
Abstract
Background:
Double crush (DC) syndrome patients presenting with C6-7 radiculopathy and median nerve compression in the carpal tunnel report greater nerve irritability and weakness postdecompression than isolated peripheral nerve decompression. We hypothesize that patient-reported outcome is inferior following release at both cervical spine and wrist versus a single site of decompression.
Methods:
Patients that underwent either anterior cervical decompression and fusion (ACDF) for C6-C7 radiculopathy, carpal tunnel release (CTR), or both within 5 years (DC) were identified. A total of 477 patients were analyzed (157 DC, 203 CTR, and 117 ACDF). Post-operative outcome Disabilities of the Arm, Shoulder, and Hand (QuickDASH), Neck Disability Index, and visual analog scale (VAS) scores were collected at an average of 2 years postoperatively.
Results:
QuickDASH scores were higher in the DC group versus CTR group (36 vs 22, P < .0002). Postoperative disability in the ACDF group was significantly higher than the DC group (50 vs 36, P < .017). There were no differences between ACDF and DC groups in arm pain intensity, but the CTR group demonstrated significantly greater arm pain intensity than the DC group (5.7 vs 3.6, 10-point scale, P < .01).
Conclusions:
Patients undergoing ACDF and CTR have greater postoperative disability than those undergoing CTR alone, but less postoperative functional disability and pain than ACDF alone, indicating cervical radiculopathy may contribute a greater proportion of long-term disability postoperatively. Additionally, CTR had greater postoperative arm pain than DC patients, potentially indicating high rates of undiagnosed cervical radiculopathy or other sources of arm pain in these patients.
Keywords
Introduction
Double crush syndrome (DCS) is defined as tandem compression of a peripheral nerve at more than 1 distinct site along its course. 1 Prior studies calculate the prevalence of DCS as ranging from 10% to 70% in carpal tunnel and cervical radiculopathy patients.1-8 DCS may provide a pathophysiologic explanation for persistent symptomatology and disability in patients with compressive neuropathy despite perceived appropriate management. 3 Patients with DCS have demonstrated higher rates of dissatisfaction and persistence of symptoms postdecompression than those with a single site of nerve compression in the upper extremity, possibly due to the synergistic effect of multiple disruptions of axoplasmic flow.3,6,9
Previous studies evaluating outcomes of patients with DCS are limited by the lack of comparison to those patients with isolated radiculopathy. In this study, we utilized isolated radiculopathy controls to evaluate the impact of proximal compression on double crush syndrome, and compare postoperative disability between double crush, isolated radiculopathy, and carpal tunnel patients. The purpose of this study was to evaluate the preoperative and postoperative patient reported outcomes (PRO) of patients with cervical radiculopathy alone versus those with tandem peripheral compression. We hypothesized that DCS patients would report worse postdecompression outcomes than patients that underwent either carpal tunnel release (CTR) or anterior cervical decompression and fusion (ACDF) alone.
Materials and Methods
Institutional review board approval was obtained for this retrospective single institution database study. All patients who underwent CTR or anterior cervical decompression and fusion (ACDF) for C6-C7 between January 1, 2003 through January 1, 2020 were identified by CPT (CTR: 64721 or 29848, ACDF: 22551) and ICD (CTR: G56.00-G560.03, radiculopathy: M50.1, M54.1, M43.22) codes. The C6-C7 nerve roots were used due to these levels making the primary contribution to the median nerve, ensuring that the cervical spine and carpal tunnel compressions occurred along the same peripheral nerve. A total of 11,394 subjects were identified as having undergone either CTR and/or ACDF.
The double crush group (DC) was defined as those patients who underwent both ACDF and CTR within a 5-year period of each other (as defined by Wessel et al) 10 and confirmed by individual chart review of postoperative reports and diagnostic codes. Only patients with ACDF at the C6/7 segment were included. The cervical decompression (ACDF) control group was defined as patients who underwent ACDF at the C6/7 level without CTR within a 5-year period at our institution. Patients were excluded from the ACDF group if they had ICD and/or CPT codes corresponding to carpal tunnel operations. The carpal tunnel control group (CTR) was similarly defined as patients undergoing CTR without ACDF within a 5-year period at our institution. Identified CTR patients were excluded from the carpal tunnel group if they had ICD and/or CPT codes corresponding to ACDF operations.
Primary outcomes consisted of patient-reported outcome measures (PRO) collected at the time of final postoperative follow-up; Disabilities of the Arm, Shoulder, and Hand (QuickDASH), Neck Disability Index (NDI), and pain Visual Analog Scale (VAS) questionnaires. For the double crush group, this was defined as the time between score recording and the patient’s most recent surgery.
The double crush group was compared to the CTR and ACDF groups utilizing students T test for QuickDASH and NDI, and the Mann Whitney U test for VAS outcome measures. Both Students T test and the Mann Whitney U test were utilized assuming nonrandom variance and the null hypothesis to be no difference between the 2 groups. An unadjusted alpha of 0.05 level of significance was used.
Results
Of the total 11,394 original patients, 242 had both an ACDF at C6-7 and CTR within a 5-year period. Of that cohort of patients, 157 had QuickDASH, NDI, and/or VAS outcome score survey results. The remainder of the cohort yielded 7,875 CTR patients 3,217 ACDF patients. (Figure 1).
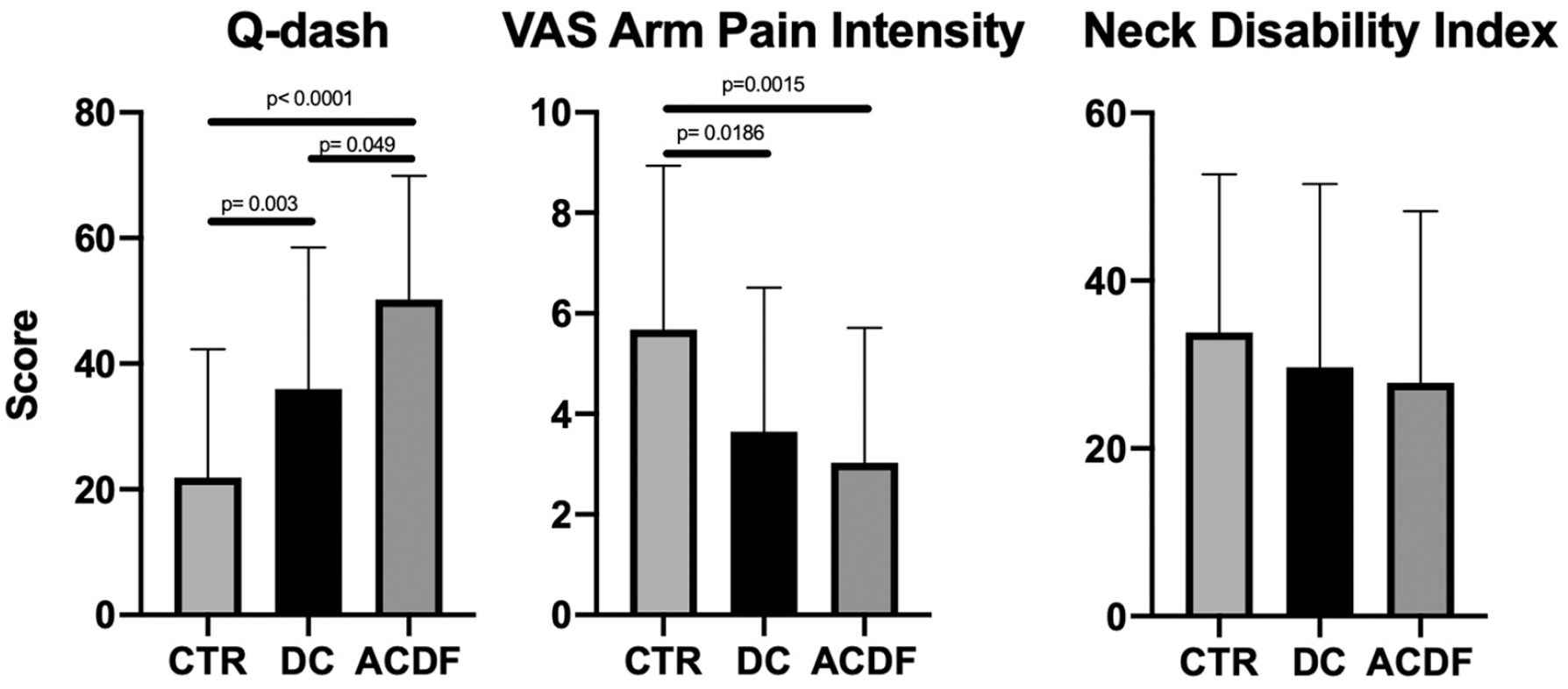
displays mean patient reported Disabilities of the Arm, Shoulder, and Hand (QuickDASH), Visual Analog Scale (VAS) arm pain intensity, and Neck Disability Index (NDI) for the Carpal Tunnel (CTR) and Cervical Radiculopathy (ACDF) groups, plotted against the Double Crush (DC) group.
Of 7,875 CTR patients, 2,057 had findings of radiculopathy as identified by ICD codes, and thus were not included. From the remaining, 3,543 patients had QuickDASH, NDI, and/or VAS PROs on file, and 137 total CTR patients had such PROs on file corresponding to times after their surgeries. From the 3,217 ACDF patients, 1,722 patient’s operations did not include the C6-C7 level. From the remaining 1,495 ACDF patients, 933 had QuickDASH, NDI, and/or VAS PROs on file, and 117 had such PROs from dates after their surgery (Figure 1). For all cohorts, patients with incomplete or missing postoperative PROs were excluded from the study.
A total of 157 patients were included in the DCS group, 137 in CTR, and 117 in the ACDF group. Postoperative PROs collected from all 3 groups averaged approximately 24 months postoperation. There were no significant differences in the age, sex, or race between the DC and CTR groups. The ACDF group contained a significantly higher percentage of white males than the other 2 groups but remained similar in average body mass index and age (Table 1). Within the DC group, CTR was performed first in 102 patients, and ACDF first in 54. 2 Patients underwent both operations on the same day.
Demographic Information.
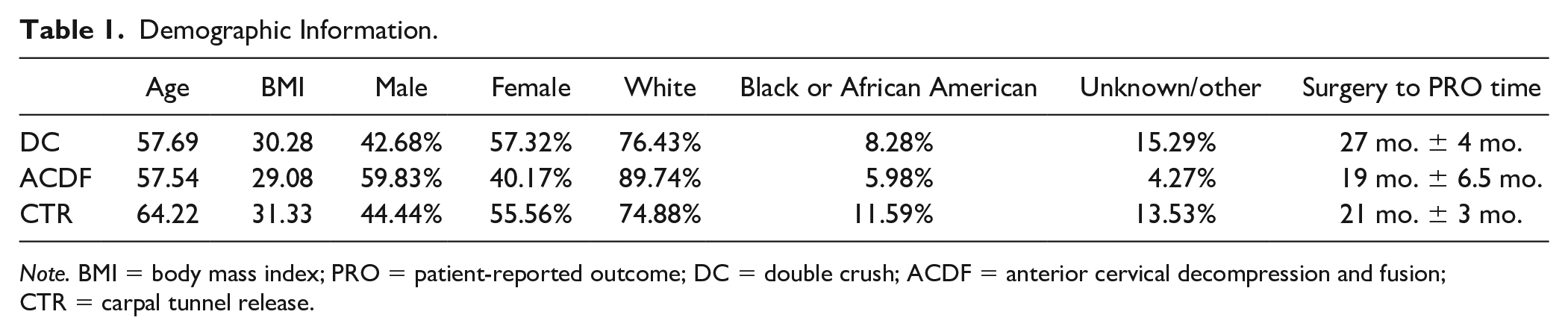
Note. BMI = body mass index; PRO = patient-reported outcome; DC = double crush; ACDF = anterior cervical decompression and fusion; CTR = carpal tunnel release.
Of the 157 DCS patients, a total of 57 (36%) had QuickDASH, 65 (41%) NDI, and 31 (20%) VAS scores reported following both surgical decompressions. The ACDF group had 17 (15%) patients with QuickDASH responses, 65 (56%) NDI responses, and 31 (26%) VAS. Finally, the CTR group yielded 95 (69%) QuickDASH, 36 (26%) NDI, and 34 (25%) VIS postoperative scores. Nerve conduction studies were available for review for approximately 47% of patients in the DC group, 70% in the CTR group, and 23% in the ACDF group. The time elapsed between surgery and final PRO collection time was the longest for the double crush group (27 months ± 4 months), with CTR (21 months ± 3 months) and ACDF (19 months ± 3.5 months) groups having less time between surgical decompression and PRO collection. (Table 1)
Patients in the DC group reported significantly higher postoperative disability on the QuickDASH survey compared to the CTR group (36 versus 22, P < .0002) (Figure 2). The ACDF group reported significantly higher disability than the DCS group on QuickDASH questionnaire (50 versus 36, P < .017) (Figure 2). There were no significant differences between the ACDF and DC group when comparing the arm pain intensity on the VAS scale. However, CTR patients reported significantly higher postoperative VAS arm pain intensity versus the DC group (5.7 vs 3.6 on a 10-point scale, P < .01) (Figure 2). The mean NDI scores did not differ between groups.
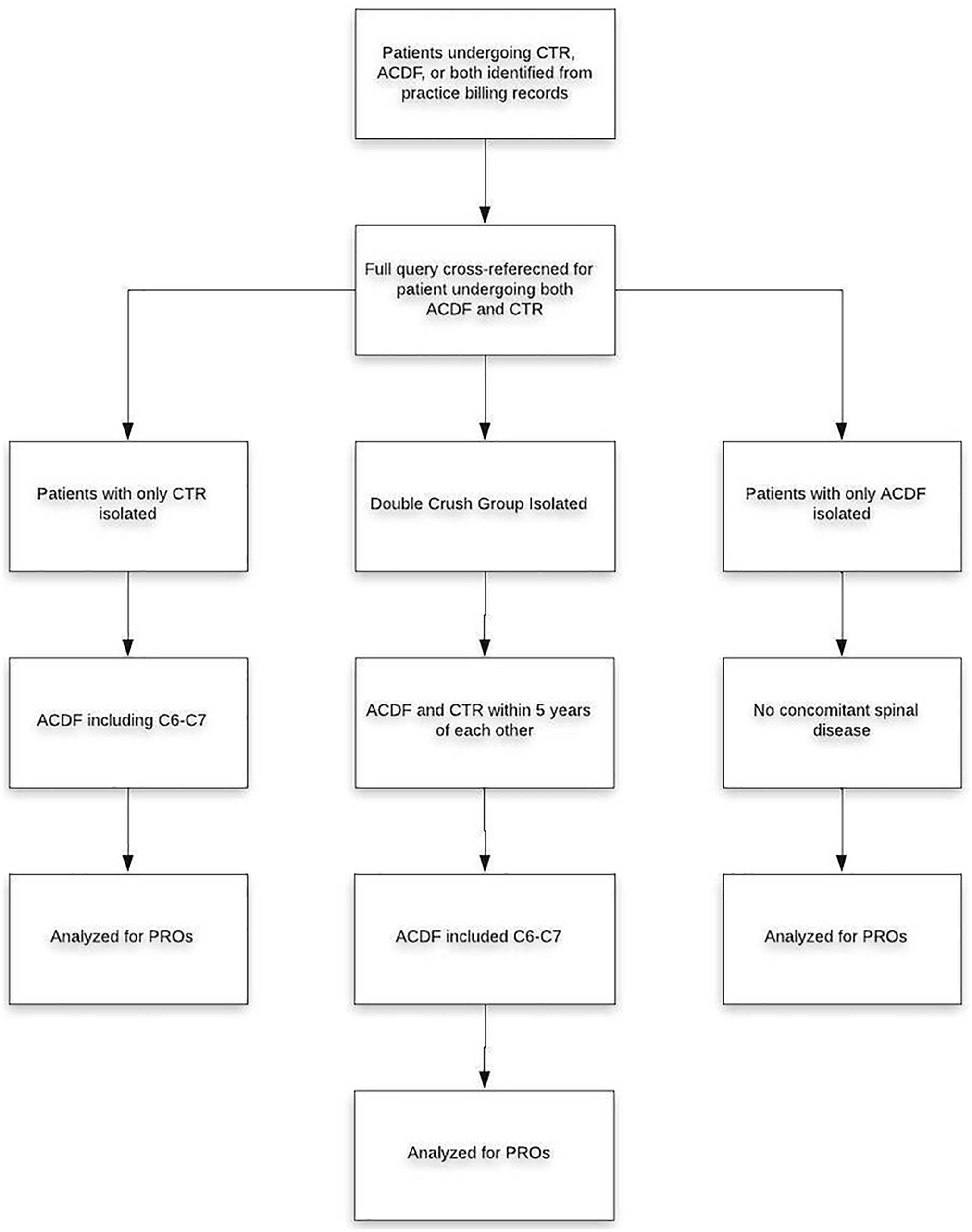
displays a flow chart outlining inclusion criteria for all 3 groups and follows the flow of processing taken for data collection.
Discussion
The purpose of this study was to evaluate outcomes of patients undergoing surgical intervention for cervical radiculopathy at the C6/7 segment compared to those with double crush syndrome undergoing concomitant CTR and CTR alone. We demonstrate that DC patients QuickDASH outcomes poorer than those of isolated CTR patients, but better than those of isolated ACDF patients. Additionally, we found that CTR patients report significantly more persistent arm pain following decompression than double crush patients. These findings may suggest that cervical radiculopathy may contribute a greater portion to long-term functional disability (as measured by QuickDASH), than distal compression, and contribute less to persistent arm pain. Additionally, there may be a high rate of undiagnosed cervical radiculopathy accompanying carpal tunnel syndrome.
In their original publication, Upton and McComas speculated that the presence of 1 peripheral nerve compression predisposed the nerve to increased susceptibility for an additional compression at another location along its length. 1 The authors explained this observation by theorizing that disruptions in axoplasmic flow through the nerve predisposed distal elements to compression symptoms and vulnerability.Such axonal disturbances have been theorized to contribute to the worse outcomes following decompressive surgery as described by Osterman 6 and Eason et al. 9
Previous studies have demonstrated that cervical radiculopathy patients with concomitant compression in the carpal or cubital tunnel (ie, double crush) report greater nerve irritability and muscle weakness postdecompression when compared to patients with isolated carpal or cubital tunnel syndrome. 10 Wessel et al also demonstrated that double crush patients report significantly higher postoperative disability and symptom persistence on QuickDASH questionnaires (29 vs 13), the Levine Katz symptom severity scale (2.0 vs 1.4), and functional status scales (1.9 vs 1.4 on a 5-point scale) versus patients with a single site of compression.10,11 Additionally, Eason et al found that 81% of patients who reported being dissatisfied after CTR surgery had signs of existing cervical spinal disease. 9
Although Upton and McComas’ theory has been widely debated, Baba et al demonstrated that constriction of the Tibial nerve in rabbits consistently lead to reduction in conduction velocity distal to the constriction as well as reduced axonal and total fiber diameter. 12 Additionally, Dellon and Mackinnon showed that banding rat sciatic nerves proximally lead to a greater rate of decline in the amplitude of compound action potentials than more distal banding (P < .0001). 13 They went on to further conclude that 2 sites of compression produced significantly greater reduction in rat sciatic nerve compound action potential than either proximal or distal banding alone (P < .0001). 13
Regardless of the pathophysiology behind DCS, there are significant difference in nerve composition and function when multiple peripheral compressions occur. In a case control study of double crush syndrome, Wessel et al found that, after decompressive surgery for both compression sites, 6 out of 29 double crush patients had a decline in sensory function, as measured by 2-point discrimination (P = .05), versus 1 in 30 patients that underwent carpal or cubital tunnel decompression alone. 10 In this study, Wessel et al included both carpal and cubital tunnel subjects in their control group, necessitating evaluation of 2 different nerves and distances between peripheral compressions. Wessel and colleagues proposed that their findings might be explained by delayed diagnosis and intervention at the second point of peripheral compression compared to the first, resulting in longer compression and worse outcomes. 10
Although Wessel et al’s conclusions are clinically relevant in understanding the manifestations of double crush syndrome, and a clear indication that double crush syndrome leads to poorer outcomes that carpal or cubital tunnel compression alone, it is not clear from this study whether DCS outcomes are poorer than those in isolated cervical radiculopathy.
Our data are consistent with the findings of Wessel et al in that rather than DC being more severe than either ACDF or CTR alone, we instead found that ACDF patients report significantly worse outcomes than double crush. We demonstrate significantly greater average disability on the QuickDASH questionnaire in DC patients than in those undergoing CTR alone (36 versus 22, P < .0002). However, the ACDF group scored significantly worse on the QuickDASH survey than the double crush group (50 versus 36, P < .017). This disparity seems to indicate that cervical radiculopathy may contribute a greater proportion of long-term functional disability (as measured by QuickDASH) than more distal compressions. This supports the work of Dellon and Mackinnon that proximal compressions show more significant nerve degeneration symptoms than distal lesions 13 and emphasized the importance of diagnosing proximal nerve compressions.
Our data also demonstrate that patients who underwent isolated carpal tunnel surgery reported significantly greater postoperative arm pain than the DC patients (5.7 versus 3.6 on a 10-point scale, P < .01). This may indicate a large proportion of existing undiagnosed cervical radiculopathy in patients affected by carpal tunnel syndrome. Such cervical compressions may develop subsequent to the carpal tunnel entrapment or be below the limit of detection by nerve conduction studies and/or physical exam. As such, the original hypothesis by Upton and McComas that even minimal proximal compressions can predispose to a second compression may be reinforced by this finding—patients with low-grade cervical spine compression potentiating carpal tunnel syndrome may have worse postoperative outcomes without decompression in the cervical spine. While the possibility of a larger portion of undiagnosed cervical radiculopathy exists, this study did not account for the degree of severity in cases of isolated carpal tunnel syndrome. As such, patients with isolated carpal tunnel syndrome may have had more severe disease with subsequently increased persistence of symptoms and/or disability due to persistent numbness or thenar muscle wasting. The relationship between severity of disease and symptom persistence represents an important area for future studies.
The nature of anatomic and surgical differences between the 2 compressions in double crush syndrome introduced an inherent limitation in our study. Certain questionnaires may not have been provided to all patients, depending on their respective complaint at presentation, limiting patient response potential. This limitation was especially relevant when comparing NDI of the lone carpal tunnel group, and QuickDASH results in the ACDF group. Hand and spine surgeons are not necessarily considering the neck and hand (respectively) after performing their respective surgeries, so responses for both outcomes were minimal. The double crush group had a similar limitation in that many patients identified as fitting the double crush criteria only had scores (ie, QuickDASH, VAS, etc) following one of their corrective surgeries, but not the second. Such responses would have only been addressing 1 of the 2 necessary decompression and thus invalidated these responses for the study. This resulted in lower power and may be subject to the bias in responder outcomes aforenoted.
As a retrospective study, it is limited by patient follow-up and self-reported outcomes. Patients were largely excluded due to missing and/or incomplete PROs, as well as PROs corresponding to presurgical intervention. The lack of appropriate PROs on file required the exclusion of a large number of potential patients. Patient outcome measures not being available for all patients potentially resulted in sampling error and potential bias. Additionally, those patients completing PRO surveys may be prone to be more satisfied. 14 Despite the potential bias toward increased satisfaction in patients filling out PRO surveys, 14 the amount of time between decompression and PRO collection in the CTR group may suggest that a high number of patients in our cohort were of the approximately 6% that suffer from persistent pillar pain postdecompression.15,16 Patients tend to only have 1 to 2 follow-up visits for CTR, indicating that longer follow-up may correlate to more persistent pain. However, the reason for such persistent symptoms are not well understood, and may be partially explained by concomitant cervical spine disease, as previously discussed.15,16
Another limitation of this study is that it was performed with records from a single institution. Patients receiving either ACDF or CTR operations and/or medical intervention at other institutions may have been erroneously added into groups they would have otherwise been excluded from. This same limitation may have resulted in some DC patients being present in either the ACDF or CTR control groups due to having the second peripheral decompression at another institution. As a retrospective study, we did not have access to such outside institutions records, resulting in a possible source of error. Additionally, concomitant carpal tunnel disease could have been ruled out as the cause for higher QuickDASH surveys among the ACDF cohort had electrodiagnostic data been available for a higher percentage of said cohort.
In this study, we found that double crush patient report significantly worse outcomes on the QuickDASH than carpal tunnel patients, but significantly better QuickDASH and VAS Arm Pain Intensity outcomes than anterior cervical spine compression patients. This may indicate a population with undiagnosed DCS. Further studies into double crush syndrome should be aimed toward evaluating the rate of underdiagnosed DCS, as well as defining risk factors.
Our data, consistent with previous literature, underlie the importance of considering proximal nerve damage when presented with distal nerve compressions. Diagnostic screening and procedures should keep in mind the importance of addressing multiple sites of compression given the clinical manifestation of different sites of compression. More specifically, patients presenting with carpal tunnel compression should be evaluated for cervical radiculopathy, as it may predispose these patients to inferior postoperative outcomes.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This study was approved by the Institutional Review Board of Thomas Jefferson University, ethics committee reference number (215) 503-2222. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.