
Abstract
Joint denervation has been proposed as a less invasive option for surgical management of hand arthritis that preserves joint anatomy while treating pain and decreasing postoperative recovery times. The purpose of this systematic review was to investigate the efficacy and safety of surgical joint denervation for osteoarthritis in the joints of the hand. EMBASE, MEDLINE, and PubMed databases were searched from January 2000 to March 2019. Studies of adult patients with rheumatoid arthritis or osteoarthritis of the hand who underwent joint denervation surgery were included. Two reviewers performed the screening process, data abstraction, and risk of bias assessment (Methodological Index for Non-Randomized Studies). This review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and was registered with PROSPERO (#125811). Ten studies were included, 9 case series and 1 cohort study, with a total of 192 patients. In all studies, joint denervation improved pain and hand function at follow-up (M = 36.8 months, range = 3-90 months). Pooled analysis of 3 studies on the first carpometacarpal joint showed a statistically significant (P < .001) reduction in pain scores from baseline (M = 6.61 ± 2.03) to postoperatively (M = 1.69 ± 1.27). The combined complication rate was 18.8% (n = 36 of 192), with neuropathic pain or unintended sensory loss (8.8%, n = 17 of 192) being the most common. This review suggests that denervation may be an effective and low-morbidity procedure for treating arthritis of the hand. Prospective, comparative studies are required to further understand the outcomes of denervation compared with traditional surgical interventions.
Keywords
Introduction
Osteoarthritis (OA) of the hands is a degenerative condition that relies on surgical intervention when medical management fails to control symptoms and improve function. Traditional surgical options include arthroplasty, arthrodesis, and osteotomy. However, each of these options possesses inherent limitations, which include risk of significant complications, decreased range of motion, need for revision surgery, and prolonged recovery time. 1 In addition, there remains clinical equipoise regarding the ideal surgical treatment for OA in the small joints of hands. 2 In practice, trapeziectomy with ligament reconstruction and tendon interposition (LRTI) is largely considered the standard treatment for arthritis of the first carpometacarpal (CMC) joint. However, there is continued debate regarding the outcomes and morbidity of the LRTI component in comparison with trapeziectomy alone and the multitude of other surgical options.2-4 For the other small digits of the hands, there is no consensus on the criterion standard.5,6 Often, arthroplasty and arthrodesis are chosen for the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints. Despite continued advancement in technology, arthroplasty is associated with high complication rates, whereas arthrodesis is often reserved as the final option due to the loss in range of motion of the affected joint.7-9 In the context of these modern surgical limitations, joint denervation has been proposed as an alternative surgical option for the management of OA in the hands.
The proposed benefits of joint denervation are straightforward. By performing neurectomies of the articular sensory branches to the osteoarthritic joint, patients will theoretically experience an alleviation in pain, which may translate to preserved or increased hand function. Denervation can be accomplished with limited dissection and disruption to the articular structure. It is a short procedure, with a brief recovery period and decreased need for rehabilitation in comparison with current surgical options. In addition, with the preservation of the bony anatomy, it is postulated that patients would still be candidates for any further surgical interventions.
Denervation has only in the recent years gained attention as a treatment option for bony pain. It has been used as a treatment for wrist arthritis and chronic bony pain with promising results. Literature on these cases reports decreased pain and maintained function of the joint in question, in addition to a minimal complication profile.10-12 It is expected then that denervation of the small joints of the hand for OA may also yield promising results. There are currently studies describing various denervation techniques, but to date there have been no reviews of the current literature to synthesize the current evidence on the outcomes and complications of denervation as a treatment for OA in the hands. The purpose of this systematic review was to evaluate and report the efficacy and safety of surgical joint denervation as a treatment for OA in the joints of the hand.
Methods
Literature Search
A literature search was conducted from January 2000 to March 2019 in the EMBASE, MEDLINE, and PubMed databases. See Supplementary Table S1 for the search terms used. Additional clinical trial databases including the Cochrane Central Register of Controlled Trials, International Clinical Trials Registry Platform search portal (World Health Organization), and Clinicaltrials.gov were also searched. Reference lists of relevant articles were reviewed for additional citations.
Two reviewers (S.Z. and E.W) independently performed title, abstract, and full-text screening, as well as data abstraction. Studies involving adult patients (aged ≥18 years) with either rheumatoid arthritis or OA of the hand undergoing joint denervation surgery were included. Studies with nonhuman participants, joint denervation surgery indicated for a nonarthritic condition, or patients with concomitant hand injuries or surgery were excluded (see Supplementary Table S2). Any articles in which the title and abstract screening was unclear were conservatively included for full-text review. This systematic review was registered with PROSPERO with ID number 125811.
Outcomes
The study collected data on 3 outcomes: pain, function, and complications following surgery. Continuous outcomes could be measured by patient-reported outcome instruments or biomechanical measurements (eg, grip strength).
Assessment of Methodological Quality
The methodological quality and risk of bias of included studies were assessed independently by 2 reviewers (S.Z. and E.W.) using the Methodological Index for Non-Randomized Studies (MINORS). 5
Data Collection
A data collection form was designed a priori to extract relevant data from each included paper. Data collection was initially completed in duplicate by 2 reviewers (S.Z. and E.W) and combined. Inconsistencies were reviewed and resolved through discussion. Data collection included author, journal, publication year, study design, sample size, type of arthritis, location of arthritis, nerves resected, outcome measures, length of follow-up, and complications. In this review, complications were defined as any outcome that was deemed an adverse event by study authors of the primary study.
Data Analysis
Quantitative statistical analysis included pooling the means and variance of the patient population characteristics and outcome measures. A paired t test comparing preoperative and postoperative scores for applicable outcome measures (2-sided test, α = 0.05) was performed. Where aggregate quantitative analysis was not possible, study results are described qualitatively.
Results
Characteristics of the Included Studies
Ten studies met the inclusion criteria and were included for analysis.13-22 The screening process is highlighted in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart (Figure 1). The design of the included studies was predominantly case series (n = 8), but also included a retrospective cohort study (n = 1) and a prospective cohort study (n = 1) (Table 1).
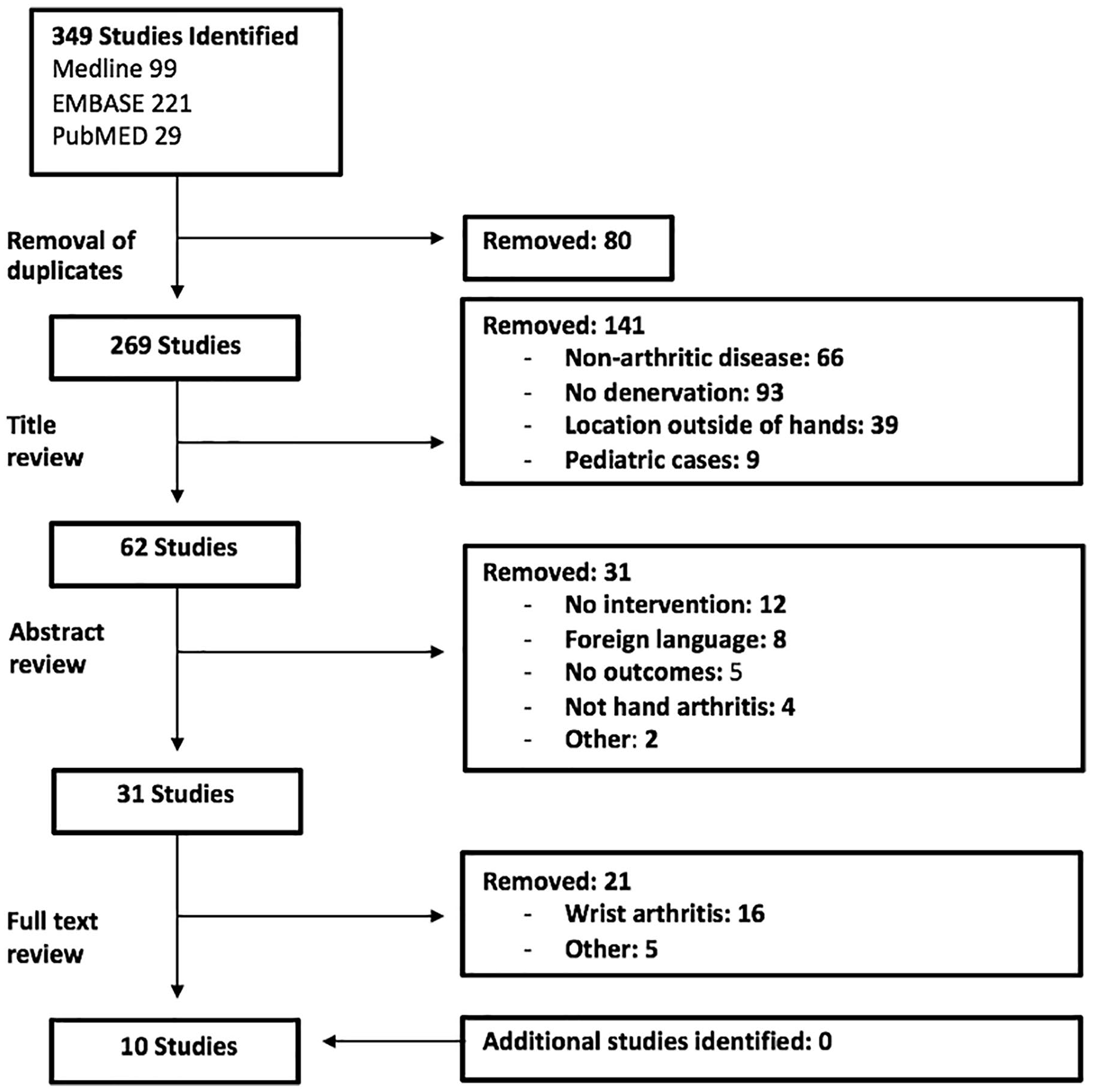
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of the screening process.
Overview of the Selected Studies.
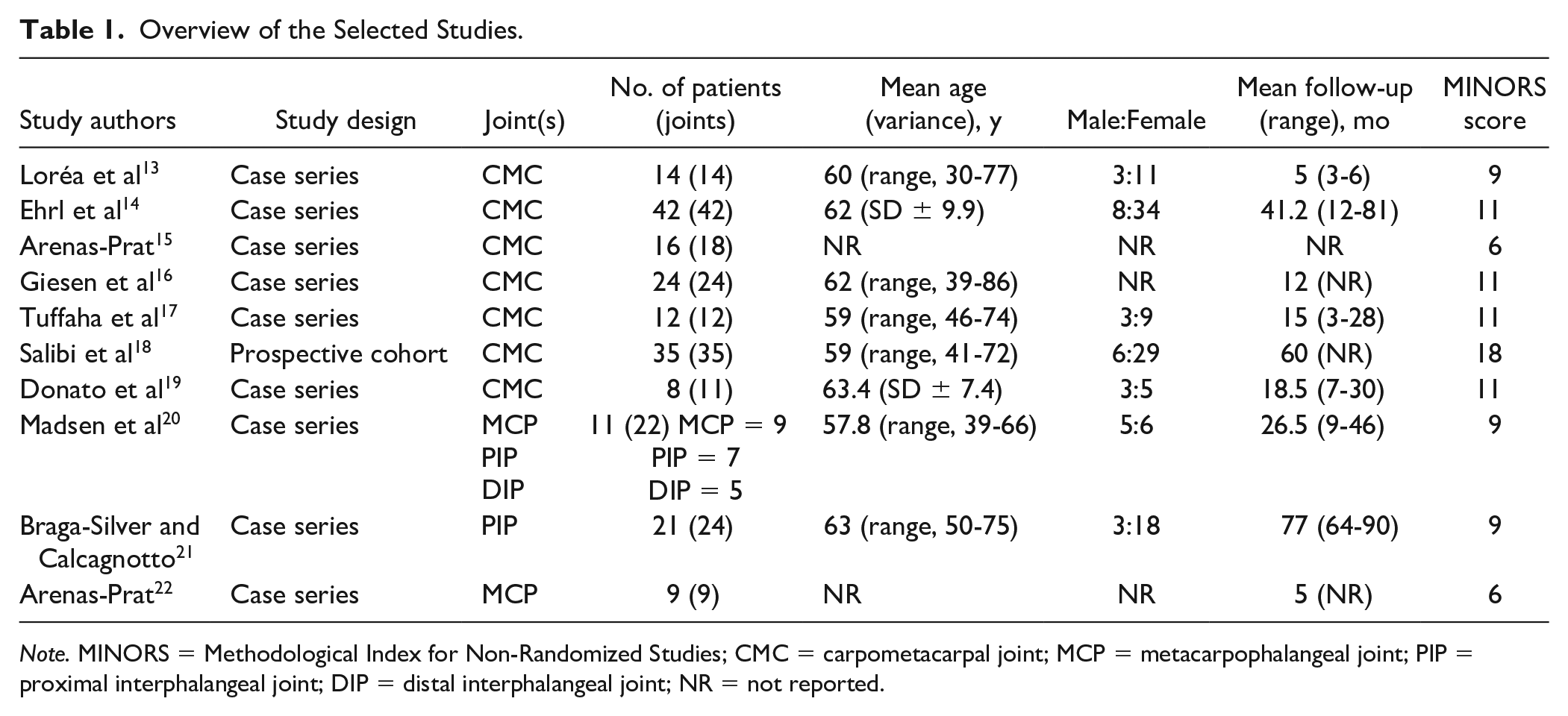
Note. MINORS = Methodological Index for Non-Randomized Studies; CMC = carpometacarpal joint; MCP = metacarpophalangeal joint; PIP = proximal interphalangeal joint; DIP = distal interphalangeal joint; NR = not reported.
There was a total of 211 joint denervation procedures in 192 patients. All included patients were diagnosed with OA. The Eaton criteria were used for OA staging in 2 studies, which included patients with stage 2 (n = 20), stage 3 (n = 20), and stage 4 (n = 4) OA.14,17 Giesen et al 16 used the Dell classification, including patients with stage 1 (n = 2), stage 2 (n = 3), stage 3 (n = 10), and stage 4 (n = 16) OA. Patient characteristics and follow-up times are listed in Table 1. Sample-weighted mean age, from the 8 articles that reported mean ages, was 60.9 years (range, 57.8-63.4 years). All but 1 study reported a mean follow-up, with a sample-weighted mean follow-up of 36.8 months (range, 3-77 months).
Operative Technique
All included articles described their surgical technique (Table 2). Seven the 10 included articles described denervation for the first CMC joint, whereas the remaining 3 articles described denervation for the MCP, PIP, and DIP joints.
Description of Operative Technique.
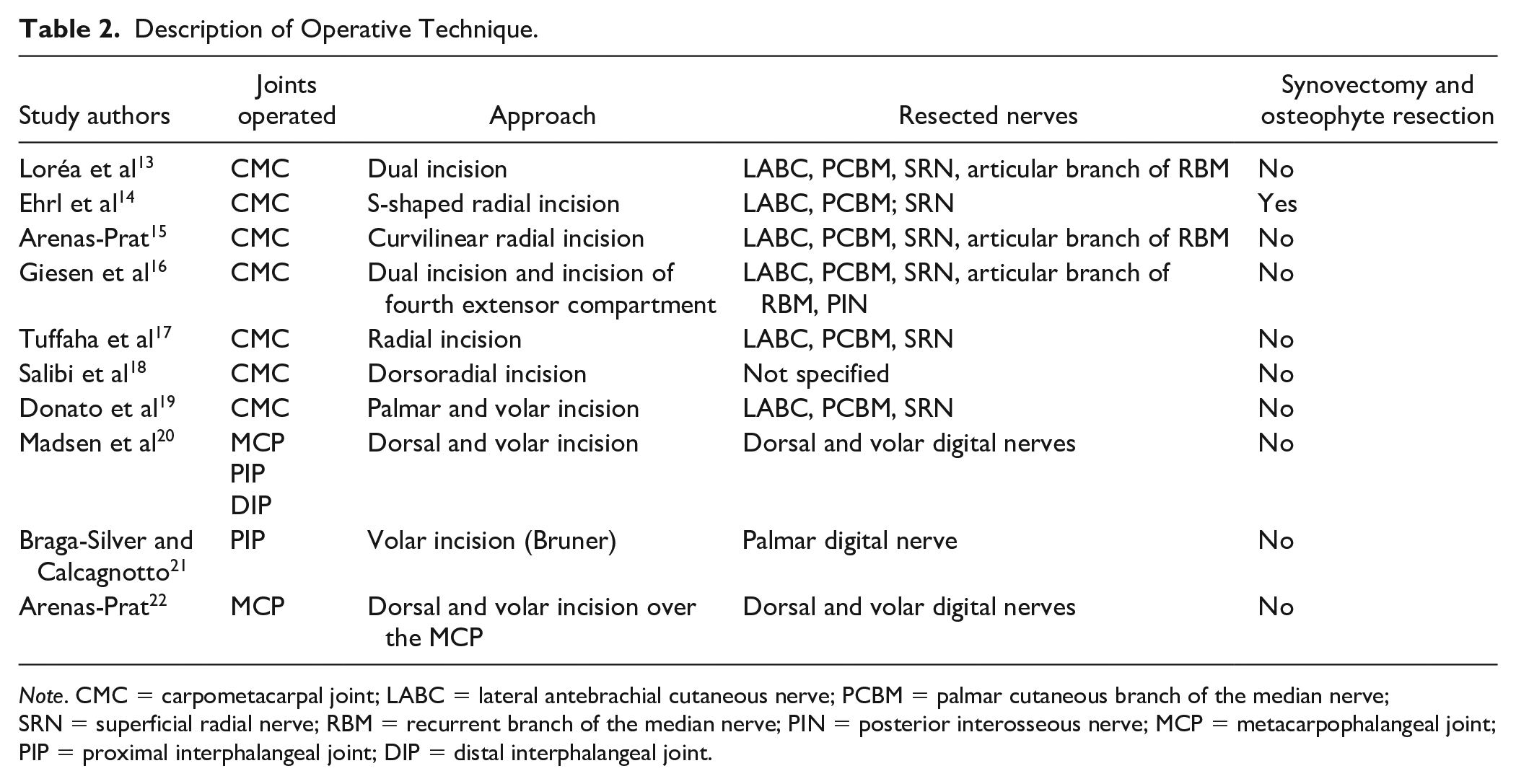
Note. CMC = carpometacarpal joint; LABC = lateral antebrachial cutaneous nerve; PCBM = palmar cutaneous branch of the median nerve; SRN = superficial radial nerve; RBM = recurrent branch of the median nerve; PIN = posterior interosseous nerve; MCP = metacarpophalangeal joint; PIP = proximal interphalangeal joint; DIP = distal interphalangeal joint.
The approach for the first CMC joint varied from a single dorsoradial incision to 2 incisions placed in various positions (Table 2). The study by Ehrl et al 14 was the only one that included a synovectomy and osteophyte resection in its procedure. All other studies did not enter the joint capsule. Regarding the nerves selected for denervation, the procedures were comparable. All 7 included studies consistently targeted the lateral antebrachial cutaneous nerve, palmar cutaneous branch of the median nerve, and the superficial radial nerve. In addition to those 3 branches, Lorea, Giesen and Arenas-Prat also resected the articular branches extending from the recurrent branch of the median nerve.23,24 The study by Giesen et al 16 was the only one resecting the posterior interosseous nerve (PIN) in the fourth extensor compartment just proximal to the wrist to prevent potential reinnervation of the first CMC joint.
Of the articles describing denervation of phalangeal joints, 2 described denervation of the MCP and PIP joints, and 1 described denervation of the DIP joint. Both volar and dorsal incision were used for denervation of the MCP to achieve resection of the palmar and dorsal branches of the digital nerves. For the PIP joint, Braga-Silver and Calcagnotto 21 described a single volar incision over the PIP joint to ablate volar digital nerve branches that contributed to the PIP joint. In contrast, Madsen et al 20 described ablation of both volar and dorsal digital nerve branches to the PIP joint. Only 1 article described denervation of the DIP, and a single dorsal incision was used to resect dorsal and volar digital nerve contributions to the joint. All 3 studies preserved the joint capsule.
Outcomes
Outcomes of denervation were reported to different degrees and using different methods. Six studies reported changes in pain using a patient-rated scale created by the paper’s authors, the Visual Analogue Scale (VAS; 0-10 cm), the Numerical Rating Scale (NRS; 0-10 points), and other validated scoring tools such as the Cooney and Krimmer scoring system.25,26 The remaining 4 studies did not measure pain changes. In all studies where pain was recorded, there was a decrease in pain postoperatively (Table 3).
Baseline and Postoperative Pain Scores.
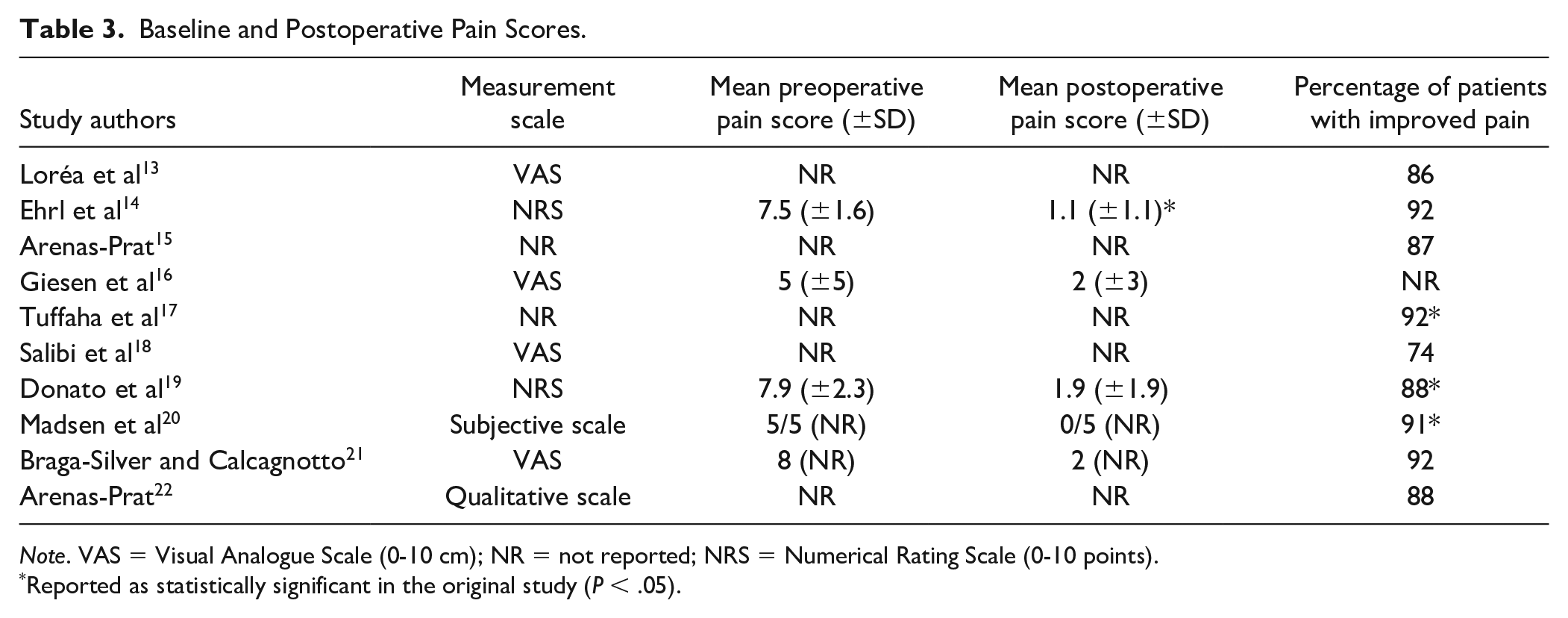
Note. VAS = Visual Analogue Scale (0-10 cm); NR = not reported; NRS = Numerical Rating Scale (0-10 points).
Reported as statistically significant in the original study (P < .05).
Three studies reported changes in pain following denervation of the CMC joint using the VAS or NRS score.14,16,19 The baseline pain scores and postoperative pain scores from these studies were pooled and analyzed using a 2-sided paired t test (α = 0.05).14,16,19 This group had a combined sample size of 80 patients (61 women and 19 men) and 84 thumbs with a mean age (±SD) of 62.53 ± 2.03 years. The average follow-up time within this cohort was 12 months after surgery (range, 7-82 months). Paired t test analysis revealed a statistically significant reduction in postoperative pain (P < .001), from a mean preoperative pain score of 6.61 ± 2.03 to a mean postoperative VAS score of 1.69 ± 1.27 (Figure 2).
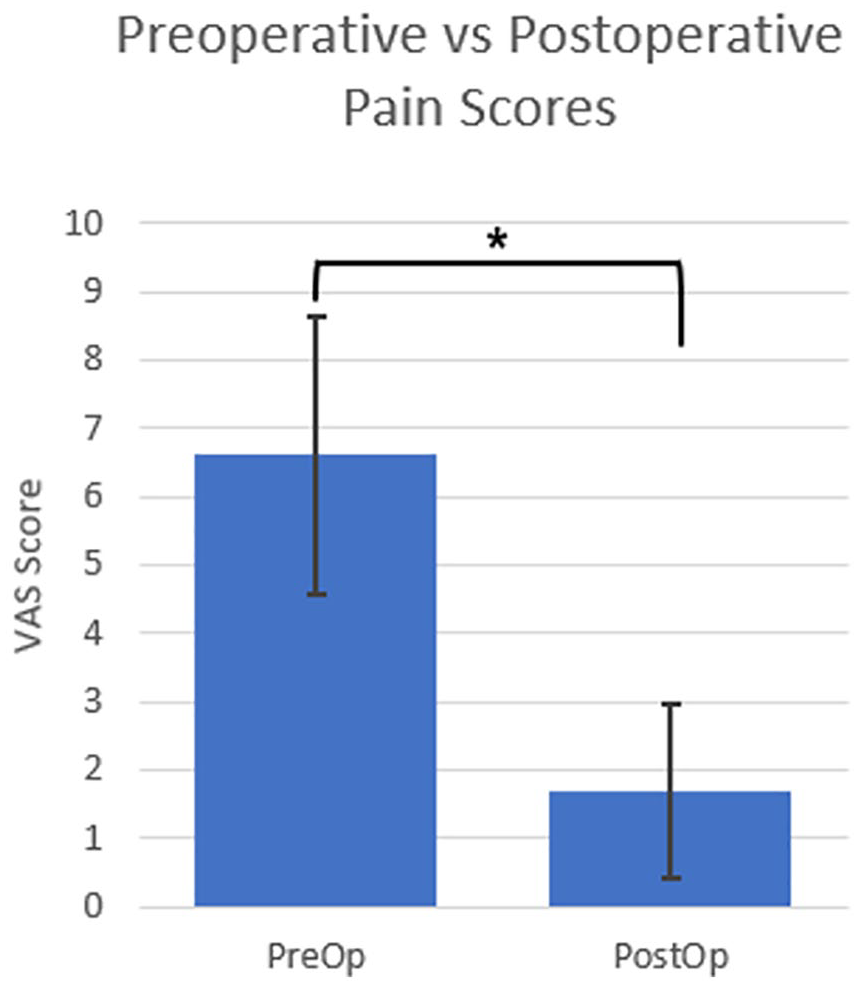
Paired t test analysis of change in pain for denervation of the first carpometacarpal joint.
Changes in patient function were measured using various tools. The study by Madsen et al 20 was the only one where a nonvalidated NRS (0-5 points) was used to measure function, which reported a mean increase in postoperative function. A number of validated measures of function were used in the remaining included studies. These included the Jamar dynameter for grip strength, Preston pinch gauge, Kapandji opposition scale, the Disabilities of the Arm, Shoulder, and Hand (DASH) score, and the Krimmer wrist score. All included studies showed an improvement in average scores for function postoperatively (Table 4).
Baseline and Postoperative Measures of Function.
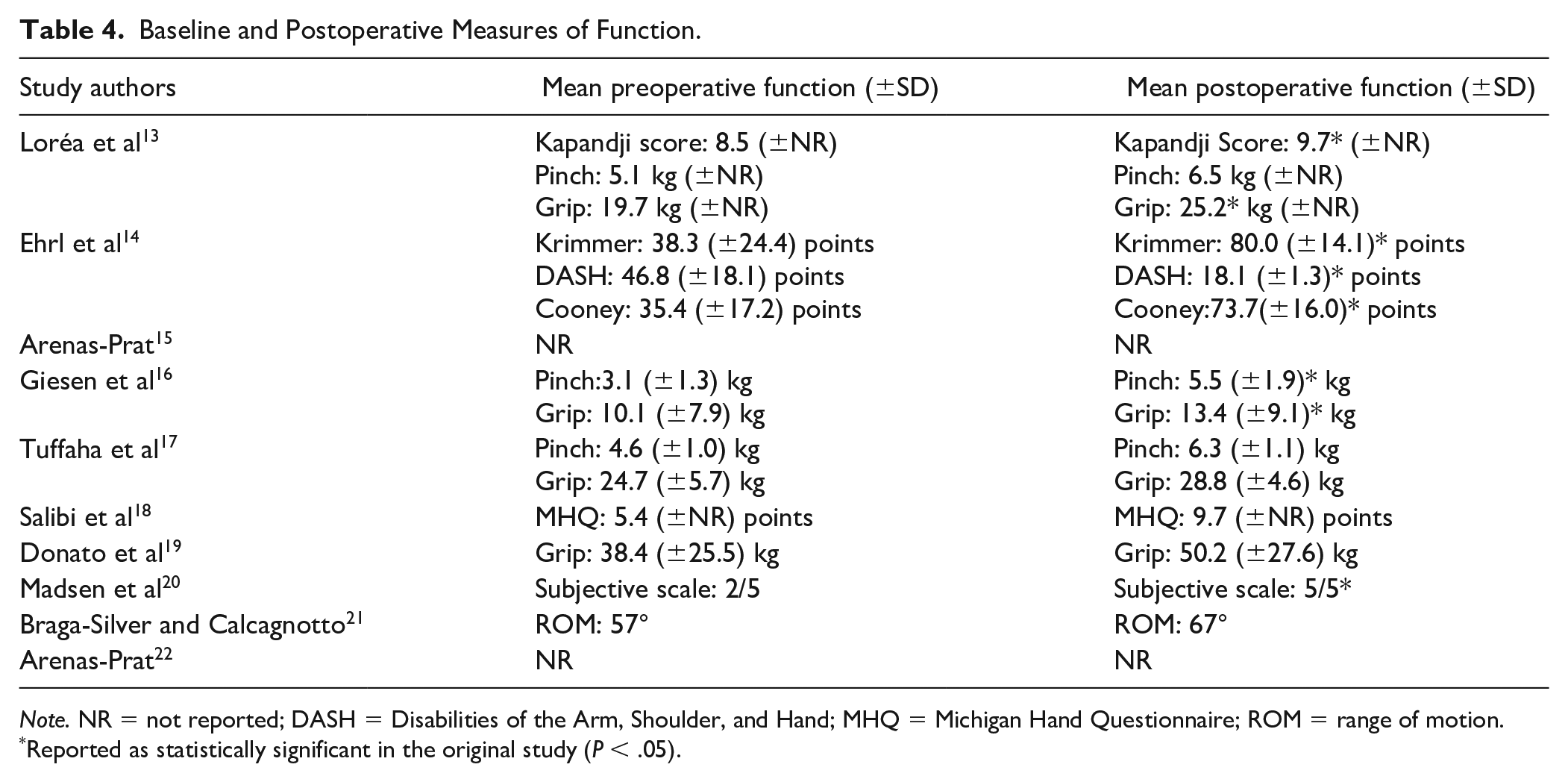
Note. NR = not reported; DASH = Disabilities of the Arm, Shoulder, and Hand; MHQ = Michigan Hand Questionnaire; ROM = range of motion.
Reported as statistically significant in the original study (P < .05).
Complications
The reported complication rates ranged from 0% to 72.7%, with a pooled complication rate of 18.8%. The complication rate for CMC joint denervation was 15.9% (n = 23 of 145), which was lower than the complication rate of 27.1% (n = 13 of 48) for MCP, PIP, or DIP joint denervation (Tables 5 and 6). Overall, the most commonly reported complications were neuropathic pain and unintended sensory loss. Within this complication group, all patients reported complete return of sensation, or it was reported as functionally insignificant by the patient. Treatment failure, defined as persistent symptoms of pain, was the second highest reported complication, affecting 11 (5.7%) of 192 patients.
Reported Complications in CMC Joint Denervation.
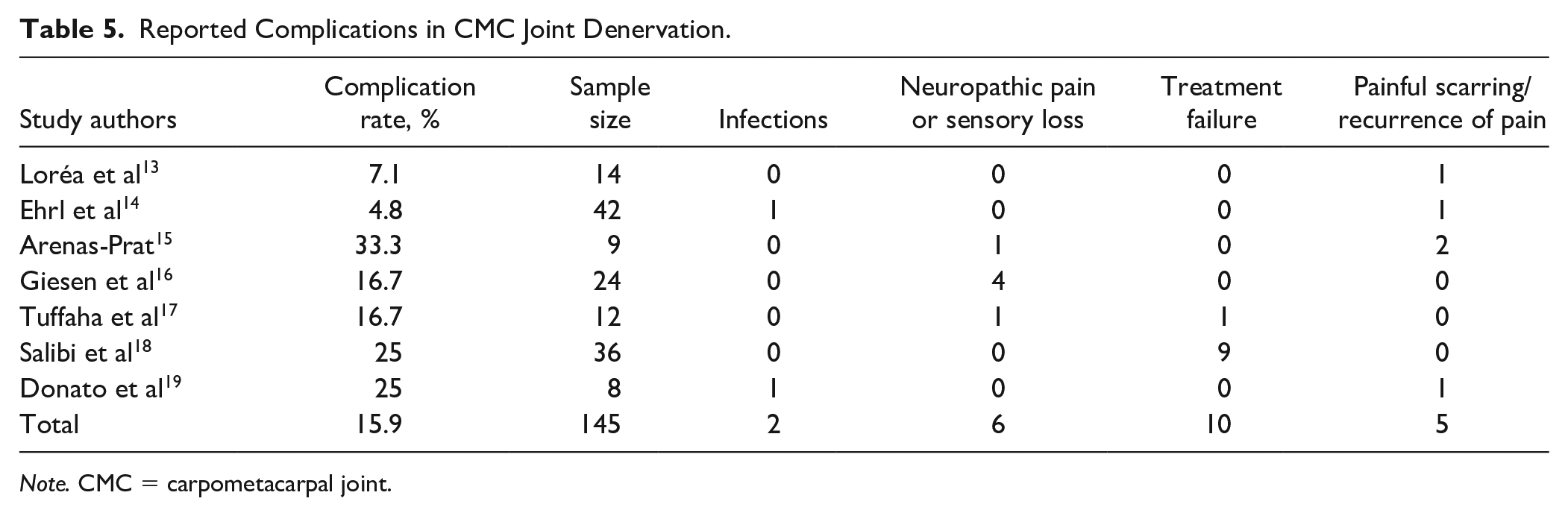
Note. CMC = carpometacarpal joint.
Reported Complications in MCP, PIP, and DIP Joint Denervation.
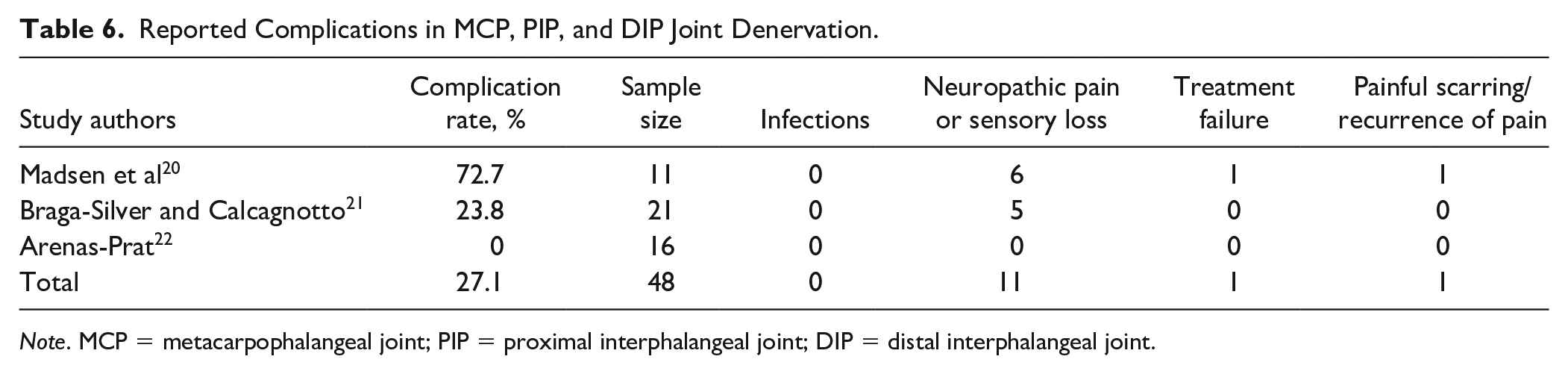
Note. MCP = metacarpophalangeal joint; PIP = proximal interphalangeal joint; DIP = distal interphalangeal joint.
Less commonly reported complications included recurrence of pain symptoms (3.1%) and infection (1.0%). There was 1 patient reported to have experienced complex reginal pain syndrome (CRPS) postoperatively. 14
Risk of Bias
See Table 1 for the averaged total MINORS score of each study. Of the noncomparative studies (n = 9), the MINORS score ranged from 6 to 11 out of 16, with a mean of 9.2. As the study by Salibi et al 18 was a comparative one, it was assessed with additional criteria and was scored 18 of 24. Also see Supplementary Table S3 for the raw scoring of the studies by both raters for each MINORS criteria.
Discussion
Denervation is a relatively novel procedure, proposed as an alternative to the more established surgical techniques in treating hand OA. The proposed benefits of denervation include a less invasive and shorter surgery while preserving bony anatomy and providing pain relief and increased function. There have been a number of studies reporting the technique and the efficacy of denervation for this population, although there is no consolidation of the existing knowledge on this subject. This article aimed to collect and review the current evidence for outcomes of denervation as a treatment for hand OA in terms of pain, function, and complications. The results of this article suggest significant pain alleviation and, at minimum, preserved joint function resultant from joint denervation for hand OA.
The current standard surgical intervention for thumb CMC arthritis is considered to be trapeziectomy with LRTI.5,6 In investigating pain alleviation, a recent study with 2-year follow-up of trapeziectomy with LRTI for CMC arthritis reported a statistically significant VAS decrease of 5.4 points (P < .05) from 6.8 to 1.4. 4 The results for denervation were comparable based on 3 first CMC denervation studies, demonstrating a decrease in VAS score of 4.92 points (P < .05) from a mean preoperative score of 6.63 ± 2.03 and a postoperative score of 1.69 ± 1.27. In addition, the finding of decreased pain is consistently reported in all 10 included studies of both CMC joints and the MCP, PIP, and DIP joints among various measures of pain including the NRS. This finding is also congruent with the current literature regarding the efficacy of denervation of the PIN and anterior interosseous neurectomy in achieving pain relief for individuals with bony wrist pain.10-12 Although we could not perform aggregate statistical comparisons of denervation to other techniques, Salibi et al 18 compared denervation with trapeziectomy in a prospective cohort study. This study reported no significant difference in VAS scores between denervation and trapeziectomy, for up to 5 years postoperatively. In addition, they reported no significant functional difference between the 2 groups using the Michigan Hand Questionnaire. 18 Based on the limited evidence presented in this review, denervation may offer pain relief that is comparable with trapeziectomy.
Given that the denervation procedure only targets sensory branches and does not change any structural features, any changes in function are likely secondary to improvements in pain. This is an idea proposed in Loréa et al. 13 Despite variant measures of function, all included studies reported functional improvements in their patient cohorts, which supports this theoretical framework.
For trapeziectomy, a recent study with 2-year follow-up reports a DASH score decrease of 30.6 (P < .001) to give a mean postoperative DASH score of 21.6. 4 Another paper investigating long-term results following a trapeziectomy found a mean postoperative DASH score of 27, whereas a more recent study of 50 patients reported a postoperative DASH score of 16.1,27 One study including 182 patients found a mean DASH score of 21.5 following a trapeziectomy with LRTI. 28 For denervation, the study by Ehrl et al was the only one that measured DASH scores. In their study with a sample of 42 patients undergoing denervation, there was a postoperative DASH score of 18 with a statistically significant decrease of 29 points. The DASH outcomes appear to be comparable, although the sample size for denervation is smaller than the trapeziectomy group. There is a corroborated minimum clinically important difference of 10.83 reported for the DASH scale. 27 This suggests that the change in function in the study by Ehrl et al and the trapeziectomy studies was not only statistically different but also clinically important.
A strong advantage of denervation, which has been proposed and confirmed in this review, is its mild complication profile. The 10 included articles in this review represent the majority of, if not all, current studies reporting denervation for the small joints in the hand as a treatment for OA. A proposed concern with joint denervation included the possible development of Charcot joint. Fortunately, this complication was not reported in any of the included studies in this review. This could be secondary to the follow-up time and the lack of proprioception testing in the included reviews. However, it is encouraging that at the time of this review neuropathic arthropathy has also not been reported following wrist denervation, which has been used and studied relatively more extensively than hand joint denervation. 29 With the exception of 1 patient who developed CRPS, all other reported complications were mild. Of the 18.8% (n = 36) of patients who experienced complications, 47.2% (n = 17 of 36) reported neuropathic pain or sensory loss, which included scar tenderness and peri-incisional numbness. These complications either completely resolved or were reported to have negligible impact on quality of life and function by the patient. In fact, in the study by Madsen et al, 20 patients who experienced sensory loss postoperatively responded that they would choose to undergo denervation again. The remaining complications included treatment failure and infection. One of the 2 reported infections was documented to have resolved without antibiotic therapy. There were 11 reported patients (6% of n = 192) who experienced treatment failure, defined as no change in symptoms postoperatively. However, 9 of those patients were from a single study. 18 Interestingly, all patients who reported treatment failure and underwent subsequent intervention with more traditional procedures such as LRTI experienced satisfactory resolution of their pain.18,20,25 This suggests that even if denervation fails, it does not affect the outcomes of patients or preclude patients from further surgical interventions. Further subgroup analysis is required to determine patient features prognostic for treatment failure.
The mild complication profile of denervation is critical given the main drawbacks of currently dominant options for hand OA, namely, invasiveness and complication profile. For example, in the PIP and DIP joints, the most commonly used surgical interventions are arthroplasty and arthrodesis. Both these procedures have significant reported complications, including implant failure, osteolysis, reoperation, infection, malunion and nonunion.30,31 In fact, for arthroplasty in the PIP joint, complications have been reported to be as high as 42.9%. 32 Arthrodesis is generally reserved as a salvage procedure due to the loss in range of motion. Although high union rates have been reported, ranging from 95% to 98%, there have also been reports of high morbidity complications.8,30,33 These include osteomyelitis, hardware exposure, skin necrosis, fracture, and complications leading to amputation.8,30,33
The main limitation of this review is the limited number of studies in the current literature regarding the use of denervation as an operative treatment for arthritis. This leads to a relatively small sample size within our review. In addition, most of the included articles were case reports and case series. There was limited direct comparison to existing treatments, with 1 comparative study included in this review comparing denervation with trapeziectomy. 18 Due to the small number of articles and the heterogeneity of the data, quantitative statistical analysis was limited. We were able to combine data for 3 studies which investigated denervation of the CMC joint, which demonstrated a statistically significant reduction in pain scores following denervation.4,5,8 We, however, cannot make any definitive conclusions on how it compares with established treatments such as trapeziectomy or arthrodesis. Future studies with direct comparison of treatments with consistent measurement tools for patient-reported outcomes such as pain and function will allow for a more robust evaluation of the efficacy of denervation surgery for OA of the hand.
Conclusion
Despite some limitations, the findings of this review suggest that denervation may be an effective and low-morbidity procedure for the treatment of OA in the small joints of the hand. Denervation may serve as a useful tool in the hand surgeon’s armamentarium, particularly for patients who have failed nonoperative management but wish to pursue less invasive management than traditionally described techniques or for patients who are functionally limited by pain as opposed to bony changes. Further prospective comparative studies are required to develop a more comprehensive understanding of the outcomes of denervation, particularly how it compares with the more conventional procedures of trapeziectomy, arthroplasty, and arthrodesis.
Supplemental Material
sj-pdf-1-han-10.1177_1558944721994251 – Supplemental material for Denervation as a Treatment for Arthritis of the Hands: A Systematic Review of the Current Literature
Supplemental material, sj-pdf-1-han-10.1177_1558944721994251 for Denervation as a Treatment for Arthritis of the Hands: A Systematic Review of the Current Literature by Sarah L. Zhu, Brian Chin, Mohamed Sarraj, Eugene Wang, Emily E. Dunn and Matthew C. McRae in HAND
Footnotes
Ethical Approval
This study did not require institutional review board approval.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This study did not involve active human participants; thus, no informed consent was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.