
Abstract
Background:
It remains unclear whether exposure for planned fixation of distal radius fractrues is superior with any given approach, and whether a single utilitarian approach exists that permits reliable complete exposure of the volar distal radius.
Methods:
A cadaveric study was performed using 10 matched specimens. Group 1 consisted of 3 radially based approaches (standard flexor carpi radialis [FCR], standard FCR with radial retraction of FCR and flexor pollicis longus [FPL] tendons, extended FCR). Group 2 consisted of 2 ulnarly based approaches (volar ulnar, extended carpal tunnel). The primary outcome was total width of exposed distal radius at the watershed line. Mann-Whitney U and Wilcoxon rank testing was used to identify differences.
Results:
The standard FCR approach exposed 29 mm (90%), leaving on average 3 mm (10%) of the ulnar corner unexposed. Retracting the FCR and FPL tendons radially allows for an extra 1 mm of volar ulnar corner exposure. Finally, converting to an extended FCR approach provided 100% exposure in all specimens. The volar ulnar exposure however provided exposure to only 9 mm (37%), leaving 20 mm (62.5%) left unexposed radially. The extended carpal tunnel provided exposure to 21 mm (65%), leaving 11 mm (35%) radially unexposed. Differences between each group were statistically significant (P < .05).
Conclusions:
The extended FCR approach exposed 100% of the volar distal radius in our study and may serve as a utilitarian volar surgical approach for exposure and fixation of distal radius fractures. Additional knowledge of the limitations of alternative approaches can be helpful in surgical planning.
Introduction
Fractures of the distal radius are common upper extremity injuries, with estimated incidence of 643 000 per year. 1 With increasing advancements in implant technology, operative intervention is becoming more frequent. 2 As an improved appreciation of the importance of reduction and fixation of the intermediate column emerges, an accurate understanding of the relevant surgical anatomy is paramount. Although multiple approaches to the volar distal radius have been described, it remains unclear whether exposure for planned fixation is superior with any given approach and whether a single utilitarian approach exists that permits reliable complete exposure of the volar distal radius including both the radial and intermediate columns.
Two common volar approaches to the distal radius are frequently used: the volar ulnar approach and the standard flexor carpi radialis (FCR) approach. The volar ulnar approach is limited in its radial exposure even when extended distally in an extended carpal tunnel fashion. 3 The FCR approach can also be extended distally as described by Orbay et al. 4 In our experience, the volar ulnar corner fragments can occasionally be exposed by the standard FCR approach; however, in obese, muscular, or edematous patients, soft tissues may further limit adequate exposure for reduction and fixation of this critical corner. Extension of the standard FCR approach (eFCR) as described by Orbay et al 4 has been proposed to potentially improve exposure of the volar ulnar corner versus a standard FCR approach. Previous work in this area has suggested that an eFCR approach may allow easier access to the distal volar ulnar fracture fragment, although this was not studied directly. 5 As such, this may represent a utilitarian approach to allow reliable visualization of both the radial and the ulnar surface of the volar distal radius. If so, this may obviate the need for fragment-specific volar and radial surgical approaches, and may permit a more fluid decision-making process regarding fixation strategy intraoperatively.
The goal of this study was to determine the ability to expose the volar distal radius for open reduction and internal fixation using the FCR, eFCR, volar ulnar, and extended carpal tunnel approaches. We hypothesize that the eFCR approach will allow for adequate exposure of the entire volar distal radius at the watershed line including the volar ulnar corner and may obviate the need for a separate volar ulnar approach for more complex distal radius fractures.
Methods
A cadaveric study was performed using a total of 5 sets of matched mid-humerus to fingertip specimens (N = 10). This was based on an a priori sample size and power analysis to have a 0.80 power and 0.05 α to detect a 10% difference in surgical approach. The specimens were evenly randomized to either the FCR group or the volar ulnar group, totaling 5 per group. Cadaveric width and circumference at the wrist were recorded for each specimen. All approaches used an 8-cm longitudinal component of the incision from the proximal wrist crease as has been described previously in the literature. 6 The FCR group (n = 5) had 3 sequential exposures performed: standard FCR, 7 standard FCR with radial retraction of FCR and flexor pollicis longus (FPL) tendons, and finally the extended FCR (Figure 1). The volar ulnar group (n = 5) had 2 sequential exposures performed: the volar ulnar followed by the extended carpal tunnel (Figure 1).
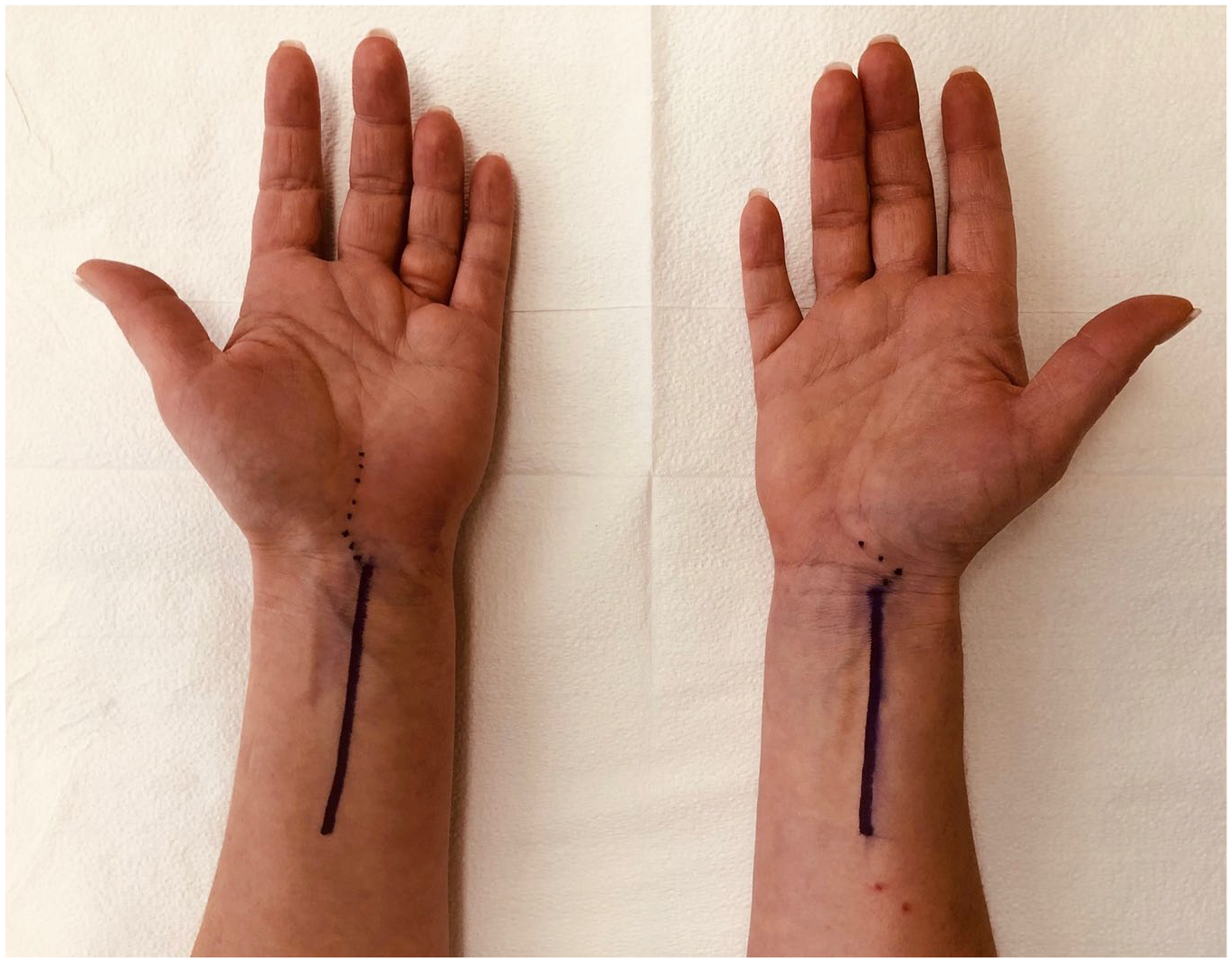
The volar ulnar (left) and flexor carpi radialis (FCR, right) approaches (solid lines) along with their respective distal extensions: the extended carpal tunnel approaches and extended FCR (dotted lines).
Within the FCR group, the standard FCR approach, a well-described modification of the volar approach of Henry, was initially performed. 7 Subsequently, the same FCR approach but with radial retraction of the FCR and FPL tendons was assessed prior to extending the exposure distally. This involved retracting the FCR and FPL tendons radially along with the radial artery rather than medially with the median nerve without enlarging the skin incision or increased soft tissue dissection. At our institution, this has been anecdotally found to allow for a marginal amount of increased ulnar exposure. Finally, the exposure was extended to complete the eFCR approach as previously described by Orbay et al. 4 Measurements as described below were obtained after each of the 3 sequential exposures.
The standard FCR approach begins with palpation of the FCR tendon prior to making your skin incision. The planned incision should run longitudinally along the radial aspect of the tendon. Our approach consisted of an 8 cm incision in length (Figure 1). The dissection is carried down through skin and subcutaneous tissue until the tendon sheath of the FCR tendon is visualized. The sheath is opened and the tendon is retracted ulnarly. The incision is then deepened between the FPL and the radial artery. It is important to be cautious and avoid damaging the radial artery on the radial side and the superficial palmar cutaneous branch of the median nerve on the ulnar side. The surgeon can then use their finger to bluntly dissect the interval between FPL and the radial artery to expose the pronator quadratus muscle on the volar aspect of the radius. The pronator quadratus is then elevated by creating an L-shaped incision that runs horizontally along the most distal aspect of the muscle and longitudinally along the most radial aspect of the muscle. Retraction of the incised edges of the pronator quadratus then reveals the volar aspect of the distal radius.
This approach can be extended as described by Orbay et al. This is done by releasing the radial septum, subperiosteal release of the proximal radial fragment, and mobilization of that fragment into pronation.
The volar ulnar exposure 3 was performed on the remaining 5 matched cadaveric specimens. At first, the exposure was stopped at the proximal wrist crease, where initial measurements were obtained (Figure 1). Second, the incision was extended distally performing an associated carpal tunnel release, and measurements were repeated to determine whether this would assist with further radial exposure. 3 All approaches used an 8-cm longitudinal component of the incision from the proximal wrist crease for standardization (Figure 1).
The volar ulnar approach uses the plane between the flexor carpi ulnaris and the tendons of the flexor digitorum. The incision starts at the wrist crease and runs proximally in line with the radial border of the ulna. The incision is carried down through skin, subcutaneous tissue, and fascia to find the interval between the flexor carpi ulnaris and underlying ulnar neurovascular bundle ulnarly and the flexor tendons radially. The flexor tendons and the median nerve are retracted radially, which provides exposure to the underlying pronator quadratus. The pronator quadratus is incised and elevated to reveal the ulnar aspect of the distal radius. This approach can be extended distally by continuing the incision obliquely toward the radial aspect of the hand, crossing the carpal tunnel.
The primary outcome was the total width of distal radius exposed at the watershed line. We defined the watershed line as described by Orbay et al 4 as the anatomical line between volar radial tubercle and the volar rim of the lunate fossa and the point at which the flexor tendons are naturally in contact with bone.
After exposure was completed, a Kirschner wire (K-wire) was driven into the most ulnar and radial aspects of the exposed radius. The K-wire was driven perpendicular to the volar rim to simulate the ulnar or radial-most extent of visualized bone that was exposed adequately enough to permit successful hardware placement and as a proxy for adequate exposure for successful fragment reduction. A digital caliper was then used to measure the width of the exposed distal radius at the watershed line, defined as the width of exposed volar rim of the radius from the K-wire ulnarly to the radial-most exposed radius or vice versa (Figure 2). Finally, a simulated intraoperative binary distinction was made to determine whether each approach provided adequate visualization of the volar ulnar corner based on K-wire placement and width of radius exposed.
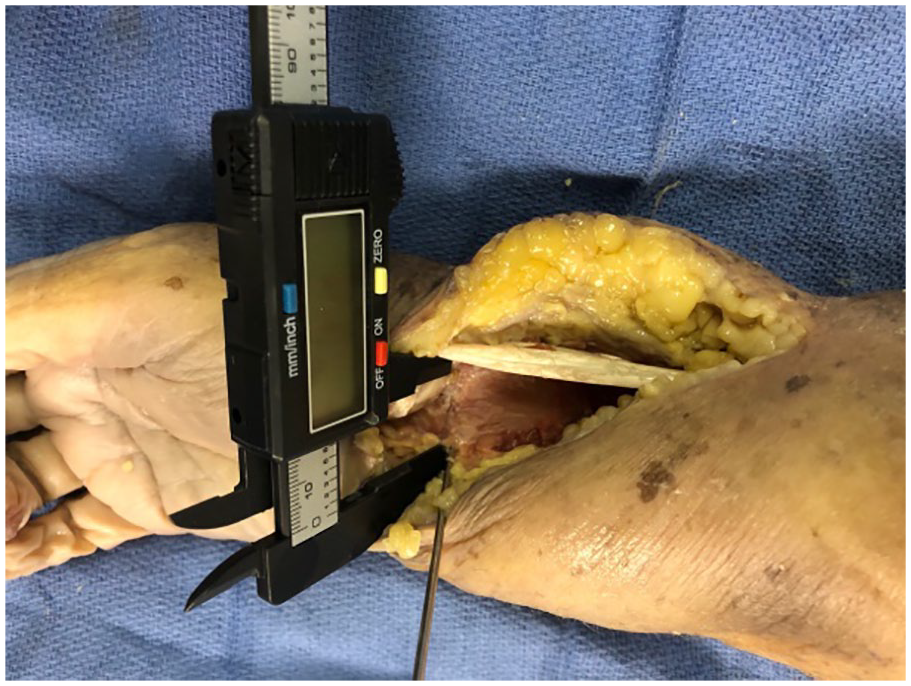
Width of volar distal radius measured at the watershed line with a digital caliper.
After each subsequent exposure and K-wire placement, digital pictures were taken of the exposed volar radius with a smart phone camera (iPhone X; Apple, Cupertino, California). Image J software (National Institute of Health) was then used to calculate the area of exposed distal radius as a secondary outcome measure. The digital pictures of each exposure stage were imported into the software system and the surface area of exposed distal radius was calculated (Figure 3). Using the known measurement of width exposed radius, we were able to calibrate the software to the number of pixels in the given length. This has previously been described for exposures of the proximal humerus. 11 The average total area exposed was then used as the denominator to calculate the percentage of area exposed for each approach.
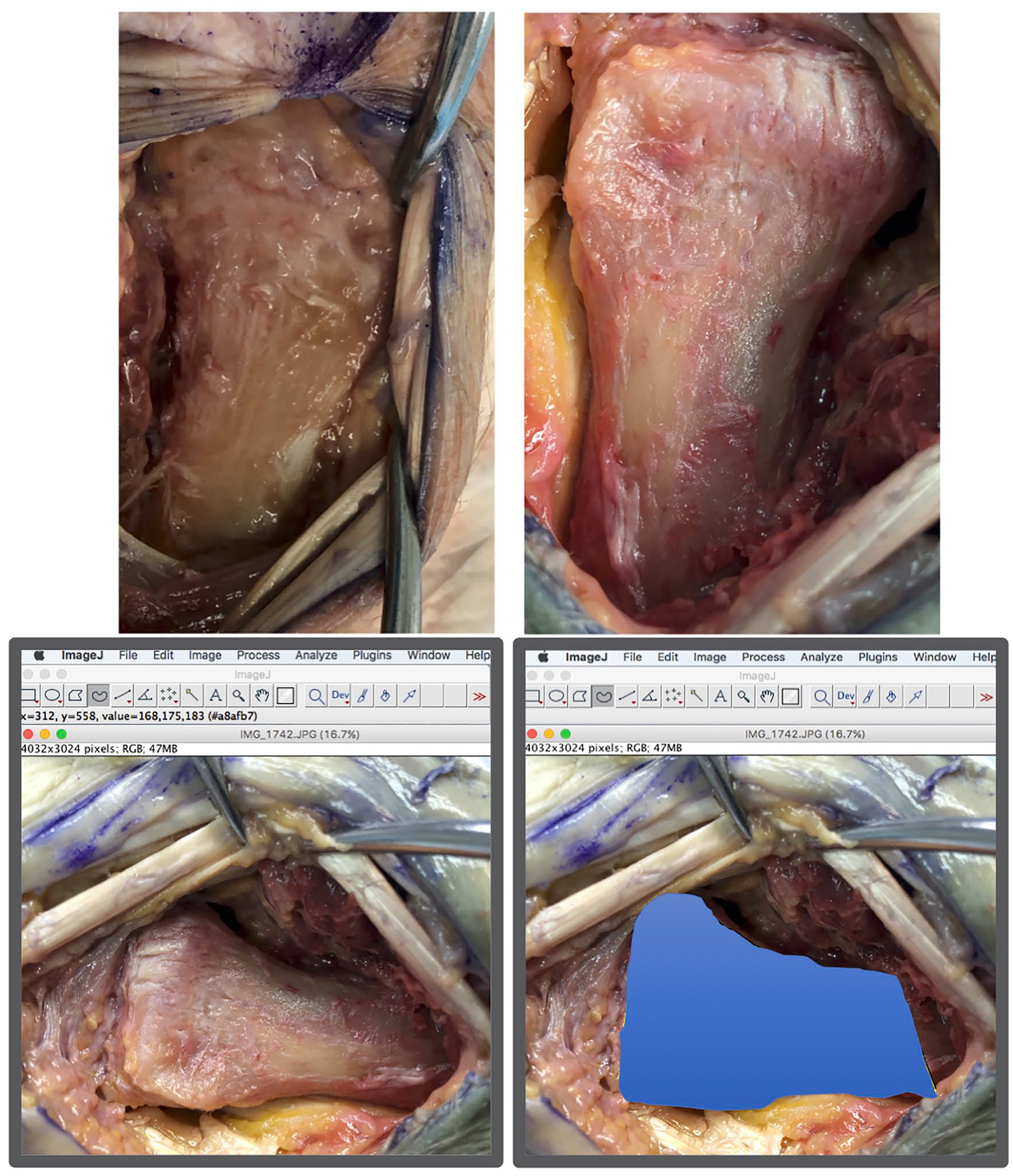
Measurement of the surface area of volar distal radius exposed using Image J software. The top left image depicts the area exposed with flexor carpi radialis (FCR) radial retraction, whereas the top right image depicts exposure with the extended FCR approach. The bottom two images demonstrate measurement of surface area using the image J software.
Finally, a binary analysis was performed to combine the first 2 calculations and simply classify whether the volar ulnar corner was exposed adequately. Mann-Whitney U and Wilcoxon rank testing was used to identify differences in the exposed portion of the distal radius between the multiple exposures.
Results
Raw data can be found in Supplemental Tables 1 and 2. Demographic information for the specimens can be found in Table 1. The mean circumference in both groups of cadaveric specimens at the distal wrist crease was 16.4 cm (range, 14.9-18.1 cm). The mean width of the cadaveric specimens at the distal wrist crease with inclusion of the soft tissue envelope was 6.3 cm (range, 5.4-6.8 cm). The mean width of the bony distal radius in the cadaveric specimens was 32.6 mm (SD = 2.9 mm), and the mean total area was 1393.5 mm2 (SD = 197.9 mm2) after complete exposure to a point 8 cm proximal to the wrist crease.
Specimen Demographic Information.
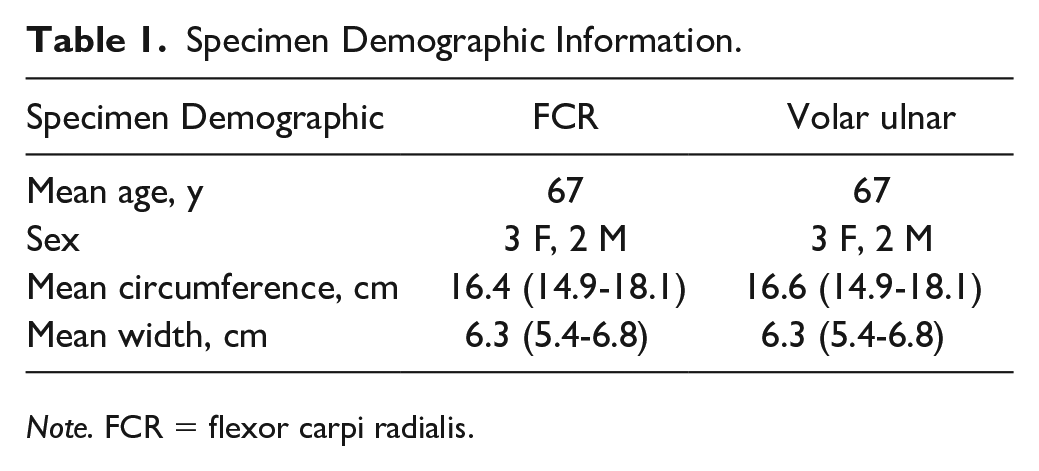
Note. FCR = flexor carpi radialis.
The standard FCR approach exposed 29 mm (SD = 3 mm) of the width of the distal radius at the watershed line, leaving on average 3 mm (10%) of the volar ulnar corner left unexposed (Figure 4). This corresponded to a mean total area of exposure with the standard FCR approach of 82% (1135 mm2, SD = 159.9 mm2) (Figure 5). Two of the 5 specimens were found to have adequate volar ulnar corner exposure despite leaving some measurable radius unexposed (Table 2).
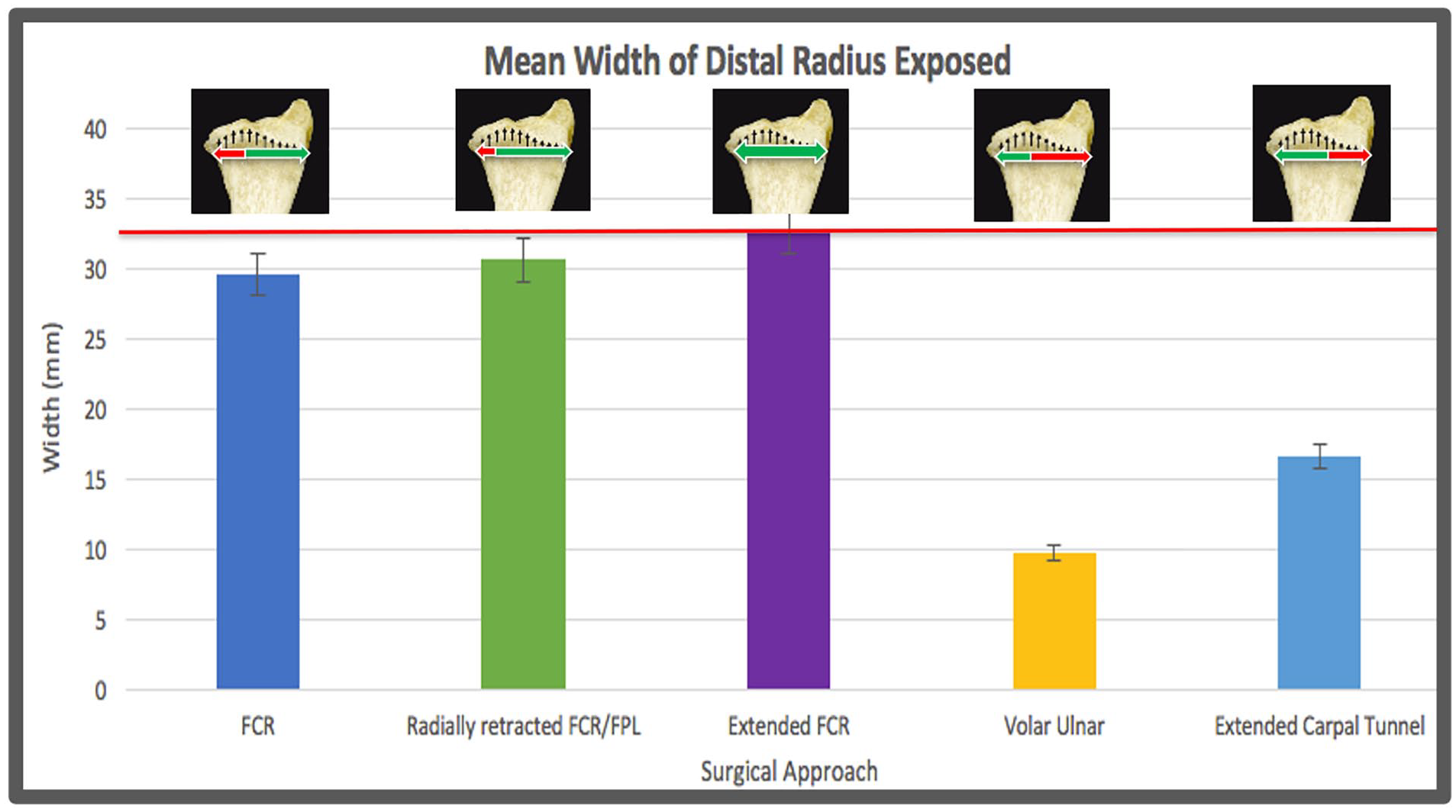
Mean width of volar distal radius exposed at the watershed line.
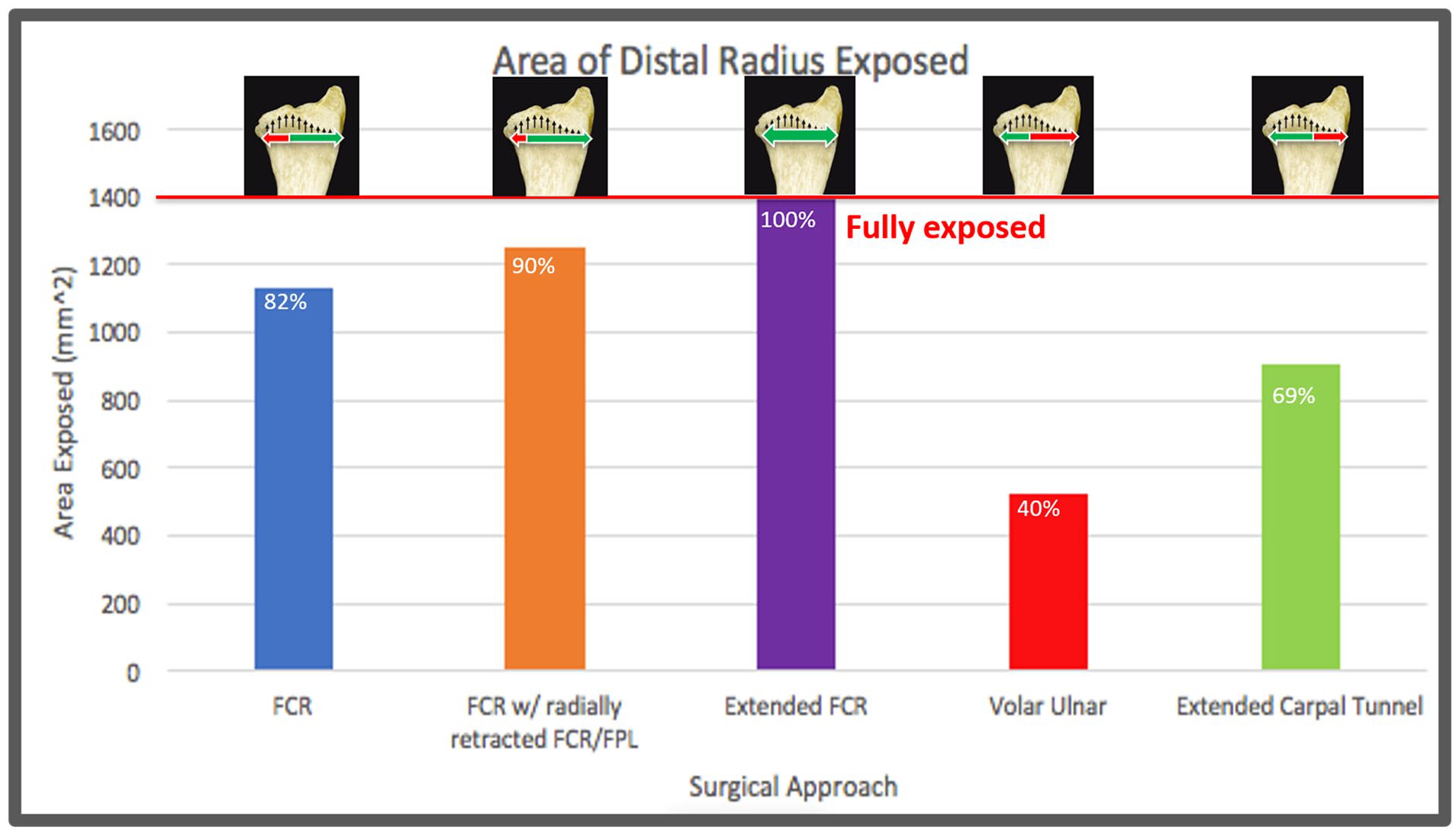
Mean surface area of distal radius exposed.
Adequate Exposure of Volar Ulnar Corner by Approach.
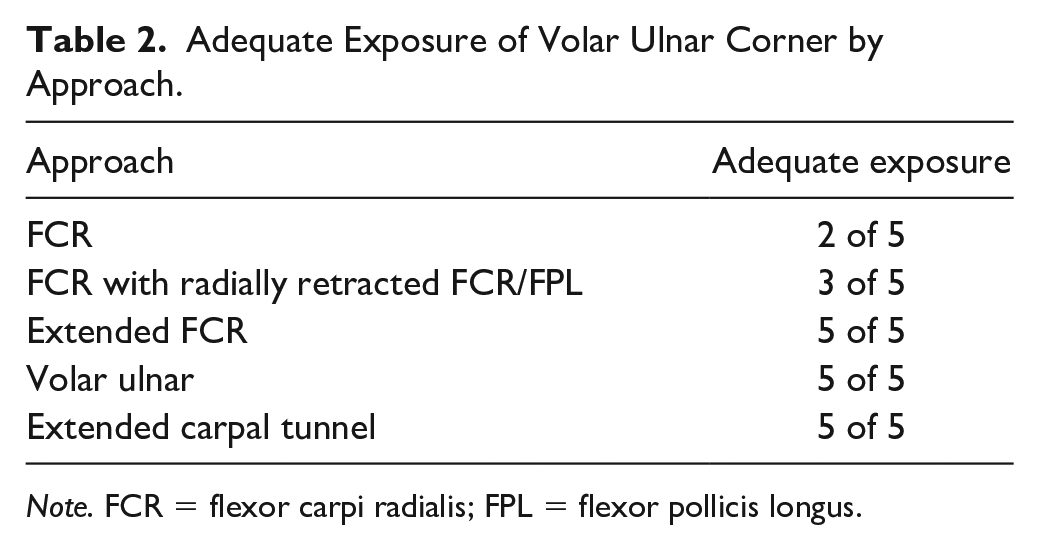
Note. FCR = flexor carpi radialis; FPL = flexor pollicis longus.
Retracting the FCR and FPL tendons radially allowed exposure of an average of 30.6 mm (SD = 3.4 mm) of the width of the distal radius at the watershed line. This extra 1.6 mm of volar ulnar corner exposure left on average 6% of the volar ulnar radius unexposed. The mean total area exposed was 90% (1253 mm2, SD = 199.6 mm2) (Figures 3 and 4). Three of the 5 specimens were found to have adequate volar ulnar corner exposure despite leaving some measurable radius unexposed (Table 2).
Converting to an extended FCR approach provided 100% exposure of the width and surface area of the distal radius in all cadaveric specimens (Figures 4 and 5). All 5 specimens had adequate volar ulnar corner exposure.
The volar ulnar exposure without distal carpal tunnel release provided exposure to only 9.7 mm (SD = 1.6 mm) or 33% of the distal radial width leaving 20 mm left unexposed radially, and provided exposure to only 522.8 mm2 (SD = 116.95 mm2) or 40% of the total area (Figures 4 and 5). Extension to the extended carpal tunnel approach provided exposure to 63% of the width distal radius, 16.6 mm (SD = 2.9 mm), leaving 11.8 mm left unexposed radially. The mean area exposed was 69% (905.8 mm2, SD = 126 mm2) (Figures 4 and 5). The volar ulnar corner was exposed in its entirety with both of these approaches (Figure 3).
When comparing the results of the Mann-Whitney U and Wilcoxon rank sum test, the width and area exposed were significantly greater for the FCR approach than the volar ulnar approach (P < .05). Retraction of the FCR and FPL tendons after an FCR approach provided a statistically significant improved exposure (P < .05) when compared with the aforementioned standard FCR approach, given the improved exposure of the volar ulnar corner. Similarly, the extended FCR approach provided a significantly greater exposure of the volar distal radius, exposing 100% of the volar radial surface (P < .05), when compared with both ulnar approaches and both FCR approaches.
Discussion
Jockel et al 9 previously evaluated approaches to the volar forearm and identified the proximal and distal limitations of each exposure. Our analysis builds on these results with the addition of the eFCR approach, the possible utilitarian approach to the volar distal radius. Our results differed in that the volar ulnar corner was exposed consistently with their standard FCR approach. As a cadaveric study, soft tissue mobility and tension is certainly a confounding variable. We attempted to control for this by not only obtaining paired specimens of varied muscularity and adiposity as reflected in our demographic data, but also by using mid-humeral specimens to preserve the origins of forearm soft tissue structures. However, we were unable to perform a direct comparison with the study by Jockel et al as they did not publish data on the size of their specimens nor did they report the specimen level. Similar to our findings, the authors concluded that the volar ulnar approach provided less access to the radial styloid. In addition, their study, however, did not include an evaluation of the eFCR approach. 9 In our current study, we found that the standard FCR approach provided insufficient exposure of the volar ulnar corner in most circumstances; however, with a conversion to an extended FCR approach, complete exposure and simulated instrumentation of the entire width of the volar distal radius at the watershed line were achieved. In addition to improved exposure, the extended FCR approaches confer a number of additional advantages described in the literature such as access to the radial styloid for plating, access to the dorsal cortex 4 for fracture mobilization, and carpal tunnel release. 6 Given these attributes, the extended FCR approach has demonstrated additional utility for intra-articular fractures, subacute fractures, and malunions. 8
A utilitarian volar approach that would allow for identification, appropriate reduction, and fluid intraoperative decision-making regarding fixation of all fracture fragments including the volar ulnar corner would be of great interest, especially in circumstances where surgical intervention is undertaken without a preoperative computed tomography (CT) scan, where fracture fragmentation may be better appreciated intraoperatively. In our experience, extension of the standard FCR approach according to Orbay et al has allowed for successful visualization and access to the entire volar distal radius including the volar ulnar corner. This added exposure has proven especially helpful in cases when a preoperative CT scan was not available and a volar ulnar corner fragment was recognized intraoperatively necessitating improved ulnar exposure, and in cases in patients with enlarged body habitus or substantial traumatic edema. This anecdotal evidence is supported by the findings of our study. Although a fragment-specific approach could be employed initially to access the volar ulnar radius, based on the findings of our study and our clinical experience, this would limit radial exposure and potential fixation options. In addition, the results of our study demonstrate the deficiency of the standard FCR approach at exposing the volar ulnar radius. Although this was improved by retracting the FCR and FPL radially, the added exposure was marginal. However, our study found that the eFCR approach exposed the entirety of the volar distal radius, permitting adequate exposure for fixation of the volar ulnar corner, while maintaining exposure to the radial column.
Given the findings of our study, unless a fragment-specific approach and fixation is definitively planned based on preoperative imaging of the fracture pattern, the authors recommend starting with a standard FCR approach. If more ulnar visualization is needed, radially retracting the FCR and FPL along with the radial artery may be attempted. If this does not provide the necessary visualization, it is reasonable to extend the exposure distally in an extended FCR fashion and expect significantly improved access to the volar ulnar corner. Moreover, based on the results of our study, we believe the eFCR approach may be used as a utilitarian approach to the volar distal radius, which would minimize commitment to a fixation strategy at the onset of the surgical intervention.
Limitations of this study include its small sample size and cadaveric nature. In an attempt to preserve innate soft tissue tensioning of the specimens, we used cadavers from the mid-humerus down. Although this does not account for muscle tension, the testing conditions of our model would more closely match intraoperative conditions under a preoperative brachial plexus block. Though minimal, the risks associated with extending the standard FCR approach include injury to the superficial palmar branch of the radial artery, and the terminal lateral antebrachial cutaneous, radial sensory, and palmar cutaneous nerve branches. Although we use the extended exposure when visualization of the volar ulnar radius is limited, we believe that it can be more routinely employed as it would presumably provide more reliable visualization for facilitation of hardware placement and reduction with minimal added risk. Our model also does not account for the variability in edema seen in this patient population at the time of surgery, but it should account for the variability in soft tissue size due to muscularity and obesity. Considerable variability exists in the morphometry of the volar distal radius, with sex and race as contributing factors. 10 As such, it is possible that our sample did not proportionately represent all morphologic possibilities. In addition, the assumption that we were able to visually identify the watershed line was made; however, there may have been some subtle variation from specimen to specimen, which could affect the location of width measurements. We believe a perpendicular K-wire is an appropriate proxy for adequate exposure for fixation, but there may be case-specific variations which may require more exposure for adequate reduction and fixation. Last, our study did not have a control for the extra incision length of the extended FCR. The extended FCR approach was performed on the same cadaver limbs as the standard approach. This was done to limit cost.
Improved knowledge of the anatomy and the limitations of each exposure to the volar distal radius may facilitate surgical planning and intraoperative exposure of key fracture fragments. Given that these are already challenging fractures, optimal visualization is critical for both accurate reduction and adequate fixation. Identifying a potentially utilitarian surgical exposure may obviate the need to commit to a fixation strategy based on the chosen initial surgical approach. Ideally, if we are able to visualize the volar radial and intermediate columns with an extension of the standard FCR approach as the findings of this study suggest, this may diminish the need for a fragment-specific surgical approach to the volar distal radius.
Supplemental Material
sj-pdf-1-han-10.1177_15589447221094320 – Supplemental material for A Cadaveric Comparison of Approaches for Exposure of the Volar Distal Radius: Is There a Utilitarian Approach?
Supplemental material, sj-pdf-1-han-10.1177_15589447221094320 for A Cadaveric Comparison of Approaches for Exposure of the Volar Distal Radius: Is There a Utilitarian Approach? by William J. Warrender, Daniel J. Wagner, Reed W. Hoyer, Gregory A. Merrell, William B. Kleinman and Brandon S. Smetana in HAND
Supplemental Material
sj-pdf-2-han-10.1177_15589447221094320 – Supplemental material for A Cadaveric Comparison of Approaches for Exposure of the Volar Distal Radius: Is There a Utilitarian Approach?
Supplemental material, sj-pdf-2-han-10.1177_15589447221094320 for A Cadaveric Comparison of Approaches for Exposure of the Volar Distal Radius: Is There a Utilitarian Approach? by William J. Warrender, Daniel J. Wagner, Reed W. Hoyer, Gregory A. Merrell, William B. Kleinman and Brandon S. Smetana in HAND
Footnotes
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This was a cadaveric study and therefore no patients were actively enrolled; informed consent was not required for study completion.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Specimens and research equipment were paid for in full by a grant from the Ascension St. Vincent Hand Research and Education Endowment Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.