
Abstract
Concussion rates are commonly reported in high school and National Collegiate Athletics Association (NCAA) sports. Given that participation in collegiate recreation is on the rise, institutions should examine concussion rates within their recreational programs. We, therefore, retrospectively examined a recreational department's injury reports establishing concussion rates across (n = 16) club and (n = 10) intramural sports at a public university in the southeastern United States from 2016 to 2019. One hundred and thirty-five concussions (club n = 56; intramural n = 79) were identified and constituted 12.4% of documented injuries (n = 1,088). The intramural concussion rate was 0.57 per 1,000 athletic exposures (AEs) and AE was greatest in outdoor soccer (0.99 per 1,000 AE). Therefore, our data suggests an increased incidence of concussions in intramurals compared to published rates in NCAA and high school sports. Collegiate recreational departments should consider these concussion rates when formulating risk management strategies.
Introduction
Interest and participation in recreational sports have risen, with an estimated 8.1 million students participating at National Intramural and Recreational Sports Association (NIRSA) member institutions across the United States and Canada (Granholm, 2023). NIRSA estimates, however, may underscore total participation as estimates do not extend to and include institutions without membership. Regardless of NIRSA status, collegiate recreation departments may offer upwards of 40 + intramural sports (e.g., flag football, indoor soccer, and basketball) and 50 + club sports (e.g., rugby, ultimate frisbee, and lacrosse), with each competing in separate leagues and under governance by unique regulatory bodies (Copp et al., 2017; Lifschutz, 2012; Lower-Hoppe et al., 2021; Stier et al., 2008). Intramural sports have provided students an opportunity to participate in intracampus competitions (Copp et al., 2017). Club sports provide a more formalized alternative for students to compete between institutions (Lifschutz, 2012). Collegiate recreation can serve as the highest level of competition for a collegiate sport when an institution does not offer a varsity counterpart (e.g., Quadball (Quidditch), ultimate frisbee, and water polo) (Stier et al., 2008).
Despite similar sports offerings club and intramural sports are severely underserved compared to high school and collegiate varsity levels. Intramural and club sports are often student-led organizations operating with limited institutional oversight and funding for access to standardized medical supervision (Lifschutz, 2012; Lower-Hoppe et al., 2020; Schneider et al., 2008). Executive boards overseeing clubs are often comprised of students. Students, therefore, are responsible for the club's operations, including but not limited to practice arrangements, competition scheduling, fundraising, and team travel (Warner et al., 2012). Unfortunately, as a student-guided and directed organization, medical care is often outside the feasible budgetary scope (Lifschutz, 2012; Lower-Hoppe et al., 2020; Schneider et al., 2008). If an injury has occurred during practice or competition, the coaching staff, without sufficient expertise, are ultimately responsible for assessing and determining whether the participant returns to play (Beidler et al., 2018). Consequently, the concussed student and their peers (e.g., teammates), in addition to volunteers and untrained staff (e.g., facility staff, referees, and scorekeepers), are vulnerable and, by default, proximally responsible for recognizing injuries and facilitating early injury management.
Despite rising participation in recreational clubs and intramural sports, the available injury data for these programs are limited. Published data is often constrained to a single institution because recreational sports do not share a common injury surveillance database (Lifschutz, 2012; Schneider et al., 2008; Stier et al., 2008). Among the available data, Morogiello et al. (2023) examined injuries to participants in indoor and outdoor collegiate recreation over a four-year period. Morogiello et al. (2023) included all injuries reported to the collegiate recreation-affiliated athletic training clinic and found, in addition to informal recreation (e.g., free play), intramural and club sports participation to result in the most injuries among the institution's recreational programming. In addition to circumstances where first aid was administered, musculoskeletal injuries and concussive injuries were most documented (Morogiello et al., 2023). McElveen et al. (2014) observed that floor hockey, soccer, basketball, and softball constituted the highest intramural injury rates at their respective institution. Others have quantified injury incidence, where the incidence rate is the number of injuries divided by the number of athlete exposures (AEs) and is based on the epidemiologic concept of person-time at risk (Knowles et al., 2006). Arthur-Banning et al. (2018) reported intramural sports to have 10.28 injuries per 1,000 AE. Intramural AE was surpassed by club sports (18.3 injuries per 1,000 AE) and notably club sports had a greater injury incidence than varsity participation (13.79 per 1,000 AEs) at the National Collegiate Athletics Association (NCAA) level (Arthur-Banning et al., 2018). While these studies provide generalized insight, concussion rates, and incidence are not provided.
Concussions are at the forefront of public health concerns. Most recently, research has focused on the identification, management, and treatment of concussions (Coxe et al., 2020). Conn et al. (2003) outlined that 3.7 million sports and recreation injuries required emergency room visits annually with 2.6 million of these visits among persons aged 5–25 years old. Concussions constituted 17.2% of the 1.1 million localized to the head or the neck region. More recently, Gaw and Zonfrillo (2016) determined that 30% of the reported 2 million concussions were associated with participation in generalized sports or recreational activity. Previous research has outlined that concussions have accounted for 8.9% (high school) and 5.8% (varsity collegiate) of all athletic injuries (Gessel et al., 2007). While it may be assumed that concussive incidence rates would present similarly to those at the high school and collegiate level, limited research suggests that club sports may result in a higher overall injury incidence than NCAA sports (Schneider et al., 2008). Increased injury incidence creates a need for the injury to be reported to appropriate medical personnel to provide appropriate evaluation and management.
Collegiate athletes who delayed receiving immediate care due to delayed reporting missed an average of five more days of sports activity than those who were removed from play immediately (Asken et al., 2016). Individuals who do not report their concussive injury directly after the incidence are at a larger risk for additional problems and poor recovery outcomes. Although general surveillance information regarding concussions is more widespread, less is understood concerning surveillance, trends, and effects within the recreational community (Bartley et al., 2017).
Concussions in club sports are of increasing concern when considering the lack of institutional oversight and the limited number of sports medicine staff dedicated to collegiate recreation (Lifschutz, 2012). Therefore, the primary purpose of this study was to report epidemiological data on concussions in intramural and club sports within a Division I recreation department. Secondarily, we aimed to establish incidence rates (IRs) of concussions per AE in intramural sports.
Methods
This study retrospectively reviewed club and intramural sports injury reports from 2016 to 2019 at an NCAA Division I University in the Southeastern United States. Injury reports were part of the recreation department's preexisting protocol, which, outside the scope of the current work, is reported to the University as part of risk management guidelines. Injury reports were completed postinjury and on-site by certified athletic trainers (AT) and recreation department staff certified as first responders.
Following approval from the University's institutional review board, we retrospectively reviewed paper injury reports (2016–2017) and electronic records (2018–2019) (Connect2, Lorensberg Ltd., New York, NY, USA). A total of (n = 1,849) injuries were documented across the recreation department's six programs (i.e., informal recreation, general fitness, aquatics, adventure activities, intramural sports, and club sports). Injury reports were excluded if: (a) the report failed to include diagnosis or did not distinguish the intramural or club sport programs (n = 37), (b) the injury was the result of classwork (e.g., physical education class) or the injured was a bystander not participating in club or intramural sport (n = 85), (c) the injury occurred off-site (n = 7), or injuries were to external community members not affiliated with the university and occurred during facility rental (n = 4) and, (d) injuries sustained were occupational not from participating in club or intramural sports (e.g., employees and staff) (n = 36). Injury reports were retained for analysis if the documented injury was due to participation in club or intramural sport and received medical attention from the AT. Therefore, a subsequent database was established for intramural and club sport data (n = 1,088). Included injury reports were reviewed and vetted by ATs that de-identified data and categorized injuries by self-reported sex, sport type, and diagnosis. Incidence rates were calculated as the number of concussion injuries per 1,000 athletic exposures for intramural sports. An AE was defined as one athlete participating in one intramural event in which they were exposed to the possibility of injury, regardless of the time associated with that participation (Dick et al., 2007; Morogiello et al., 2023). Intramural IRs were compared yearly and between sports by the respective percentages of concussive injury, calculated ([concussions/total injuries] × 100%). Data were analyzed using Microsoft Excel (Microsoft Corporation, Redmond, WA). We were unable to calculate IRs for club sports as practice and competitions were often held off-campus, and, as a result, AE was not well documented or not reported to the recreation department by the club.
Results
A total of 1,088 participants (n = 740 males, n = 342 females, and n = 6 who did not report sex) sustained injuries resulting in injury reports between 2016 and 2019. Intramurals accounted for 68.2% (n = 742) of total injuries, whereas 31.8% originated from participation in club sports (n = 346). Ninety-seven participants required first aid, and (n = 36) had generalized (i.e., nonconcussive and nonmusculoskeletal) medical concerns. Two injury reports did not meet the above criteria (e.g., participants injured their heads but returned to play with no further issues reported) and were categorized as other.
Concussions were the second most (n = 135) prominent after musculoskeletal injuries (n = 818). Concussions accounted for 12.4% of total documented club and intramural sports injuries among the (n = 10) intramural and (n = 16) club sports. Individually, during the 4 years, concussions accounted for 16.2% (n = 56) of club sports injuries and 10.6% (n = 79) of intramural sports injuries. A larger percentage of female (females: 19.4% vs. males: 9.1%) participants reported concussions. However, the total number of concussions was similar (females: n = 66 vs. males: n = 68). Concussion numbers are outlined by the club (Figure 1) and intramural sport (Figure 2) and sex. The highest intramural concussion incidences were in flag football and outdoor soccer. The total number of intramural concussions and resultant AEs are reported across intramurals by year (Table 1) and within each sport (Table 2).
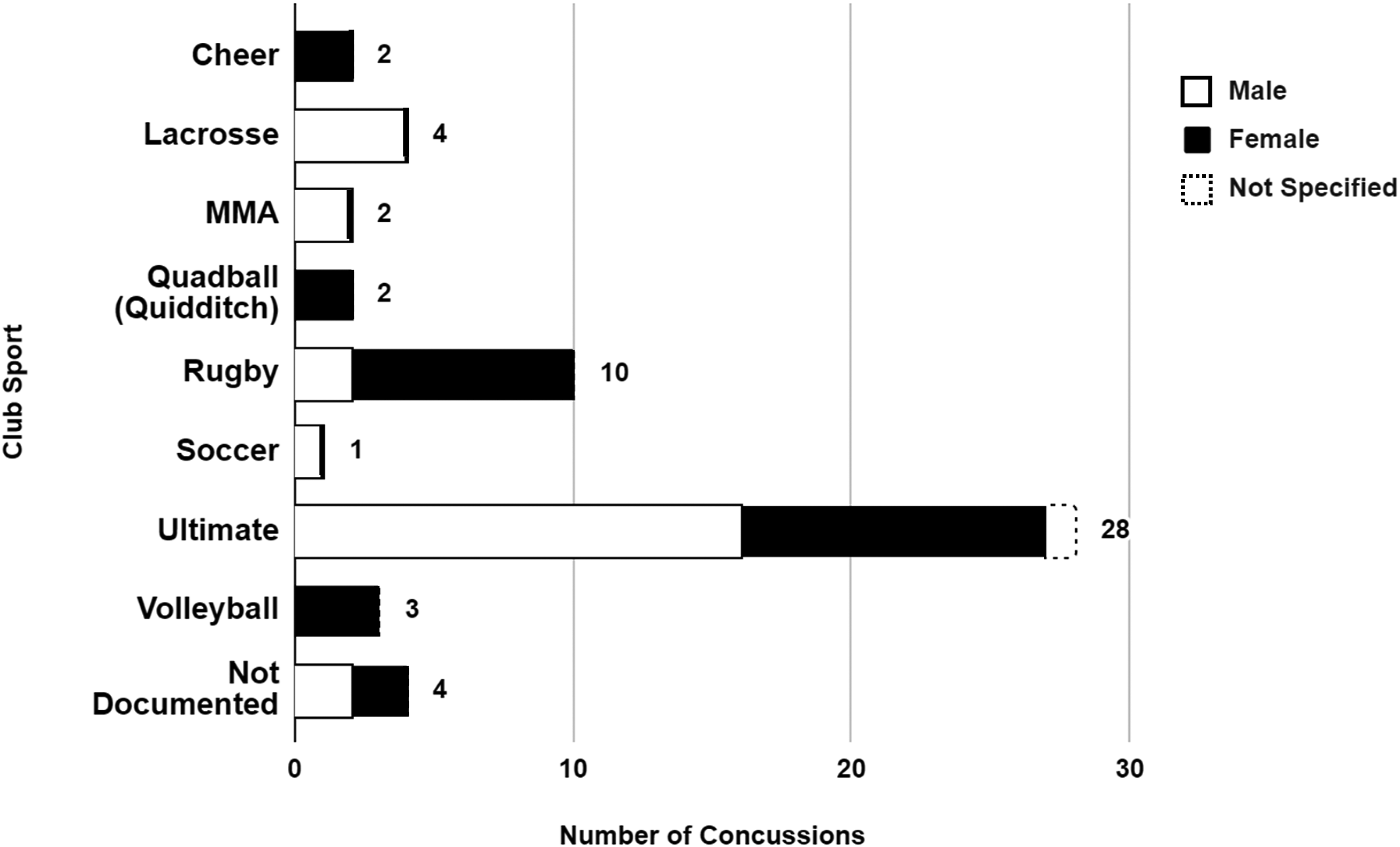
Concussions in Club Sports from 2016 to 2019.
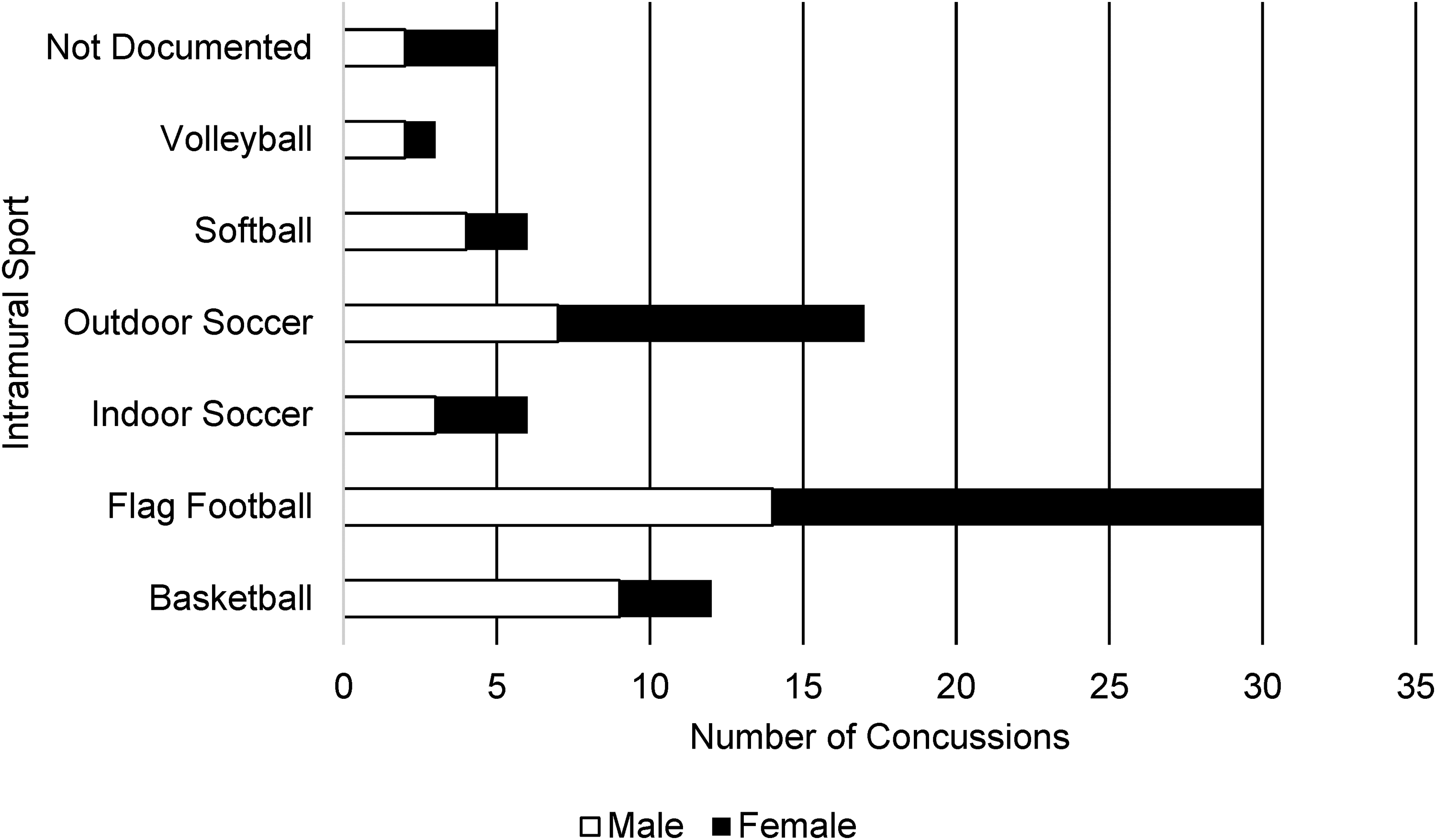
Concussions in Intramural Sports from 2016 to 2019.
Incidence Rate of Intramural Sports Concussions from 2016 to 2019.
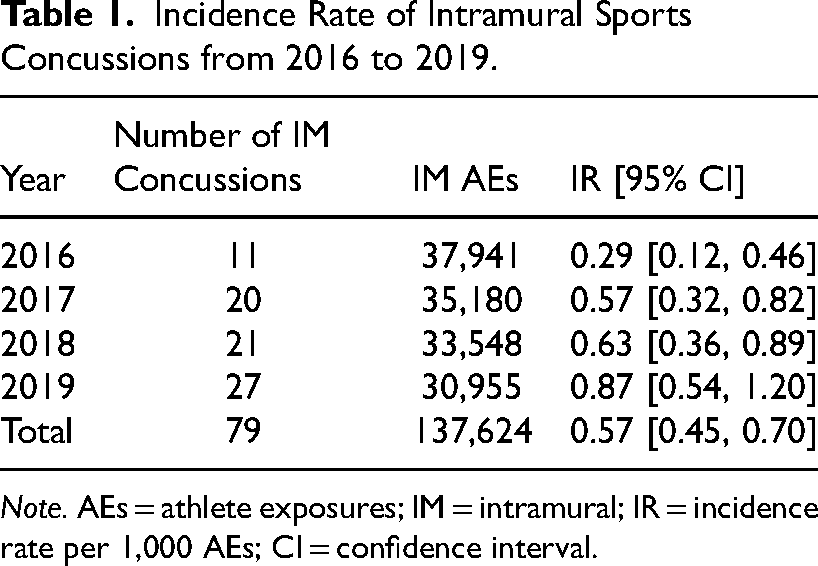
Note. AEs = athlete exposures; IM = intramural; IR = incidence rate per 1,000 AEs; CI = confidence interval.
Incidence Rate of Intramural Sports Concussions by Sport.
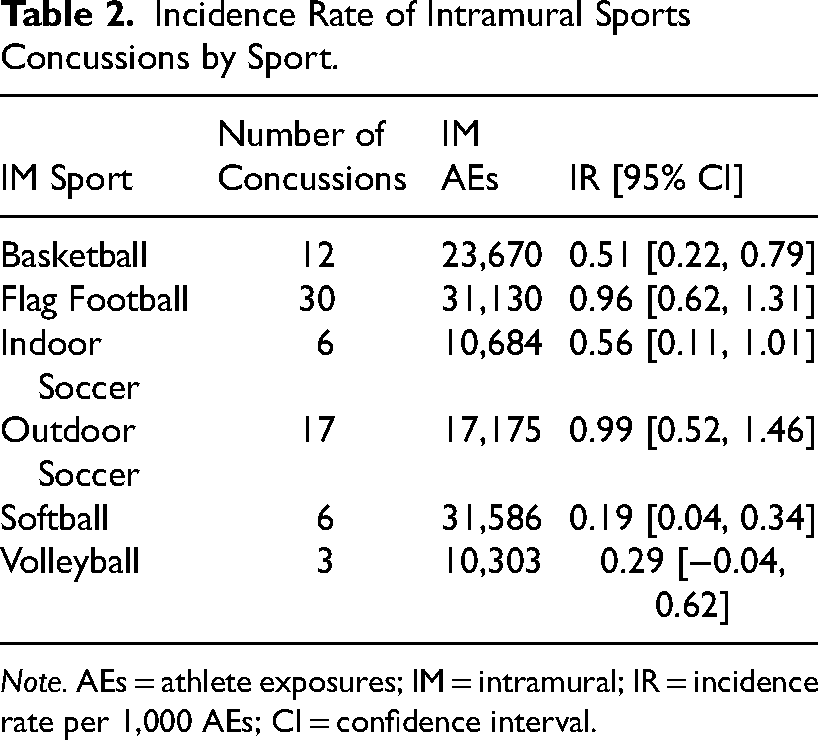
Note. AEs = athlete exposures; IM = intramural; IR = incidence rate per 1,000 AEs; CI = confidence interval.
The total number of AEs for onsite intramurals was 137,624 AEs. The intramural sports concussion IR per 1,000 AEs was 0.57 (95% CI [0.45, 0.70]). The total number of concussions increased annually over the course of the study. Further, AEs decreased annually over the course of the study and corresponded with relative increases in IR.
Discussion
This study provides initial insight into concussive injuries within intramural and club sports. Our primary finding was a greater percentage of concussions in intramurals (10.6%), club sports (16.2%), and across intramural and club sports (12.4%) than most previously published high school (reported data ranged from 5% to 18%) (Gonzalez et al., 2020; Kerr et al., 2018; Noble & Hesdorffer, 2013) and collegiate athletics averages (6%) (Hootman et al., 2007; Kerr et al., 2017; Noble & Hesdorffer, 2013). Secondarily, concussion four-year incidence rates of 5.7 per 10,000 AEs for intramural sports were greater than the high school and collegiate rates previously reported (O'Connor et al., 2017; Zuckerman et al., 2015). IR for NCAA athletes across 25 sports was reported at 4.5 per 10,000 AEs over 5 years (Zuckerman et al., 2015). Similarly, O’Connor et al. (2017) reported 3.9 per 10,000 AEs among 27 high schools over a three-year period.
While we were unable to separate IRs based on the participant's sex, outdoor soccer (9.9 per 10,000 AEs) and flag football (9.6 per 10,000 AEs) resulted in the highest concussion IR among the studied intramural sports. Our data is consistent with previous NCAA and high school reports that American football and soccer had increased IR. However, clear differences in the task (e.g., flag football vs. American football), rules, and league structure (i.e., same-sex and mixed-sex teams) limit our capacity to directly compare intramural sports to sanctioned, same-sex competition at the high school and NCAA levels. How task characteristics and environmental features interact and combine to increase concussion rates should be considered (Noble & Hesdorffer, 2013; O'Connor et al., 2017; Prien et al., 2018; Zuckerman et al., 2015). From this perspective, we acknowledge that American Football (9.2 per 10,000 AEs) and lacrosse (6.6 per 10,000 AEs) are the high school sports where male IRs are highest (O'Connor et al., 2017). In comparison, IR for women is greatest in soccer (6.1 per 10,000 AEs) (O'Connor et al., 2017). For NCAA, increased concussion rates are predominated by men's wrestling (10.9 per 10,000 AEs), men's (7.9 per 10,000 AEs), and women's (7.5 per 10,000 AEs) ice hockey, and men's American football (6.7 per 10,000 AEs) (Zuckerman et al., 2015).
Four intramural sports, including outdoor soccer, flag football, indoor soccer, and basketball, resulted in the greatest intramural concussion incidence rates. When observed rates are compared to those of the same sport in collegiate and high school athletics, we observed equal or higher concussion incidence rates (O'Connor et al., 2017; Zuckerman et al., 2015). The intensity of activity, level of competition, and participant skill have been cited to affect injury rates (Arthur-Banning et al., 2018; Hootman et al., 2007; Luiggi et al., 2018). Luiggi et al. (2018) found that increased levels of competition resulted in increases in sports injury percentages. While the physical stress and intensity of play may be greater in NCAA and high school sports, Hootman et al. (2007) noted that poorly conditioned athletes may react negatively to high-intensity and high-load activity, potentially increasing injury rates. It is important to note how the perceived reduction in preparation (coaching, practice, and off-field conditioning) for intramural participants might influence IR (Arthur-Banning et al., 2018; Hootman et al., 2007; Luiggi et al., 2018). While it is contrary to literature that intramurals would result in greater concussion rates compared to collegiate and high school athletics, future research is warranted to identify factors and whether these factors act in isolation or combination to predict IR in intramurals.
While this study could not calculate incidence rates for club sports, club sports resulted in a greater overall percentage of concussive injuries than intramural sports. This may reflect an increased intensity of play or higher competition level (e.g., absolute skill of players) than intramurals (Arthur-Banning et al., 2018; Hootman et al., 2007; Luiggi et al., 2018). The greater competitive context may positively influence the injury rate (Luiggi et al., 2018). Future research should investigate club sports concussion IR to compare club sports to intramurals and varsity collegiate sports adequately.
Sex has been previously documented to influence concussion incidence and reporting (Chandran et al., 2017; Cheng et al., 2019). Therefore, we provided an initial exploration of concussions across club sports and intramural regarding sex. Consistent with previous studies (Chandran et al., 2017; Cheng et al., 2019), females in this study sustained a higher percentage of concussions compared to their male counterparts. Although males and females had similar absolute number of concussions for intramural and club sports combined, females resulted in a greater percentage of concussive injuries due to fewer total females in the included injury reports. The intersection of social and cultural norms may explain our observations as females are more likely to report symptoms (Chandran et al., 2017; Gessel et al., 2007). Males may also be more reluctant to report symptoms for fear of being withdrawn from competition (Chandran et al., 2017; Gessel et al., 2007). Anthropometric sex differences are also cited to explain differences in IR (Chandran et al., 2017; Cheng et al., 2019; Gessel et al., 2007). One aspect that is unique to intramural sports and club sports is the integration of the sexes. How mixed-sex teams may influence reporting should be explored in future research.
The interpretation of our findings should consider our limitations. Due to the retrospective nature of this study, our conclusions are based upon the delimitations of data collection. We assumed participant details (e.g., participant's sex, injury, and sport) were accurately recorded in the injury reports. Additionally, the injury reports were, in part, reliant upon self-reporting as the AT on staff was often responsible for the oversight of multiple competitions that occurred at the same time.
Application to Practice
Among the approximately 8.1 million participants in collegiate recreation, only approximately 35% have access to an AT (Arthur-Banning et al., 2018; Lifschutz, 2012; Schneider et al., 2008). Unlike the institution studied, many colleges and universities rely upon a separate healthcare system (e.g., student health clinic) that is not directly associated with the collegiate recreation department. Therefore, the on-site AT is a clear advantage of this institution and supports our data capturing a greater percentage of actual concussive events sustained during intramural and club sports. The concussion incidence reported here is problematic when recreational participants do not have access to medical care, or knowledge that medical care is available. This absence of medical supervision may have cascading effects on postconcussion management and outcomes for the student whose limited access to healthcare often predates postconcussion management. Collegiate recreation departments should mitigate liability and improve outcomes for recreational athletes through, in part, the provision of on-site medical care (e.g., the Certified Athletic Trainer) at a minimum for sports at the highest risk. Further, institutions should capture all athletic exposures to adequately capture injury risk across all sports to help inform risk management practices. Specifically, to support injury management, the inclusion of a formalized concussion and injury education for club sport officers and their support staff (e.g., recreation department staff and club sport coaches) would enhance reporting if concussion symptoms or injuries arise, which would be expected.
Conclusion
Limited epidemiological data has historically encumbered collegiate recreational departments’ efforts to support medical supervision of clubs and intramural sports with concussion risk. The findings from this study provide initial estimates of concussive injuries for collegiate club and intramural sports, with flag football and soccer sustaining the highest incidence of concussion. This study may serve as a catalyst for other institutions to evaluate their own recreational department's concussion rates and incidence in club and intramural sports in order to make more informed decisions regarding sports risk. At a minimum, campus recreation departments should consider employing on-site certified athletic trainers and/or other medical professionals to ensure proper sport safety and limit institutional risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.