within the context of its limitations. First, due to technical limitations we were unable to evaluate the movement of the contact pressure centroid and how this would be affected by performing a PRC. We also did not evaluate changes in contact pressure or area based on different wrist positions (eg, greater degrees of extension or flexion). Future studies are needed to investigate this point further. Interestingly, there was 1 specimen in the intact group that demonstrated a sole peak contact area in the lunate fossa. This specimen did demonstrate low signal in the scaphoid fossa that did not achieve the threshold of a second peak. The lack of a second peak may be due to differences in ulnar variance or scapho-radial osseous morphology compared to the other specimen, but there is always potential for human and technical errors during data acquisition, which could have occurred when inserting the Tekscan into the radiocarpal joint or when analyzing the Tekscan data. In addition, while an a priori power analysis was performed to determine the sample size number, these calculations were performed based on prior investigations that used FujiFilm. It is possible that this study may be underpowered to detect the pressure difference nuances that Tekscan is able to capture. Furthermore, as a biomechanics study utilizing cadaveric specimen, our study has inherent limitations; specifically, it is unclear how generalizable our findings are to the in vivo radiocarpal joint. Lastly, our figures depicting contact pressure and area were not performed with any computational transformations or manipulations. Thus, it is possible that there are slight inaccuracies in the location of the pressure maps compared to the true biomechanical finding. This is in part due to our inability to denote the edge pixels of the Tekscan and orient this landmark directly to the CT scan. This limitation should be considered when evaluating the included figures. However, despite these limitations, our study has interesting implications that contradict prior, similar investigations that utilized FujiFilm. Our results suggest that contact changes due to PRC may not be significant enough to directly contribute to the pathogenesis of radiocapitate osteoarthritis after PRC.
Despite being relatively well studied, the literature on the effect of PRC on contact pressures is heterogeneous and based on results acquired with older technology. The purpose of this study was to add upon existing literature by investigating the role of a PRC on contact pressure and contact area of the lunate fossa using Tekscan, the most current pressure sensing technology. Our study demonstrated no significant differences in any of these 3 tested outcomes (mean contact pressure, peak contact pressure, and contact area) between the intact and PRC groups. These findings suggest that alterations in contact pressures after PRC are unlikely to be the sole or main contributing factor in the pathogenesis of degenerative changes after PRC, which can result in the need for a wrist arthrodesis. Based on our negative findings, we hypothesize that alterations in joint kinematics and differing ROCs of the capitate versus the lunate may play a greater role in the development of degenerative changes after PRC than contact pressure changes. Future studies are needed to support this hypothesis and investigate these relationships directly.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained when necessary.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.K. is a committee member of the American Society for Surgery of the Hand (ASSH); a paid consultant and speaker for Integra LifeSciences, Inc; a paid consultant for Tissium, Inc.; a stockholder and member of the medical advisory board for Reactiv, Inc.; and a speaker for TriMed, Inc. No other authors have any disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.