
Abstract
Background:
The purpose of this study was to evaluate the influence of socioeconomic factors on access to congenital hand surgery care, hospital admission charges, and analyze these geographic trends across regions of the country.
Methods:
Retrospective cohort study was conducted of congenital hand surgery performed in the United States from 2010 through 2020 using the Pediatric Health Information System. Multivariate regression was used to analyze the impact of socioeconomic factors.
Results:
During the study interval, 5531 pediatric patients underwent corrective surgery for congenital hand differences, including syndactyly repair (n = 2439), polydactyly repair (n = 2826), and pollicization (n = 266). Patients underwent surgery at significantly earlier age when treated at above-median case volume hospitals (P < .001). Patients with above-median income (P < .001), non-white race (P < .001), commercial insurance (P < .001), living in an urban community (P < .001), and not living in an underserved area (P < .001) were more likely to be treated at high-volume hospitals. Nearly half of patients chose to seek care at a distant hospital rather than the one locally available (49.5%, n = 1172). Of those choosing a distant hospital, most patients chose a higher-volume facility (80.9%, n = 948 of 1172). On multivariate regression, white patients were significantly more likely to choose a more distant, higher-volume hospital (P < .001).
Conclusions:
Socioeconomic and geographic factors significantly contribute to disparate access to congenital hand surgery across the country. Patients with higher socioeconomic status are more likely to be treated at high-volume hospitals. Treatment at hospitals with higher case volume is associated with earlier age at surgery and decreased hospital admission charges.
Keywords
Introduction
Socioeconomic and demographic determinants of health have been demonstrated to influence surgical outcomes.1-17 Racial disparities in pediatric plastic surgery have been suggested to result in older age at consultation, as well as influence complication rates, lengths of stay, and hospital costs.3,5,6,18-20 Hospital length of stays after orthognathic surgery have been shown to be significantly longer in black and hispanic patients. 3 Admission costs for orthognathic surgery have been shown to be significantly higher for black, hispanic, and asian patients compared to white patients. 3 Emergent admissions and lengths of stay after cleft palate surgery have also been shown to be significantly higher in black patients. 5 Admission costs for cleft palate surgery have been shown to be significantly higher for black and hispanic patients, and black patients had more postoperative complications, including higher rates of postoperative fistula formation. 5 Inequalities in hand surgeon distribution across geographic regions of the country have been well-documented, 21 but it remains unclear whether socioeconomic factors affect access to surgical care for congenital hand differences.
Understanding the risks and resources in patient environments and how they interact with innate and acquired biologic factors to affect healthcare outcomes remains complex and multi-dimensional, but appreciating socioeconomic indicators influencing surgical care is the foundation for optimizing outcomes in marginalized and vulnerable populations. 4 We hypothesized that patients from families with greater socioeconomic advantage would have better access to high-volume centers, even if distantly located from their homes. The purpose of this study was to utilize a multicenter dataset to elucidate the influence of socioeconomic factors on access to pediatric congenital hand surgery, treatment at high-volume centers, and hospital admission charges. The secondary objective of this study was to analyze these trends across geographic regions of the country.
Methods
A retrospective cohort study was conducted of congenital hand surgery procedures performed in the United States from 2010 through 2020 using the Pediatric Health Information System (PHIS). This is an administrative database that contains encounter-level data from over 50 nonprofit tertiary pediatric hospitals in the United States. Data quality and reliability are assured through a joint effort between the Children’s Hospital Association and participating hospitals. Data are subjected to several reliability and validity checks before inclusion in the database. Data are deidentified at the time of data entry, and institutional review board approval was not required.
Syndactyly repair was defined by CPT procedure codes 26560, 26561, and 26562. Polydactyly repair was defined by CPT procedure code 26587. Pollicization was defined by CPT procedure code 26550. Additionally, patients were concurrently required to meet respective ICD-9 and ICD-10 codes corresponding to these diagnoses [Supplemental Table 1]. In order to control for elective procedures, patients undergoing procedures with emergency department charges, or procedures scheduled as urgent, emergent, or trauma were excluded.
Hospital case volume was defined as total congenital hand surgery procedures performed during the 10-year study period. High-volume was defined by the 80th percentile, 22 and highest-volume was defined by the 90th percentile.23,24
Billed charges represented the amount patients were billed for the entire hospital admission. All financial data was adjusted by the CMS wage/price index for the hospital’s location. Additionally, all financial data was adjusted for inflation to be represented in 2020 US Dollars. Charge-to-cost ratio represents the hospital markup and was defined as billed charges divided by costs incurred by the hospital. Median household income was based on the postal code of each patient’s home address. Urban was defined as cities or surrounding suburbs. Underserved areas were based on counties meeting the standard for Health Professional Shortage Areas, defined as population to primary care physician ratio exceeding 3500:1.25,26
Mann-Whitney U test and Kruskal-Wallis test were used to compare continuous nonparametric variables between independent groups. Pearson’s chi-square test was used to compare categorical variables. Linear multivariate regressions were represented by the beta coefficient of each variable. Binary multivariate regressions were represented by the adjusted odds ratio of each variable. Central tendency was reported using median and its corresponding confidence interval. P values were all 2-tailed, and significance was set at the α < 0.05 level. Statistical analysis was conducted on SPSS v28 (IBM Corporation; Armonk, New York), Prism v9 (GraphPad; San Diego, California), and Tableau v2020.4 (NorthEdge; Seattle, Washington).
Results
During the study interval, 5531 patients underwent corrective surgery for congenital hand differences, including syndactyly repair (44.1%, n = 2439), polydactyly repair (51.1%, n = 2826), and pollicization (4.8%, n = 266) [Table 1]. Most patients were white (52.8%, n = 2920) and lived in an urban area (84.6%, n = 4679). Up to 6.6% (n = 364) patients came from underserved areas. Median household income was $43385 (95% CI: $42857-43822), and most patients had government insurance (56.3%, n = 3116).
Patient Demographics.
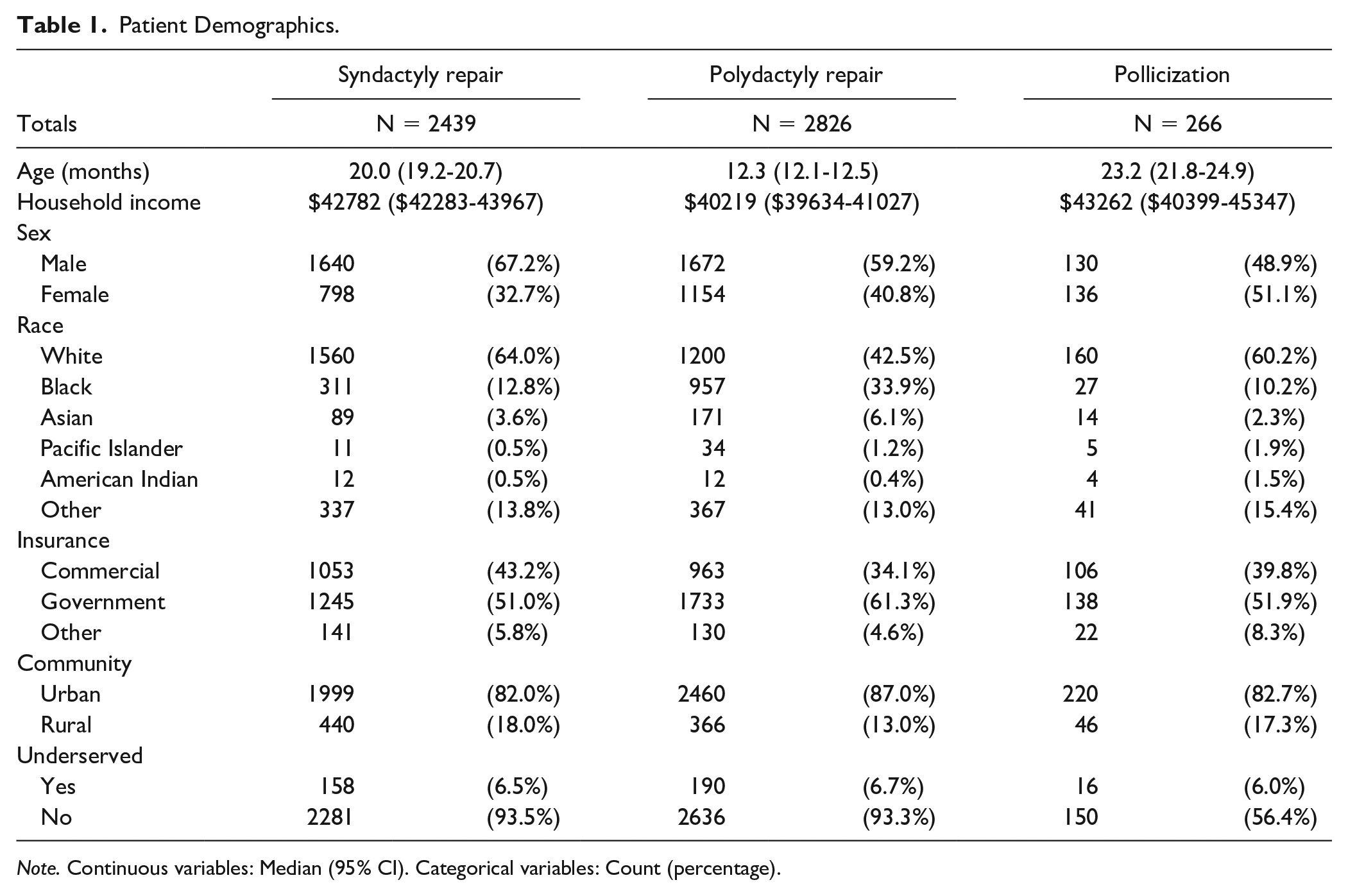
Note. Continuous variables: Median (95% CI). Categorical variables: Count (percentage).
Hospital Case Volume
Median hospital congenital hand surgery case volume was 149 (95% CI: 149-157) procedures during the 10-year study interval, such that high-volume hospitals above the 80th percentile performed 299 (95% CI: 299-311) procedures, and highest-volume hospitals above the 90th percentile performed 375 (95% CI: 375-375) procedures during this interval. Children underwent corrective surgery for congenital hand differences at significantly earlier age when treated at above-median case volume hospitals (P < .001, 14.2 months vs 16.4 months). Family income was significantly higher for patients treated at above-median case volume hospitals (P < .001, $45002 vs $41819), high-volume hospitals (P < .001, $49665 vs $41732), and highest-volume hospitals (P < .001, $52065 vs $42220). Patients living in urban communities (P < .001, 27.6% vs 12.0%) and patients with commercial insurance (P < .001, 31.2% vs 21.5%) were significantly more likely to be treated at high-volume hospitals. Those living in underserved areas were significantly less likely to be treated at high-volume hospitals (P < .001, 9.9% vs 26.5%). Patients treated at highest-volume hospitals had significantly lower billed charges (P < .001, $16064 vs $18256). On multivariate regression, patients with above-median income (P < .001, AOR = 1.7), living in an urban community (P < .001, AOR = 2.7), and with commercial insurance (P < .001, AOR = 1.6) were significantly more likely to be treated at high-volume hospitals [Figure 1].
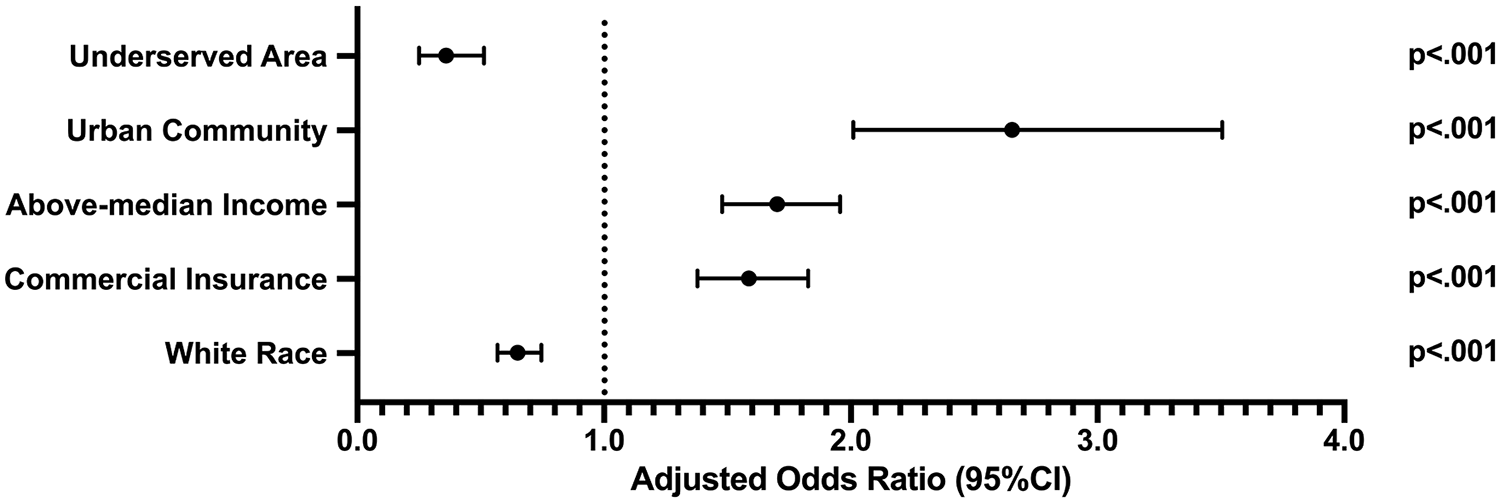
Logistic regression adjusted odds ratios of being treated at a high-volume hospital.
Hospital Choice
Median distance to the nearest hospital for children undergoing congenital hand surgery was 66 miles (95% CI: 61-69). There were 89.1% of patients (n = 2094) with a tertiary children’s hospital available in their state, however nearly half of patients chose to seek care at a distant hospital rather than one locally available (49.5%, n = 1172). Of those choosing a farther hospital, most patients chose a higher-volume hospital (80.9%, n = 948 of 1172). These patients traveled an additional 60 miles (95% CI: 54-68) beyond their local hospital to seek higher-volume care. In multivariate regression, white patients were significantly more likely to choose a farther higher-volume hospital for congenital hand surgery (P < .001, AOR = 2.1).
Financial Disparities
Patients encountered median billed charges of $17846 (95% CI: $17498-$18216) for their admission encounter undergoing surgery for congenital hand surgery. There was a significant difference among these procedure types (P < .001), such that patients were charged the most for pollicization (median $27,871), followed by syndactyly repair (median $22,932) and polydactyly repair (median $13,916). On multivariate regression, patients with white race (P < .001, B = + $3038) and above-median income (P = .011, B = + $1054) were billed significantly more. Insurance type (P = .231), living in an urban community (P = .137), and living in an underserved area (P = .485) did not affect amount billed [Figure 2].
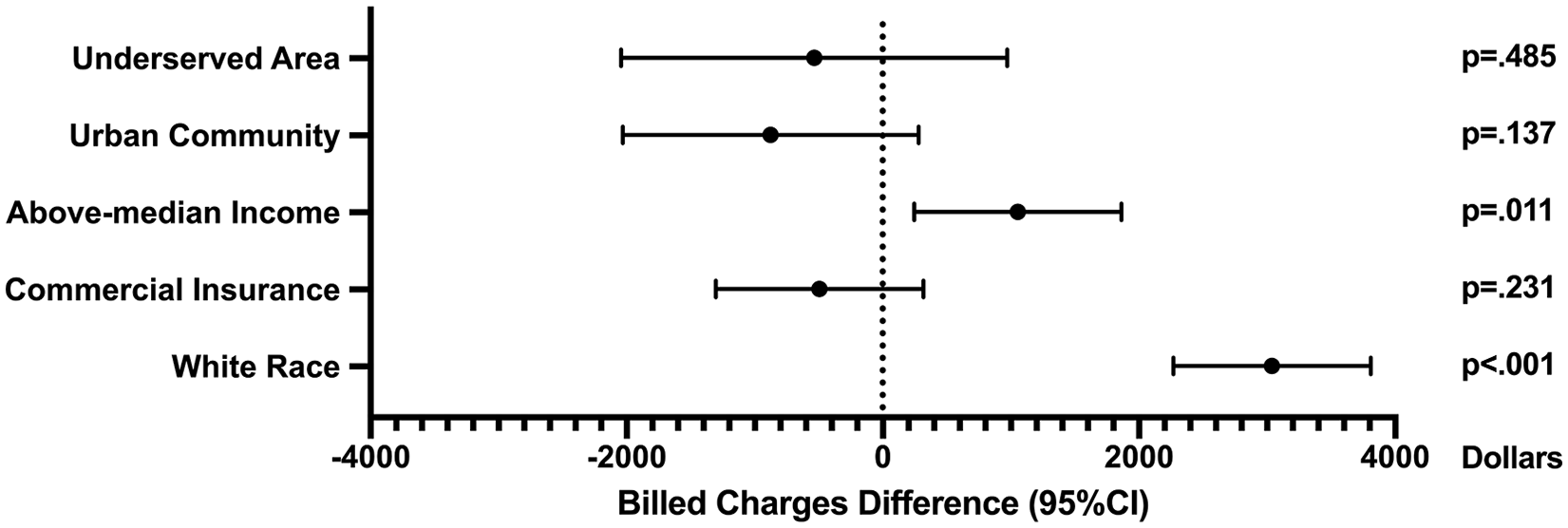
Linear regression beta coefficients of socioeconomic factors affecting billed charges.
Median overall charge-to-cost ratio was 3.31 (95% CI: 3.31-3.39) [Figure 3]. There was significant difference among these procedure types (P < .001), such that patients were imposed the highest charge-to-cost ratio for polydactyly repair (median 3.42), followed by syndactyly repair (median 3.23) and pollicization (median 2.67). On multivariate regression, patients living in an urban community (P < .001, B = + 0.147 ratio points) and living in an underserved area (P = .041, B = + .119 ratio points) were imposed a significantly higher charge-to-cost ratio, whereas patients with above-median income (P = .031, B = −0.067 ratio points) and with commercial insurance (P < .001, B = −0.213 ratio points) were imposed a significantly lower charge-to-cost ratio [Figure 4].
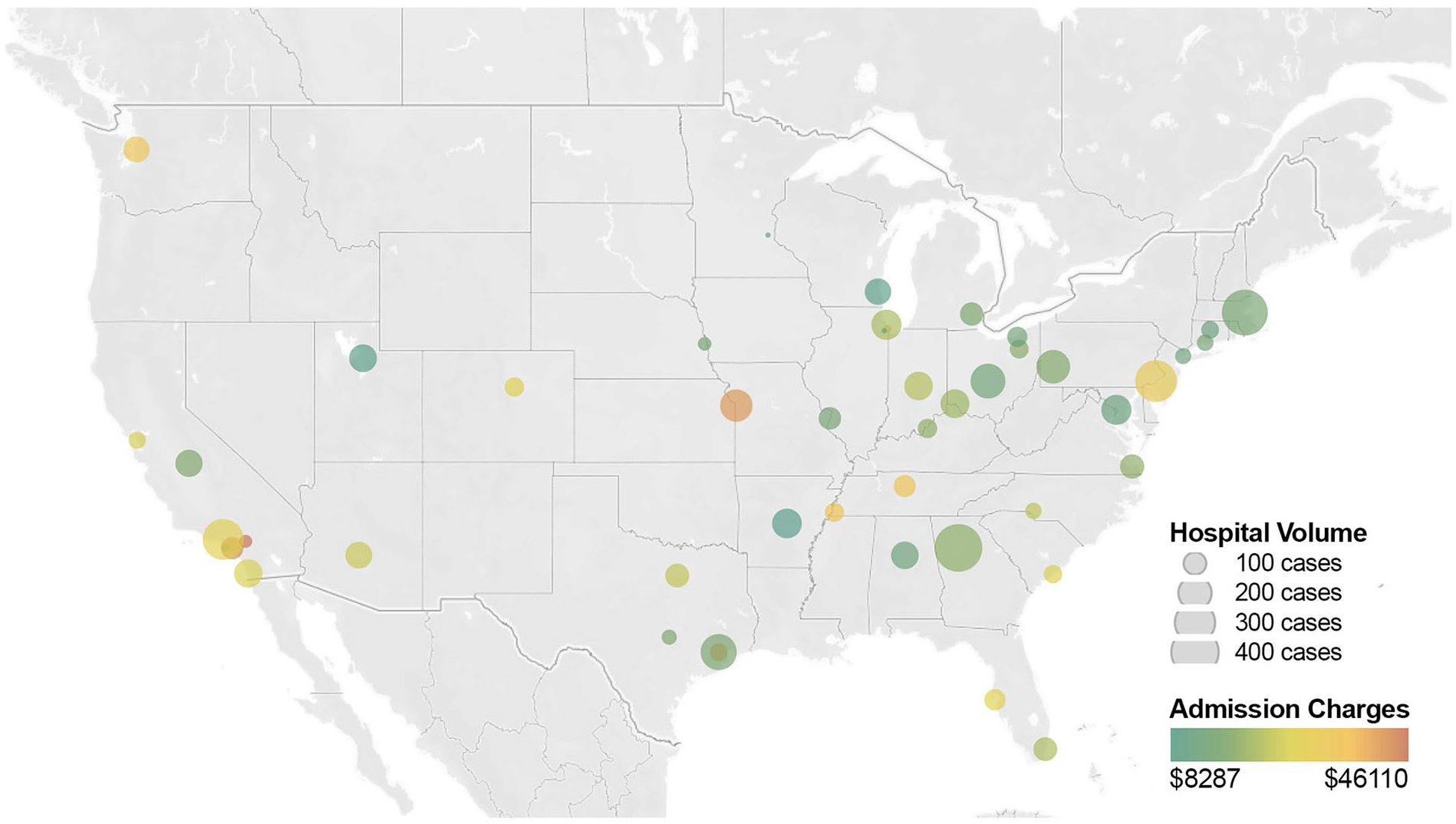
Hospital case volume and billed admission charges.
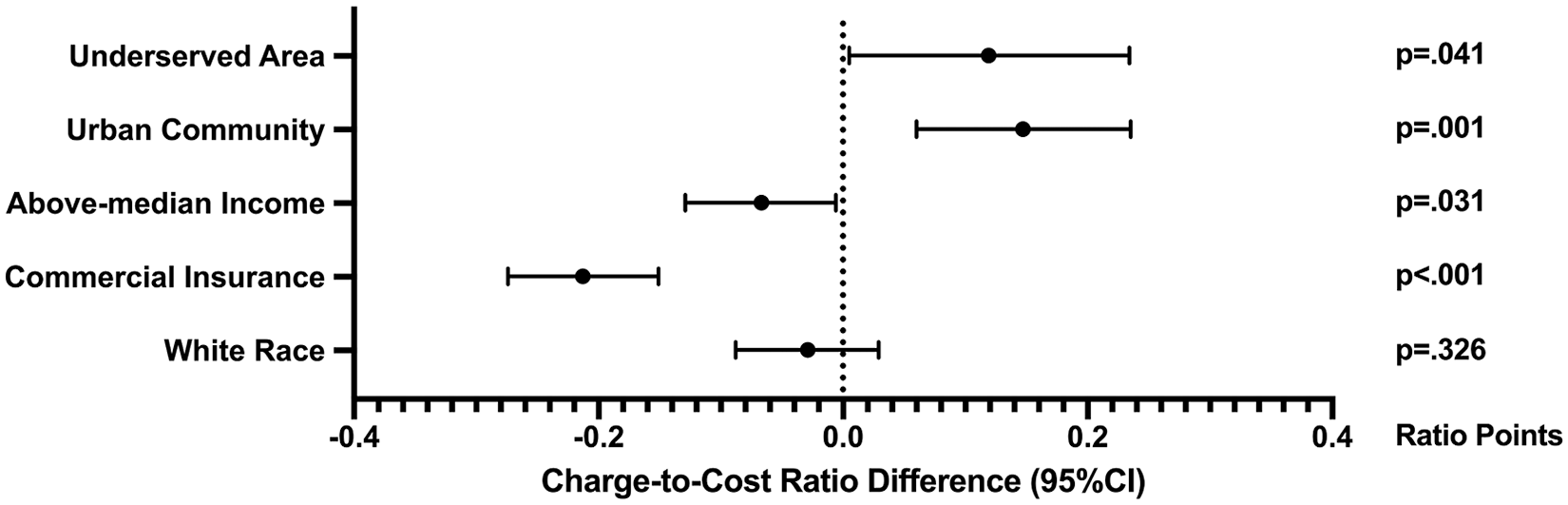
Linear regression beta coefficients of socioeconomic factors affecting charge-to-cost ratios.
Regional Differences
Billed charges varied significantly across the country (P < .001), such that patients from the Pacific region were billed the most (median $24009), and patients from New England were billed the least (median $14043) [Figure 5]. Charge-to-cost ratios likewise varied significantly across the country (P < .001), such that patients from the East South Central region had the highest charge-to-cost ratio (median 4.84), and patients from New England had the lowest charge-to-cost ratio (median 2.14). Patients in New England had the highest proportion of commercial insurance (56.7%, n = 272 of 480), whereas those in the East South Central region had the lowest (30.3%, n = 108 of 356). Proportion of patients treated at high-volume hand surgery centers was significantly different across regions of the country (P < .001) [Figure 6]. Patients from New England were most likely to be treated at high-volume centers (78.1%, n = 375 of 480) whereas those in the East North Central (0.0%, n = 0 of 1050), East South Central (0.0%, n = 0 of 356), Mountain (0.0%, n = 0 of 333), West North Central (0.0%, n = 0 of 317), and West South Central (0.0%, n = 0 of 590) regions were the least likely to be treated at high-volume centers.
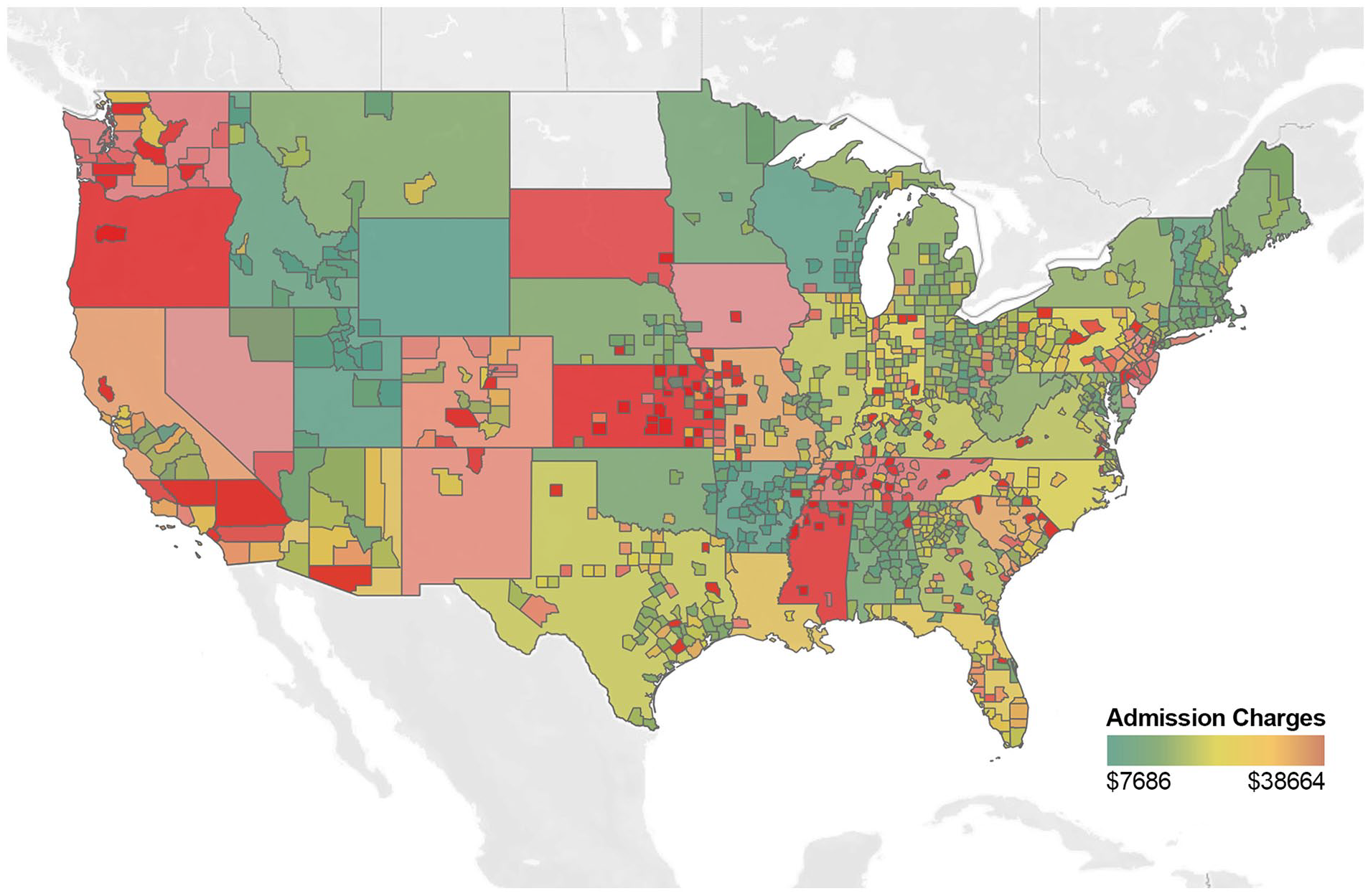
Admission charges by patient state and county.
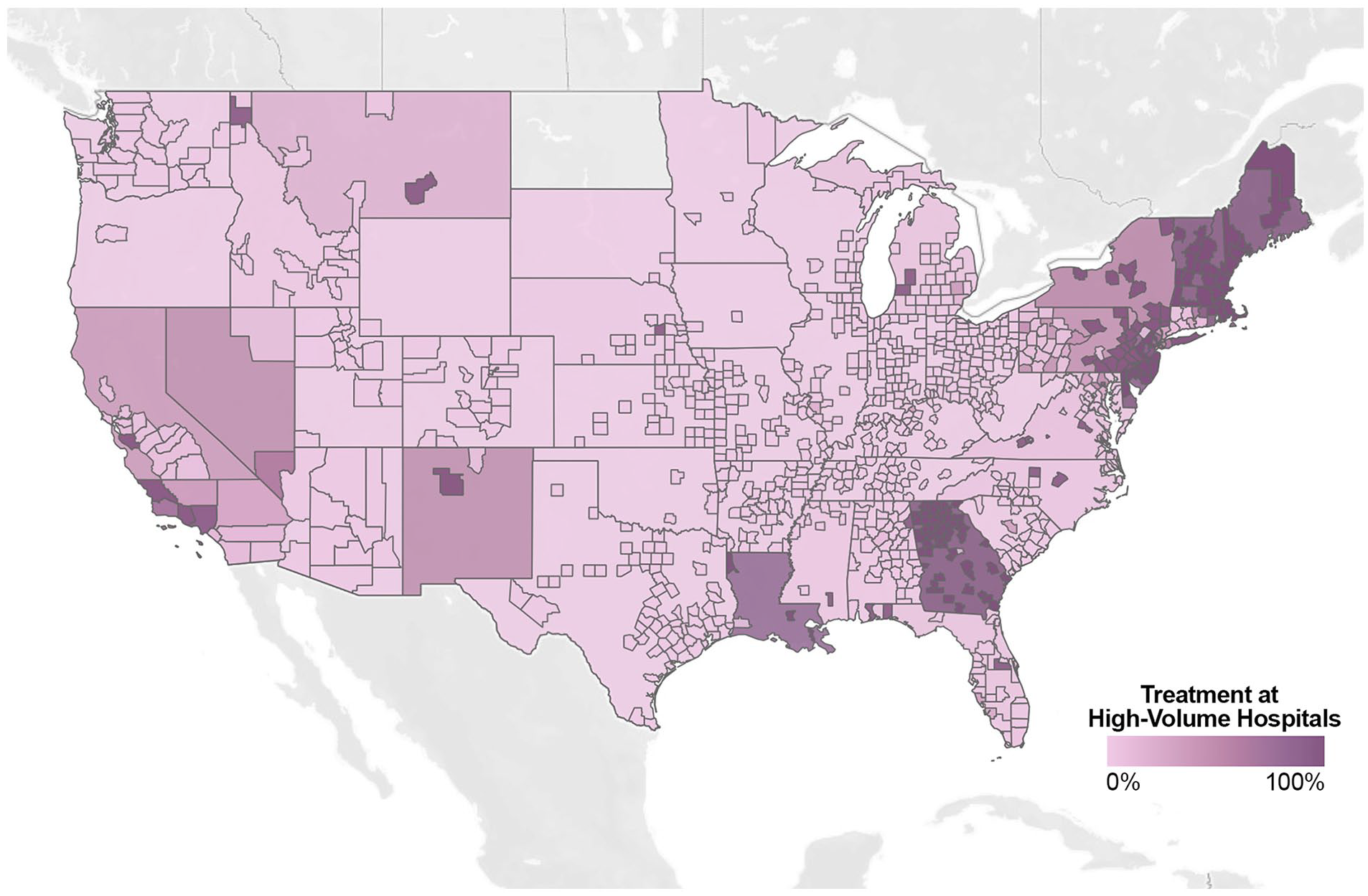
Proportion of patients treated at high-volume hand surgery centers by state and county.
Discussion
This study demonstrates the influence of socioeconomic factors on access to congenital hand surgery and financial disparities across the country. Not surprisingly, patients from areas of higher socioeconomic status have greater access to higher-volume hospitals, and treatment at hospitals with higher case volume is associated with significantly earlier age at surgery and decreased hospital admission charges. In addition to inequalities within individual communities, these disparities also exist more broadly across geographic regions of the country.
Although these disparities are rooted in deeper social determinants than any multivariate regression can accommodate, developing an appreciation for socioeconomic factors that affect access to specialty care may help improve outcomes for patients undergoing surgery for congenital hand differences. Given the compounded downstream effects of inadequate healthcare access, 27 the presence of disparities so early in life is especially concerning.
Receiving earlier care may be an indicator of better healthcare access,19,28,29 and living in rural communities has been demonstrated to result in longer intervals until definitive surgical management. 30 Patients of non-white race, with government insurance, living in distant areas of residence, and other forms of socioeconomic disadvantage have been demonstrated to suffer delayed diagnosis and/or treatment of pediatric surgical pathologies.19,28,29,31-35
Congenital disease treated by other pediatric surgical specialties have noted significantly younger age at operation when treated by high-volume centers. 36 Children underwent surgery for congenital hand differences at significantly earlier age when treated at above-median case volume hospitals (P < .001), and this was correlated with family income as well. Infants undergoing surgery for craniosynostosis have similarly been shown to experience delays in surgical intervention if they were non-white and had government insurance. 37 Patients with above-median income (P < .001), living in an urban community (P < .001), and with commercial insurance (P < .001) were significantly more likely to be treated at high-volume hospitals. Infants undergoing surgery for other conditions have similarly been shown to receive care at higher-volume hospitals if they were white and had private insurance. 9
Patients undergoing procedures by plastic surgeons for other pediatric pathologies have been demonstrated to achieve better outcomes at lower costs when treated by high-volume hospitals.38-40 In this study, patients with congenital hand differences treated by the highest-volume hospitals (P < .001) had lower billed charges. Children undergoing orthognathic surgery have similarly been shown to experience lower costs when treated by high-volume surgeons. 40 Further research will be needed into these admission charges to decipher whether there were socioeconomic disparities in the amount billed for procedures, or whether these hospital charges were higher due to prolonged lengths of stay and increased hospital resources utilized in certain populations.
Limitations of this study include its retrospective design and lack of procedure-specific outcomes, which precludes capturing clinical results. Second, although CPT procedure codes utilized by this database reliably delineate the index surgical procedures, the underlying complexities of pathology and surgical repair are difficult to capture. Third, household income underestimates socioeconomic disparities. Household net worth would be a more accurate assessment of financial assets available for influencing medical care. Fourth, this database only includes encounter-level data, which precludes longitudinal analysis of long-term outcomes. Fifth, this study is not equipped to demonstrate whether these disparities are causative of differences in postoperative outcomes. For example, the 2-month difference in age at surgery based on treatment at high-volume centers may or may not result in better functional and aesthetic outcomes. We hope that this nationwide study will be an impetus for institution-specific studies that can perform more granular analyses to track the entry of patients into their hand surgery care pathway from time of referral, as well as track patient follow-up duration to ensure patients are able to adequately access postoperative physical and occupational therapy.
Despite some limitations, this is the first study of socioeconomic disparities in children undergoing surgery for congenital hand differences. This robust dataset with thousands of patients across the country from 50 pediatric hospitals over 10 years helps to provide a substantially representative sample of congenital hand surgery procedures nationwide to highlight several modifiable and unmodifiable factors affecting pediatric patients with congenital hand differences.
Conclusion
Access to highest-volume hospitals and admission charges are disproportionally experienced across socioeconomic spectrums of pediatric patients undergoing surgery for congenital hand differences. Patients with higher socioeconomic status are significantly more likely to be treated at high-volume hospitals, and treatment at hospitals with higher case volume is associated with significantly earlier age at surgery and decreased hospital admission charges. Future study of initiatives to combat these inequalities with an analysis of their impact would be helpful for communities to begin implementing necessary policies that would effectively begin mitigating these disparities in care.
Supplemental Material
sj-pdf-1-han-10.1177_15589447221092059 – Supplemental material for Socioeconomic Disparities in Surgical Care for Congenital Hand Differences
Supplemental material, sj-pdf-1-han-10.1177_15589447221092059 for Socioeconomic Disparities in Surgical Care for Congenital Hand Differences by Christopher L. Kalmar and Brian C. Drolet in HAND
Footnotes
Supplemental material
Supplemental material is available in the online version of the article.
Ethical Approval
Institutional Review Board approval was not required.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This article does not contain any studies with identifiable human information and informed consent was not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.