
Abstract
Background:
Despite increased public awareness to dispose of unused narcotics, opioids prescribed postoperatively are retained, which may lead to drug diversion and abuse. This study assessed retention of unused opioids among hand surgery patients and describes disposal methods and barriers.
Methods:
Participants undergoing hand surgery were given an opioid disposal information sheet preoperatively (N = 222) and surveyed postoperatively to assess disposal or retention of unused opioids, disposal methods, and barriers to disposal. A binomial logistic regression was conducted to assess whether age, sex, pain intensity, and/or the type of procedure were predictors of opioid disposal.
Results:
There were 171 patients included in the analysis (n = 51 excluded; finished prescription or continued opioid use for pain control). Unused opioids were retained by 134 patients (78%) and disposal was reported by 37 patients (22%). Common disposal methods included returning opioids to a pharmacy (49%) or mixing them with an unwanted substance (24%). Reasons for retention included potential future use (54%), inconvenient disposal methods (21%), or keeping an unfilled prescription (9%). None of the patient factors analyzed (age, sex, type of procedure performed, or pain score) were predictors of disposal of unused narcotics (P > .05).
Conclusions:
Most patients undergoing hand surgery retained prescribed opioids for future use or due to impractical disposal methods. The most common disposal methods included returning narcotics to a pharmacy or mixing opioids with unwanted substances. Identifying predictors of disposal may provide important information when developing strategies to increase opioid disposal.
Keywords
Introduction
Prescription narcotic use has increased substantially over the past 2 decades. This increase has been followed by a rise in opioid-related abuse and overdose deaths which has led to investigations regarding prescribing patterns among physicians and opioid disposal patterns among patients.1,2 Overprescribing narcotics may be contributing to the opioid crisis. In a study that examined opioid-prescribing patterns among medical specialties, surgeons had the second highest rate of prescribing opioids (37%) and contributed to approximately 10% of the total number of narcotic prescriptions. 3 In another study, 23% of narcotic prescriptions for patients undergoing joint arthroplasties were provided by orthopedic surgeons even though one-third of these patients had other prescribers. 4 These findings are particularly distressing as 40% of opioid-related overdoses include patients with multiple prescribers.
Addressing patient expectations and providing preoperative counseling regarding pain management can help to reduce postoperative opioid consumption and improve disposal.5-8 Holman et al 4 found that patients with an orthopedic injury who received counseling were more likely to stop opioid use 6 weeks after their procedure compared with those who did not have any counseling (73% vs 64%). Providing patients with an educational tool may also help reduce analgesic requirements. Rose et al 8 introduced an educational pamphlet describing proper disposal techniques and found that disposal rates significantly increased. Similarly, Hasak et al 9 found that postoperative patients who received an educational brochure were more likely to dispose of unused opioids (22%) compared with those who did not receive any information (11%).
Although educational tools can improve disposal, many patients retain prescribed narcotics despite having greater awareness. Inadequate disposal of unused opioids may be contributing to the opioid epidemic. 11 Excess medications have led to divergent use or abuse by individuals other than the patients themselves. 5 Manchikanti and Singh 11 reported that 56% of persons (aged 12 years or older) obtained opioids from a friend or relative, and 81% of these medications were originally prescribed by a physician. A concerted effort among health care practitioners may be needed to counsel patients on methods of opioid disposal when these medications are no longer needed for pain control.
The purpose of this study was to assess if patients undergoing hand surgery retain unused opioids and to identify the methods of disposal and barriers to disposal. Identifying barriers to opioid disposal may change practice among surgeons who routinely prescribe postoperative narcotics. We hypothesized that most patients would retain unused narcotics, that the barriers of disposal would be related to inconvenience and the desire to keep the medications for future use, and that surgeries involving skeletal tissue or high pain scores would be associated with higher retention of opioids.
Materials and Methods
Study Design
A cross-sectional study design was used. Adults 18 years or older, English-speaking, and undergoing hand surgery were invited by a member of the research team to participate during their preoperative visit. In this discussion, each patient was informed that they would receive an information sheet on how to dispose of excess opioids on the day of their surgery in addition to their prescribed narcotics. Patients were excluded if they were taking opioids up to 4 weeks preoperatively, were still taking medications for pain control, did not receive a prescription for narcotics, did not have unused opioids, or had incomplete data. Patients with traumatic injuries were also excluded to control for pain related to concomitant trauma rather than isolated surgical-related pain. On the day of surgery, patients were given an information sheet, describing how to dispose of unused opioid medications, in addition to receiving a prescription of narcotics from either a resident, fellow, or staff surgeon. Each procedure was performed by 1 of 7 hand surgeons who agreed to participate in the study and were performed using local anesthetic or a regional block. Postoperatively, patients were given a questionnaire to complete, which included demographic data (age, sex), type of surgery, pain intensity score, whether the patient retained or disposed of opioids, reasons for retention, and methods of disposal. Given the variability in elective procedures, the quantity of opioid medication prescribed to each patient was determined by the treating surgeon. Institutional research ethics approval was obtained for this study.
Opioid Disposal Information Sheet
An information sheet was developed based on the different opioid disposal methods recommended by the Government of Canada, 12 the Institute for Safe Medication Practices Canada, 13 and the Health Products Stewardship Association. 14 Participants were given information on methods to find a local pharmacy that would accept returned opioids and to return unused pills to a participating pharmacy and methods to dispose of excess opioids at home (Figure 1).
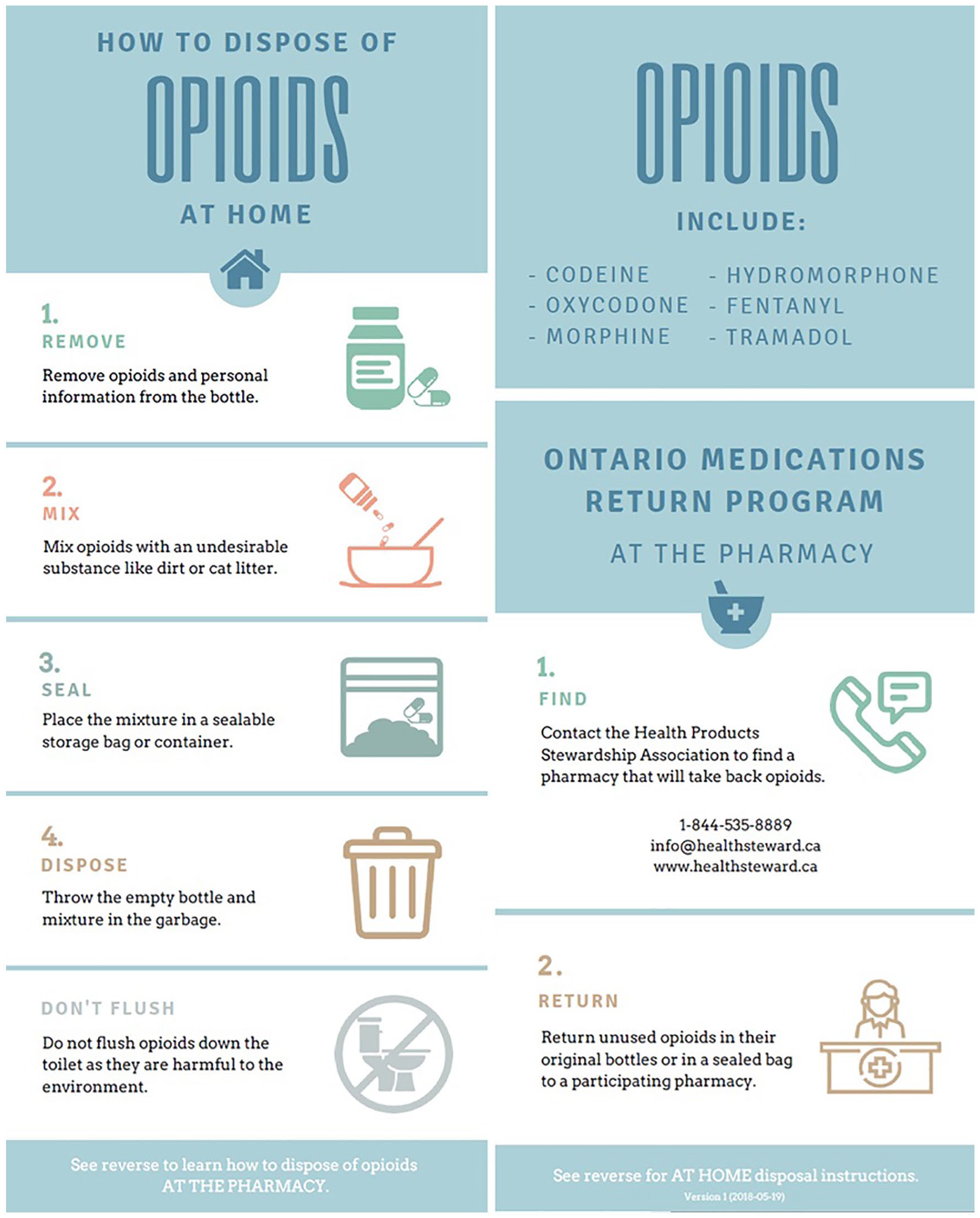
Opioid information sheet that was given to patients prior to surgery.
Statistical Analyses
Data were summarized with means and standard deviations for continuous variables and with frequencies for categorical variables. Parametric or nonparametric t tests were used to assess differences between patients who retained narcotics compared with those who disposed of unused narcotics. A binomial logistic regression analysis was used to assess the association between age, sex, pain scores, and type of procedure and the likelihood of opioid disposal among patients undergoing hand surgery. The required sample size was calculated using G*Power analysis program (n = 106). 16 The following parameters were used with the assumption that 25% of patients undergoing hand surgery dispose of their opioids and 75% retain opioids: β = .80; α = .05; and an odds ratio between those that dispose and retain was 0.11.
Results
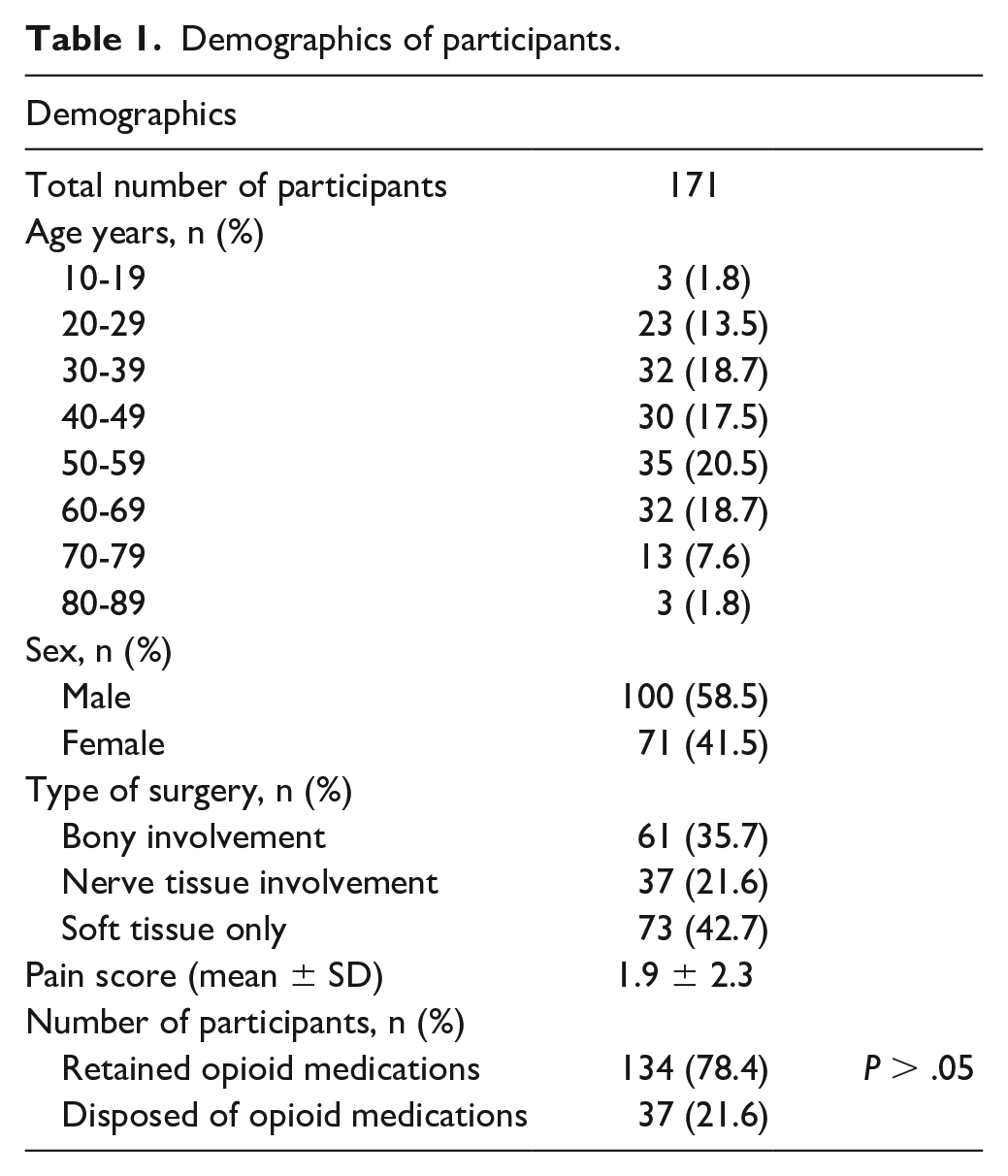
There were 222 patients who participated in the study. Data from 171 patients were included in the analysis, and there were 51 patients excluded: still taking their analgesics, n = 20; did not get a prescription, n = 4; finished their prescribed narcotics, n = 25; and incomplete data, n = 2 (Table 1). There were no significant differences in demographics between patients who disposed of opioids compared with those who retained opioids (P > .05). Among the 171 patients, there were 229 procedures performed; the types of surgeries performed have been summarized in Table 2. Procedures that were classified as “Other” included infrequent procedures (eg, tendon transfer, local flap reconstruction, joint arthroplasty).
Demographics of participants.
Types of surgeries performed.
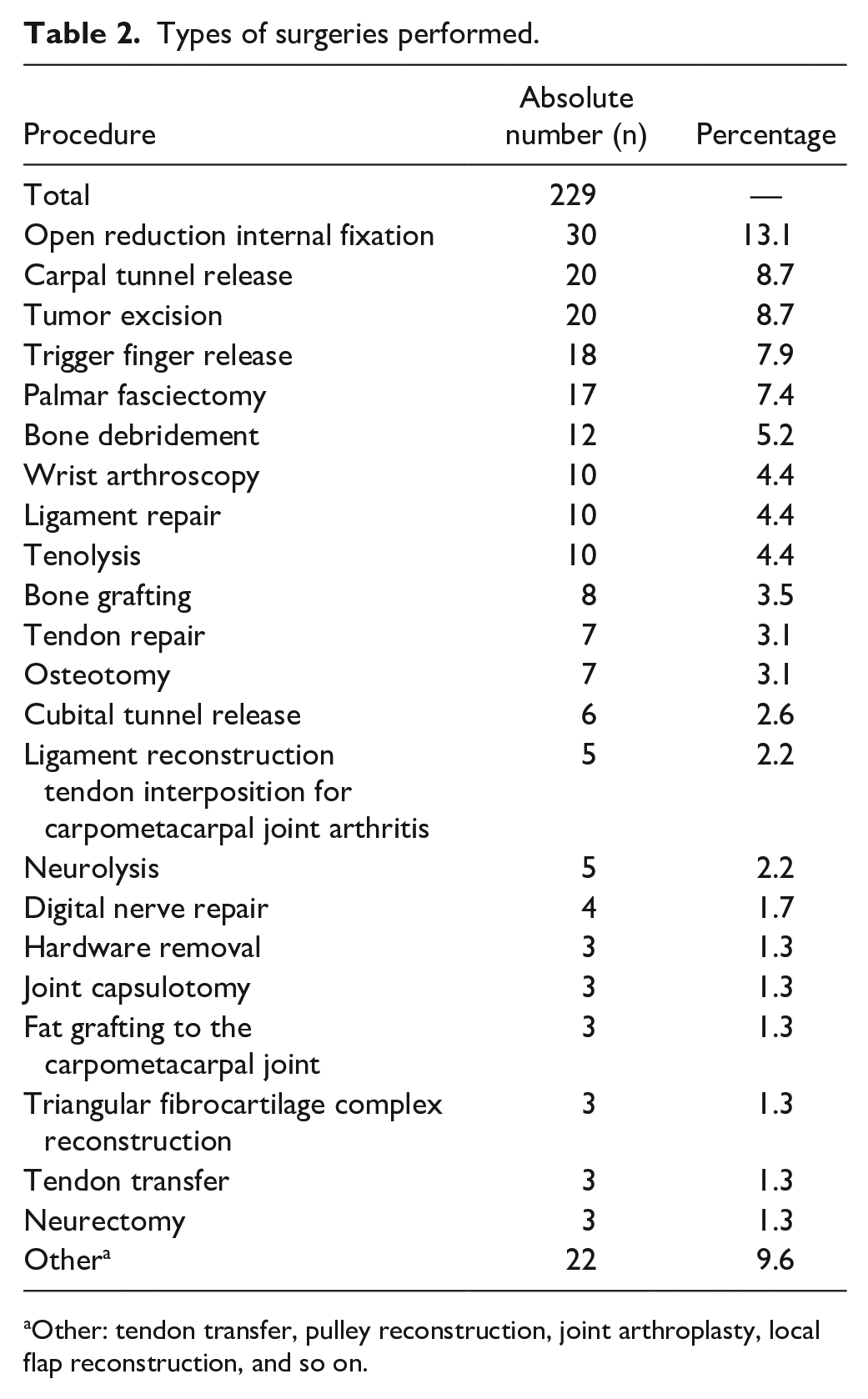
Other: tendon transfer, pulley reconstruction, joint arthroplasty, local flap reconstruction, and so on.
Unused opioids were retained by 134 patients (78%). Of the patients who disposed of unused narcotics (n = 37), the most common methods of disposal include returning narcotics back to a pharmacy (49%) and mixing the narcotics with an unwanted substance (24%; Figure 2). Other methods of disposal that patients described include shredding unfilled prescriptions. Among those that retained unused opioids, participants selected 1 or more reasons for keeping their medications and in total, there were 155 reasons for retention that were shared by the participants. Reasons for opioid retention included potential future use (54%), inconvenient disposal methods (21%), or keeping an unfilled prescription (9%; Figure 3). Other described reasons for retention include forgetting to dispose or using excess opioids to help with management of other medical conditions like migraines or insomnia.
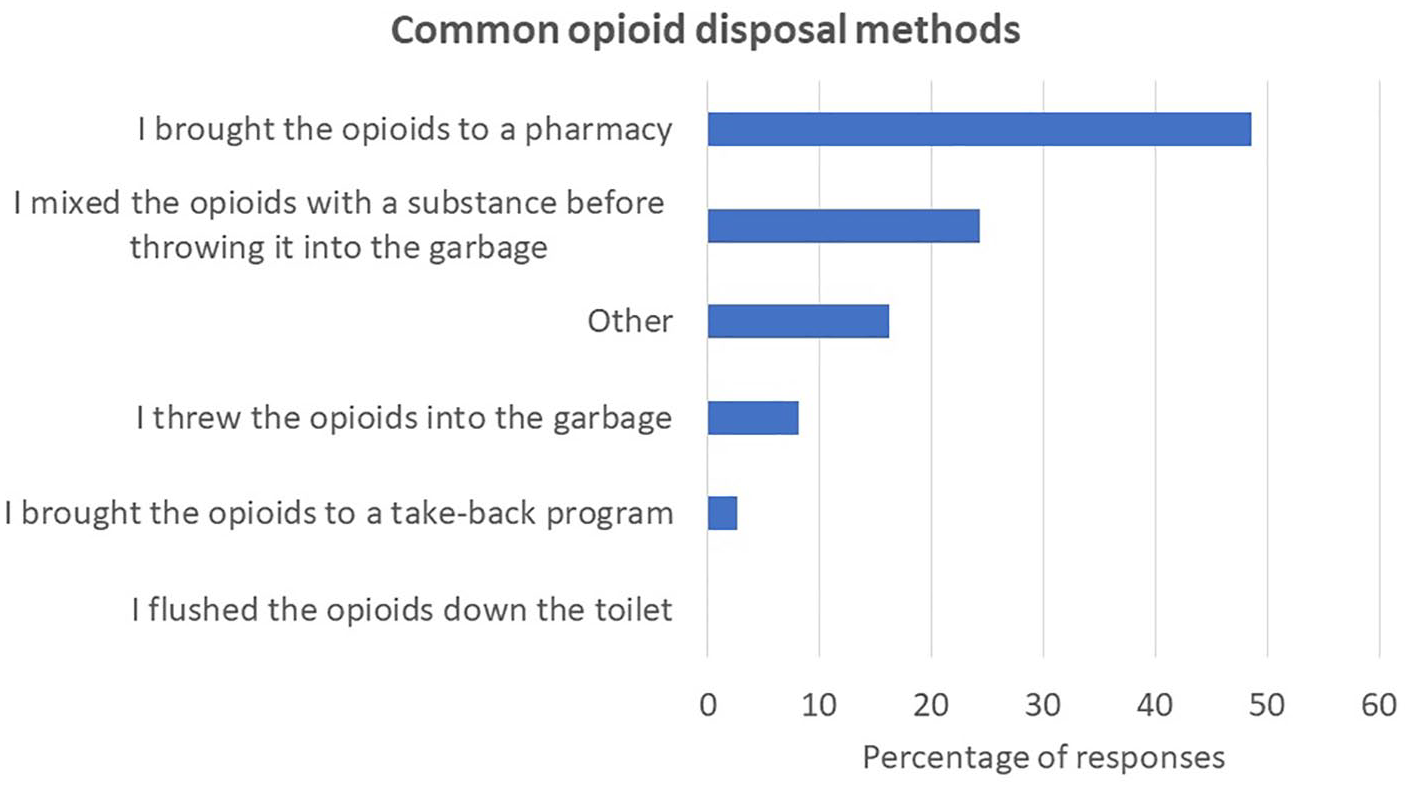
Common opioid disposal methods among patients undergoing hand surgery.
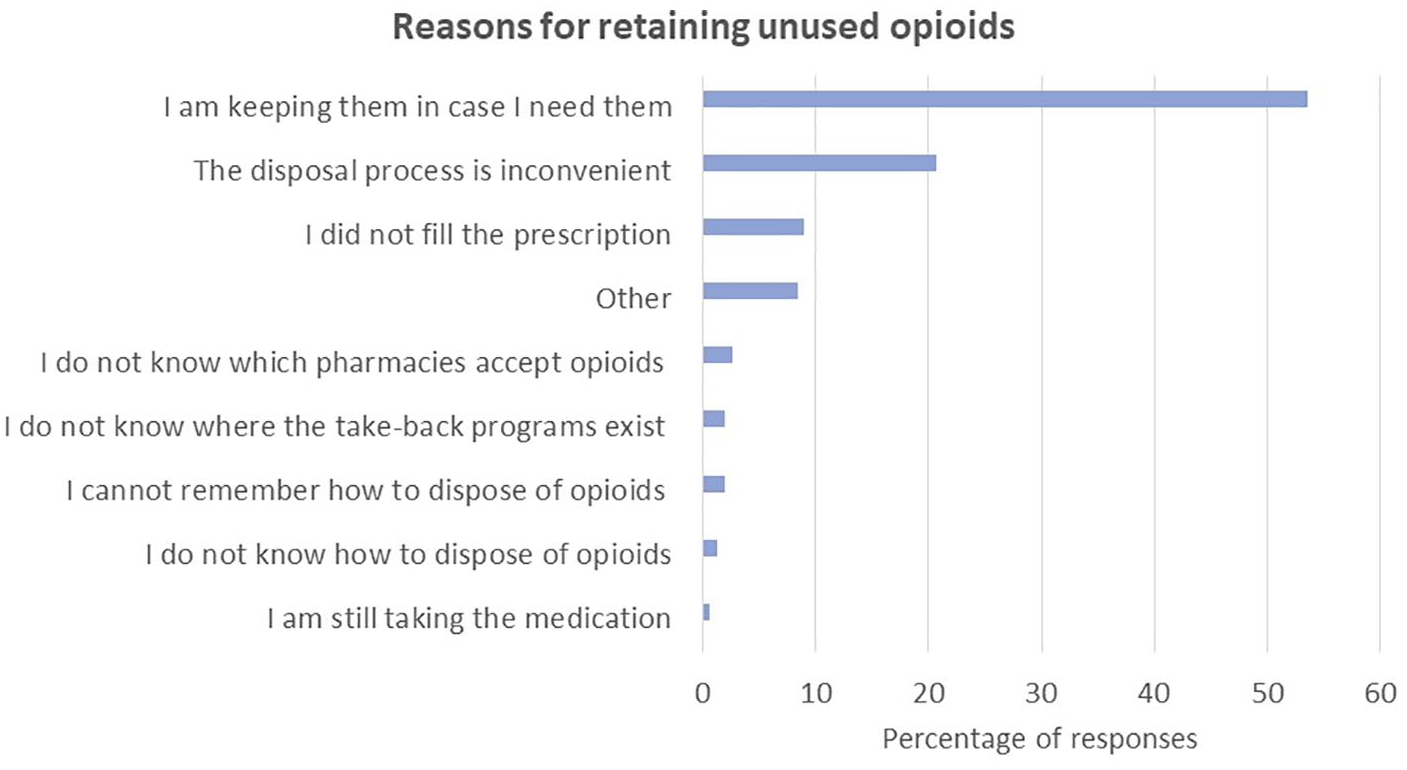
Reported reasons for opioid drug retention among patients undergoing hand surgery.
In the logistic regression model, there were no significant predictors for disposal of unused narcotics (P > .05; age, sex, type of procedure performed, or pain score).
Discussion
In this study, 78% of patients following hand surgery retained their opioid medications. Most patients retained unused narcotics for future use (54%), had unfilled prescriptions (9%), and/or found the disposal process too inconvenient (21%). These findings are consistent with the results from a systematic review which found that 42% to 71% of surgical patients from various surgical specialties retained unused narcotics. 16 Among these studies, 3% to 21% of patients had an unfilled prescription which was similar to our study of hand surgery patients. 17 Other reported reasons for retention include using narcotics for sleep, nonsurgical pain, indigestion, gastrointestinal discomfort, anticipation of pain, or because they were given narcotics. 18 Retaining narcotics is a major public health risk as controlled substances are unregulated and may be abused or diverted to different sources. 19 In a survey of college-age students, approximately one-third of participants reported obtaining narcotics from a loved one, most of which originated from a legitimate prescription. 11
The high amount of unused prescribed narcotics may be contributing to the opioid epidemic as the number of overdose-related deaths continues to rise. Despite these statistics, the rates of opioid disposal have been low. Disposal methods may also not align with guidelines stipulated by the US Food and Drug Administration. 17 Previous investigators have found that few patients receive appropriate disposal instructions from their health care providers. 19 Kim et al 20 found 5% of patients received information on disposal from providers, including physicians, recovery room nurses, and pharmacists and that almost half of the patients were unaware of safe disposal techniques or the dangers of retaining unused pills. Other barriers to disposal were related to inconvenience as disposal options outside of the home environment (eg, narcotic drop boxes, take-back events) led to retention. 19
Among patients who disposed of opioids in our study, the most common method of disposal included returning the narcotics back to a pharmacy (49%) or mixing the medications with an unwanted substance prior to throwing the mixture in the garbage (24%). Harbaugh and Waljee 21 found that only 6.1% of their patients returned the medications back to a pharmacy and 3.7% threw the medications in the trash. This discrepancy between our results and previous studies may be related to diverse disposal methods that are available in the United States or regional variations in disposal policies (eg, take-back events).
In our study, patient factors, including age, sex, type of procedure performed, and pain scores, were not associated with opioid disposal or retention. Previous studies have described increased opioid consumption among younger patients, those with specific insurance types (eg, Worker’s Compensation, self-pay, and Medicaid), and those undergoing fracture or joint-related surgeries as these surgeries involved more pain. In our study, we hypothesized similar results, where bony-related surgeries that involved more pain would have greater narcotic retention. However, the association between pain scores and disposal patterns was not found and may be related to the low levels of pain reported following elective hand surgery (85% rated pain intensity <5). Perhaps in the acute, traumatic patient population where pain scores may be higher, these factors may have a greater effect on disposal patterns and may warrant further investigation.
There are several limitations associated with this study. Although patients were given narcotics following their surgery, information regarding whether they were opioid naïve or taking other analgesic adjuncts were not obtained. These factors may have also had an effect on disposal behavior and should also be explored in future studies. Other patient information, such as the patient’s comorbidities (eg, anxiety, depression, rheumatologic conditions), smoking status, and history of substance abuse, were not obtained; these factors may also contribute toward opioid retention and may warrant investigation. Finally, given the potential sensitive questions asked in the survey, the study may be limited by a social desirability response bias in which patients may answer questions in a way that may be more favorable.
The results from our study emphasize the need for increasing public awareness on how to safely dispose of excess narcotics. Surgeons may be encouraged to provide disposal counseling if including this discussion into their practice can decrease drug abuse and diversion. Harbaugh and Waljee 22 found that patients who were educated on the topic were more likely to dispose of medications. Perioperative counseling in other surgical specialties have demonstrated a 22% increase in the proportion of patients who disposed or reported intent of disposal. 23 Similarly, disposal rates increased when patients were given tangible educational pamphlets that outlined how to dispose leftover narcotics.9,10 Other strategies that have been described include multimedia education tools,7,10 formal take-back programs, 24 and at home disposal kits. Brummett et al found a significant increase in disposal among patients who had access to an activated charcoal bag at home (57%) compared with those who received the standard of care (29%) or written information (33%). 24
While there have been efforts on the systemic and provider level to address the opioid epidemic, the amount of unused prescription opioids that eventually enter the community also rely on patients disposing of unused narcotics. This study demonstrated that most patients undergoing hand surgery retain unused narcotics despite receiving education on methods of disposal. The decision to retain or dispose unused narcotics is complex and multifactorial. Identifying extrinsic patient-related factors or societal factors may lead to a better understanding of the reasons patients retain opioids and to help design better strategies to increase disposal rates.
Footnotes
Acknowledgements
The authors would like to thank the staff at the Toronto Western Hospital for their support during this study and Dr Tomas Saun for his assistance in creating the opioid disposal information sheet.
Disclosure
Preliminary data related to this study have previously been presented at 2 conferences: 2020 American Association for Hand Surgery Meeting and the 65th Annual Plastic Surgery Research Council Meeting.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.