
Abstract
The one-bone forearm (OBF) is a salvage technique that may be used to correct global forearm instability secondary to osseous defects. This study aims to provide an overview of the contemporary literature regarding the OBF. A literature review was conducted electronically across MEDLINE, Embase, and PubMed databases in May 2020. Studies were eligible for inclusion if published in the English language; detailed the use of the OBF procedure to correct forearm instability; and were original data studies reporting qualitative or quantitative outcomes. Thirty-four studies, describing a cohort of 210 patients undergoing 211 OBFs, were documented in the literature. The primary etiology necessitating the OBF was trauma, followed by genetic/congenital disorders and infections. Technically, the OBF was most frequently achieved via an end-to-end osteosynthesis with plate fixation. In total, 85.0% (154/182) of OBF were fused in neutral rotation or varying degrees of pronation. Union was achieved in more than 80.0% (174/211) of OBFs. The OBF is a feasible salvage technique that has been used for a wide spectrum of pathology, providing satisfactory outcomes in most cases.
Introduction
The one-bone forearm (OBF) is a salvage surgical option in the setting of forearm instability secondary to significant bony and/or soft tissue deficits, where other reconstructive techniques have failed or are unlikely to succeed. In constructing an osseus bridge between the deficient forearm bones, the OBF aims to alleviate pain, improve forearm growth potential in the pediatric setting, and promote functional use of the affected limb.1-4 The OBF has been used to address forearm instability due to a range of pathology, including trauma, benign and malignant tumor resections, failed corrective surgeries, infection, genetic disease, and congenital abnormalities.2,5 Preliminary results from the implementation of the OBF note reasonable functional and cosmetic outcomes, as well as patient satisfaction.6-9
The principles of the OBF procedure were initially described over a century ago; in 1921, Hey Groves successfully fixed the distal radial metaphysis to the proximal ulna following failure of bone grafting for a distal radius nonunion.7,10 Anatomically and functionally, the OBF is the fusion of the proximal ulna to the distal radius (also known as the “ulnius”), resulting in a stable link between the elbow and wrist joints4,11 (Figure 1). Wang et al 12 believed that “end-to-end” fusion was the optimal approach to achieve this outcome. An alternative methodology is radioulnar synostosis—the “side-to-side” collocation and osteosynthesis of the proximal ulna and distal radius.2,11 Independent of the technique used, anatomical prerequisites for a satisfactory result are intact radiocarpal and ulnohumeral joints—as emphasized by Vitale, “the ulna makes the elbow” and “the radius makes the wrist.”4,10,12-15 Inevitable in the creation of the OBF is the loss of forearm rotation, justified by the symptomatic relief and functional gain, as well as the compensation afforded at the shoulder and within the wrist joint.2,16-18
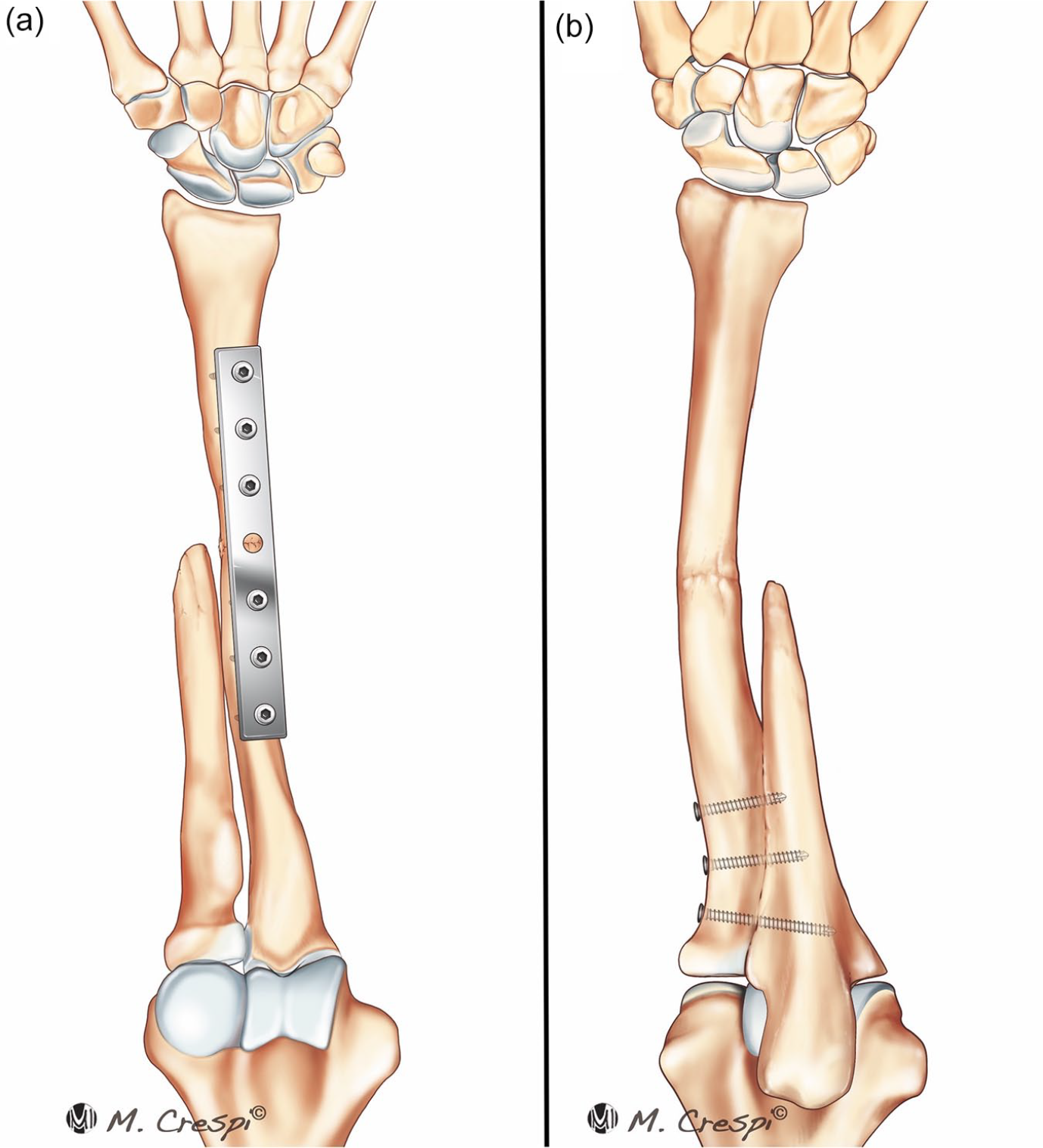
The one-bone forearm. The one-bone forearm is commonly constructed in either (a) an “end-to-end” or (b) “side-to-side” mode of fixation.
Although used for a range of pathology, there is no consensus as to the appropriate indications or optimal technique. 19 Various authors have postulated that the OBF should be ideally used in the context of forearm angular, axial, or radioulnar instability due to significant or refractory osseous defect and comminution where reconstruction of the defective forearm is not amenable to other fixation methods (eg, structural or nonstructural bone grafting with rigid internal fixation, vascularized bone transfers, prosthetic spacer interposition, and shorting osteotomy with subsequent internal fixation).1,7,11,19
Due to disparate etiologies, techniques, and patient demographics, the outcomes of the OBF are heterogeneous and, to our knowledge, have not been previously collated. Thus, the aim of this review is to review the literature on OBF, synthesizing the available data and providing an overview.
Methods
Literature Search
In May 2020, an electronic literature search was performed across 4 electronic databases (OVID MEDLINE, PubMed, the Cochrane Controlled Register of Trials, and Embase). To maximize sensitivity, the search was conducted with the following terms and operatives: ([“Single Bone Forearm”] AND [“outcomes”]) OR ([“One Bone Forearm”] AND [“outcomes”]).
Study Selection and Screening
A predefined set of inclusion and exclusion criteria were applied to determine relevance. Eligible studies included those reporting on OBFs with original quantitative and/or qualitative data. Studies were excluded if the manuscript was published in a language other than English, were not peer reviewed, or did not contain original data. Reference lists of included studies were then reviewed for any additional relevant articles.
The 2-stage screening process was independently performed by 2 authors (I.M. and J.M.) via Rayyan Qatar Computing Research Institute (QCRI; Ar-Rayyan, Qatar) and EndNote (Clarivate, Philadelphia, Pennsylvania), respectively. Any conflicts were resolved by the senior author (B.S.).
Data Extraction
Data were extracted from the text, illustrations, and tables of each selected study as available. Extracted data included study details, patient demographics, operative indications and techniques, and clinical outcomes.
Data Analysis
Given the heterogeneity of the study designs and reporting methods, a meta-analysis of the data could not be performed. Simple statistics and pooled analysis of the data was performed where possible.
Results
Search Results
An initial search of the electronic databases identified 258 potential studies for review. Following abstract and full-text screening, a total of 19 studies were available for full-text analysis. Manual review of reference lists from each study yielded an additional 15 studies for inclusion and analysis.1,2,4-35 See Figure 2.
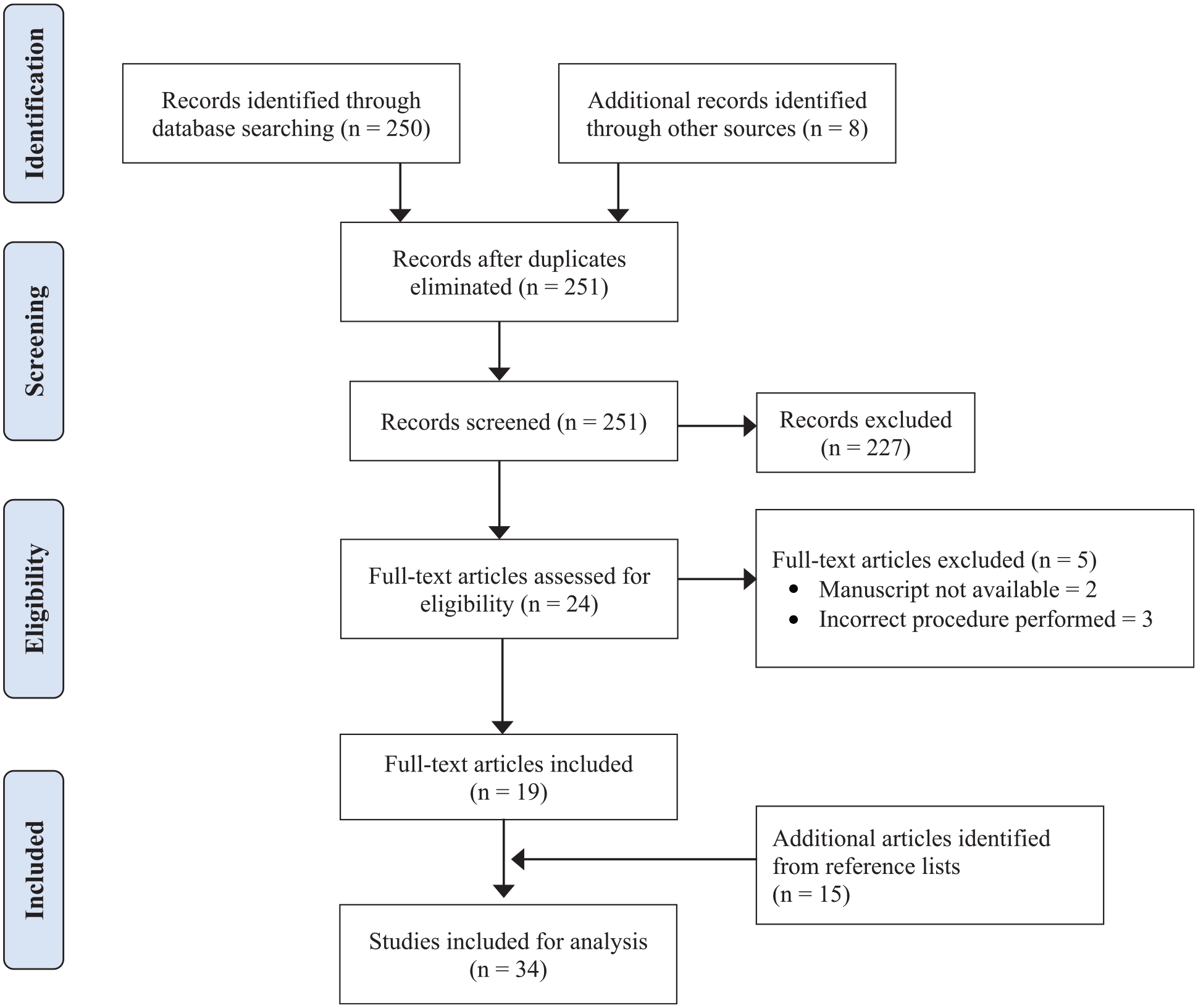
Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA] diagram of one-bone forearm literature search.
Study Characteristics
As the per the Oxford Centre for Evidence-Based Medicine classification, 73.5% of the studies were of level 4 quality (n = 25) with the remaining 26.5% being level 5 quality (n = 9). The included studies were published between 1934 and 2020. Study characteristics are summarized in Table 1.
Summary of Included Studies.
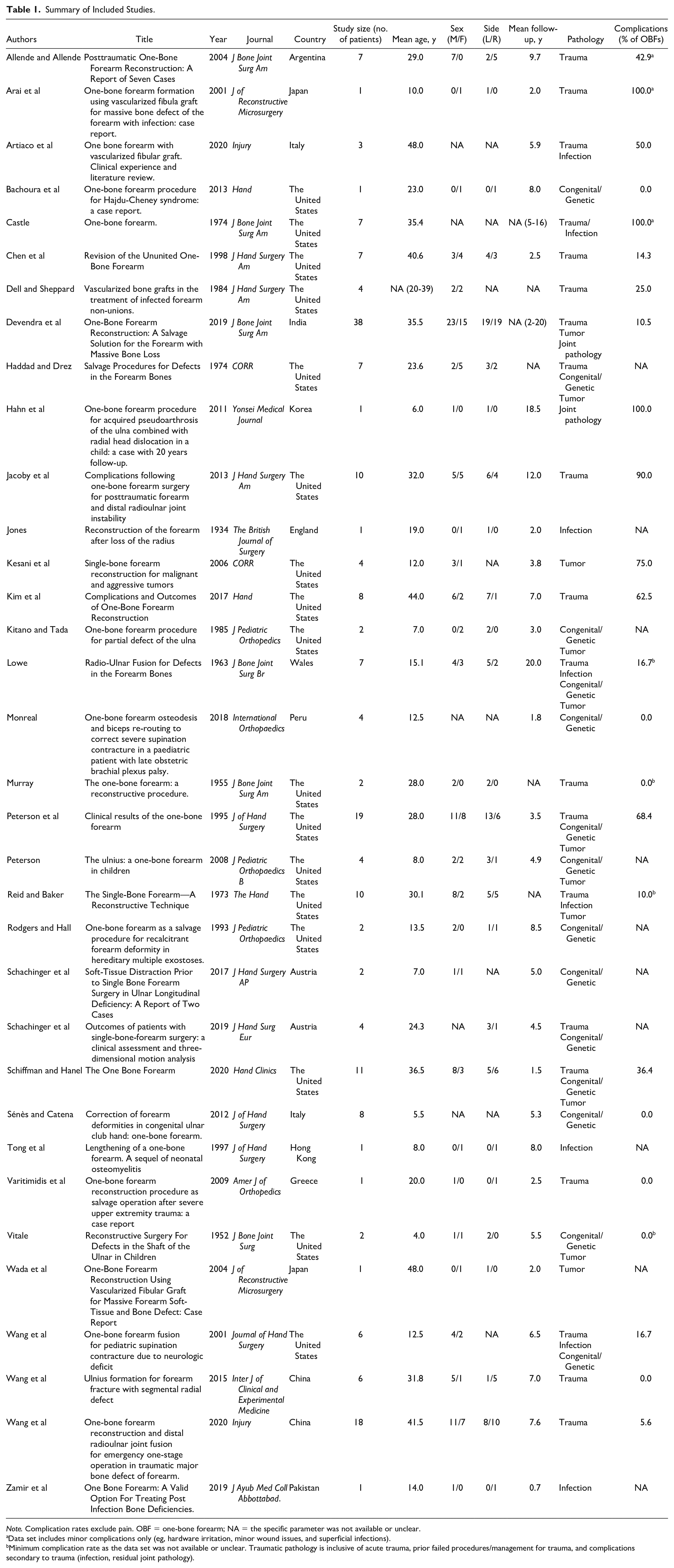
Note. Complication rates exclude pain. OBF = one-bone forearm; NA = the specific parameter was not available or unclear.
Data set includes minor complications only (eg, hardware irritation, minor wound issues, and superficial infections).
Minimum complication rate as the data set was not available or unclear. Traumatic pathology is inclusive of acute trauma, prior failed procedures/management for trauma, and complications secondary to trauma (infection, residual joint pathology).
Patient Demographics
The 34 studies yielded a cohort of 210 patients with 211 OBF procedures performed. Patient age was reported in 33 of the studies, with a weighted mean of 28.9 years (range: 3-70 years). Sex was mentioned in 29 of the studies (n = 184), with women composing 38.6% of patients undergoing the OBF procedure. The affected limb was reported in 26 studies (n = 170), with 38.8% of operations performed on the dominant side. The number of surgeries before OBF was cited in 14 studies (n = 95) with a weighted mean of 3.2 surgeries (range: 0-20 surgeries). Twenty-eight studies (n = 142) reported a weighted mean follow-up of 6.4 years (range: 0-21 years).
Clinical Pathology
The clinical pathology for OBF was recorded in all studies. Approximately two-thirds (140/211) of the OBFs performed were due to trauma or an associated complication (such as failed reconstruction or infection); 15.6% (33/211) of OBFs were undertaken secondary to congenital disorders (such as neurofibromatosis or ulnar longitudinal deficiencies), followed by tumors and malignancy (10.9%, 23/211). Infection (4.7%, 10/211) and atraumatic joint pathologies (2.4%, 5/211) made up the remainder.
Surgical Technique
The most common technique for the OBF was an end-to-end fusion (74.6%, 144/193); side-to-side osteosynthesis was also commonly performed (25.4%, 49/193). For approximately 8.5% (18/211) of OBFs, either the technique used was unclear or another technical variant was used.
Plates and screws (54.9%, 96/175) were the most common fixation medium, followed by screws alone (21.1%, 37/175) and intramedullary fixation (9.7%, 17/175); 14.3% (25/175) of OBFs were constructed by other means inclusive of Kirschner wire (K-wire) or cross-pin fixation. The method of fixation was unclear or undocumented in 17.5% (37/211) of OBFs.
The use of bone augmentation was documented in 93 of 112 OBF, with 26 of these using a free fibular bone flap.
The most frequent fixation position was pronation (34.6%, 63/182), followed by neutral rotation (28.0%, 51/182), then supination (15.4%, 28/182). Of the OBFs secured in pronation, 81.0% (51/63) were fixed between 1° and 30° of pronation; 71.4% (20/28) of those fixed in supination sat in between 60° and 90° of supination. Ultimately, fixation in neutral or pronation made up 84.6% (154/182) of OBFs in the literature. The fusion position was unclear or not documented in 13.7% (29/211) of OBFs. See Table 2.
Mode of Fixation and Position of Fusion Used for OBFs Where Reported.
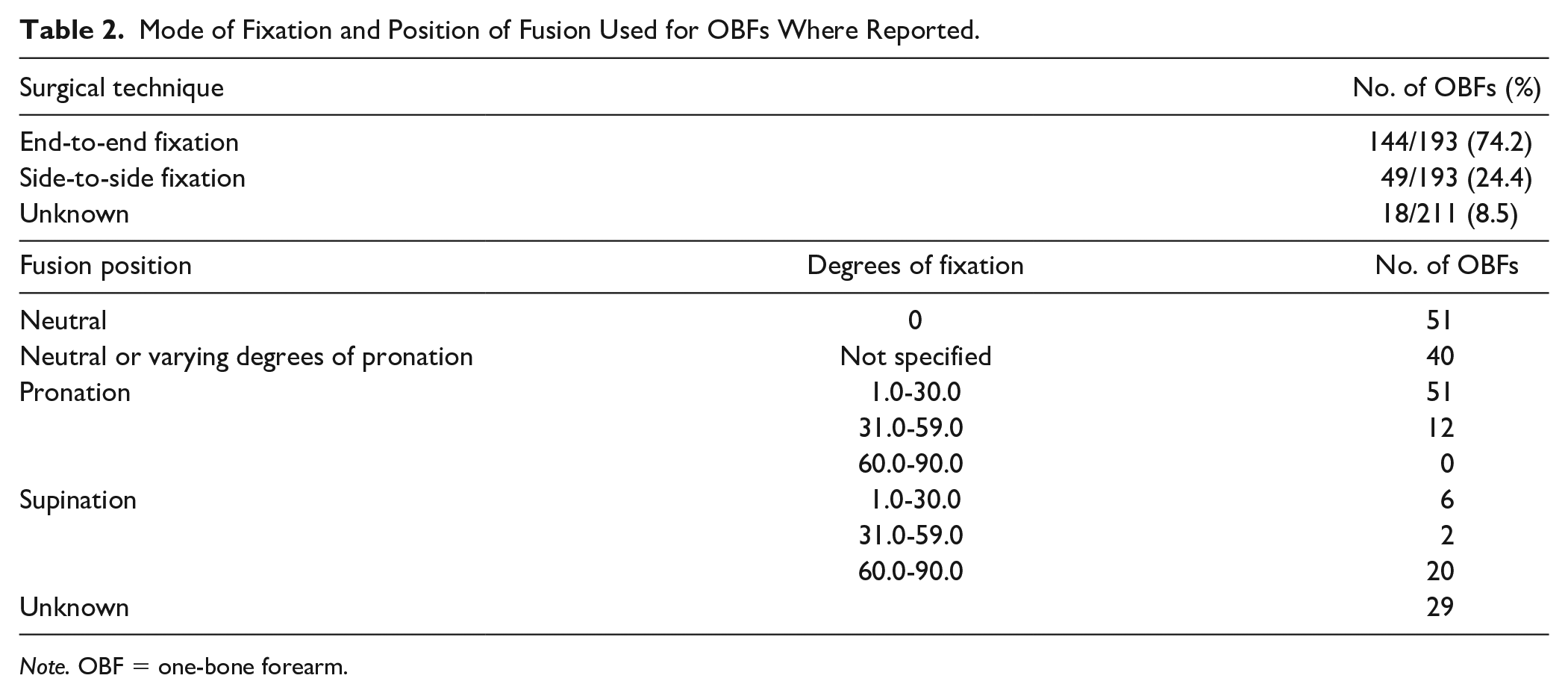
Note. OBF = one-bone forearm.
Clinical Outcomes
Union
Union was reported in 34 studies (n = 199, 94.3% of cohort) with a nonunion range of 0% to 50%. Union (including delayed union) was achieved in 87.4% (174/199) of OBFs. The time to union ranged between 1.5 and 24 months.
Functional Outcomes
Functional outcomes were presented for 29 studies (n = 137, 65.2% of cohort). A total of 137 patients, as a minimum, had acceptable function of their limb as defined by clinical assessment, ability to perform activities of daily living (eg, household chores), or the patient’s faculty to contribute to society—with 63.5% (87/137) being able to return to some form of work.
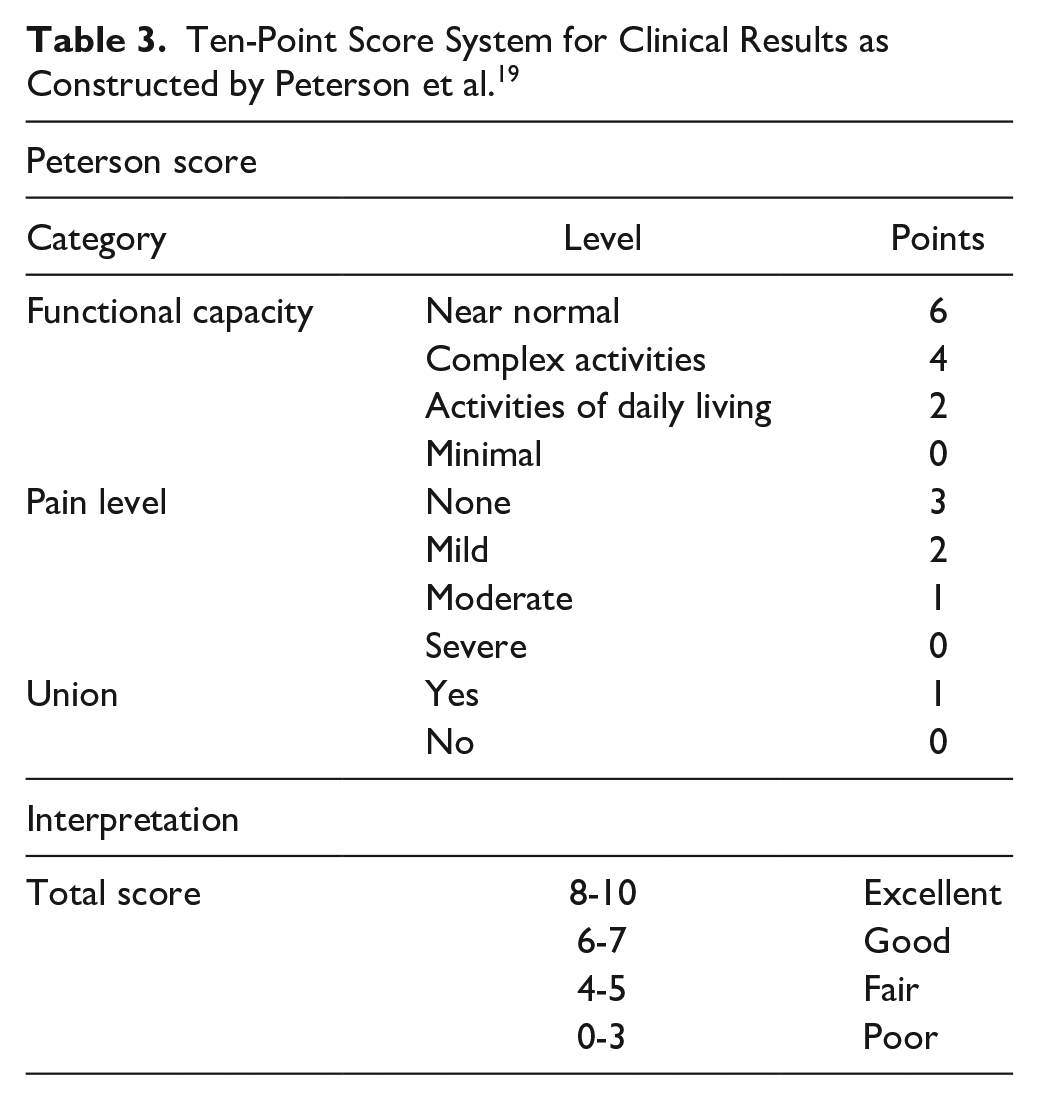
The Peterson score, a subjective 10-point scoring system based on functional capacity, pain level, and union, was reported for 81 patients with a weighted mean of 7.0—which corresponds to a good clinical outcome. 19 In addition, this score was presented qualitatively in 88 patients, with 37, 34, 10, and 7 patients being classified as excellent, good, fair, and poor, respectively. See Table 3.
Ten-Point Score System for Clinical Results as Constructed by Peterson et al. 19
Range of Motion
Elbow range of motion was reported to varying degrees in 21 studies (n = 94, 44.5% of cohort). The weighted average of postoperative elbow extension and flexion was 5.1° and 128.0°, respectively (n = 51, extension range: 0.0°-40.0°, flexion range: 80.0°-141.3°). Qualitatively, full range of motion was recorded for 43 patients.
Similarly, range of motion at the wrist was reported in 92 patients. The weighed mean of postoperative wrist extension and flexion was 31.5° and 36.3°, respectively (n = 76, extension range: 19.1°-80.0°, flexion range: 26.8°-70.0°). Full range of motion at the wrist was recorded for an additional 16 patients.
Satisfaction
Patient satisfaction was reported in 20 studies (n = 115 patients, 54.8% of the cohort); 96.5% (111/115) of patients were satisfied with their function, outcomes, or cosmesis.
Shortening
Shortening was reported in 90 patients (42.7% of cohort) with a range of forearm reduction between 0.0 and 14.0 cm and a weighted mean of 4.0 cm (n = 78); 86.7% (78/90) of OBFs were shorter than the contralateral side.
Pain
Pain outcomes were noted in 22 studies (n = 155, 73.8% of cohort). In total, 62.5% (60/96) of patients were pain free at follow-up, with the remainder reporting some level of pain or discomfort; 59 patients had their pain score incorporated into the Peterson score.
Complications
Complication outcomes were reported in 24 studies (n = 175, 82.9% of cohort), with rates of complications ranging between 0.0% and 90.0%; 33.1% (58/175) of patients had 83 complications (excluding pain) inclusive of nonunion (30.1%), symptomatic hardware (25.3%), infection (12.0%), wound-related issues (9.6%), nerve pathology (eg, carpal tunnel syndrome, 7.2%), musculoskeletal pathology (7.2%), and deformity (1.2%). See Table 4.
Clinical Outcomes of the Available Data.
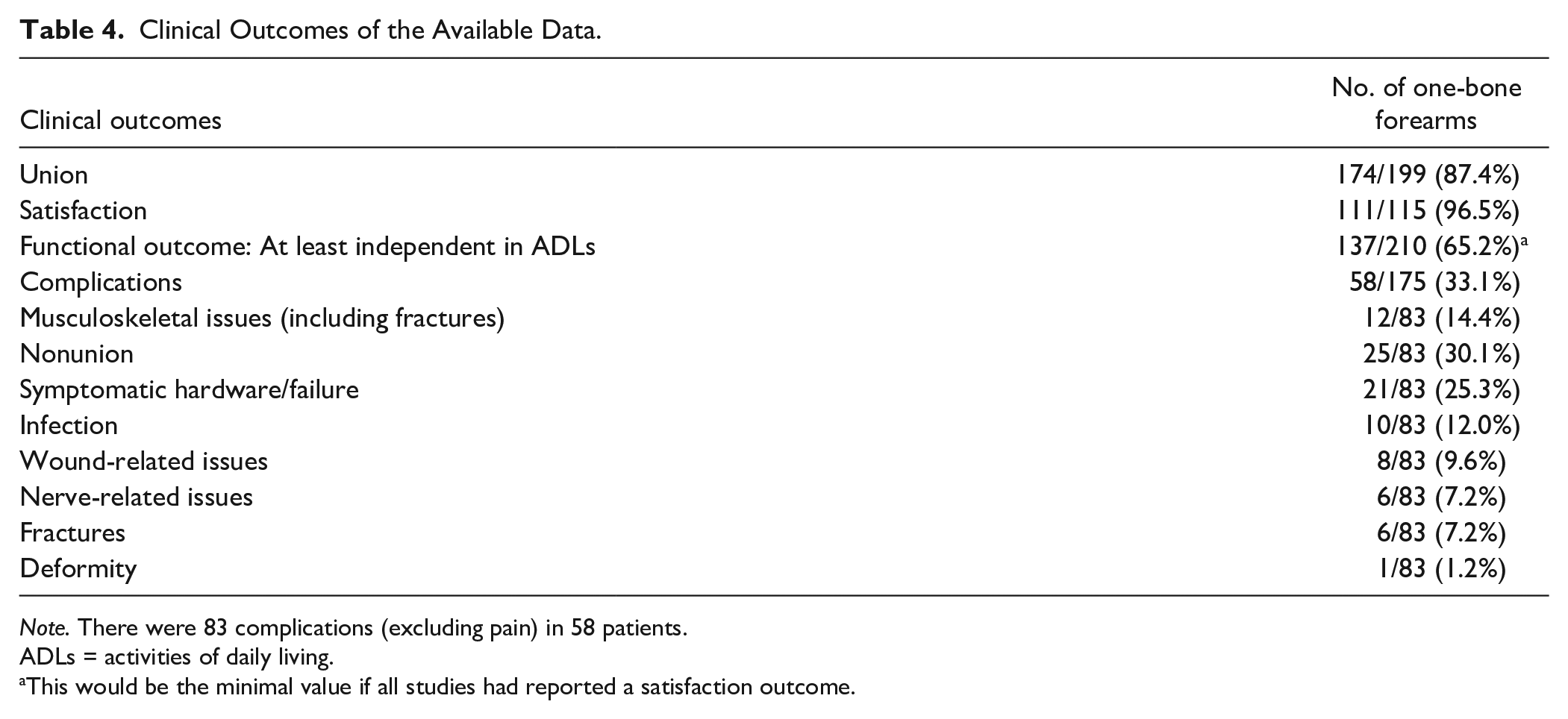
Note. There were 83 complications (excluding pain) in 58 patients.
ADLs = activities of daily living.
This would be the minimal value if all studies had reported a satisfaction outcome.
Discussion
The OBF as a salvage procedure for global forearm instability has provided largely positive outcomes in terms of functional outcomes and patient satisfaction.2,5,15 This study reviewed the contemporary literature and found that many patients were satisfied with their outcomes and had regained at least independence in activities of daily living. However, the pooled complication rate (where reported) was close to 33% with a 12.6% risk of nonunion.
The OBF has been performed for a spectrum of clinical pathologies and is indicated in the setting of instability or bone loss which is nonreconstructable via bone grafting or other methods, particularly when there is no likelihood of restoring forearm rotation. 16 In this review, it was employed most commonly following traumatic injuries or their sequalae, followed by congenital disorders or post-tumor resection.
The surgical techniques used to create a successful OBF vary throughout the literature and include both side-to-side osteosynthesis via screw or cross-pin fixation and end-to-end osteosynthesis using K-wires, intramedullary rods, or plates. The anatomical prerequisites to ensure a “good” result are a structurally intact hand, ulnocarpal, and radiocarpal joints. 10 This study revealed that more than two-thirds of the OBFs in the literature were constructed in an end-to-end technique, with plate fixation being the most common stabilization method. Chen et al 11 found success in using end-to-end osteosynthesis when revising multiple OBFs performed via the side-to-side method. Furthermore, several studies have revealed higher rates of nonunion with side-to-side osteosynthesis.1,11,12 The optimal mode of fixation remains unclear. Plating promotes primary bone healing and allows for rigid fixation with rotational control.11,12 However, champions of intramedullary fixation advocate that the limited soft tissue dissection and periosteal stripping required may lead to more reliable bony union.1,6,10
The position of forearm fusion is important to ensure optimal postoperative function. Neutral rotation, or slight pronation, is usually advocated, although good outcomes have also been reported with the forearm fixed in supination.7,19 Increased supination allows for hand movement around the body (eg, hygiene), whereas greater pronation allows for interaction with the external environment.19,32,36 Chan et al 3 found that an OBF in 30° of pronation provided the best function for writing and working with small objects in the dominant arm. Pronation also plays a key role in typing—a function prevalent in today’s society. Moreover, the shoulder has the capacity to compensate for rotational restriction by allowing the neutral or slightly pronated forearm to attain pronation, neutral, or even slight supination. 19 Ideally, the position of fixation should be decided in discussion with the patient, and after consideration of limb dominance, occupation, and leisure pursuits. 3 In a simulated study of forearm fusion, 63% of participants preferred a neutral position, and 33% favored pronation, when asked to perform activities of daily living. 37 Peterson 4 suggested preoperative planning with bracing or casting to trial various degrees of rotation to determine the optimal forearm position. Greater than 80.0% of OBFs have been constructed in either neutral rotation or varying degrees of pronation, with approximately 15.0% in supination.
Reported complication rates range from 0% to 90%. Virtually 87% of discussed OBFs went on to unite. Peterson et al 19 reported a 32% rate of nonunion in his series (n = 19) and emphasized the need for rigid fixation, bone grafting, and appropriate postoperative immobilization to reduce this risk. Bone grafting or free fibular osseous flaps were used in more than 40.0% of OBFs, and likely reduce nonunion rates via osteogenic, osteoconductive, and osteoinductive mechanisms, with several authors suggesting that bony augmentation is essential.5,35,38 Other complications included symptomatic hardware, painful impingement of the proximal radius on the OBF, wound-related issues, nerve pathology (eg, carpal tunnel syndrome), fracture, infection, and deformity. A traumatic etiology, 2 or more prior reconstructive surgeries, past or present infection, extensive periosteal stripping and soft tissue dissection, history of nerve injury, neurofibromatosis type 1, smoking, ulnohumeral and radiocarpal arthritis, and side-to-side arthrodesis have all been identified as risk factors for complications and poorer postoperative function.1,2,5,11,12,19
It is important to acknowledge the limitations of this study. The included studies were of low quality (level 4 or 5) and heterogeneous in nature. The sporadic and sometimes limited reporting of outcomes in the included studies meant that strong inferences could not be derived, and further pooled meta-analysis was not appropriate. However, the strength of this study is that it is an extensive contemporary review on the indications, techniques, and outcomes following OBF available in the literature.
Conclusions
The OBF is a viable salvage procedure which has been used for a spectrum of pathology with largely positive outcomes in the context of function and patient satisfaction. Several complications have been associated with the procedure, including chronic pain and malunion or nonunion. These may be minimized with careful patient selection and preoperative management of risk factors, the utilization of specific surgical techniques, and diligent postoperative rehabilitation.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
Not applicable.
Statement of Informed Consent
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.