
Abstract
Background
Postoperative care after dorsal wrist ganglion (DWG) excision is highly varied. The effect of immobilization of the wrist on patient outcomes has not yet been examined.
Methods
A systematic review of the literature was performed to determine whether wrist immobilization after DWG surgical excision is beneficial. A survey of hand surgeons in Canada was performed to sample existing practice variations in current immobilization protocols after DWG excision.
Results
A systematic review yielded 11 studies that rigidly immobilized the wrist (n = 5 open excision, n = 5 arthroscopic excision, n = 1 open or arthroscopic excision), 10 studies that used dressings to partially limit wrist motion (n = 5 open, n = 5 arthroscopic), 1 study (open) that did either of the above, and 2 studies (arthroscopic) that did not restrict wrist motion postoperatively. This ranged from 48 hours to 2 weeks in open DWG excision and 5 days to 3 weeks in arthroscopic DWG excision. The survey of Canadian hand surgeons had a similarly divided result of those who chose to immobilize the wrist fully (41%), partially (14%), or not at all (55%). Most surgeons surveyed who immobilized the wrist postoperatively did so for 1 to 2 weeks.
Conclusion
The systematic review and survey of Canadian hand surgeons reveal that hand surgeons are divided regarding the need to immobilize the wrist after DWG excision. In terms of functional outcome, there is no compelling data to suggest 1 strategy is superior. The time frame for immobilization when undertaken was short at 2 weeks or less.
The systematic review is registered in the PROSPERO database (PROSPERO 2016:CRD42016050877).
Keywords
Introduction
Ganglions are the most common tumor of the hand and are commonly found on the dorsal aspect of the wrist, arising from the wrist capsule at the scaphoid-lunate interval. 1 The cause of dorsal wrist ganglion (DWG) remains unknown.2-4 While typically firm, round, and painless, compression of nearby terminal branches of the posterior interosseous nerve may cause pain.1,5,6 Treatment options include no intervention, needle aspiration, and surgical excision. Recurrence rates vary from 25% to 67% for patients treated with needle aspiration and between 8.3% and 42% after surgical excision.7-9
Despite the prevalence of DWG and routine surgical treatment, there is a lack of consensus among hand surgeons as to the length of time a wrist should be immobilized postoperatively, if at all. The objectives of this study were to conduct a systematic review of the literature to examine outcomes following various immobilization protocols and survey Canadian hand surgeons to assess the variability in postoperative protocols following DWG excision.
Methods
Systematic Review
Search strategy and study selection
This review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. This systematic review has been registered in the PROSPERO database (PROSPERO 2016:CRD42016050877). The following databases were searched: CINAHL, Embase, MEDLINE, and SportDiscus on September 13, 2016, and repeated on January 3, 2020 (refer to Supplemental Material for search strategy).
Included, full-text articles were: (1) a randomized controlled trial (RCT) comparing different postoperative splinting protocols in DWG excision patients; or (2) any other RCT, observational study, or case series specifying a postoperative care protocol for DWG excision patients. Articles were excluded if they demonstrated any of the following: an entirely pediatric population, nonsurgically managed DWG, case studies, and non-English articles. All outcomes were considered, including grip strength, range of motion, pain, quality of life, and recurrence rates.
Data abstraction and collection
Studies were screened by 3 independent reviewers (A.C.H., M.K., and C.R.W.). Reviewers conducted a pilot screen of the titles and abstracts of the first 50 articles to practice applying the inclusion/exclusion criteria. Once consistency was established, title and abstract screening was completed and authors proceeded with full-text review of the identified studies. In the case of disagreement, the senior author (M.C.M.) was consulted. Interrater agreement for both review phases was calculated using an unweighted kappa statistic. Data were extracted using a predefined, standardized data collection instrument. Extracted data included demographic information, the type of surgical intervention, the postoperative protocol, follow-up duration, and any reported outcomes. The updated review was performed by 2 independent reviewers (C.R.W. and M.H.M.).
Risk of bias assessment
Risk of bias (RoB) was assessed individually by 2 reviewers (C.R.W. and M.H.M.). Disagreements were resolved through discussion until consensus was achieved, and consultation with an arbitrator (M.C.M.), if needed. Included studies that were nonrandomized were evaluated using the Risk of Bias in Non-Randomized Studies-of Interventions (ROBINS-I) scale, and randomized studies were evaluated using the Cochrane RoB 2.0 tool.10,11
Survey of Hand Surgeons
Following the systematic review of the literature, a survey was conducted to assess current postoperative dressings and immobilization protocols by hand surgeons in Canada.
The survey was first piloted in a small sample of McMaster University senior plastic surgery residents and staff to gather feedback. Using the Canadian Society of Plastic Surgeons 2016 Member Roster, all Canadian plastic surgeons who perform hand surgery were mailed a copy of the survey, a personalized cover letter explaining the purpose of the survey, and a return envelope. This study was exempt from ethics review by a research ethics officer. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all participants (surgeons) being included in the survey.
Data Analysis
All data from the systematic review and survey were summarized descriptively. Proportions and descriptive statistics were reported, where applicable.
Results
Systematic Review
Article selection
The database search identified 1598 articles, 51 of which underwent full-text review. Of these, 24 articles met inclusion criteria and were included in the review (see PRISMA flow diagram presented in Figure 1). Agreement between reviewers in the first review stage was substantial (kappa = 0.76), and almost perfect in the second stage (kappa = 0.81).
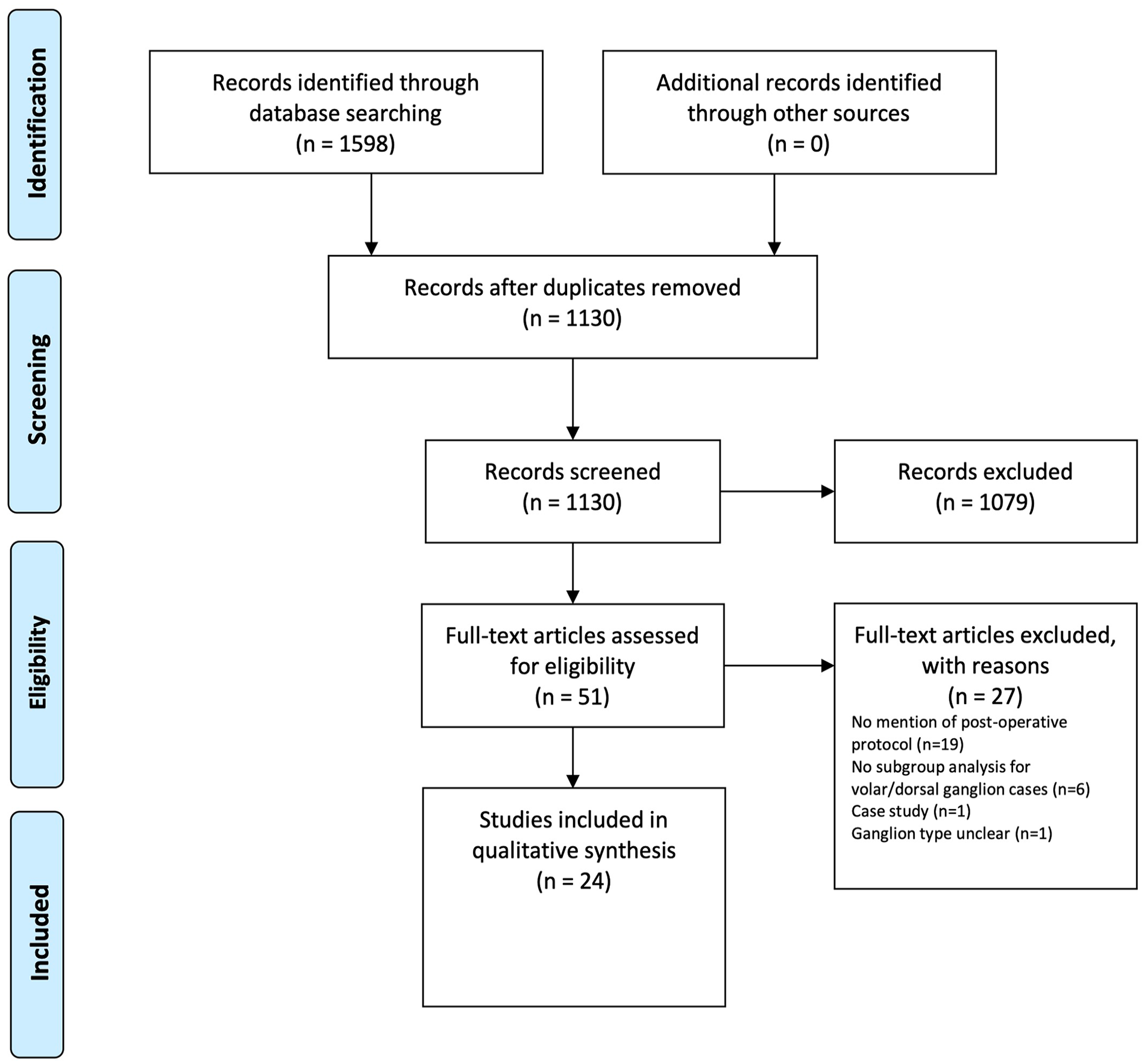
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram.
Characteristics of included studies
Of the articles included, 3 were RCTs and 21 were observational studies. Eleven studies involved open DWG excision (Table 1), 12 studies involved arthroscopic DWG excision (Table 2), and 1 study involved both open and arthroscopic DWG excision (Tables 1 and 2).
Summary of Studies (Open Dorsal Wrist Ganglion Excision).
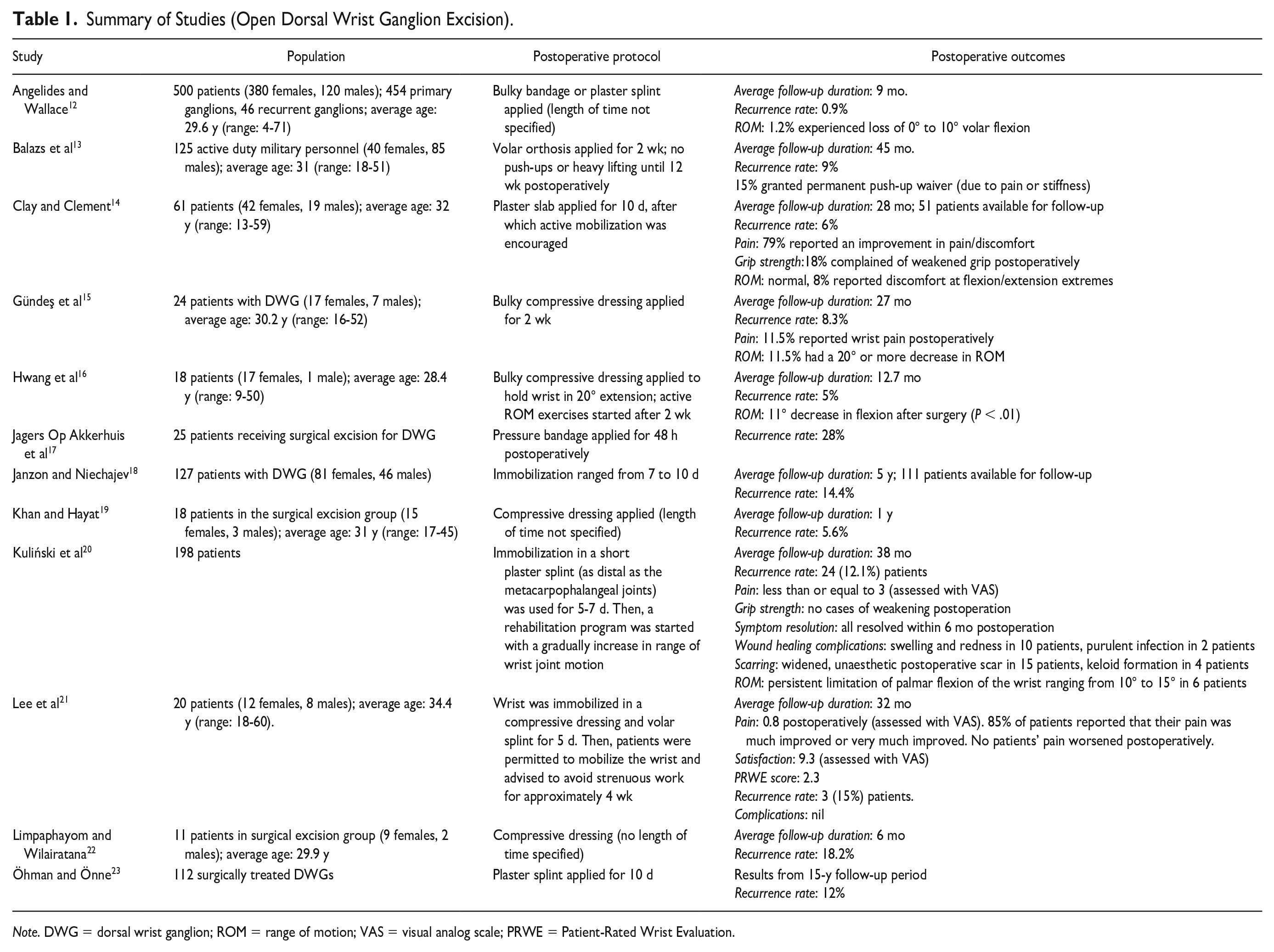
Note. DWG = dorsal wrist ganglion; ROM = range of motion; VAS = visual analog scale; PRWE = Patient-Rated Wrist Evaluation.
Summary of Studies (Arthroscopic Dorsal Wrist Ganglion Excision).
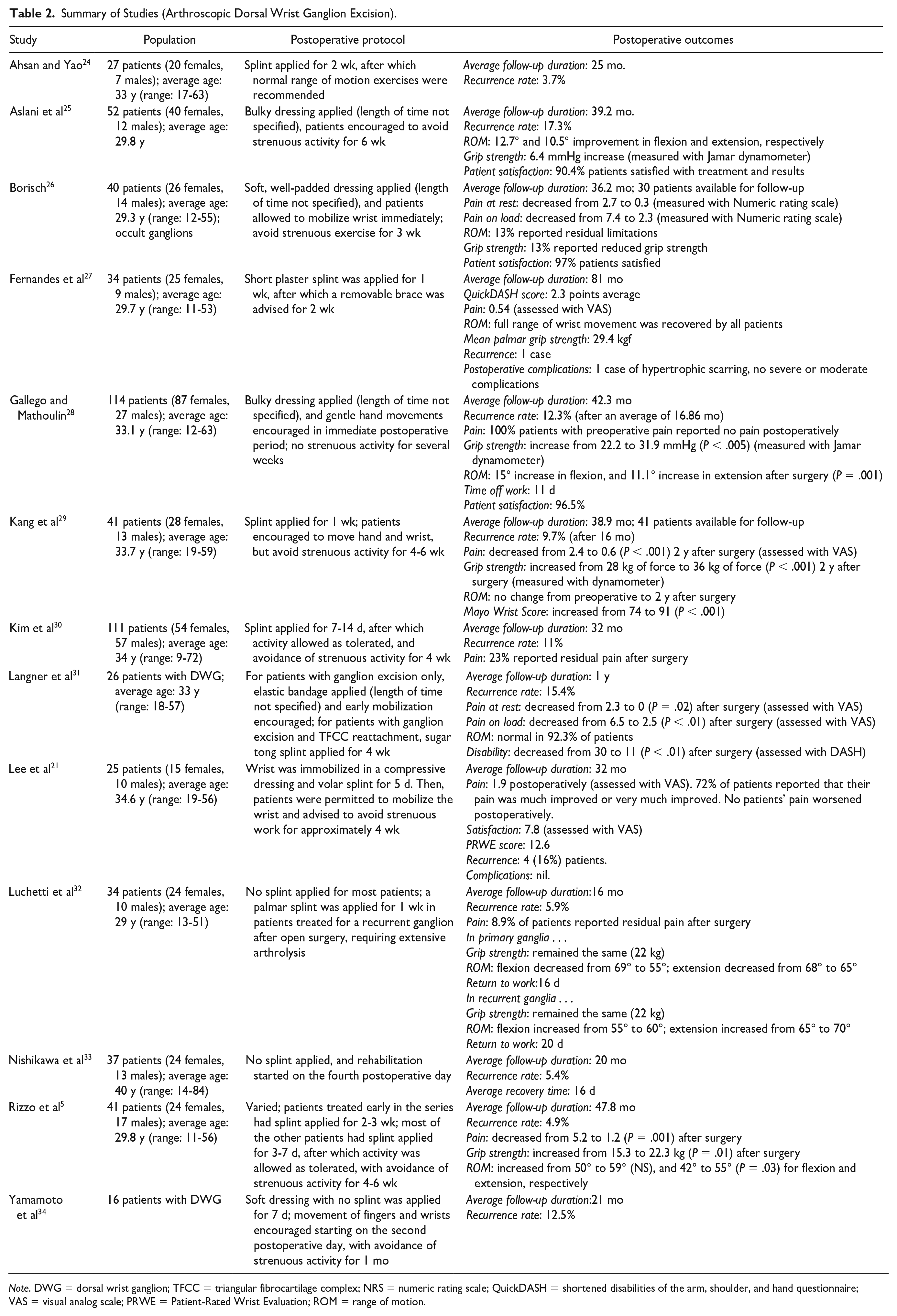
Note. DWG = dorsal wrist ganglion; TFCC = triangular fibrocartilage complex; NRS = numeric rating scale; QuickDASH = shortened disabilities of the arm, shoulder, and hand questionnaire; VAS = visual analog scale; PRWE = Patient-Rated Wrist Evaluation; ROM = range of motion.
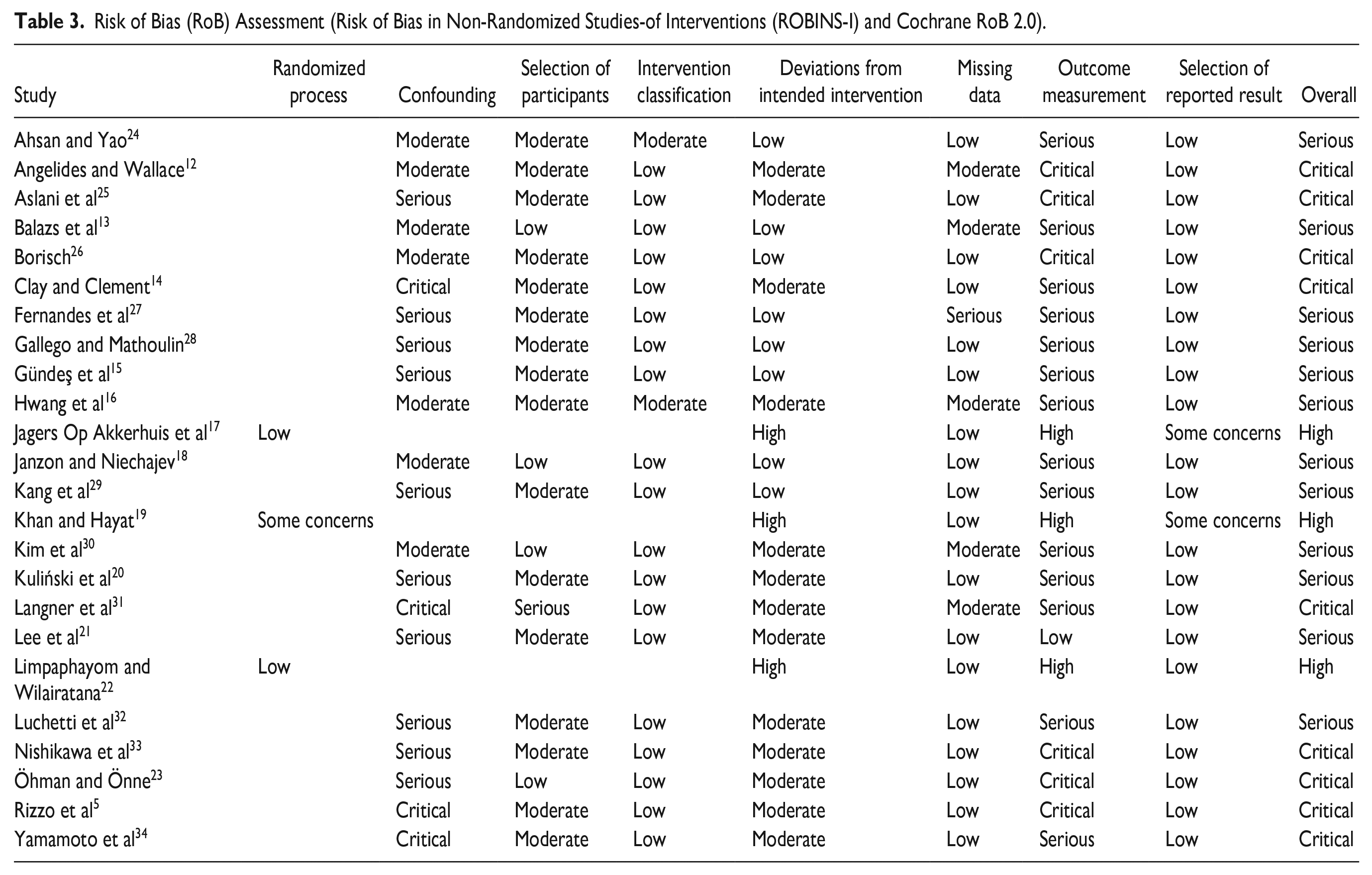
Included studies had a high degree of bias as evaluated by the ROBINS-I and Cochrane RoB 2.0 tools (Table 3).10,11 Of the 21 nonrandomized studies, 9 studies had critical and 12 studies had serious RoB. The 3 RCTs had high levels of bias related to the outcomes measured. The interreliability kappa score was 0.99 for RoB assessment.
Risk of Bias (RoB) Assessment (Risk of Bias in Non-Randomized Studies-of Interventions (ROBINS-I) and Cochrane RoB 2.0).
Open DWG excision
Of the 12 studies on open DWG excision (Table 1), 6 (50%) used rigid immobilization of the wrist with splinting, 5 (42%) used soft dressings with variability in allowed wrist movement due to pressure and bulk, and 1 (8%) used either. The limited mobility time ranged from 48 hours to 2 weeks, with 3 (25%) studies not specifying the exact length of time.
The follow-up duration ranged from 6 months to 15 years. Angelides and Wallace 12 reported the lowest ganglion recurrence rate of 0.9% after 9-month follow-up. The postoperative protocol involved a bulky bandage or plaster splint. However, the duration of the postoperative protocol was not specified. In contrast, Jagers Op Akkerhuis and colleagues 17 reported the highest recurrence rate (28%) in patients immobilized with a pressure bandage for 48 hours after DWG excision. The follow-up duration was not specified.
Arthroscopic DWG excision
Among the 13 studies on arthroscopic DWG excision (Table 2), 6 (46%) used rigid immobilization, 5 (39%) allowed some wrist movement, and 2 (15%) studies did not limit wrist movement. Of the studies that limited wrist mobility, the limited mobility time ranged from 5 days to 3 weeks, with 4 (31%) studies not specifying the exact length of time.
The patient follow-up duration ranged from 12 to 81 months. Fernandes and colleagues 27 presented the lowest recurrence rate of 2.9% after 81-month follow-up. In this study, a short plaster splint was applied for 1 week and followed by a removable brace for 2 weeks. The highest recurrence rate (17.3%) was reported by Aslani and colleagues 25 after 39.2-month follow-up. These authors used a bulky dressing for an unspecified length of time.
Patient outcomes
In general, functional outcomes were inconsistently reported in all included studies. Therefore, comparisons to determine the relative effectiveness of the various immobilization protocols were not possible.
In open DWG excision, Clay and Clement 14 postoperative protocol had the best outcomes for postoperative wrist range of motion. Patients’ wrists were immobilized in a plaster slab for 10 days postoperatively. “Normal” range of motion was restored for all 51 (100%) patients available for follow-up. Gündeş and colleagues 15 showed postoperative wrist range of motion was most severely reduced in patients immobilized with a bulky compressive dressing for 2 weeks. Specifically, in patients with a bulky compressive dressing, 11.5% of patients had a 20° or more decrease in range of motion. Lee and colleagues 21 reported the best improvement in pain, where 85% of patients reported that their pain was much improved or very much improved. These authors immobilized the wrist in a compressive dressing and volar splint for 5 days.
In terms of arthroscopic DWG excision, Fernandes and colleagues 27 reported the best outcomes for postoperative range of motion, with all patients recovering full range of motion using the previously described postoperative protocol. Luchetti and colleagues 32 reported a decrease in range of motion, with no splint applied postoperatively. Gallego and colleagues 28 had the best documented improvement in pain, where 100% of patients who experienced preoperative pain reported no postoperative pain. These patients were immobilized with a bulky dressing for an unspecified length of time. 28
Patient satisfaction was reported in 4 studies. Within the arthroscopic DWG excision group, when immobilized with a bulky dressing, high satisfaction rates were reported, ranging from 90.4% to 97%.25,26,28 However, Lee and colleagues 21 performed both open and arthroscopic DWG excision, immobilizing their patients with a compressive dressing and volar splint. Within this study, patient satisfaction was reported to be better in the open group (9.3 vs 7.8 using visual analog scale [VAS], P = .042). 21
Time to return to work was only reported in 2 studies, both of which were DWG that underwent arthroscopic excision.28,32 Patients immobilized with a bulky dressing for an unspecified period of time returned to work after 11 days, compared with 16 and 20 days in nonimmobilized patients with primary and recurrent ganglia, respectively.28,32
The lack of consistent outcome reporting made it impossible to make inferences about the effect of the immobilization protocols on grip strength.
Survey of Canadian Hand Surgeons
Of the 65 Canadian hand surgeons contacted, 22 completed the online survey (34%). For surgeons who fully immobilized the wrist postoperatively (45%; n = 10/22), the majority do so for 8 to 14 days (80%; n = 8/10). The most common dressing applied is a volar wrist splint (80%; n = 8/10) in 30° of extension or less (60%; n = 6/10). The most cited purpose of postoperative immobilization is for improving patient comfort (50%; n = 5/10). There were 2 exceptions to immobilization expressed in this surgeon group, including not splinting patients older than 70 years and not splinting patients with specific phobias related to wrist immobilization.
For the hand surgeons who did not immobilize the wrist postoperatively (55%; n = 12/22), most applied a soft dressing allowing full mobility (75%; n = 9/12), while others used a compression dressing (17%; n = 2/12), or a soft dressing permitting a limited range of motion of wrist (8%; n = 1/12). One surgeon noted that immobilization may be necessary should an incision and repair of the extensor retinaculum be required.
Discussion
The results of the systematic review highlight the lack of consensus amongst hand surgeons regarding the optimal postoperative care protocol in DWG excision patients. Although many of the included studies did employ some form of either rigid or limited immobilization, the type of dressing and the length of time for which it is applied are highly variable. Our survey of Canadian hand surgeons corroborates the highly variable practices of immobilization of the wrist after surgical excision of DWG. Interestingly, surveyed surgeons who did immobilize the wrist postoperatively most often limited the duration to 1 to 2 weeks, but never for more than 3 weeks. In contrast, many surgeons found no need for immobilization. The variability of postoperative immobilization has been documented in other areas of hand surgery, including carpal tunnel release. 35 Despite critical evaluation through 5 RCTs concluding that splinting following carpal tunnel release does not have an appreciable effect on postoperative outcomes, surgeons’ opinions and practices remain divided. As with other aspects of surgical practice, deciding upon a specific postoperative dressing can be influenced by personal experience or learned behaviors from mentors.
The resources necessary for a RCT is likely not indicated for our clinical question as both groups seemingly have overall very good outcomes but a core outcome set would allow even work done as a case series to potentially meaningfully answer this question through meta-analysis. There is inconsistent reporting of outcomes in the DWG literature. For example, range of motion, grip strength, and pain outcomes were reported as either a percentage of patients experiencing improvement, a percentage of patients with residual symptoms, or as a preoperative and postoperative score on a questionnaire or measuring tool. The variation in outcome reporting makes it difficult to amalgamate these results into a meta-analysis. As a result, although preliminary inferences can be made about the relative success of the immobilization protocols, the degree to which 1 protocol is better or worse than the other remains unclear, especially in the context of varying surgical techniques. This substantiates the need for standardized core outcomes, such as those being developed by the Core Outcomes in Effectiveness Trials initiative. 36
There are several limitations to our study. First, it is acknowledged that functional and patient-reported outcomes are influenced by not only postoperative care as we have studied but also surgical technique. Second, many included studies were observational in nature, with only 3 RCTs. Third, our survey results may be prone to selection bias.
Conclusion
This systematic review of the literature has revealed a paucity of evidence available to inform the decision of wrist immobilization following DWG excision, either open or arthroscopic. Similarly, a survey of Canadian hand surgeons demonstrates current practice variability in postoperative dressings. Together, the data presented suggest that limited immobilization of 2 weeks or less or no immobilization after surgery does not meaningfully affect patient outcome after surgery. To detect a difference, the cumulative power of primary studies that employ a similar set of core outcomes that include patient-reported outcomes is necessary.
Supplemental Material
sj-pdf-1-han-10.1177_15589447211014631 – Supplemental material for Immobilization of the Wrist After Dorsal Wrist Ganglion Excision: A Systematic Review and Survey of Current Practice
Supplemental material, sj-pdf-1-han-10.1177_15589447211014631 for Immobilization of the Wrist After Dorsal Wrist Ganglion Excision: A Systematic Review and Survey of Current Practice by Chloe R. Wong, Marta Karpinski, Alexandra C. Hatchell, Mark H. McRae, Jessica Murphy and Matthew C. McRae in HAND
Footnotes
Acknowledgements
Thank you to Laura Banfield, medical librarian at McMaster University, for assistance with search strategy and implementation. Thank you to Dr Achilles Thoma for guidance in performing the systematic review in methodologically rigorous fashion.
Supplemental material is available in the online version of the article.
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.