
Abstract
Background:
The purpose of this systematic review is to identify whether non-salvage procedures can provide satisfactory and acceptable outcomes in Lichtman stage IV disease.
Methods:
The MEDLINE, Embase, and Cochrane databases were systematically searched for English publications between 1989 and 2019 that reported stage IV-specific primary treatment outcomes. Revisions and skeletally immature patients were excluded. Data extracted were patient demographics, pain scores, range of motion (ROM), grip strength, and patient-reported outcome measures (PROMs). The results were pooled into 3 categories: conservative management, non-salvage, and salvage procedures.
Results:
Data from 24 studies (n = 114 patients) were extracted. Compared with conservative management and non-salvage treatment (joint-leveling radial osteotomies, lunate reconstruction), salvage procedures (intercarpal and radiocarpal arthrodesis, proximal row carpectomy, total wrist arthroplasty) showed significantly decreased ROM in flexion-extension arc of motion (89° vs 95° vs 73°, respectively, P = .0001) and no significant differences in grip strength as a percentage of the contralateral side (83% vs 86% vs 79%, respectively, P = .28). All reported treatments provided pain relief, ability to return to previous occupations, and variable PROMs.
Conclusions:
In young, active, and labor-intensive patients, motion-preserving, non-salvage options may be worth trialing as they do not preclude future salvage options.
Keywords
Introduction
To date, the natural history of Kienböck disease remains unknown, and the degree of clinical symptoms as well as functional limitations do not necessarily correlate with radiographic findings.1,2 Previous retrospective radiographic studies revealed incidental findings of advanced-stage Kienböck disease (stages III and IV) in patients who were asymptomatic and had undergone plain radiographs for unrelated reasons.3,4 However, in symptomatic patients, given the degenerative changes to adjacent radiocarpal and/or midcarpal joints, the observed tendency in the treatment of Lichtman stage IV disease is to perform salvage surgeries such as intercarpal arthrodesis, proximal row carpectomy (PRC), wrist arthrodesis, and total wrist arthroplasty.5,6 While salvage interventions generally provide good pain relief, they compromise mobility, and patients should not expect predisease functional outcomes. 7
Previous studies of Kienböck disease reporting outcomes of conservative treatment, 8 radial shortening osteotomy (RSO), 9 and vascularized bone graft (VBG) 10 have suggested benefits and reported acceptable clinical outcomes for all patients, including those with stage IV changes. Innes and Strauch demonstrated that subjective pain relief was achieved in the treatment of late-stage disease (combined stages IIIB and IV) using nonsurgical management, radial osteotomies, VBG, partial wrist arthrodesis, PRC, and tendon ball arthroplasty. Improved range of motion (ROM) was observed in all treatment groups except for partial wrist arthrodesis and nonsurgical interventions. A statistically significant increase in grip strength was also achieved in all but conservatively managed patients. 11
Although salvage procedures have traditionally been favored in Lichtman stage IV Kienböck disease,1,2 there is evidence suggesting acceptable outcomes in patients treated with non-salvage procedures such as extra-articular joint-leveling osteotomies and VBG. 11 Therefore, the purpose of this systematic review was to evaluate the existing evidence to summarize and compare clinical outcomes of all reported treatment modalities in stage IV Kienböck disease. The ultimate goal is to evaluate whether the literature supports non-salvage surgical intervention in end-stage disease.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were used for this study. A systematic search using keywords Kienböck, Kienböck’s disease, Kienböck disease, lunatomalacia, avascular necrosis of the lunate, and aseptic necrosis of the lunate was performed in the MEDLINE, Embase, and Cochrane databases. All English-language papers between 1989 and 2019 that included treatment outcomes for patients with Lichtman stage IV disease were included for full-text review. Two independent reviewers (P.Q.W. and B.P.C.) performed the initial title and abstract screening for study inclusion followed by full-text review. During the title and abstract review, if there were any doubts as to whether stage IV patients were included or if the abstract was unavailable, the articles would then be included for full-text review. Publications were included in the systematic review if they reported any Lichtman stage IV-specific treatment outcome. When stage IV-specific mean outcome measurements were not reported but individual patient data were available, the study was also included. The exclusion criteria consisted of revision or secondary treatment, skeletally immature patients, and biomechanical or animal studies. To maximize the sample size, studies composed of both eligible and ineligible patients were included if specific outcomes of patients meeting the inclusion and exclusion criteria could be differentiated.
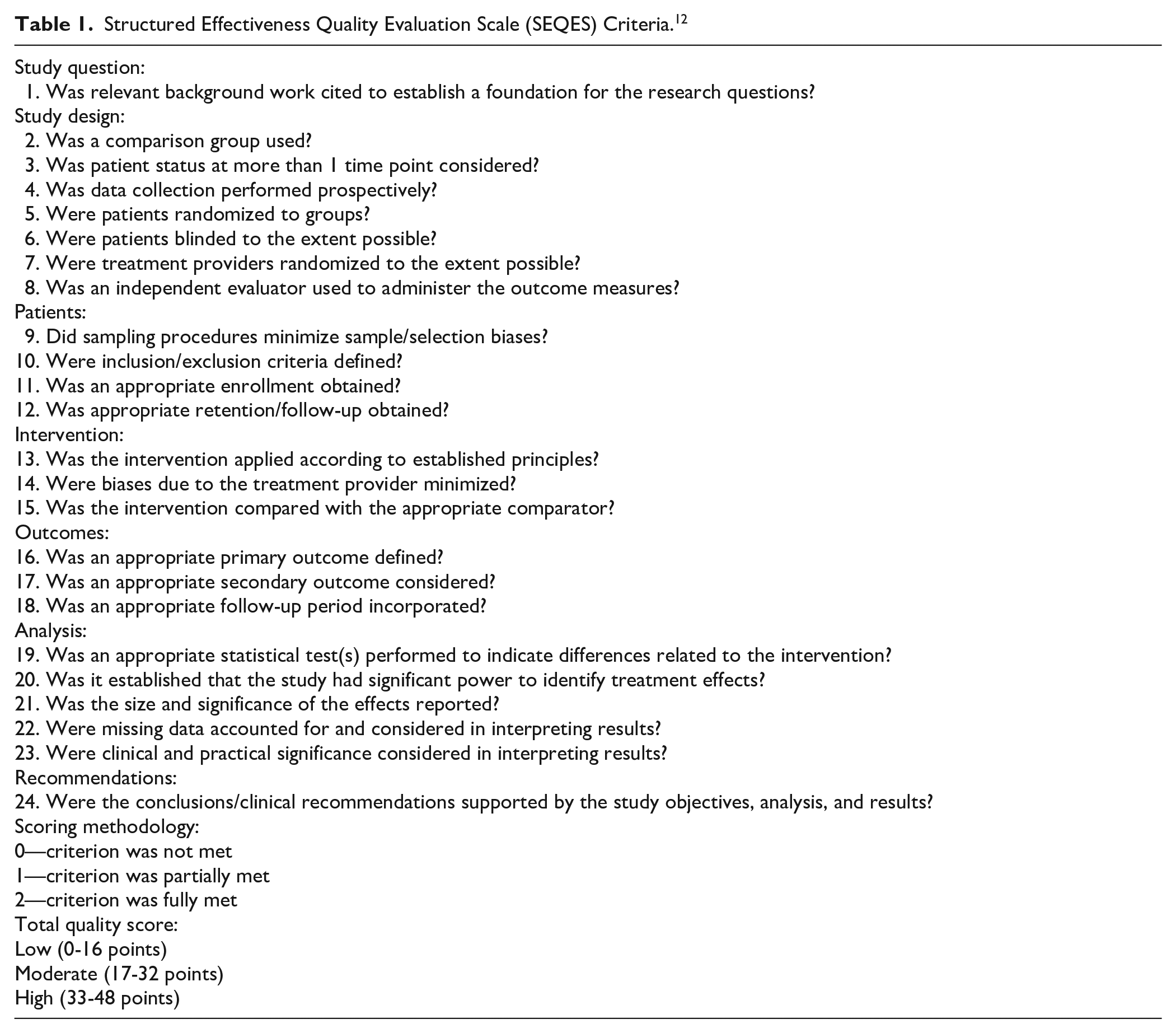
The quality of each included study was independently assessed by 2 reviewers (P.Q.W. and K.T.K.C.) using the Structured Effectiveness Quality Evaluation Scale (SEQES). The SEQES uses 7 items: study question, study design, patients, interventions, outcomes, analysis, and recommendations. Each category is given a score of 0 (criterion not met at all), 1 (criterion partially met), or 2 (criterion fully met). Scores between 0 and 16, 17 and 32, or 33 and 48 indicate poor-, moderate-, or high-quality evidence, respectively (see Table 1). 12 In the event of a disagreement, a third independent reviewer (N.S.) was available for discussion until consensus was reached.
Structured Effectiveness Quality Evaluation Scale (SEQES) Criteria. 12
Primary outcomes included pain, ROM, and grip strength. Secondary outcomes were patient-reported outcome measures (PROMs) and treatment complications or failure. Range of motion was reported either in degrees (°) of flexion and extension or as a percentage of the contralateral side. Grip strength was reported either in kilograms or as a percentage of the contralateral side. When available, outcomes reported in kilograms were converted to the percentage of the contralateral side when data from the unaffected hand were provided. When stage-specific mean outcome measures were not presented in the study but individual patient scores were available, the mean score for each outcome was calculated among the stage IV patients within the study. In addition, weighted interstudy mean ROM and grip strength scores were calculated when outcomes were reported using the same measurement scale. To do so, all patients with a reported ROM in degrees of flexion-extension and/or grip strength as a percentage of the contralateral side were pooled together and an average score was calculated. The outcomes were categorized into 3 groups: conservative (nonoperative) management, non-salvage, and salvage procedures. Non-salvage procedures included surgeries such as joint-leveling osteotomies, lunate decompression, and lunate reconstruction by lunate VBG or interposition arthroplasty. Partial or complete carpal arthrodesis, radiocarpal fusion, PRC, and total wrist arthroplasty were considered salvage procedures.6,7,13
Statistical analysis was performed using Prism version 9.0 (GraphPad, San Diego, California). The 3 treatment groups were compared using a 1-way analysis of variance (ANOVA) test with post hoc analysis using Tukey test for multiple comparisons. Subsequently, subgroup analysis within the non-salvage group comparing joint-leveling osteotomies and lunate reconstruction procedures was performed using the Student t test. A P value less than .05 was considered significant.
Results
The systematic search identified 1550 citations, of which 524 were duplicates. Following title and abstract review, 181 studies underwent full-text review and 24 articles met the eligibility criteria for this study. Following SEQES assessment, there were 11 low-quality and 13 moderate-quality studies (see Figure 1). There were a total of 114 patients treated for stage IV Kienböck disease included in the data. Demographic data (age, sex), follow-up period, and the type of studies are summarized in Table 2. Conservative management (n = 34) consisted of various treatment modalities, including cast immobilization, nighttime with or without daytime splints, course of physiotherapy, and the use of nonsteroidal anti-inflammatory drugs (NSAIDs). These regimens were individualized rather than standardized. Non-salvage procedures (n = 36) were RSO (n = 19), radial lateral closing wedge osteotomy (n = 4), and lunate reconstruction with VBG (n = 2) or interposition arthroplasty (n = 11), which included the use of vascularized os pisiform, costochondral, tensor fascia lata, plantaris, and palmaris longus grafts. Salvage interventions (n = 44) comprised intercarpal arthrodesis including the modified Graner procedure (n = 22), wrist arthrodesis (n = 1), PRC (n = 19), and total wrist arthroplasty (n = 2). In the modified Graner procedure used in 1 study, the collapsed lunate was excised followed by capitate osteotomy for which the proximal fragment was shifted to the lunate fossa. Except for the trapezium and pisiform, all other carpal bones were fused and the void created by the lunate excision was filled with autologous bone graft. 14
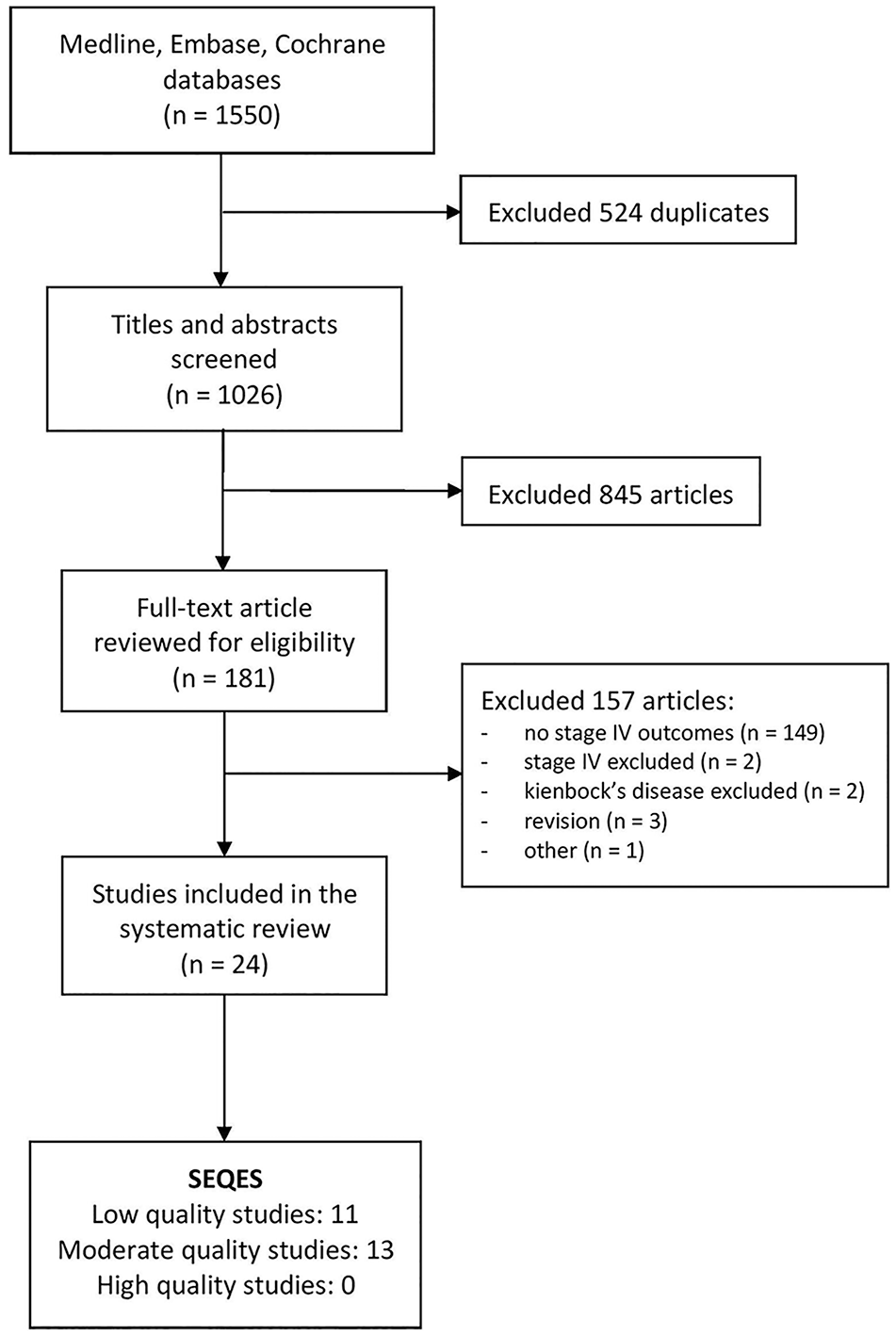
PRISMA and SEQES assessment flowchart.
Demographic Data, Follow-up Period, and Study Design.
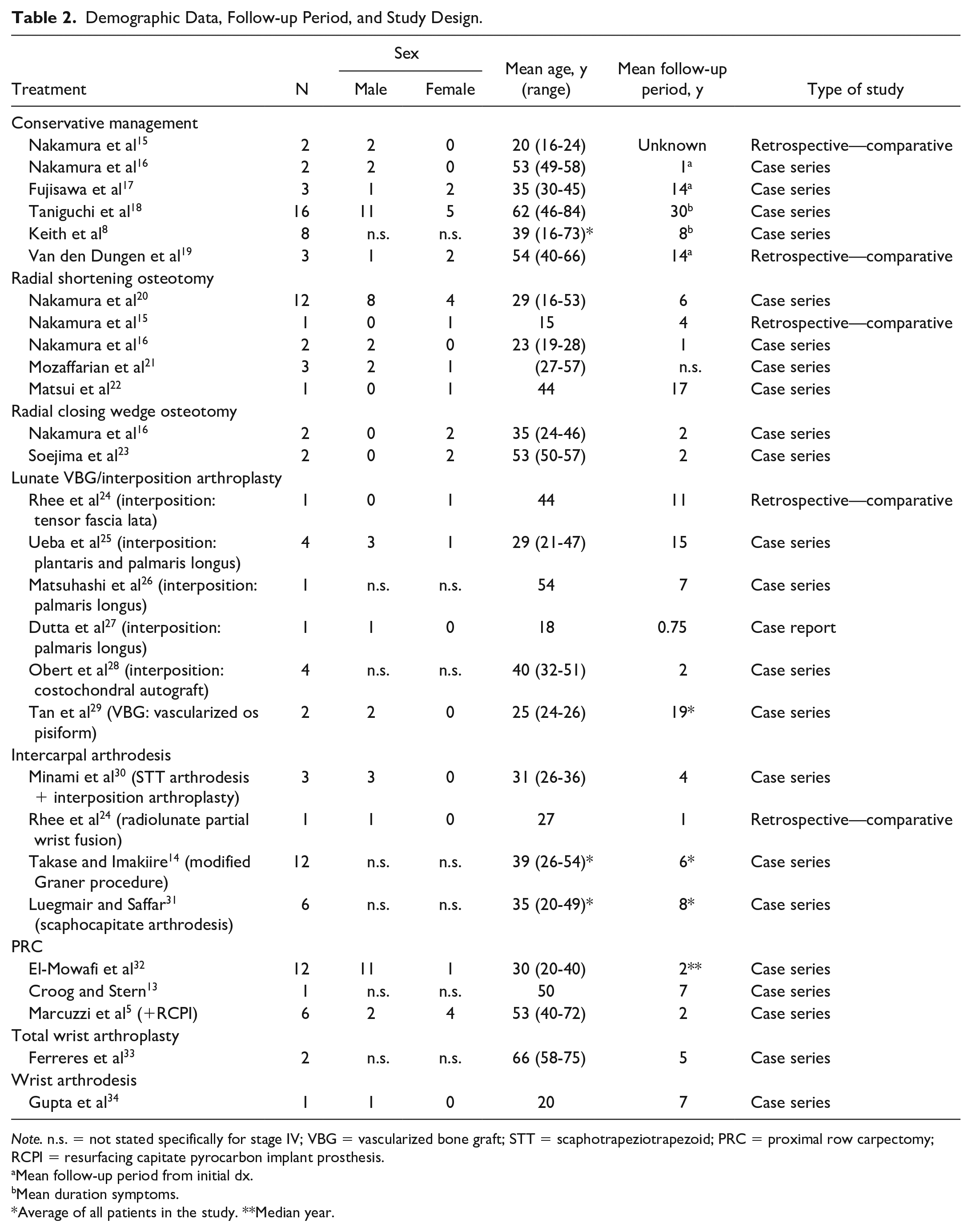
Note. n.s. = not stated specifically for stage IV; VBG = vascularized bone graft; STT = scaphotrapeziotrapezoid; PRC = proximal row carpectomy; RCPI = resurfacing capitate pyrocarbon implant prosthesis.
Mean follow-up period from initial dx.
Mean duration symptoms.
Average of all patients in the study. **Median year.
Clinical Outcomes
Pain
There were 3 studies (n = 27) that reported pain outcomes in conservatively treated patients. Two case series demonstrated an improvement in pain levels during long-term follow-up. A case series of 16 patients reported improvements to either no pain or mild pain following nonoperative management for an average of 30 years, 18 while 3 patients reported by Fujisawa et al improved to either no pain, slight discomfort related to heavy work, or occasional moderate pain at an average 14-year follow-up. 17 Keith et al reported moderate levels of pain in patients with stage IV disease with mean visual analog score (VAS) of 6.9 (n = 8); however, pain scores were similar to those of patients with earlier stages of the disease (II, IIIA, IIIB) within the same study with VAS scores of 6, 7, and 6.9, respectively. 8 Specific pain outcomes were not reported in 7 of the 34 conservatively managed patients.15,16,19
For radial osteotomies, pain outcomes were reported in a total of 18 patients.15,20,21,23 Nakamura et al reported 12 patients with stage IV disease. Preoperatively, 7 patients had mild pain with light work, while 5 patients had pain with daily use. Following RSO, all patients reported pain relief: 4 were pain free, 6 had mild pain with strenuous work only, and 2 had mild pain with light work at a mean 6-year follow-up. 20 One volleyball player reported pain relief postoperatively but had residual pain during sports 4 years after surgery. 15 In the lateral radial closing wedge osteotomy group, pain relief was obtained in the 2 patients for which pain was reported. At the 2-year follow-up, both patients showed mild pain with light or strenuous activities compared with pain with activities of daily living preoperatively. 23 On the other hand, Mozaffarian et al reported 3 patients with little relief and persistent mild or moderate pain with activities of daily living following RSO. 21
Lunate reconstruction provided significant pain relief. Interposition arthroplasty with combined plantaris and palmaris longus tendon ball resulted in 4 pain-free patients at an average 15-year follow-up. 25 A motion-sparing lunate reconstruction technique with costochondral autograft insertion as a free cartilage spacer also led to 4 pain-free patients at an average 2-year follow-up. 28 In 2 separate studies, following interposition arthroplasty using palmaris longus, 1 patient went from severe to mild pain postoperatively at the 7-year follow-up, 26 while another patient improved their VAS score from 6 to 2 at less than 1-year follow-up. 27 One patient who underwent interposition arthroplasty with a tensor fascia lata flap had occasional pain with exertion 11 years after surgery. 24 Meanwhile, 2 patients who underwent VBG with os pisiform transfer reported significant pain relief but still had either occasional or moderate pain long term. 29
In the salvage group, 14 patients were pain free (PRC and scaphotrapeziotrapezoid [STT] arthrodesis),5,30,32 6 patients had mild pain (PRC),5,32 2 patients had persistent moderate pain (PRC),13,32 and 1 patient had occasional pain with exertion (radiolunate wrist fusion). 24 The modified Graner procedure provided pain relief and resulted in either no pain or mild pain with activities among the 12 reported stage IV patients. 14 In a study including 6 patients who underwent scaphocapitate (SC) arthrodesis, pain was graded on a scale of 1 to 4 (1: no pain; 2: intermittent mild pain; 3: tolerable moderate pain; 4: severe or intolerable pain). The postoperative average score improved to 1 from 3.2 preoperatively. 31 Both patients following total wrist arthroplasty were very satisfied at the 5-year mark. 33
Range of motion
Ten studies involving surgical treatment reported both preoperative and postoperative ROM, and 5 reported postoperative ROM only. Five studies of conservatively managed patients provided ROM at the final follow-up, of which only 1 provided initial ROM (see Table 3). Improved ROM was reported in 3 studies (n = 15) of joint-leveling osteotomies15,20,23 and 1 study of PRC (n = 6). 5 Meanwhile, decreased ROM at the final follow-up was reported in 1 study of conservative treatment (n = 3), 19 2 studies of lunate reconstruction with interposition arthroplasty (n = 5),25,27 and 4 studies involving salvage procedures (STT arthrodesis, modified Graner procedure, SC arthrodesis, PRC, n = 22).13,14,30,31
Range of Motion and Grip Strength Outcomes.
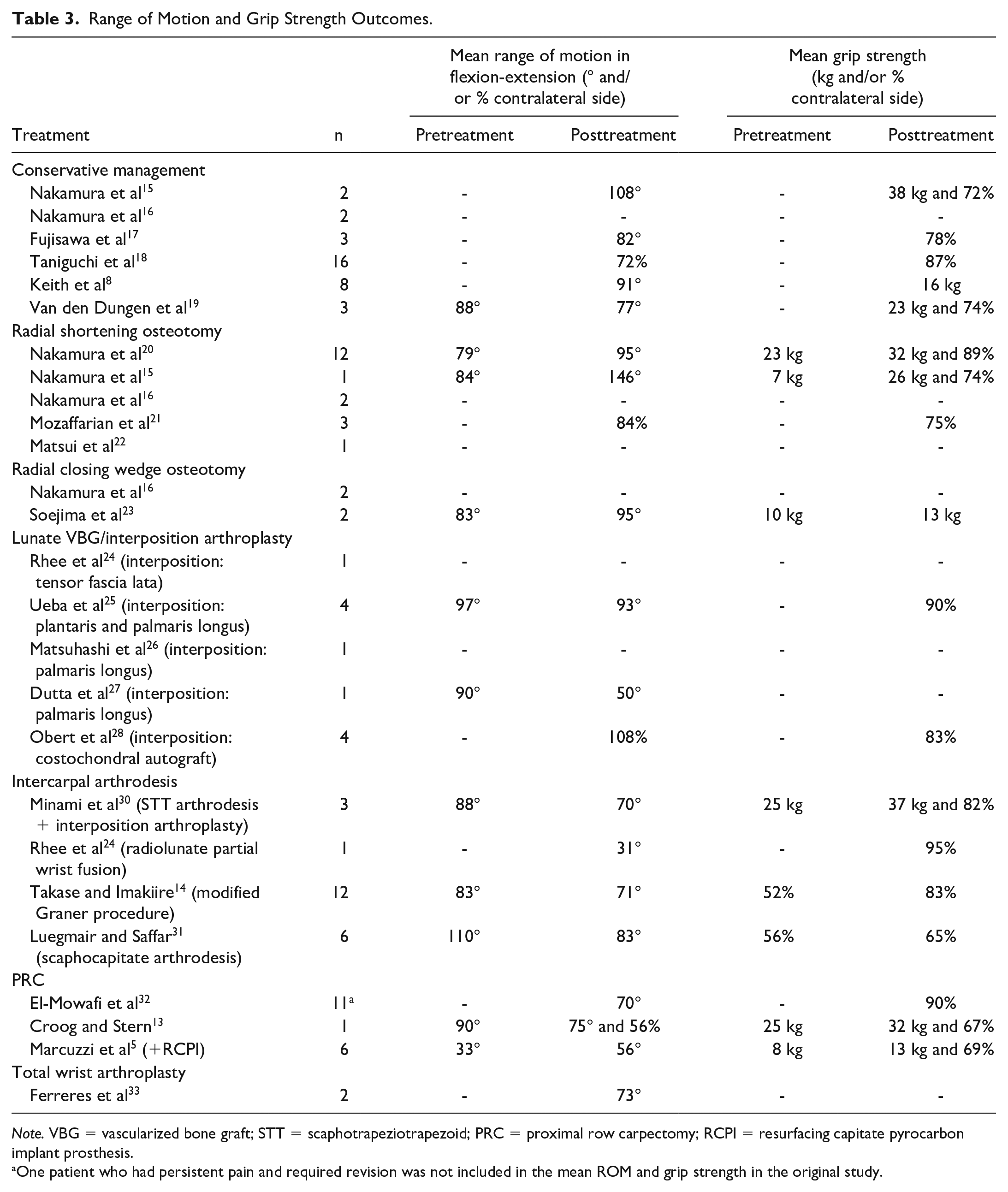
Note. VBG = vascularized bone graft; STT = scaphotrapeziotrapezoid; PRC = proximal row carpectomy; RCPI = resurfacing capitate pyrocarbon implant prosthesis.
One patient who had persistent pain and required revision was not included in the mean ROM and grip strength in the original study.
Weighted interstudy average ROM in flexion-extension arc of motion in the conservative, non-salvage group, and salvage group was 89° (4 studies, n = 16),8,15,17,19 95° (5 studies, n = 20),15,20,23,25,27 and 73° (8 studies, n = 42),5,13,14,24,30 -33 respectively (P = .0001). Range of motion in the salvage group was significantly decreased when compared with conservative and non-salvage treatment (P = .02 and .0002, respectively). No significant differences were observed between conservative and non-salvage treatment (P = .63) (see Table 4). Within the non-salvage group, weighted interstudy averages for radial osteotomies versus lunate reconstruction were 98° (3 studies, n = 15)15,20,23 and 85° (2 studies, n = 5),25,27 respectively, without significant difference (P = .30).
Weighted Mean Range of Motion and Grip Strength.
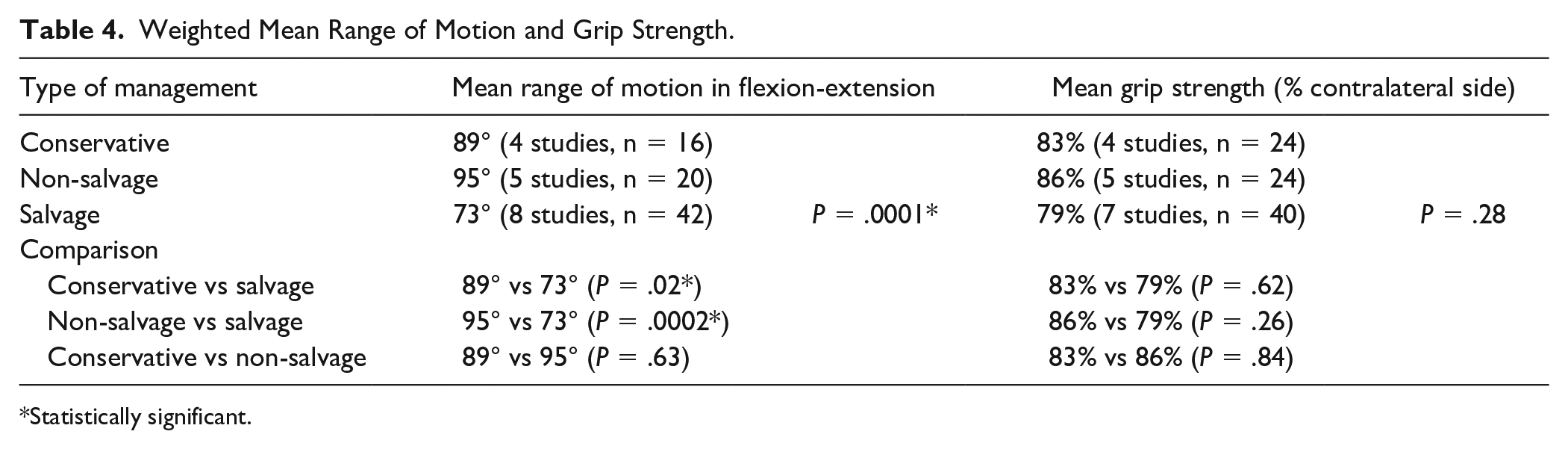
Statistically significant.
Grip strength
Preoperative and postoperative grip strength was provided in 8 studies of surgical management, and 5 provided postoperative grip strength only. Meanwhile, none of the studies of conservative treatment provided grip strength at the initial visit but 5 provided data at the final follow-up. Improvements of grip strength were reported in 3 studies of joint-leveling osteotomies (n = 15),15,20,23 3 studies of intercarpal arthrodesis (n = 21),14,30,31 and 2 studies of PRC (n = 7)5,13 (see Table 3).
There was no significant difference in the mean grip strength among the 3 groups. Weighted interstudy average grip strength as a percentage of the contralateral side in the conservative, non-salvage group, and salvage group was 83% (4 studies, n = 24), 15 ,17 -19 86% (5 studies, n = 24),15,20,21,25,28 and 79% (7 studies, n = 40),5,13,14,24,30 -32 respectively, (P = .28) (see Table 4). Within the non-salvage group, there was also no significant difference in weighted interstudy averages for radial osteotomies (86%, 3 studies, n = 16)15,20,21 and lunate reconstruction (86%, 2 studies, n = 8)25,28 (P = .90).
Functional outcomes
Patient functional outcome scores were heterogenous, ranging from excellent to poor scores, in all 3 groups. Various scores were used including the Nakamura Scoring System for Kienböck (NSSK); Mayo Wrist score; Disabilities of the Arm, Shoulder, and Hand (DASH); QuickDASH; Evans score; Dornan score; Green and O’Brien score; and Patient-Rated Wrist Evaluation (see Table 5).
Patient-Reported Outcome Measures.
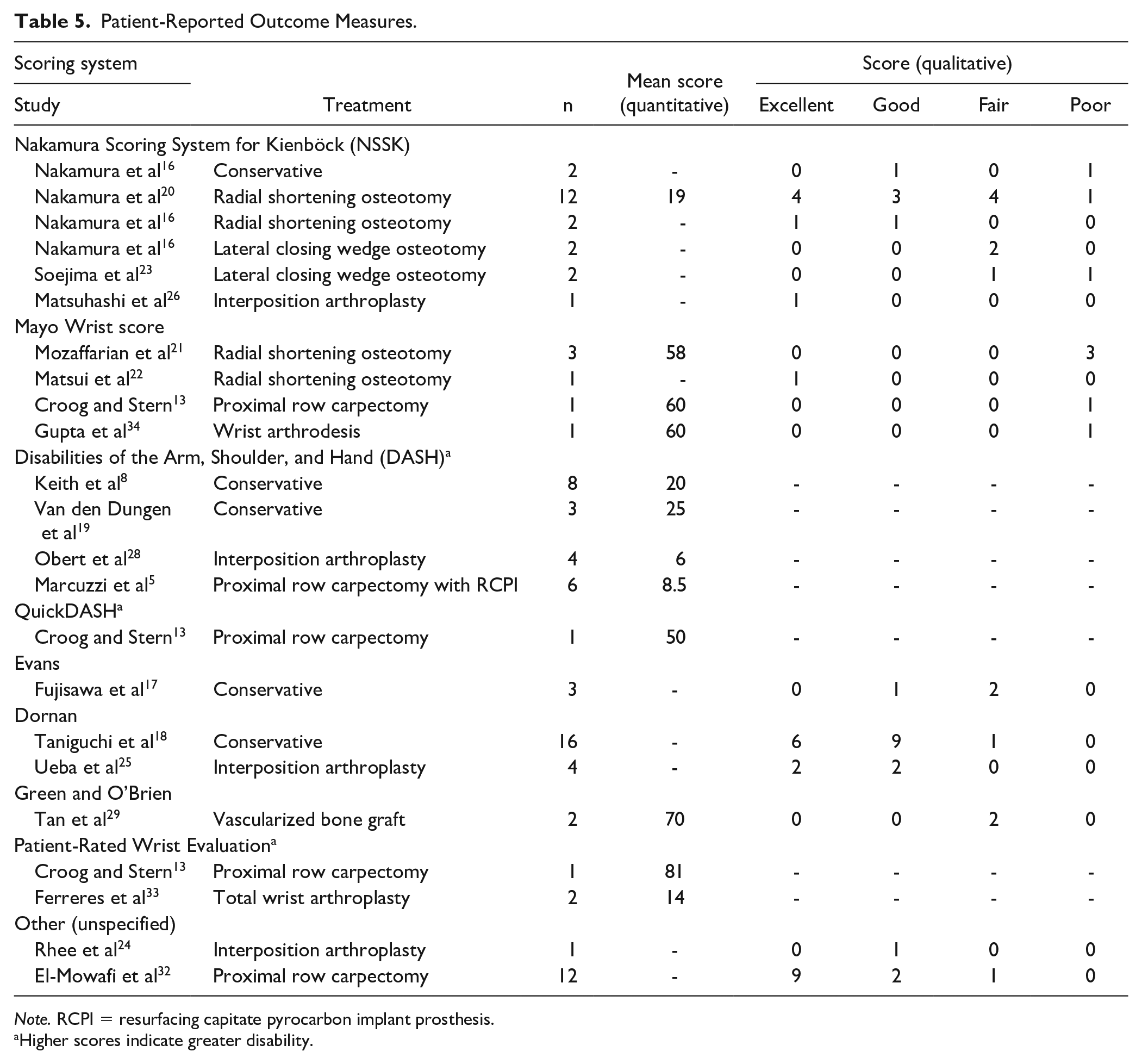
Note. RCPI = resurfacing capitate pyrocarbon implant prosthesis.
Higher scores indicate greater disability.
While clinical improvement was observed in all reported treatment options, surgical failure was reported in 3 stage IV patients who underwent PRC. These patients were young (aged 35-38 years), and 2, a mechanic and a farmer, underwent revision radiocarpal arthrodesis 3 years following the index surgery.13,32 The third patient underwent revision to wrist arthrodesis within the first year due to persistent pain postoperatively and progression of radiocapitate arthrosis. The patient would return to their previous employment as a clerk. 13 Two of the 3 patients were excluded from the data analysis in the original study and described separately. They were excluded from the pooled data from this review due to a lack of objective outcome scores or PROMs. 13
Return to previous occupation and sporting activities was also variably and inconsistently reported. Most patients were able to return to their previous occupations, including heavy manual labor. One patient in each of the conservative and non-salvage (RSO) groups were reported to have stopped participating in their high-level sport (mixed martial arts and volleyball). 15 In the VBG group, 1 patient changed to modified work in a factory following treatment while another patient, a teacher, was deemed able to return to work but remained unemployed. 29
Discussion
While the data pooled from this systematic review were not sufficient to identify a superior treatment strategy, it revealed similar results among both salvage and non-salvage procedures. Conservative treatment as well as non-salvage and salvage surgical interventions provided pain relief and positive outcomes in stage IV Kienböck disease. Most patients were either pain free or had mild pain at the final follow-up, while a few had moderate or occasional pain. Range of motion was best preserved with non-salvage procedures, particularly extra-articular joint-leveling radial osteotomies, while conservative measures and lunate reconstruction led to a slightly but not significantly lower ROM compared with radial osteotomies. A significantly lower mean ROM was observed in the salvage group. Grip strength was also best preserved with conservative and non-salvage procedures, although salvage interventions had slightly but not significantly lower grip strength when calculated as a percent of the patients’ contralateral side. Eight different PROMs were identified among the included studies. Results were quite variable and heterogenous ranging from excellent to poor results in all 3 treatment groups, with no definite trend and no treatment showing clear superiority. There were 3 reported failures (all PRCs) requiring eventual revision surgery, although the rate of failure for all treatments remains unknown. One patient from both the conservative and non-salvage groups did not return to their high-level sports and 2 patients in the VBG group did not return to their previous occupation. However, the true number of patients requiring modified work or complete change of profession remains unclear. The results of this study indicate a potential role for conservative and non-salvage treatment despite end-stage disease.
The natural history of Kienböck disease remains largely unknown. In stage IV disease, pain can be intermittent and activity related. Therefore, wrist immobilization and analgesics may be sufficient in treating acute pain crisis. Saffar et al noted that changes in occupations are rare when Kienböck disease is treated conservatively, likely due to adaptation and inherent work modification. 35 Providing a standardized treatment approach can be challenging, given the fact that the clinical presentation does not necessarily correlate with radiographic findings, where radiographic stage IV patients can also be asymptomatic.3,4 In younger patients, although progressive decrease in ROM and grip strength may lead to inevitable arthrodesis surgery in the future, initial nonoperative treatment may be worthwhile exploring, as long-term symptom improvement has been previously reported in conservatively treated patients.17,35
While joint-leveling surgery does not halt disease progression, it may play a role in revascularization around the lunate while providing satisfactory short- and long-term results. It is believed that surgical intervention around the distal radius, even if extra-articular, causes inherent revascularization by increasing postoperative hyperemic state within the anastomotic arterial blood supply around the radiocarpal region. 36 In a study by Nakamura et al, 4 stage IV patients were treated with either RSO or radial wedge osteotomy. They all underwent serial magnetic resonance imaging. Lunate T1- and/or T2-weighted signal intensity increased postoperatively in all patients suggesting some form of revascularization. 16 A multivariate study has also shown that preoperative Lichtman staging may not be a prognostic factor in the treatment of Kienböck disease with RSO. A previous study of 23 patients, including patients from stages I to IV, demonstrated that age (>30 years old) and excessive shortening (>4 mm) were predictors of poor prognosis. Meanwhile, preoperative staging did not significantly affect outcomes. 20 Furthermore, subjective pain, ROM, grip strength, and functional improvements are often observed despite further deterioration of postoperative radiographic findings.9,22,23 However, the underlying effect of joint-leveling procedures on degenerative wrist disease still needs further elucidation.
Lunate reconstruction surgery offers satisfactory outcomes and, like joint-leveling procedures, provides the advantage of maintaining carpal alignment. While complications include loss of carpal height and further degenerative changes, clinical relevance of these needs further elucidation.25,26,29 Therefore, joint-leveling radial osteotomy and lunate reconstruction surgery provide substantial short- and long-term pain relief while maintaining ROM and grip strength and most importantly, do not preclude future salvage procedures. The advantage of preserving future treatment options may be particularly beneficial in select patient groups, especially the young, active, and labor-intensive patients. 9
Despite satisfactory outcomes, salvage procedures are not without risk and complications. Long-term implications must not be minimized, given that Kienböck disease predominantly starts manifesting itself before the age of 40 years. 1 A previous systematic review assessing long-term outcomes of PRC showed that 14.3% of patients (6 studies, n = 147) underwent revision to arthrodesis or arthroplasty at a mean 53.4 months postoperatively due to failure, where a significant proportion of failures were from patients younger than 35 years. Thus, patient selection factors should include age and physical demands. 37 While PRC can still be successfully performed despite degenerative changes to the capitate and/or lunate fossa, the arthritis may further progress eventually requiring revision surgery with limited options.5,37 Despite positive outcomes, partial or complete arthrodesis led to restricted ROM which may not be ideal depending on the patient’s occupation and lifestyle.5,14 In addition, the risk of dislocation, loosening, and infection in total wrist arthroplasty should not be overlooked and little is known about long-term outcomes of such procedures. 2 As the natural history of this disease is yet to be fully understood, perhaps conservative and non-salvage procedures should be explored before a definitive salvage procedure is offered.
Limitations to this study are inherent to the rarity of the disease. Virtually all publications analyzed were underpowered and uncontrolled case series or case reports. The inconsistency in outcome reporting among studies limited the number of included patients and ability to pool data. Combining results with heterogenous sample sizes, demographic data, and follow-up periods also acted as a source of bias. Despite achieving positive outcomes in all treatment modalities described, it is unclear whether any surgical intervention provides superior results to conservative management, given the unknown natural history of the disease.1,11 Furthermore, it appears that the remodeling potential in the younger patients increases the likelihood of recovery with conservative management or less invasive procedures.1,20 Thus, the wide age range in this study may be a source of bias.
To overcome the limitations of Kienböck disease research, multicentered trials are needed to increase sample size and generalizability as very few centers, if any, are capable of performing sufficiently powered studies. Furthermore, standardized outcome measurements should be agreed upon. As observed in this study, multiple different PROMs were used hindering the ability to draw conclusions from these results. Reported results for ROM and grip strength were also heterogenous as different metrics were used and many studies lacked preoperative/initial data. As a result, researchers and surgeons must come to a consensus regarding study metrics. At present, the NSSK score is the only disease-specific score but has not yet been validated. 38 Moving forward, developing uniform disease-specific, valid, reliable, and responsive outcome measurements and PROMs will only enhance the collaborative efforts in Kienböck disease research.
Footnotes
Ethical Approval
Ethics approval was not required for this systematic review.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was not required as this was a systematic review of published and publicly available data. No patients were recruited.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.