
Abstract
Background:
Diabetes is a well-established risk factor for severe digital infection, and patients are more likely to require digital amputation for adequate source control. This study aims to identify factors predictive of digital amputation compared with preservation in patients with diabetes who present with surgically treated finger infections.
Methods:
Current Procedural Terminology (CPT) and International Classification of Diseases Versions 9 and 10 (ICD-9/10) databases from a single academic medical center were queried to identify patients with type 1 or type 2 diabetes mellitus who underwent surgical treatment in the operating room for treatment of a digital infection from 2010 to 2020. Electronic medical records were reviewed to obtain historical and acute clinical variables at the time of hospital presentation. Bivariate and multivariable regression were used to identify factors associated with amputation.
Results:
In total, 145 patients (61 digital amputation, 84 digital preservation) met inclusion criteria for this retrospective cohort study. Mean hospital stay was 6 days, and the average patient underwent 2 operations. Multivariable analysis revealed that the presence of osteomyelitis, ipsilateral upper extremity dialysis fistula, end-stage renal disease, and vascular disease each had significant independent predictive value for amputation rather than digital preservation.
Conclusions:
Digital amputation is common in the setting of diabetic finger infection. The 4 variables found to independently predict the outcome of amputation can be understood as factors which decrease the likelihood of successful digital salvage and increase the potential consequence of ongoing uncontrolled infection. Further study should focus on clinical factors affecting surgical decision making and how the treatment rendered affects patient outcomes.
Introduction
Diabetes is a well-established risk factor for infections. Due to impaired wound healing and defects in cell-mediated immunity, patients have an increased susceptibility to infection and often present with more severe infections than patients without diabetes.1-6 While less common than diabetic foot infections, hand infections can also have devastating consequences causing long-term disability, ranging from chronic pain to stiffness and joint contractures to amputation.7,8 Compared with patients without diabetes, patients with diabetes who present with hand infections are more likely to require repeat debridement or amputation for adequate infectious control. 9 In the most severe cases, diabetic patients with hand infections present with sepsis requiring intensive care unit (ICU) admission and extensive resuscitative efforts in addition to prompt surgical treatment. 3
In diabetic hand infections limited to cellulitis alone, medical treatment with antibiotics is often curative. However, in the presence of devascularized tissue, abscess, tenosynovitis, osteomyelitis, or other deep infection, surgical treatment is indicated. This may entail digit preserving drainage/debridement with or without soft tissue reconstruction (Figure 1), or amputation of the affected digit (Figure 2). In some cases, either surgical strategy is feasible, and the surgeon and patient can engage in shared decision-making to decide which option is best. In other cases, amputation is necessary due to extensive tissue necrosis or infection, which is uncontrollable by other means. The functional consequences of even minor amputations are significant: Studies of patients who have undergone digital amputation reveal they have poorer motor function and impaired activities of daily living. 10 In a study of 127 patients who had 1 or more digits amputated proximal to the distal interphalangeal joint, one-quarter stated they had to change their jobs. 11 Furthermore, amputation puts patients at risk of painful neuroma, which can also substantially decrease quality of life. 12

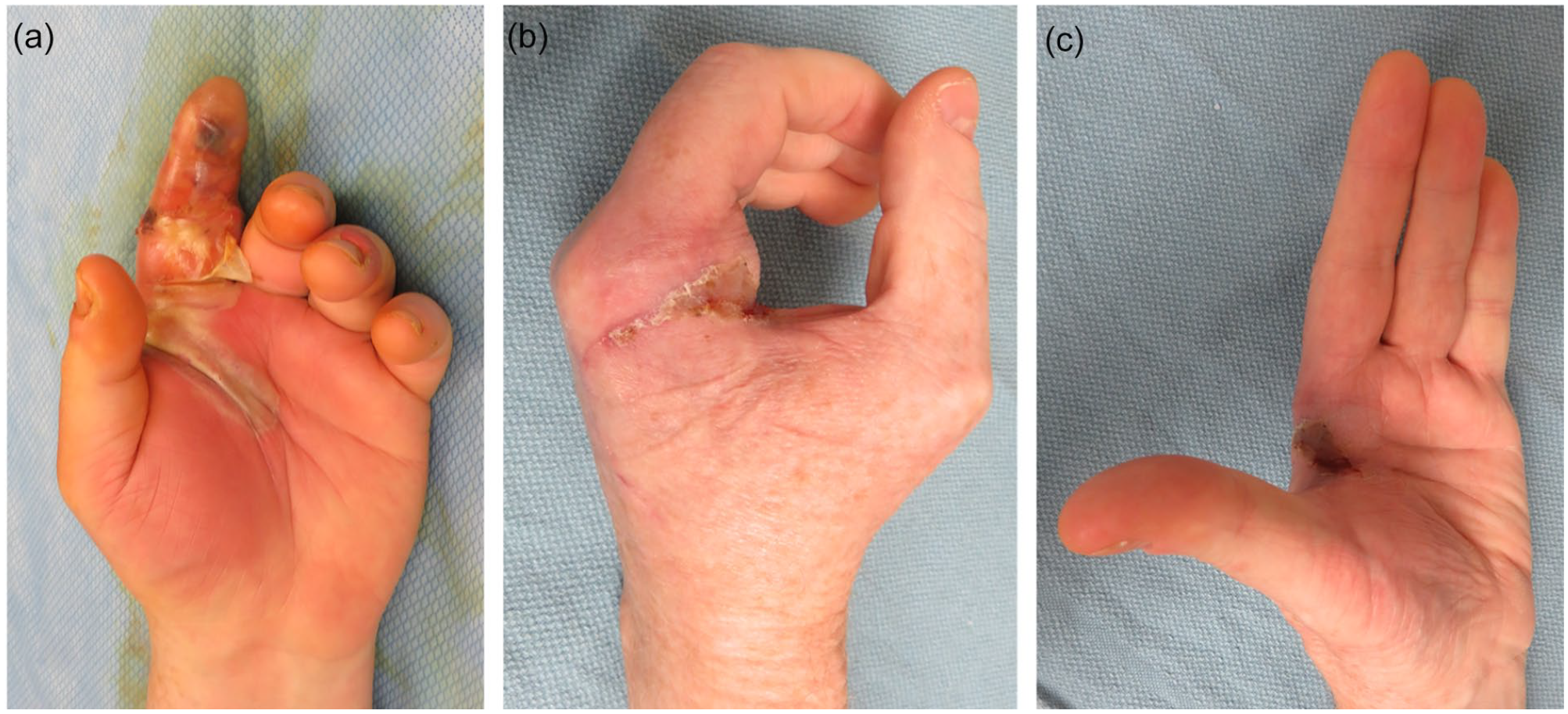
This patient presented with a dorsal middle finger subcutaneous abscess and overlying skin necrosis (a). After serial debridement and dressing care, the infection was controlled and the wound was deemed clean (b). The patient elected for reconstruction. During the first stage of reconstruction, a reverse cross-finger flap was raised from the adjacent ring finger (c), and then inset into the critical dorsal middle finger defect and covered with skin graft (d). After 3 weeks, the flap pedicle connecting the adjacent fingers as divided and final inset was completed. The patient on to heal all wounds, and hand function was satisfactory (e, f).
This patient presented with advanced bacterial flexor tenosynovitis of the index finger (a). The patient was treated with index finger ray amputation, and a small amount of skin graft was used to resurface a residual defect (b, c).
While the threshold for amputation varies by surgeon, the decision may be influenced by patient demographics, comorbidities, and preferences, as well as characteristics of the infection. Yet while the majority of hand surgeons have faced the clinical dilemma of digit preservation versus amputation, little is known about what factors affect this decision. Current literature examining the outcomes of diabetic digital infection is generally limited to small case series or cohort studies.5,6,13-17 The aim of this study is to examine how patient history and other clinical factors predict the outcome of digit preservation versus amputation after diabetic hand infection. We hypothesized that older patients with higher degrees of comorbidity, as well as patients with delayed presentation and osteomyelitis would be more likely to undergo amputation compared with preservation.
Materials and Methods
Patients
After receiving approval from the Washington University School of Medicine institutional review board, CPT and ICD-9/10 databases were queried to identify patients with diabetes mellitus who underwent incision and drainage, debridement, arthrotomy, or amputation for treatment of a hand infection between December 2010 and December 2020. Inclusion in this retrospective cohort study required a diagnosis of type 1 or 2 diabetes mellitus, upper extremity infection clearly involving at least 1 digit, and surgical management of the infection in the operating room by a hand surgeon. Both inpatient and outpatient cases were included. Given our interest in examining factors associated with digit preservation or amputation, we excluded 7 patients with a history of dry gangrene that was non-viable even prior to the development of an infection. Furthermore, patients with upper extremity infections that did not critically involve a digit were also excluded. This was determined by documented involvement of the anatomic structures of a digit based on detailed review of the operative notes and radiographs by a single reviewer (E.G.). The senior author (M.A.P.) reviewed the relevant records if there was any ambiguity. A diagram of enrollment flow is shown in Figure 3.
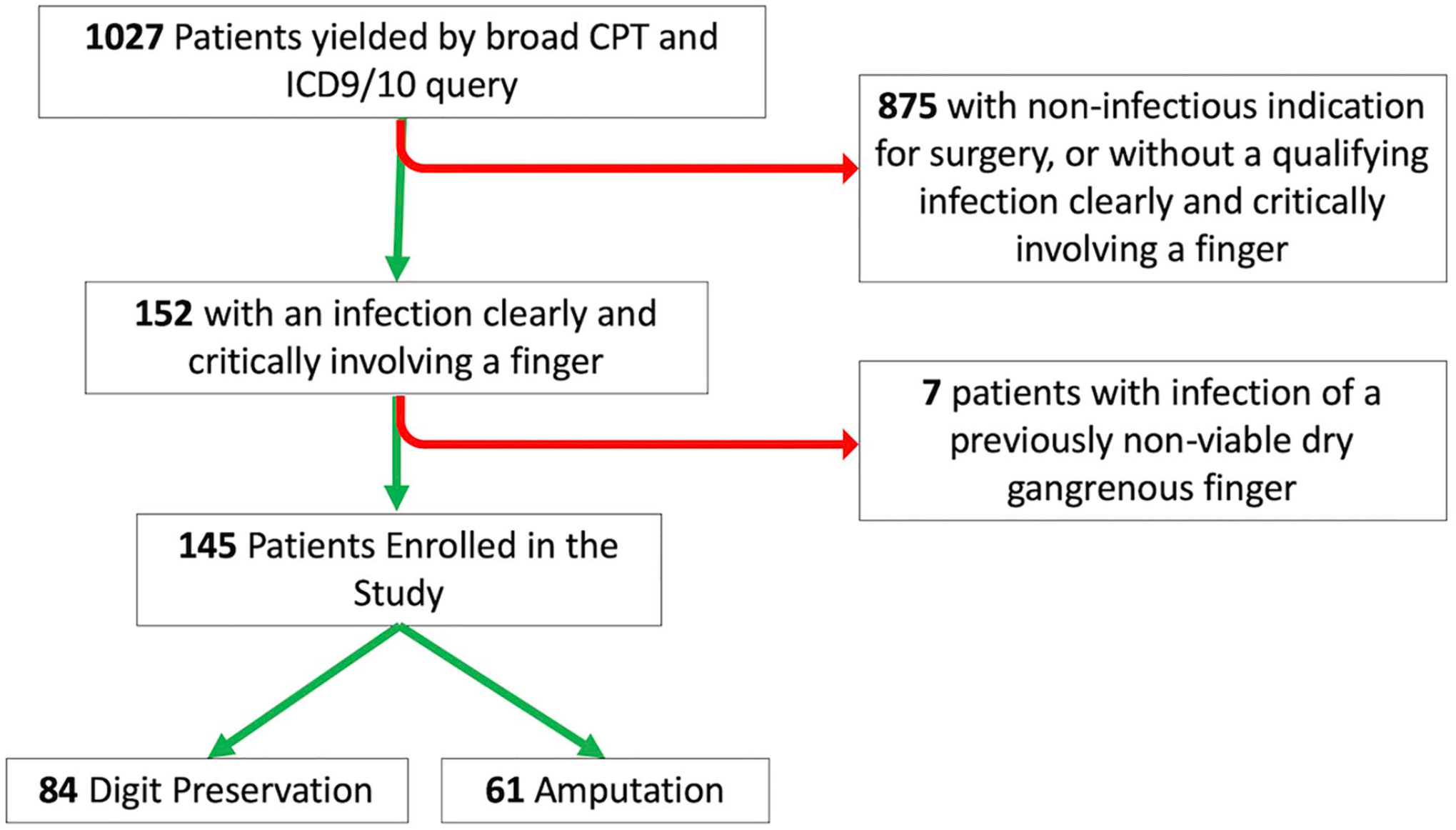
Patient enrollment flow diagram.
Electronic medical records were reviewed for patient demographics, comorbidities, laboratory values, type and etiology of infection, pathogenic organisms, duration of infection prior to presentation, surgical treatment, and clinical course. Body mass index (BMI) calculations were omitted for patients with a previous major extremity amputation, and creatinine was omitted for patients on dialysis. Type of hand infection was classified as a felon, paronychia, osteomyelitis, pyarthrosis, superficial abscess, deep space abscess, or necrotizing soft tissue infection. Deep space abscess was defined as involvement of the thenar, hypothenar, midpalmar, dorsal subaponeurotic, or Parona’s space as documented in the operative report. The comorbidity of vascular disease was defined by the documented history of cerebrovascular accident, myocardial infarction, or peripheral arterial disease. End-stage renal disease (ESRD) was defined by the patient being on dialysis at the time of the infection.
Home address was used to determine area deprivation index (ADI), a measure of socioeconomic status in which higher scores represent greater social deprivation. 18 If a patient underwent multiple episodes of treatment for multiple distinct and unrelated hand infections, only the first episode was included.
Statistical Analysis
Explanatory variables were treated as dichotomous, interval, or continuous. Bivariate relationships between all explanatory variables and the primary outcome (preservation vs amputation) were assessed using linear regression. Explanatory variables with bivariate P values ≤.05 were entered into the multivariable analysis. Multivariable analysis was achieved using stepwise regression with pairwise exclusion. Proportions were compared using a χ2 test. Statistical significance was defined as P < .05.
Power Analysis and Sample Size Calculation
Conservative a priori power calculation revealed that to obtain 80% power for detection of a moderate effect size (f2 = 0.15) in a multivariable model with up to 10 entrant explanatory variables, a minimum sample of 118 patients would be required.19,20
Results
In total, 145 diabetic patients with digital infections met inclusion criteria. A description of the study population at large, including demographic factors, comorbidities, clinical status upon presentation, microbiology, and clinical course, is presented in Table 1. Of the145 patients, 84 (58%) underwent digit preservation, whereas 61 (42%) were treated with amputation. Among the patients who required amputation, 46 (75.4%) required amputation proximal to the level of the proximal interphalangeal (PIP) joint, and 9 (14.7%) required amputation of more than 1 digit.
Description of Enrolled Population, Including Demographic Information, Comorbid Medical Conditions, Clinical Status on Presentation, Microbiology Results, and Clinical Course.
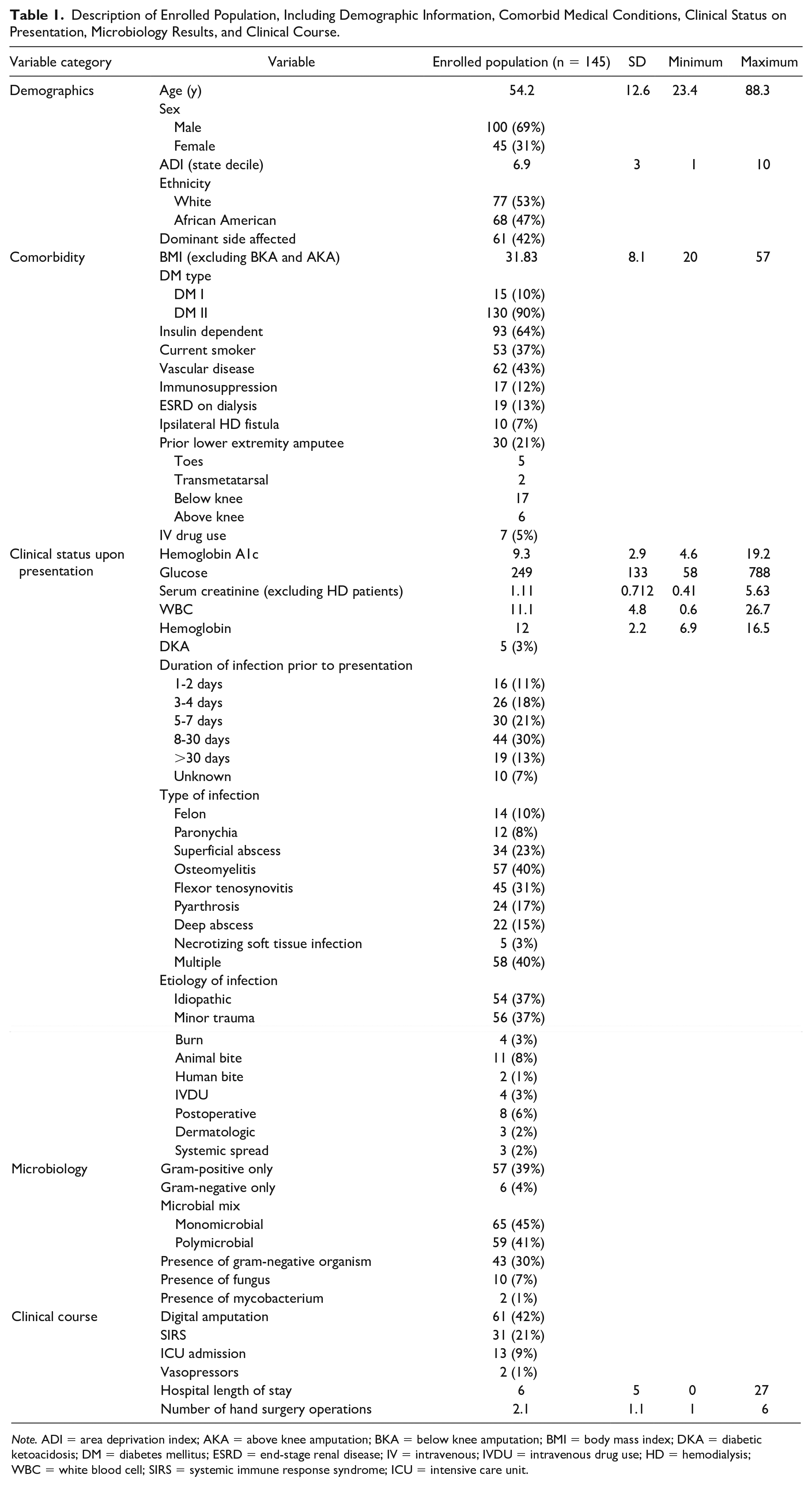
Note. ADI = area deprivation index; AKA = above knee amputation; BKA = below knee amputation; BMI = body mass index; DKA = diabetic ketoacidosis; DM = diabetes mellitus; ESRD = end-stage renal disease; IV = intravenous; IVDU = intravenous drug use; HD = hemodialysis;WBC = white blood cell; SIRS = systemic immune response syndrome; ICU = intensive care unit.
Twenty-one percent of patients presented with evidence of systemic immune response syndrome (SIRS) and 9% required ICU admission. Mean hospital length of stay was 6 days (range = 0-27 days) and patients underwent an average of 2 operations (range = 1-6). None of the patients died during hospitalization; however, 2 patients (3.2%) in the amputee cohort were discharged to hospice. Confirmed mortality within 5 years of infection in the amputee cohort was significantly higher (18%, 11/61 patients) than the digit preservation group (5%, 4/84 patients) (P = .01).
Bivariate analysis of historical variables revealed that high ADI, vascular disease, ESRD, prior lower extremity amputation, the presence of an ipsilateral dialysis fistula, low hemoglobin concentration, duration of infection greater than 1 week, the presence of osteomyelitis, polymicrobial infection, and infection with a gram-negative organism predicted amputation rather than digit salvage (Table 2). Stepwise multivariable regression analysis using these 10 entrant explanatory variables demonstrated that only the presence of osteomyelitis, presence of an ipsilateral upper extremity fistula, comorbid vascular disease, and ESRD were independently associated with the outcome of amputation (model R2 = 0.43, Table 3).
Bivariate Analysis of Historical and Acute Clinical Variables Associated With Increased Risk of Amputation in Patients With Diabetes Who Present With Surgically Treated Finger Infections.
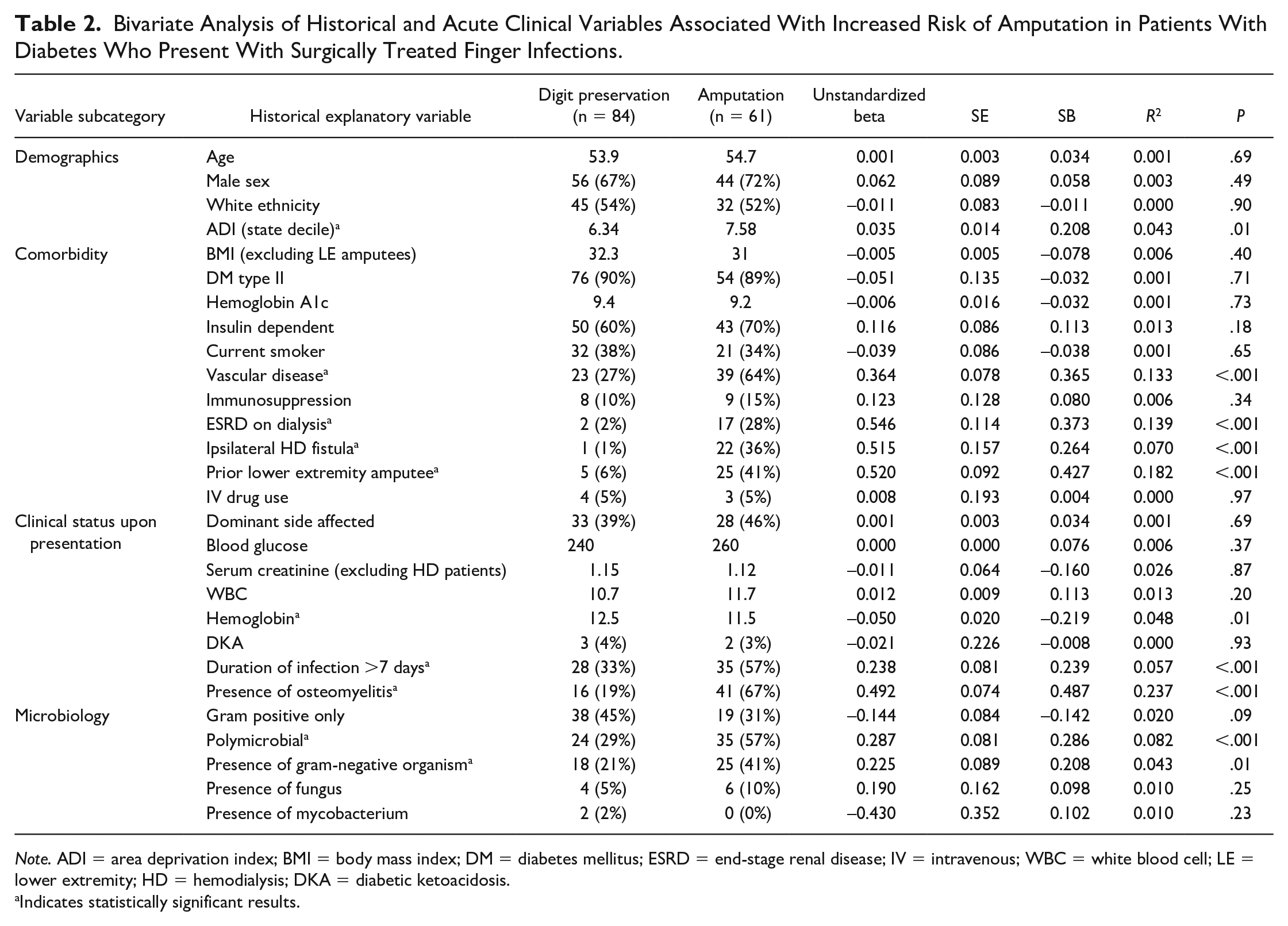
Note. ADI = area deprivation index; BMI = body mass index; DM = diabetes mellitus; ESRD = end-stage renal disease; IV = intravenous; WBC = white blood cell; LE = lower extremity; HD = hemodialysis; DKA = diabetic ketoacidosis.
Indicates statistically significant results.
Multivariable Analysis Revealing Statistically Significant Historical and Acute Clinical Variables Associated With Increased Risk of Amputation in Patients With Diabetes Who Present With Surgically Treated Finger Infections.

Discussion
This retrospective cohort study analyzed historical and acute clinical factors as potential predictors of digital preservation versus amputation in the setting of diabetic hand infections. Amputation was common in this cohort and was the ultimate outcome for nearly half of the included population. Four clinical factors were found to have independent predictive value for the outcome of digital amputation rather than preservation, and this 4-factor model accounted for 43% of the variability observed.
The presence of osteomyelitis has been repeatedly shown to predict lower extremity amputations in patients with diabetic foot infections and was the strongest predictor of digital amputation in this study.21-23 While medical treatment of osteomyelitis is possible (16/41 patients with osteomyelitis in the series were treated without amputation), this often requires many weeks of intravenous antibiotics, which may be unfeasible or overly burdensome for the patient and/or health care system. Furthermore, medical treatment of osteomyelitis has a high risk for failure especially in patients with impaired immune systems and poor peripheral circulation.24-26 As such, this relationship between the presence of osteomyelitis and the outcome of the amputation is likely attributable to a recognition by patient and surgeon that amputation reflects a faster and more reliable route to clearance of infection. Of note, osteomyelitis was the only acute infectious characteristic that was predictive of outcome. Laboratory values, patient-reported duration of infection, and microbiology had no detectable impact.
The likely outcome of digital amputation in patients with ESRD may be explained by surgeons consciously or unconsciously harboring a lower threshold for amputation in this population due to perceived end-of-life status. In our experience, these patients are also more likely to present with advanced infections and systemic illness, and prompt amputation may be undertaken to achieve rapid and unequivocal source control. In addition, patients with ESRD are known to have impaired cellular immunity due to mechanisms of action that are independent of the pathophysiologic factors that increase risk of infection in diabetes.27-29
Presence of an ipsilateral upper extremity hemodialysis fistula was also associated with the outcome of digital amputation. Given that vascular access–related infections are one of the leading causes of morbidity and mortality in patients on long-term dialysis, this finding likely reflects appropriate conservatism on the part of surgeon and patient in situations where ascending infection during attempted digital salvage could threaten critical dialysis access (especially if this is composed of a synthetic graft). 30 Furthermore, given the high incidence of symptomatic and clinically occult vascular steal, these patients may be deemed less likely to successfully undergo digital preservation due to impaired distal perfusion. It should be noted that because both ESRD on dialysis and ipsilateral hemodialysis fistula were found to have independent relationships with the outcome of amputation, it can be inferred that while all dialysis patients are likely to be treated with amputation, patients with a hemodialysis fistula ipsilateral to the infection are even more likely to become amputees.
Finally, the impact of vascular disease can reasonably be attributed to impaired peripheral circulation, which may influence the surgeon to estimate a low likelihood of successful digital salvage, or cause failure of salvage attempts, which ultimately progress to amputation.
While digital infections in the general population are often treated as a nuisance, the findings of this study highlight that in the diabetic population these occurrences have permanent consequences for both the patient and the health care system at large. While an assessment of cost was beyond the scope of our study, it should be noted that caring for these 145 diabetic hand infections required over 300 operations and 870 days of inpatient hospitalization at a single institution. Further studies are necessary to understand how surgical management decisions (eg, decision to proceed with digital amputation vs salvage, whether to perform amputation and closure in 1 or 2 stages, as well as the decision to admit the patient postoperatively) affect both patient outcomes and health care costs.
In this study, mortality in the 5 years following infection was found to be higher in the group treated with amputation rather than digital salvage. This finding is unsurprising, as digital amputation seems to be the preferred modality of treatment in patients with negative prognostic indicators such as vascular disease or ESRD. This secondary finding of our study is consistent with a recent report by Stone et al 31 demonstrating that patients with ESRD undergoing upper extremity amputation have a 5-year survival rate half that of patients with ESRD who do not require similar operations. While it is unlikely that upper extremity amputation truly represents a unique risk factor for mortality, physicians treating diabetics with amputation-requiring hand infections need to be aware that this might represent near end-of-life care.
The primary limitation of this study is its retrospective nature. Therefore, we are only able to determine whether preservation/amputation was performed, and we are unable to analyze the decision-making process that led to this outcome. As a result, we have likely included some patients who had no feasible option other than amputation, in addition to patients who might have reasonably undergone either treatment. Further prospective mixed-methodology observational studies would facilitate greater understanding of how surgeons and patients process data and clinical information to arrive at a decision about amputation versus digit salvage.
In addition, the premise of this study assumes that digital amputation represents a negative outcome for the patient, but this point is not directly studied and we do not believe this is true in all cases. To address this issue, a related patient-reported outcome study is already underway. Given that the outcome of mortality was detected only by review of the patient’s chart, and because 5 years since infection had not elapsed for some patients, we have necessarily underestimated the true rate of mortality in both the cohorts. While a more thorough analysis using data from the national death index would improve our estimate, it is unlikely that the elevated mortality risk observed in the amputee cohort would be proven artefactual.
Conclusions
All diabetic patients should be encouraged to regularly check their hands and nails for early signs of infection, and avoid finger-stick blood glucose measurement in limbs with dialysis access. Minor hand trauma in this population should be taken seriously and cared for meticulously. Surgical care of hand infections in this population represents a substantial expenditure of resources within the health care system. Once surgical treatment is indicated for digital infection in patients with diabetes, nearly half of patients will go on to digital amputation. The presence of osteomyelitis, ipsilateral upper extremity dialysis fistula, vascular occlusive disease, and ESRD are each independently predictive of digital amputation in these scenarios. Further studies should focus on clinical factors affecting surgical decision making and how the treatment rendered affects patient outcomes.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with animal or human subjects.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I.K.F. has received funds from the Department of Defense for separate, unrelated research projects. M.A.P. has received funds from Silk Biomaterials, 3M, and Checkpoint, Inc, for separate, unrelated research projects.