
Abstract
Keywords
Introduction
Distal radius fractures (DRFs) are common and account for 16% of all fractures seen in emergency departments (EDs). 1 Fractures of the radius and ulna account for 44% of those fractures seen in the EDs in all age groups. 2 They are frequently associated with falls in older populations. 3 Because the optimal treatment for a DRF remains an ongoing discussion and the duration of immobilization is still a subject of debate, this study observed whether early activity postinjury can lead to prevention of type 1 complex regional pain syndrome (CRPS-1),4-7 a syndrome that can lead to high health care costs and inability to work. 8
Type 1 complex regional pain syndrome is described as a posttraumatic pain syndrome combined with an autonomic disorder and includes excessive pain, edema, changes in skin blood flow, abnormal sudomotor activity, sensory and motor disturbances and severe disability leading to mood changes, loss of work capacity, and decreased participation in recreational activities.9,10 The diagnosis is based on a combination of symptoms reported by the patients and signs observed during physical examination by the physician. Type 1 complex regional pain syndrome can be diagnosed after 3 months, the normal healing time for most fractures. 10
According to the current literature, the incidence of CRPS-1 after nonoperatively treated DRFs ranges between 1% and 37%.11-14 The difference in incidence can be explained by the lack of standardized and reproducible diagnostic criteria.15,16 Harden et al validated the criteria to diagnose CRPS-1 at 3 months after the fracture, the so-called Budapest Criteria, which are now internationally accepted in clinical practice and research. By using these criteria, it was shown that in many patients diagnosed primarily with CRPS-1, an underlying alternative diagnosis such as arthrosis, avulsion fracture, malalignment, ulnar-sided wrist pain, or cellulitis could be made. 13
Concerning the treatment for CRPS-1, the perspectives on treatment options have changed. 17 National and international guidelines showed that drug treatment in patients with chronic CRPS-1 had limited effects. 18 After the introduction of several more cognitive and behavioral treatment methods, such as pain exposure in physical therapy (PEPT) and exposure in vivo, it appeared that disuse and kinesiophobia played an important role in the maintenance of CRPS-1.2,19-21
During a small proof-of-concept study, we tested the hypothesis that early mobilization and activation could prevent the appearance of CRPS-1. In a group of patients with nonoperatively treated DRFs, we introduced a home exercise program immediately after cast removal. The incidence of CRPS-1 was studied using the Budapest Diagnostic Criteria. A total of 56 patients with 57 fractures were included, and none was diagnosed with CRPS-1 after 3 months. This proof-of-concept study showed that the incidence of CRPS-1 may be positively influenced when early mobilization is stimulated.
The aim of this study was to observe the incidence of CRPS-1 in a larger group of patients with nonoperatively treated DRFs combined with an early mobilization protocol 2 months or more after fracture.
Materials and Methods
Study Protocol
This clinical observation study was designed as a continuation of the proof-of-concept cohort study, which was started in December 2012. The study was performed between December 2012 and July 2017 in a level 1 trauma center in the Netherlands. The local ethical committee approved the study (NL2014-1361).
Participants
Adult patients (age >18 years) who were undergoing nonoperative treatment for a DRF were asked to participate in this study by their physicians. Patients predisposed to unreliably answering questions due to intellectual or language problems were excluded. Patients who gave informed consent received, after fracture reduction and plaster cast immobilization, an information leaflet with instructions for a home exercise program and an explanation about the role of pain. Moreover, they were informed that they would be approached for a telephone interview after at least 2 to 3 months following the fracture. When necessary, patients were invited for a visit to the outpatient clinic.
Clinical Treatment Procedure
The Orthopaedic Trauma Association (OTA) system was used for the classification of DRFs. After removal of the plaster cast (after 4-6 weeks of plaster cast immobilization), patients were taught how to exercise their fingers, forearm, and wrist. They were allowed to resume normal activities, gradually increasing the amount of weight and force the affected arm and wrist used, based on the expected course of fracture healing explained by the home exercise leaflet (Figure 1). The instructions instructed the patients on the importance of using and safely strengthening the arm and/or wrist for proper healing of the fracture and for optimizing arm-hand function. The patients were strictly instructed to perform all exercises on a daily basis at home as soon as possible for a 6-week period.
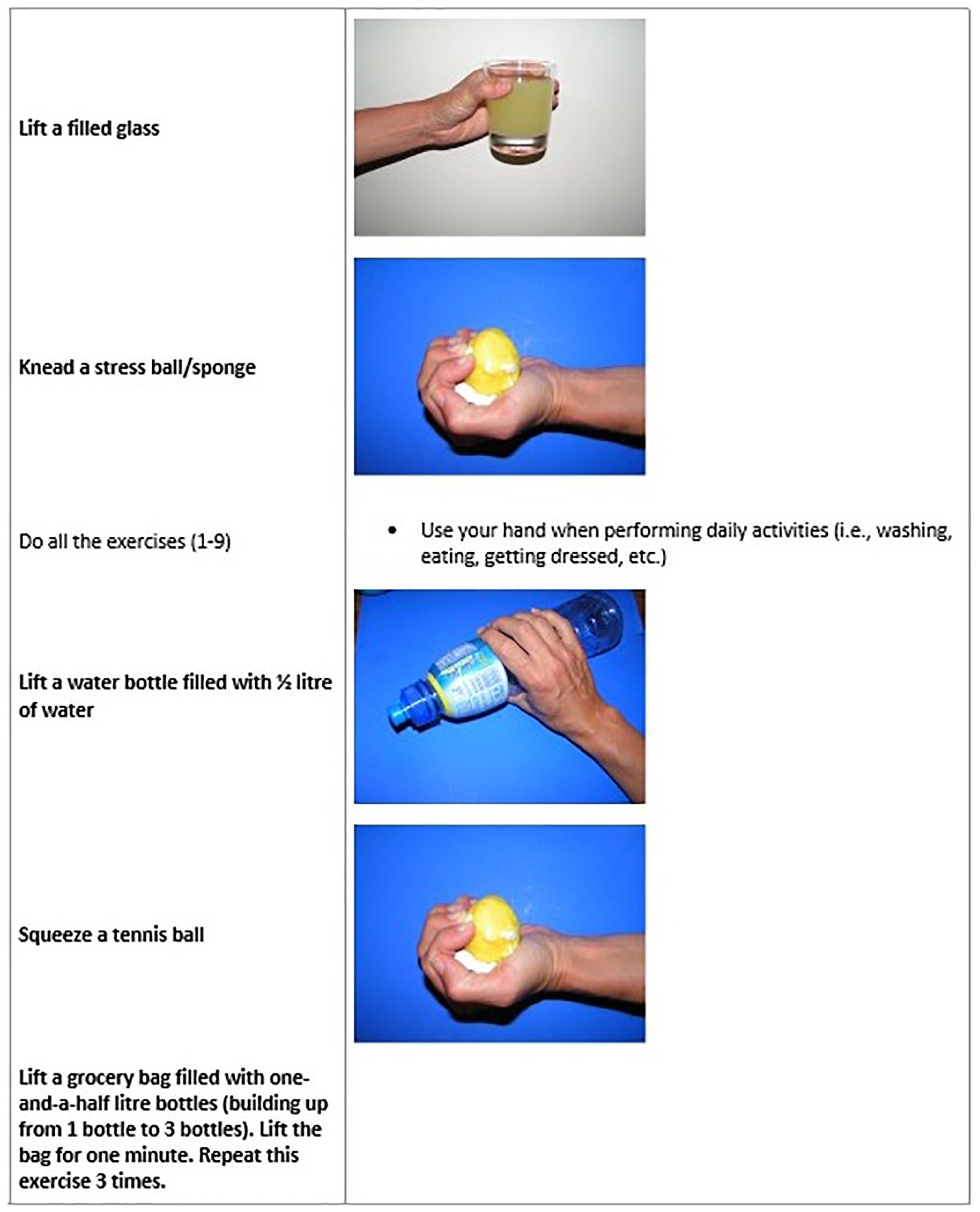
Example of a page from the instruction leaflet (English version). In this leaflet, the home exercise program is explained. Patients need to perform the exercises every day, and the exercises are intensified over the 3 months.
Measurements
After a minimum of 2 months following the fracture, the patients were interviewed by the attending physician/researcher by telephone. Compliance with the exercise program was evaluated by a telephone interview using the question, “Have you been performing all the exercises from the instruction leaflet?” The telephone interview focused on the presence of disproportionate pain, and the subjective items of the Budapest Diagnostic Criteria for CRPS-1 were scored by the interviewer (Figure 2). 10 Patients were scored positively on the subjective items of the Budapest Diagnostic Criteria when they answered “yes” for the first question and when they answered “yes” for 1 or more of the other questions (Figure 2). These patients were invited to visit the specialized CRPS-1 outpatient clinic of Radboudumc. During the consultation at the outpatient clinic, an experienced clinician assessed the objective symptoms of the Budapest Criteria (signs), and a radiography of the wrist was performed to establish a diagnosis (Table 1).
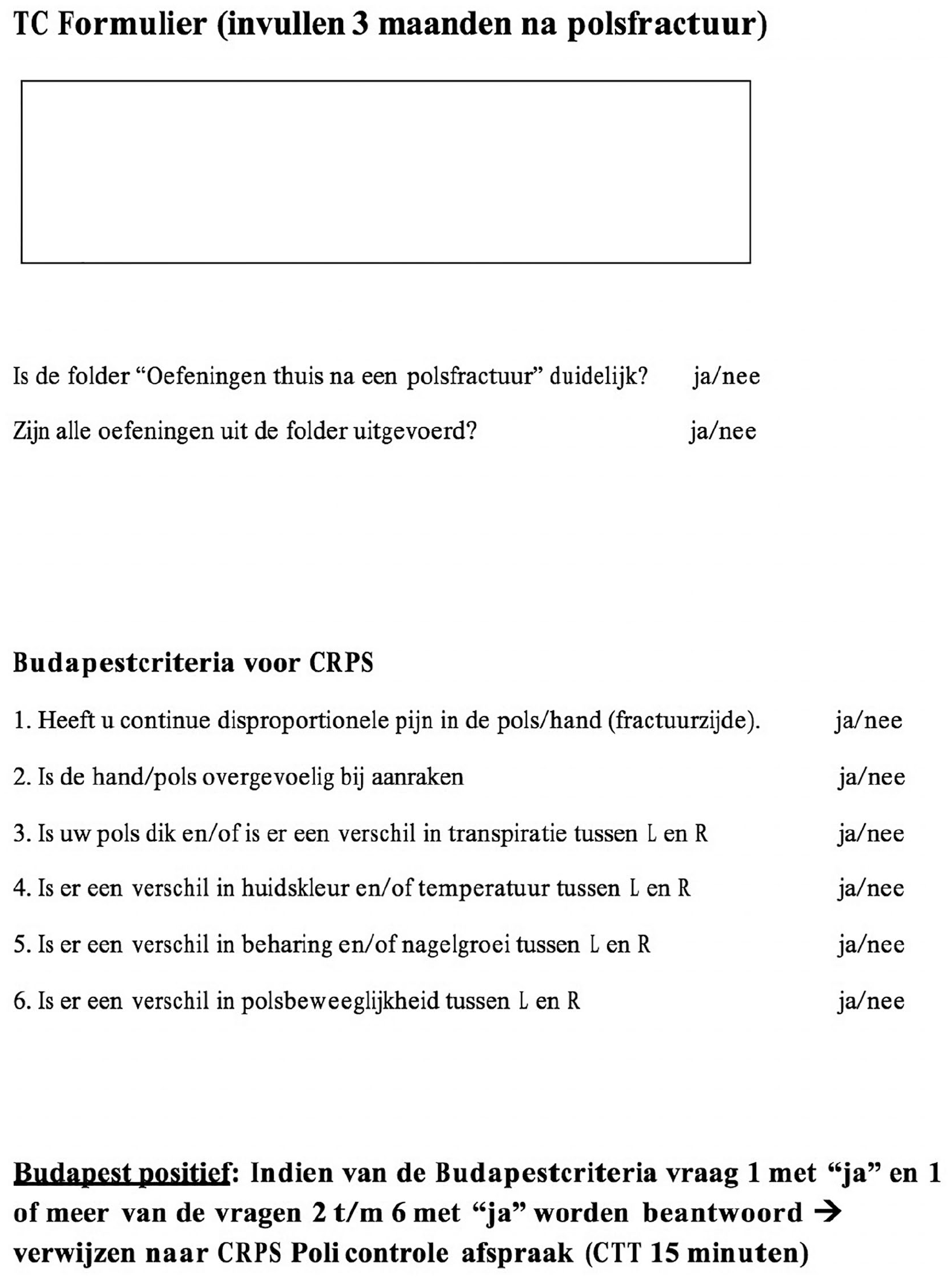
The subjective items of the Budapest Criteria are shown. These items were used to score the patients during the telephone interview. The items are translated to Dutch.
Budapest Diagnostic Criteria for CRPS-1.
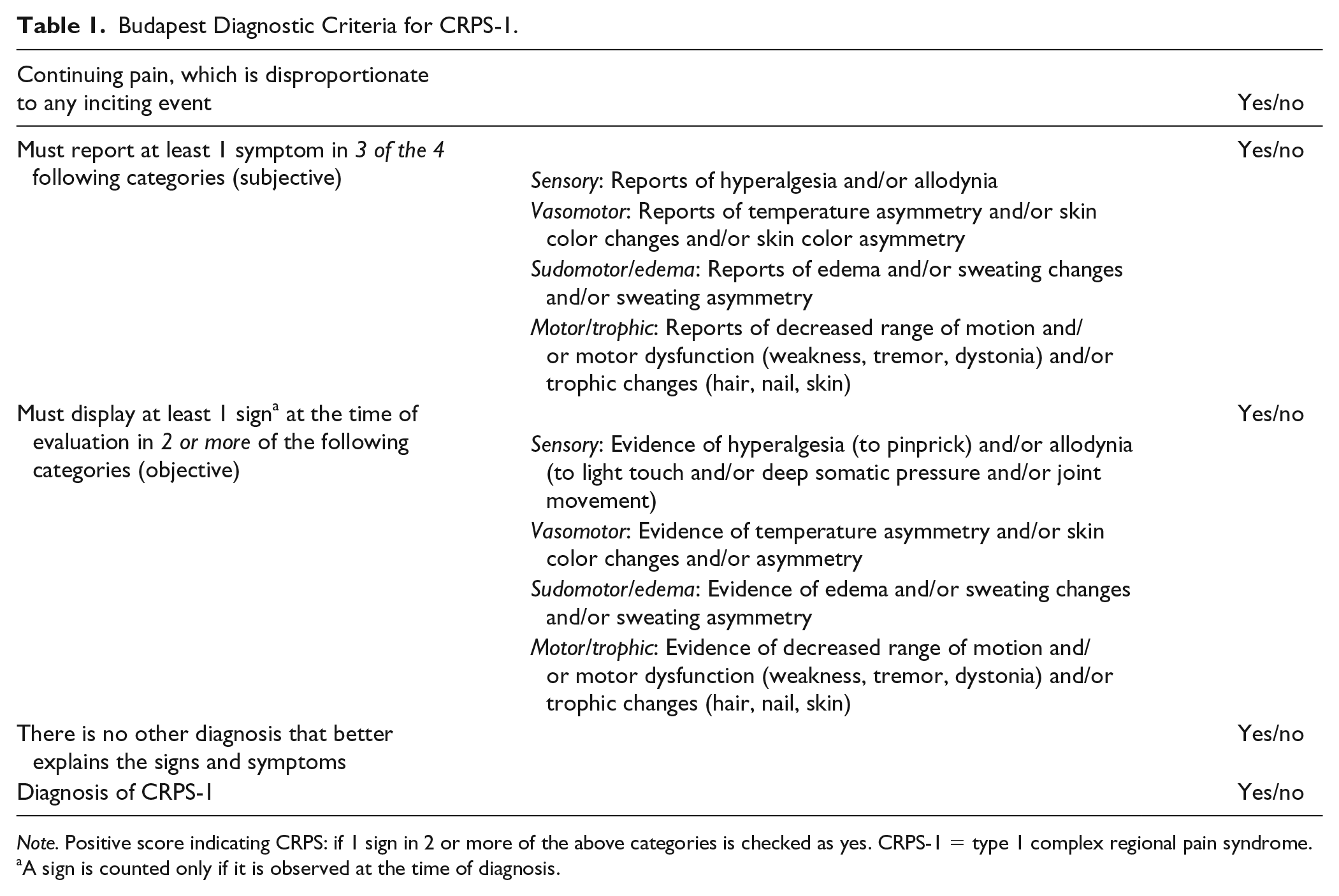
Note. Positive score indicating CRPS: if 1 sign in 2 or more of the above categories is checked as yes. CRPS-1 = type 1 complex regional pain syndrome.
A sign is counted only if it is observed at the time of diagnosis.
Variables that could potentially be associated with the occurrence of pain and CRPS-1, for example, age, sex, classification of the fracture (OTA classification), side of the fracture (left or right arm), and complaints during the cast period, were obtained from the patient’s medical file and during the potential CRPS outpatient clinic visit.
Sample Size Calculation
A priori power analysis indicated that a sample of 134 patients would provide 80% statistical power (β = .20; α = .05) to detect a difference in the incidence of CRPS-1 of 7%, 1% for the expected incidence of the study population and 8% for the incidence based on the mean incidence in the literature.11-13
To account for a 10% loss to follow-up, we aimed to enroll 148 patients.
Statistical Analysis
The continuous variables were described using means and standard deviations, and categorical variables were described using absolute numbers with percentages. To assess differences in descriptive results between the included patients and the dropout patients, we used a χ2 test for the dichotomous and nominal variables and a t test for the continuous variable.
The primary outcome was defined as the incidence of CRPS-1 diagnosed at the CRPS-1 outpatient clinic. The secondary outcomes were diagnoses other than CRPS-1 and the incidence of disproportionate pain. The incidence of CRPS-1 was calculated by the number of patients with CRPS-1 divided by the total number of patients. The 95% confidence interval (CI) was calculated from the CRPS-1 incidence. The results and CIs in this study were compared with the incidences and CIs reported in the literature of CRPS-1 after a DRF treated with plaster cast immobilization.
A multivariate logistic regression analysis was performed to investigate whether different patient characteristics influenced the incidence of CRPS-1.
Results
Patient Characteristics
Of the 375 patients with a wrist fracture treated between December 2012 and July 2017, 165 patients were eligible and were willing to participate in the study (Figure 3).
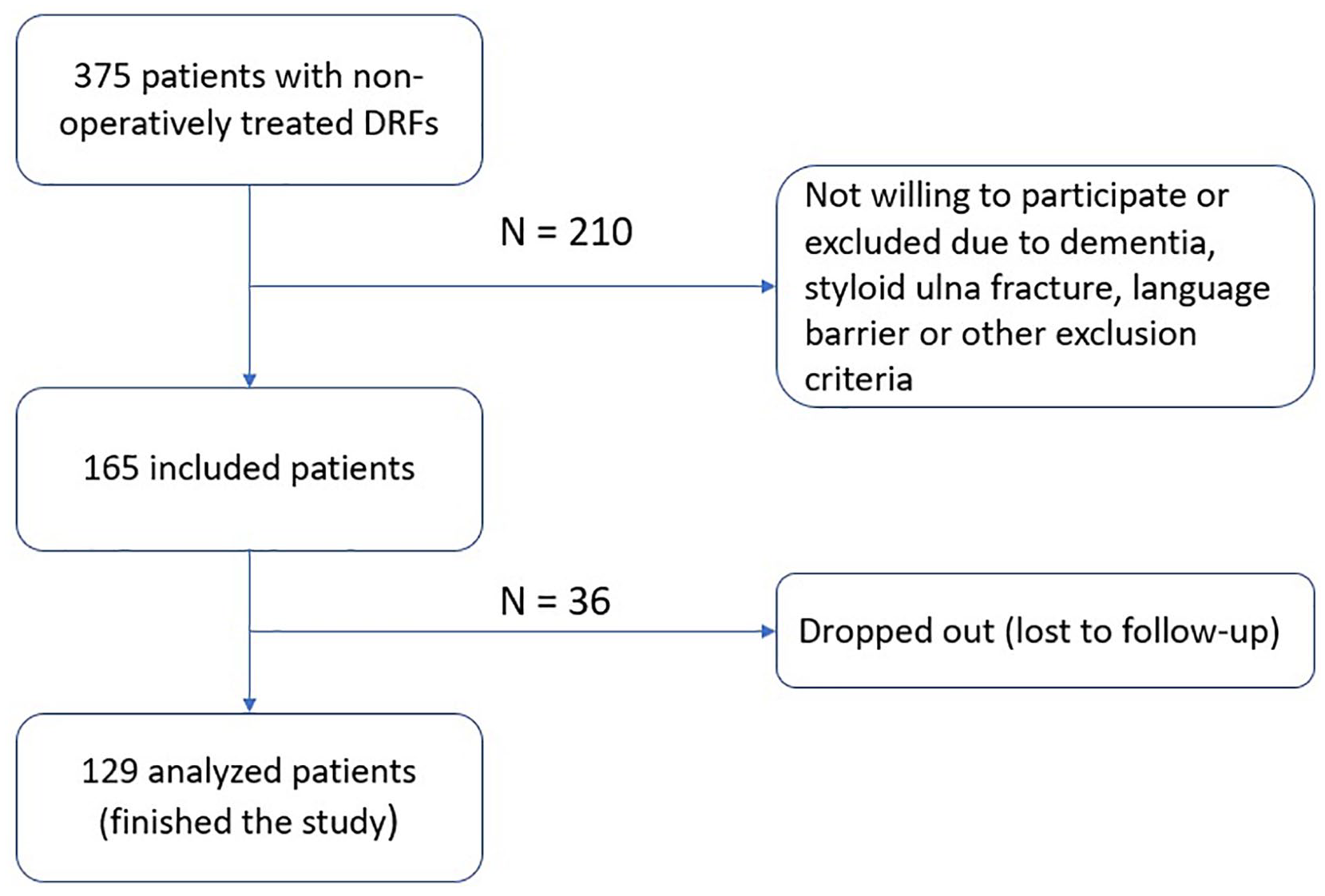
A flowchart of the process of the included patients and the excluded and dropout patients.
We enrolled 165 patients with DRFs. Of these 165 patients, 36 (22%) could not be reached by telephone. Thus a total of 129 patients with 131 fractures (2 patients had a bilateral fracture) were included in the study. Patients were called after a minimum of 2 months postinjury. The mean time for calling patients for a follow-up (time between removing the cast and first follow-up with telephone interview) was 14 months (range, 2-36 months; median, 13 months). Twelve patients were seen at the outpatient clinic, and all of them were seen after 3 months postinjury.
The baseline characteristics of the included patients are shown in Table 2. The mean age was 59 (SD = 17.71) years, and 77.5% of the patients were women. Of the 131 fractures, 75 (57.3%) were on the left side, 55 patients had a type 23A fracture (42%), 24 had a type 23B fracture (18.3%), and 52 had a type 23C fracture (39.7%). During the plaster cast immobilization period, 22 (16.8%) patients complained of pain. According to the patients’ replies during the telephone interviews, compliance with the exercise program was 100%.
Patient Characteristics of the Included and Dropout Patients.
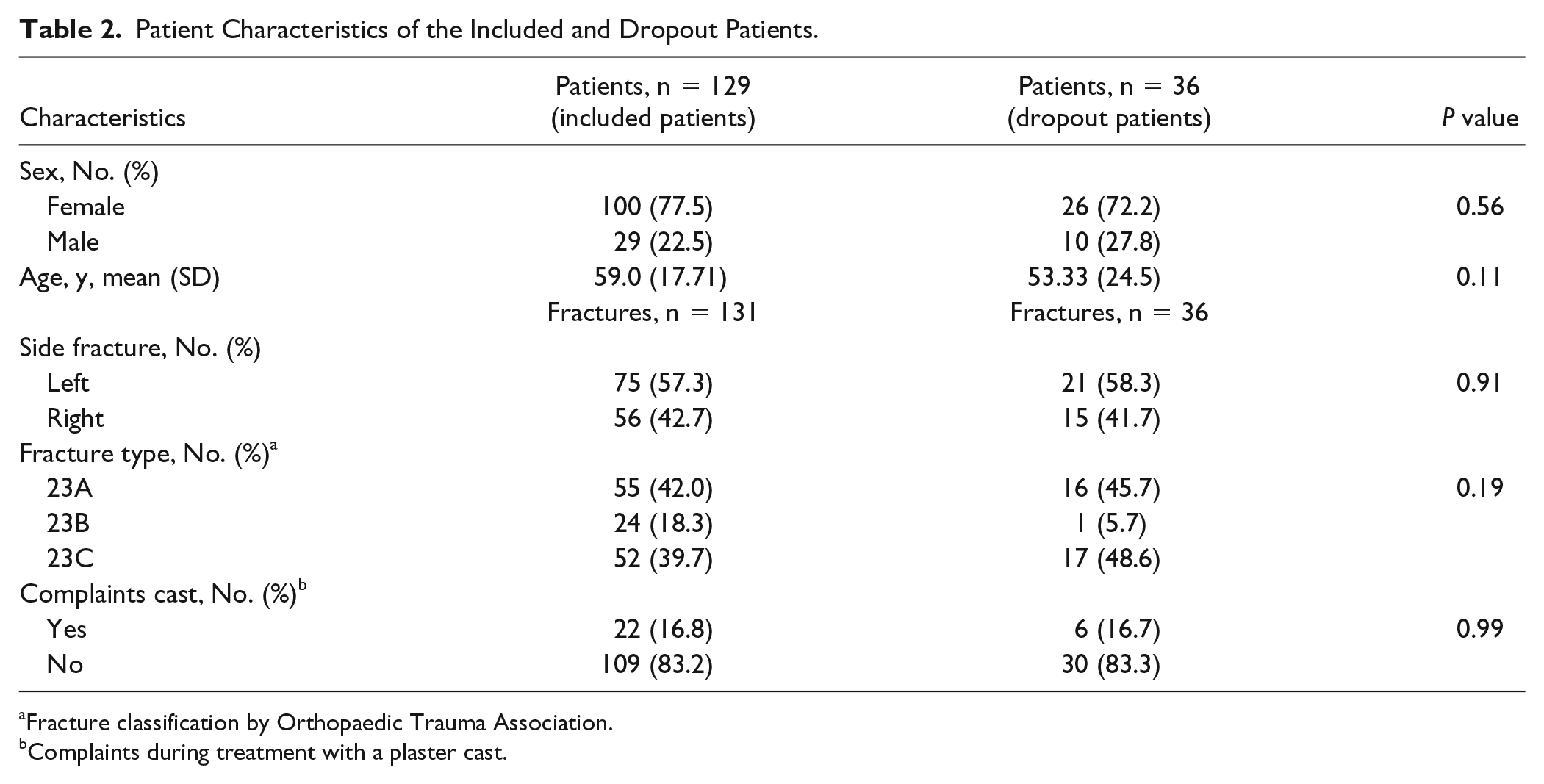
Fracture classification by Orthopaedic Trauma Association.
Complaints during treatment with a plaster cast.
The characteristics of the dropout patients (ie, patients who could not be reached by telephone) were not significantly different compared with the characteristics of the included patients, as shown in Table 2.
Incidence of CRPS-1
Of the 129 patients, 117 (89%) did not report disproportionate pain during the telephone interview, whereas 12 patients (9.2%) reported disproportionate pain and were positive for the subjective Budapest Diagnostic Criteria. During the outpatient visit, none of the 12 patients were diagnosed with CRPS-1 when the objective symptoms of the Budapest Criteria were assessed, resulting in a CRPS-1 incidence of 0% (95% CI, 0.00-0.028).
Of the 12 patients who were seen in the outpatient clinic, 2 patients were diagnosed with arthrosis (1 preexistent hand arthrosis, 1 thumb arthrosis), 5 with malunion, and 1 with carpal tunnel syndrome. In 4 patients, the pain was associated with stiffness in the hand and wrist. These 12 patients were called approximately 5.5 months postinjury.
Discussion
In this study, we observed no patients with CRPS-1 when using an active approach, including a home exercise program started immediately after a nonoperatively treated DRF. Twelve (9.2%) patients had disproportionate pain and scored positive on the subjective items of the Budapest Diagnostic Criteria during a telephone interview. None of these 12 patients were diagnosed with CRPS-1 during an outpatient visit more than 3 months postinjury. In 8 patients, an underlying diagnosis could be found, whereas in 4 patients, the pain was associated with stiffness in the hand and wrist. Therefore, we agree with Teunis et al 22 that CRPS-1 is less common than expected and that to eradicate the stigma on CRPS-1, it is advisable to describe the disproportionate pain and rule out possible existing disability.
Type 1 complex regional pain syndrome is characterized by excessive pain, edema, changes in skin blood flow, and abnormal sudomotor activity after excluding other more common causes of these signs and symptoms. 10 Despite extensive research, the exact mechanism of the pathophysiology of CRPS-1 remains unclear. Recent literature shows that CRPS-1 should be seen as a multifactorial disease after injury (upper or lower extremity injuries).13,19,22,23 As it is difficult to provide an effective treatment, it might be important to seek recent evidence for possible factors that are correlated with the onset and possible prevention of CRPS-1. Catastrophic thinking, cast tightness, level of education, disuse, and higher pain intensity are examples of factors correlated with a higher incidence of CRPS-1 after wrist fractures.22,24-26 Terkelsen et al 23 showed that even in healthy volunteers, immobilization of an upper extremity with a plaster cast for 4 weeks causes transient changes in skin temperature, mechanosensitivity, and thermosensitivity. In line with the study of Terkelsen et al, it seems highly likely that immobility and disuse can be an important factor in the development of CRPS-1 (including disproportionate pain) after a DRF. One way to treat these symptoms and prevent disuse is PEPT. Pain exposure in physical therapy was developed as a countermeasure for disuse and pain-avoidance behavior. It is based on the assumption that behavioral and psychological factors can exacerbate pain and dysfunction. It was shown to be a good and cost-effective treatment for patients with CRPS-1 in the upper or lower extremity.19,27-30
In addition to disuse, catastrophic thinking (ie, negative beliefs about pain leading to an overprotective response) is another factor that can lead to disproportionate pain and CRPS-1 after a fracture. Catastrophic thinking has often been correlated with chronic pain, disuse, and CRPS-1. 24 If it remains unnoticed, it can lead to fear and avoidance of activity and disuse, which in turn causes stiffness and skin changes (eg, swelling, shiny skin, and changes in hair patterns). 26 In this study, we did not measure the tendency for catastrophic thinking. In future studies, this should be studied in the outpatient clinic using the Pain Catastrophizing Scale, Short Form (PCS-4). 31 Patients who are prone to catastrophic thinking, as determined by the PCS-4, should receive an extra follow-up and better explanations for their pain complaints, possibly combined with additional care by a physical therapist.
Finally, a wait-and-see policy is important. In our study, we observed that patients who had disproportionate pain were called after approximately 5.5 months. In comparison with the mean of this study, which was 14 months, these patients were called quite early. It seems that symptoms of disproportionate pain and CRPS-1–like symptoms will disappear but require a longer period than 3 months. As mentioned in the validation of the Budapest Diagnostic Criteria, CRPS-1 can only be diagnosed after 3 months postinjury. 10 However, as seen in our study, after 3 months, CRPS-1–like symptoms could still be present. Patients should, however, receive an adequate explanation for these pain complaints and instructions about how to address them.
Taken together, this study and previous literature show that by describing CRPS-1 as a normal variation of the healing process after a traumatic injury and treating these multifactorial symptoms with a treatment focused on physical symptoms, and social and psychological factors, fewer people will suffer from the debilitating syndrome CRPS-1, and more people will receive adequate treatment. Most importantly, the stigma associated with CRPS-1 and the severity of the disease it represents can be changed.
This study has several limitations. First, we eventually had a lower number of participants than suggested by the power analysis calculation: 129 patients and 131 fractures available for the analysis instead of 134 patients and fractures. Second, a telephone interview may result in an underestimation or overestimation of CRPS-1 prevalence. However, a telephone interview as a screening tool for CRPS-1 in patients with a wrist fracture is an accepted method, and little discrepancy was found between the telephone interview and the in-person assessments.32,33 Third, a selection and motivation bias might have influenced the results. Of the 375 patients, 165 were eligible for this study and were enrolled. It could have been the case that the most motivated patients agreed to participate in this study. Fourth, 36 patients (22%) dropped out because we could not reach them for telephone interviews. The descriptive analysis of these dropout patients was not different from the included patients; therefore, we do not expect this created bias. Fifth, the mean time for the follow-up interview was 14 months postinjury. As shown in this study, patients with disproportionate pain were diagnosed with an underlying alternative diagnosis or were associated with hand and wrist stiffness but eventually recovered without CRPS-1. Therefore, we think that contacting these patients after an average of 14 months will not have created bias. It also showed us that even after more than a year, disproportionate pain symptoms may disappear and patients can have good functional outcomes. Sixth, we measured 100% compliance with the home exercise program. However, we do not know whether patients actually performed all the exercises and how strictly they adhered to the exercise program (ie, frequency, proper form). In addition, it is not clear what the exact influence of the instructions and exercise program was on the increase in early mobilization. Seventh, the specificity of the CRPS-1 diagnosis remains difficult. There is no criterion standard for diagnosing CRPS-1, which limits the results. We used the CRPS-1 diagnostic criteria based on the most recent CRPS-1 diagnosis consensus meeting in Budapest. 10 These criteria have the highest sensitivity (0.99) and specificity (0.68) and are generally accepted as the first choice for diagnosing CRPS-1 in research projects.10,12,16 In addition, the Budapest Criteria have been used in the CRPS-1 outpatient clinic at Radboudumc for several years and are well known by the clinic’s physicians. Based on these advantages, we chose to use the Budapest Criteria.
Conclusion
The incidence of CRPS-1 after a nonoperatively treated DRF was zero in this study. A more active treatment approach seems to lower the incidence of CRPS-1. We should stop stigmatizing CRPS-1 as a severe chronic disease that is debilitating but consider it as a posttraumatic symptom that can be treated adequately. The symptoms, which can be seen after a traumatic injury, are common 3 months after a DRF and require multifactorial treatment. The first steps are the following: informing the patient properly, managing the patient’s expectations for the upcoming year, and preventing disuse with a prompt and active home exercise program. If disproportionate pain is still present after 3 to 5 months, other causes should be excluded. When these are not found, CRPS-1–like symptoms can be accepted for up to 12 months while keeping psychological aspects in mind. However, a prospective study with a standardized mobilization program is needed to investigate the exact influence of an active treatment approach.
Footnotes
Acknowledgements
The authors thank Dr R. van Dongen for reviewing this article.
Ethical Approval
This study received approval from the local ethics committee of the RadboudUmc, Nijmegen (NL2014-1361).
Statement of Human and Animal Rights
This study has been performed in accordance with the ethical standards in the 1975 Declaration of Helsinki, as revised in 2008. This study has been carried out in accordance with relevant regulations of the US Health Insurance Portability and Accountability Act (HIPAA).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.