
Abstract
While many advances have been made mixing other methodologies with mixed methods research (MMR), there are few examples of narrative MMR or detailed procedures for integrating the narrative approach into mixed methods studies. This article contributes to the MMR field an example of integrating narratives in MMR by applying a methodological approach that is shaped by stories. The example integrated findings from cancer narratives with survey data to explore emotional support and quality of life of older people living with cancer. Integration was achieved by, firstly, following a thread through the research phases, and secondly, by using joint displays to align findings. The narrative MMR methodology presented is a tool for putting stories at the center of the research process.
Introduction
It has been noted that research following a mixed methods approach can provide comprehensive answers to complex problems, particularly common in the health services (O’Cathain et al., 2007; Vaughan Dickson et al., 2011). Cancer, for example, is a complex and multifaceted topic that attracts researchers from across a wide range of disciplines (Hiatt & Breen, 2008). Cancer researchers use a variety of both qualitative and quantitative methods. From a qualitative perspective, talking about cancer is emotive and telling real stories resonates with many people (for example, Evans et al., 2014; McQueen et al., 2011); however, equally powerful is quantitative research highlighting cancer statistics (Miller et al., 2019) and it is often quantitative data that provides the rationale to implement change (Pluye & Hong, 2014), such as the approval of different treatments. From a medical-sociological perspective, understanding the ramifications of a cancer diagnosis would be enhanced by situating the patient and their experiences at the center of research and service provision (Kerr et al., 2018), while still utilizing relevant statistical data to influence change. Therefore, the on-going methodological challenge is to integrate narratives into mixed methods studies in a way that uses the participant’s voice, their story, to truly guide the research.
To address this challenge, this article outlines an example of integrating narratives in mixed methods research (MMR) by applying a methodological approach that is shaped by stories. The example was a multiphase study that explored the value of social support to older people with cancer. Specifically, the study used narratives to develop the quantitative research approach in an exploratory sequential MMR design. In the qualitative phase of the research, narratives were gathered and analyzed from written case studies and semi-structured interviews. The findings from these narratives were then used to guide the quantitative phase of the research in which secondary data analysis of a large-scale social survey was carried out. In the final phase of the research, the qualitative and quantitative findings were integrated and inferences were drawn.
While other researchers have used exploratory sequential designs that gather and analyze narratives (for example, Munce et al., 2021), the explicit role of the narratives has not in the past been articulated. The exception is a recent study by Waller and colleagues (2021) who through an exploratory sequential design used qualitative narratives (gathered from semi-structured interviews) to construct narrative case histories from survey data (Waller et al., 2021). The study from Waller and colleagues highlighted the underuse of narratives in MMR and presented a novel narrative approach to data analysis in longitudinal MMR. Adding further to the literature, the methodology presented in this article advances our knowledge about the explicit use of narratives in MMR and the value this methodology can bring to addressing complex research problems.
The rest of this article is structured as follows. First, we provide further details of the use of narratives in MMR and a definition of narrative MMR as a methodology. Second, contextual background information is provided about older people, cancer, and social support. Third, the methods and results of the example study are presented. The article concludes with a discussion including limitations and the contribution of this article to MMR.
Narrative Use in Mixed Methods Research
In MMR, it is common for narrative sources to be used in the qualitative phase of the research. Sources of narratives vary and include both written documents (such as diaries, autobiographies, and biographies) and oral statements (such as oral histories and interviews). For some time, interviews have been popular and the most common source of narratives (Polkinghorne, 1995). It has been observed that using narratives enhances the “potential of combining qualitative and quantitative techniques for reaching a better understanding of causal processes and for allowing a prominent place for the role of human agency in sociological explanations” (Elliott, 2005, p. 171). In this context, narratives are generally understood as stories that include both a temporal ordering of events and a purpose, such as sharing of experiences (Labov & Waletzky, 1997; McAlpine, 2016; Sandelowski, 1991). Put another way, narratives convey meaning to events (Elliott, 2005).
How narratives are integrated in MMR varies according to the MMR design, for example, whether convergent, explanatory sequential, or exploratory sequential (Creswell & Plano Clark, 2018). Narratives in convergent designs, have been used to complement, provide context to and enrich the quantitative findings (for example, Beletsky et al., 2016; Vaughan Dickson et al., 2011; Wagner et al., 2017). In explanatory sequential designs, inferences drawn from narratives have been used to support survey findings (for example, Carpentieri et al., 2016; Shammas, 2017) and answer questions raised by the quantitative phase (for example, McCrudden & McTigue, 2019; Zeng et al., 2012). In exploratory sequential designs, the qualitative phase of the research is used to develop the quantitative phase (Creswell & Plano Clark, 2018). Therefore, when using narratives in an exploratory sequential MMR design, the important constructs and variables to be explored in the quantitative phase of the research are defined by the findings from the qualitative narratives.
We define narrative mixed methods research as a MMR approach that is shaped by stories about the phenomenon under investigation. This definition, and the following example, represents a valuable contribution to the field of MMR.
Our Study: Older People, Cancer, and Social Support
In our study, our purpose was to explore the impact of social support on the treatment and quality of life of older people living with cancer. Although advances have been made in the treatment of most health conditions, older people are still more likely to be affected by an array of health conditions than younger people, and this includes cancer (Lavelle et al., 2014; Lawler et al., 2014). In our study, we adopted a life-course perspective to aging, which promotes human development as influenced by the context surrounding the individual (Elder, 1998). The research was conducted in the context of the aging population (Phillipson, 2013), which has resulted in increasing numbers of older people being diagnosed with cancer (Maddams et al., 2012; Smittenaar et al., 2016), and also increasing numbers of older people surviving beyond cancer (De Angelis et al., 2014).
Social support has been recognized as having an important role to play in the experiences of older people with cancer. For some time, better assessment throughout the cancer experience has been advocated as a means of improving understanding of the factors affecting older people with cancer (Extermann et al., 2005; Shariat et al., 2009). It has been recommended that the social support available to older people with cancer is assessed to ensure the necessary emotional and practical support is able to be provided (Shariat et al., 2009) and ensure improved quality of life post-treatment (Ashley et al., 2017). However, to assess access to social support, clinicians and health professionals need to know, firstly, what the social support needs of older people with cancer are, and secondly, how they can best be met.
Throughout our study, social support was conceptualized using four commonly used subtypes of social support (Berkman et al., 2000; Weiss, 1974): 1. emotional (often provided by a partner or other close family member, and translates to the provision of love, caring and understanding), 2. practical (provision of instrumental support, such as transport or cooking, or providing financial aid), 3. informational (provision of information and advice, based on knowledge and services), and 4. appraisal (help with appraising a situation and making decisions). Using the social support subtypes has the potential to increase understanding of what aspects of social support have the greatest impact, if any, on the lives of older people living with cancer.
Using a narrative MMR methodology to bring together the concepts of older people, cancer, and social support, our study asked the following research questions:
Phase 1: How does social support impact on the treatment offered to and received by older people with cancer?
Phase 2: Is social support associated with the quality of life of older people who are cancer survivors? Is any association between social support and quality of life altered by the source of social support?
Phase 3: What is the impact of social support on the experiences of older people with cancer?
Methods
The research reported in this article was a multiphase study that was integrated through an exploratory sequential MMR design; the individual studies did not share the same source of data.
Using an Exploratory Sequential Design
The research followed an exploratory sequential design, as defined by the timing of the studies and the integration procedure (Creswell & Plano Clark, 2018). First, the problem was explored through qualitative data collection and analysis, secondly, the quantitative study was designed, and then the quantitative analysis was carried out. Therefore, the exploratory sequential design followed a building process (Figure 1). The exploratory sequential design was deliberately chosen following a narrative MMR methodology; the research started by listening to the stories and experiences of older people with cancer. However, within the research program, both the qualitative and quantitative studies had equal status (Moran-Ellis et al., 2006). No study was seen as worthier, and all brought valuable findings to the research. Phases of the mixed methods research program with an exploratory sequential design.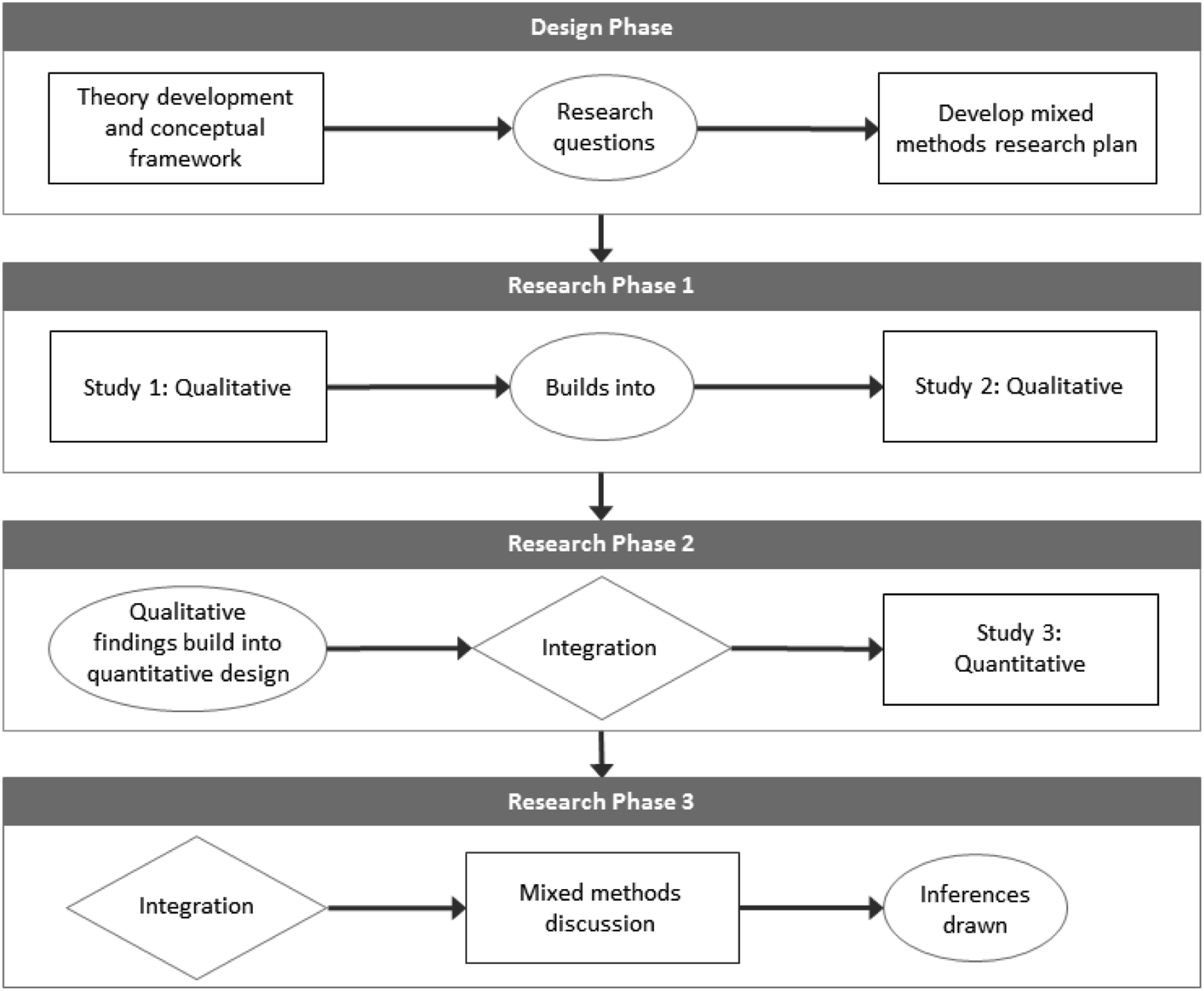
Project Data and Methods
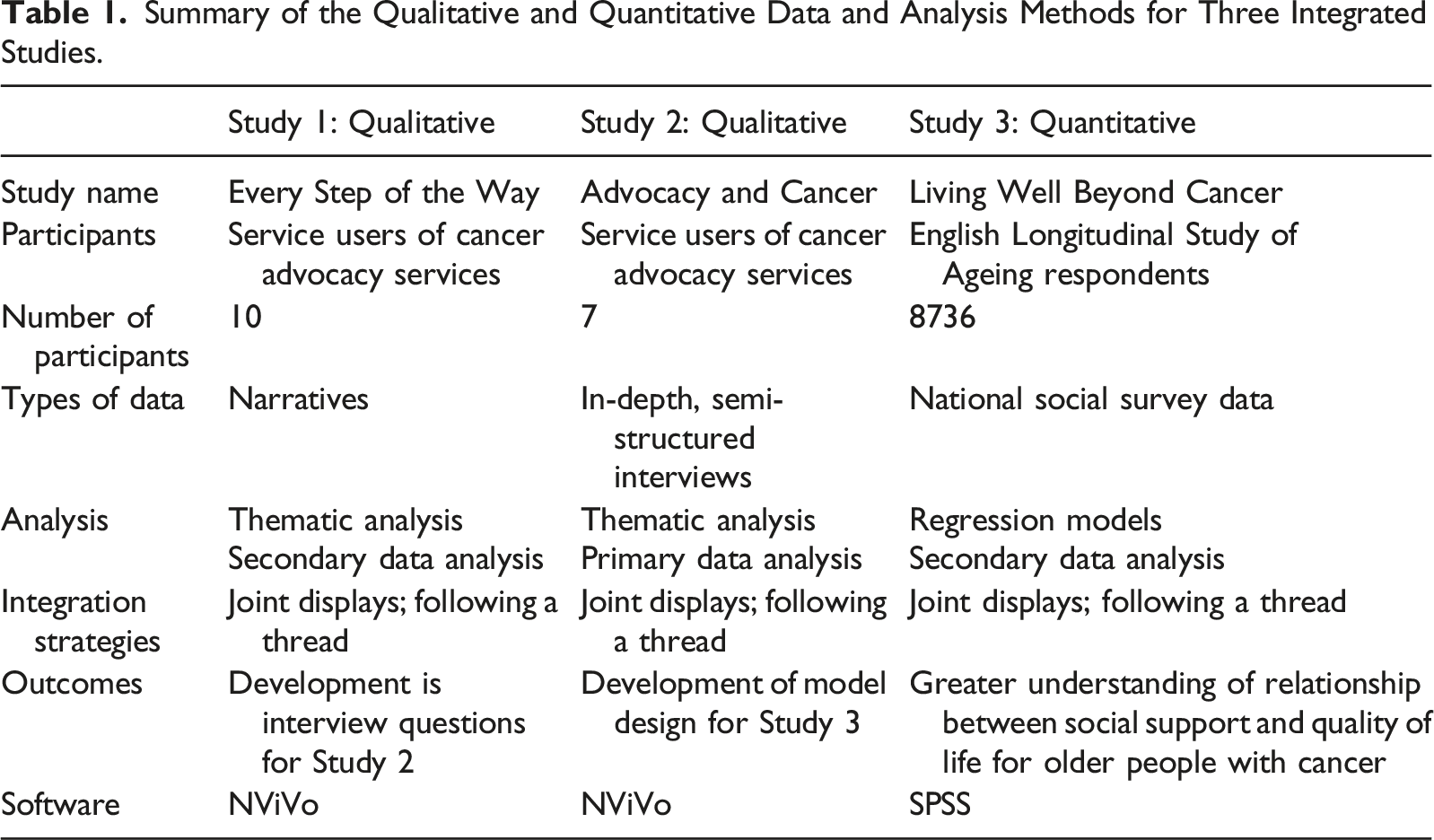
Summary of the Qualitative and Quantitative Data and Analysis Methods for Three Integrated Studies.
Phase 1: Qualitative Narratives
The first qualitative study conducted (Every Step of the Way ‐ Study 1) was a thematic analysis of the stories from Every Step of the Way (OPAAL, 2014), a book containing 13 stories about people who had used advocacy services after receiving a cancer diagnosis. The book was published by the Older People’s Advocacy Alliance (OPAAL), a national membership-based organization for UK advocacy services for older people. The people whose stories were used were purposely selected based on the richness of the story and the willingness of the older person affected by cancer, and their advocate, to participate. The data, that is the content of the stories, was not originally collected for the purposes of systematic analysis. Rather, the stories were published as a report to “illustrate the wide-ranging issues that affect older people affected by cancer and the nature and types of support offered by advocates to address these [issues]” (OPAAL, 2014, p. 1). Through this illustration, the authors hoped to encourage both new and existing advocates, raise awareness with health professional colleagues, and influence commissioners to recognize the value of advocacy (OPAAL, 2014). By carrying out secondary data analysis of the Every Step of the Way narratives, the aim was to gain new knowledge about the experiences of social support during cancer treatment.
The second qualitative study (Advocacy and Cancer ‐ Study 2) involved primary interviews with people who had used cancer advocacy services, and the interviews were carried out between June and September 2015. The interviews were planned in partnership with OPAAL; participants were referred to the study by advocacy support services and were purposely selected. All participants had low social support resources, as evidenced by their use of the advocacy services. Participant recruitment was actively pursued over a period of 6 months and was on-going while the initial interviews were being conducted and initial analysis carried out. Due to the vulnerability of the participants, recruitment was difficult. No further referrals were pursued from the advocacy services as soon as data saturation was achieved (that is, no new themes were emerging). In-depth semi-structured interviews were carried out with seven participants from four different advocacy services.
The Advocacy and Cancer Study was built on previous research that highlighted a divergence between patient and consultant perceptions of the shared decision-making process (Lavelle et al., 2014; Sowerbutts et al., 2015). It asked what it meant for the older person to be involved in their cancer treatment decisions, or whether they felt they were involved at all. The method of in-depth semi-structured interviews was chosen as it is a versatile method that allows for fully exploring the experiences of the participants as they relate to the research questions (Galletta, 2013). The interviews were designed to take an inductive, non-directive approach.
The qualitative studies were carried out sequentially. The themes that emerged as final results from the Every Step of the Way Study were built in to the interview questions used in the discussion guide for the Advocacy and Cancer Study. The data from both the stories and interviews was managed using NVivo (NVivo for Mac Version 10.2.2 © QSR International). Principles of thematic analysis (Braun & Clarke, 2006; Thomas, 2008) were applied to identify common themes from the data. A framework was developed to allow comparison of themes and participant attributes where available (including age, cancer type, cancer stage, access to social support, and living arrangements). Principles of reflexivity were applied (Swift & Tischler, 2010) to ensure that an awareness of the co-construction of the knowledge produced through the narratives and interviews was acknowledged. Additionally, as the studies were designed in partnership with other organizations (OPAAL and the advocacy services), the influence of their involvement was also considered. After analysis of all data from the Every Step of the Way Study and the Advocacy and Cancer Study, no further sources of qualitative data were gathered as data saturation was reached. Full inclusion criteria, discussion guide and full detail of both the Every Step of the Way Study and the Advocacy and Cancer Study is available elsewhere (Doran, 2018).
Phase 2: Quantitative Analysis of Survey Data
Data from Wave 1 of the English Longitudinal Study of Ageing (ELSA) was used in the Living Well Beyond Cancer Study (Study). ELSA is a long-running, social survey that aims to explore the dynamics of aging in England (Marmot et al., 2017). The survey is conducted face-to-face in people’s homes and is followed up with a self-complete questionnaire (SCQ). Detail is collected from people aged 50 and over on health, well-being, economic position, and social factors. Wave 1 of ELSA was conducted in 2002 and there have been consecutive waves every 2 years. As with most longitudinal studies, there is loss in retention of respondents. Data from Wave 1 was used in the Living Well Beyond Cancer Study as it provided the highest numbers of respondents, an important consideration as only a small proportion of respondents were cancer survivors (approximately 6%). Using Wave 1 data meant that the experiences reported in the quantitative data were from many years apart from the qualitative data. This has been considered when interpreting the results.
Cross-sectional analysis was carried out on the Wave 1 ELSA data. The outcome variable was Quality of Life (QoL), measured using the CASP-19 tool. The CASP-19 measure of QoL was created in response to the growing population of healthy older people and the need to have a QoL measure that was not solely (ill) health related (Hyde et al., 2003). The CASP-19 QoL measure is needs based and covers four domains: Control, Autonomy, Self-realization, and Pleasure. Questions do not focus on health or physical ability; rather, questions are asked about well-being, aspirations, and the ability to achieve personal purpose. For example, I can do the things that I want to do (Control); I feel that my life has meaning (Autonomy); I feel that the future looks good for me (Self-realization); and I enjoy the things that I do (Pleasure). The related CASP-19 questions have been included in all waves of ELSA. Bivariate analysis was carried out to test if any domain of QoL was particularly related to social support.
The key predictor variable was emotional support, derived from a combination of three questions within ELSA. Respondents were first asked if they had a partner/children/other family/friends, if “yes” they were then asked for each source of support: 1. How much do they really understand the way you feel about things? 2. How much can you rely on them if you have a serious problem? 3. How much can you open up to them if you need to talk about your worries? Each of the questions could be attributed to a different aspect of emotional support: empathy, dependability and confiding (Rouxel et al., 2015), and therefore, the derived measure is referred to as emotional support. Variances between the source of support and QoL were also explored.
Relationships between social support and QoL for both cancer survivors and those without cancer were tested using linear regression models. Both a comparative model and an imbedded model were used to explore the differences in outcomes of cancer survivors compared to people without cancer. Controls included age, gender, wealth, education, having a long-standing illness, and various attributes relating to the cancer diagnosis (for the cancer survivors sub sample). Age was measured on a continuous scale; being a cancer survivor, gender and illness were dichotomous variables; and wealth and education were measured in quintiles. Tests for multicollinearity were carried out and the change in R2 values was reported. Interaction variables testing for a significant interaction between social support and living with cancer were also used. Full details of the analysis techniques and findings are reported elsewhere (Doran et al., 2019).
Phase 3: Mixed Methods Integration
Integration was carried out using two analysis techniques. Firstly, integration took place when each study built on to the next through the research process, a “thread was followed” (Moran-Ellis et al., 2006) through the research phases. Joint display tables were used to ensure validity in the design process (Creswell & Plano Clark, 2018) by aligning findings from each study with the design of the next study. The final research phase involved the “third effort” (O’Cathain et al., 2010); using a final joint display, integration of the findings from the qualitative and quantitative studies was carried out to produce further understanding of the experiences of older people living with and beyond cancer. The final joint display table was produced by focusing on the findings as they related to the overall research themes (Bazeley, 2016). Qualitative quotes and themes were placed alongside quantitative variables and scales, followed by a summary of how the qualitative and quantitative elements compared. The findings were discussed in respect to where they converged, diverged, complemented, or produced silence (Fetters et al., 2013; O’Cathain et al., 2010). Convergent findings suggested partial agreement, divergent findings addressed different aspects of a single phenomenon, complementary findings suggested a strong alignment of findings, and silence referred to an absence of common finding across studies. Silence in one study does not mean that there is dissonance in the findings; rather, it is an example of how different approaches can reflect different aspects of a phenomenon (Moran-Ellis et al., 2006).
Results
Phase 1: Qualitative Results
From the thematic analysis of the cancer stories in the Every Step of the Way Study, there were five final themes: (1) Loneliness - Isolation, not having someone to help you cope; (2) Shock - Sudden change, inability to think straight, numbness, disbelief, and confusion; (3) Empowerment - By knowledge, plans, direction; to continue, move on, have hope, and survivorship; (4) Gratefulness - For the medical system, to the advocates, for the (small) positives; and (5) Going through the system - Not in control, following the motions, not being treated as a person, constant change, or no change, unknown, and many people involved in care. Using a joint display table, themes from the Every Step of the Way Study were built into the design of the interview guide used in the Advocacy and Cancer Study (Figure 2). Joint display of strategy for integration of narrative themes from Study 1 into qualitative interviews of Study 2.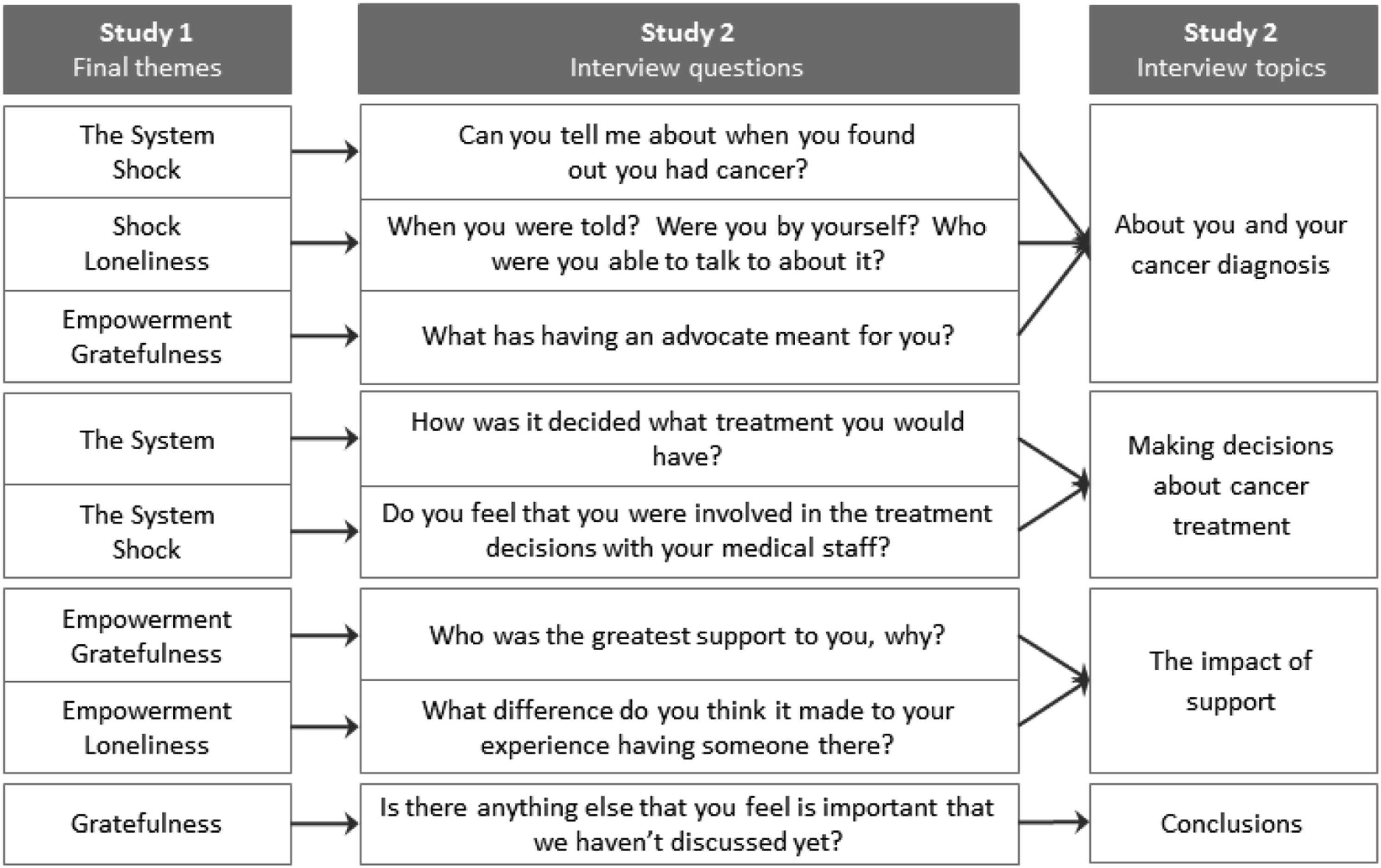
Following the same thematic analysis process used in the Every Step of the Way Study, at the conclusion of the Advocacy and Cancer Study, six themes were identified: lack of control; cancer knowledge; someone to talk to; blurring of practical and emotional support; complexity; and living with cancer. The theme of lack of control highlighted the perceived lack of choice around treatment options. The theme also resonates with the findings from the Every Step of the Way Study relating to going through the system and shock. Lack of control fed into the theme of cancer knowledge. The older people interviewed expressed the tendency to defer to opinions of clinicians, as they were the perceived experts. The lack of cancer knowledge led to the need to pass control to other people who were working in the cancer system. However, lack of knowledge was also evident in relation to seeking support, or knowing where to look for help with practical issues when affected by cancer.
The issue of social isolation was discussed frequently in the interviews. Even if partners or family members were able to provide support, there was a sense that what was needed was someone to talk to who would empathize and show understanding. The theme of blurring of practical and emotional support highlights that emotional support was often received, for example, through company and talking, while practical support was being provided, for example, when providing transport or helping with paperwork. This is illustrated by a quote from Tina: “She came with me regularly to chemo and it was brilliant … she was so much company, you know, and she put me on the taxi then to bring me home and she’s brilliant, helped an awful lot.” (Tina)
Complexity emerged as a strong theme throughout the interviews. Living with cancer in and of itself is multifaceted, and the complexity of the situation is often overwhelming. People living with cancer have to adjust to being told they have a very serious illness and then cope with the various specialists and appointments needed to treat their condition – as well as manage their day-to-day life and relationships. If life before cancer was already complex (perhaps as a result of other health problems, caring responsibilities, or financial strains), a cancer diagnosis can compound the situation and create added complexity. Many of the older people living with cancer involved in the Advocacy and Cancer Study were dealing with very complex situations, as illustrated by Dan: “At the same exact time as I was first diagnosed with my prostate cancer, my partner started getting depression and anxiety and was in and out of care.” (Dan)
Despite their complexities, it was clear from the interviews that people were living with cancer. Once diagnosed with cancer it is understood that you will be living with (and beyond) cancer for the rest of your life. In many cases, living with cancer for the older people in interviewed meant that the support needs associated with cancer did not end with treatment at the hospital. Relating back to cancer knowledge, the older people still had unanswered questions and still needed someone to talk to.
Phase 2: Quantitative Results
Figure 3 shows the final themes from the Advocacy and Cancer Study and illustrates how the themes were integrated into the design and final linear regression model from the Living Well Beyond Cancer Study (Study). The ELSA dataset contains a wealth of information about all aspects of living as older people in England (such as health, wealth, well-being, retirement, and social participation), aspects that could also be affected by living with cancer. The specific focus and design of the Living Well Beyond Cancer Study was determined by the findings from the Advocacy and Cancer Study. Therefore, the qualitative themes from Phase 1 of the research influenced the quantitative research questions in Phase 2, which in turn directed the approach to the secondary data analysis. For example, in response to the theme of blurring of practical and emotional support (Advocacy and Cancer Study), a single indicator of emotional support (derived from three questions on different aspects of support) was used in the Living Well Beyond Cancer Study. Joint display of strategy for integration of qualitative themes of Study 2 into the quantitative Study 3. Note. Key findings from Study 3 are presented. These are the results from a linear regression model of relationship between emotional support and quality of life (CASP-19 was the dependent variable). For full quantitative results see Doran et al. (2019).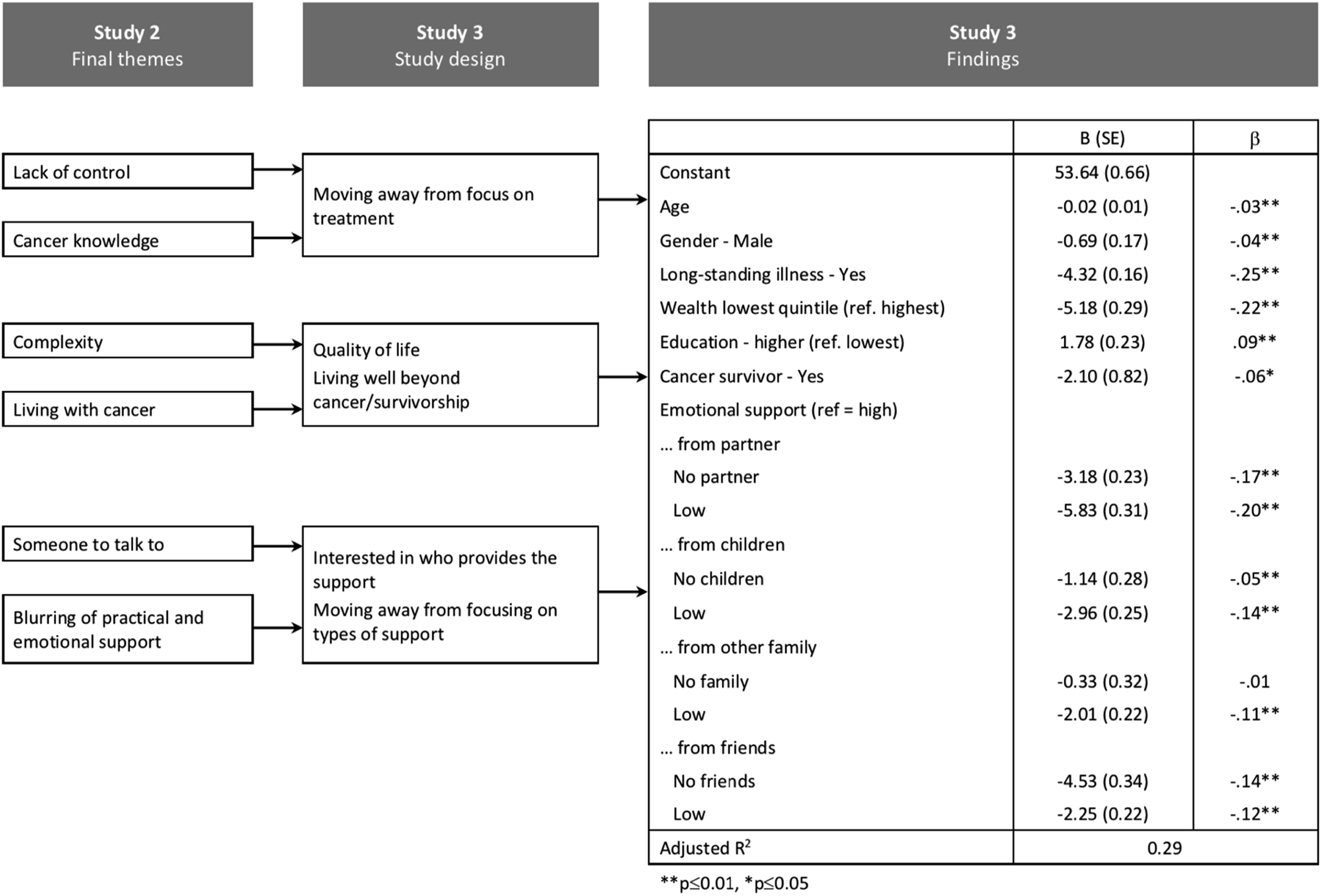
In the Living Well Beyond Cancer Study, the impact of emotional support on the QoL of older people with cancer was explored and a strong relationship between emotional support and QoL was found. Figure 3 shows the results from the final linear regression model produced in. An interesting result emerged; low level of emotional support from partners, children, and family resulted in poorer QoL compared to not having any support from that source. For example, while not having a partner had a negative effect on QoL (−3.18 SE = 0.31), there was a greater negative effect seen for older people who had a partner but received little support from them (−5.83 SE = 0.23). When looking specifically at cancer survivors, the final regression analysis indicated that after considering emotional support, and any interactions between emotional support and cancer, the negative impact of having a cancer diagnosis still added significantly to lower QoL (−2.10 SE = 0.82).
When comparing the different sources of support and QoL across the full sample, having a high level of support from any of the sources produced a very similar mean CASP-19 score (around 44), there was greater variance encountered when low levels of support were reported. The biggest impact on QoL came from having a low level of support from a partner (−5.83 SE = 0.23) or having no friends (−4.53 SE = 0.34). Having no friends may suggest a small social network and perhaps social isolation, and having a low level of support from a partner may suggest a caring role, further analysis would need to be carried out to test these theories. However, it was concluded that the source of support influences the emotional support being received (Doran et al., 2019).
Phase 3: Integration
Joint Display Table of Findings: Integrating the Qualitative and Quantitative Phases of the Research Program.
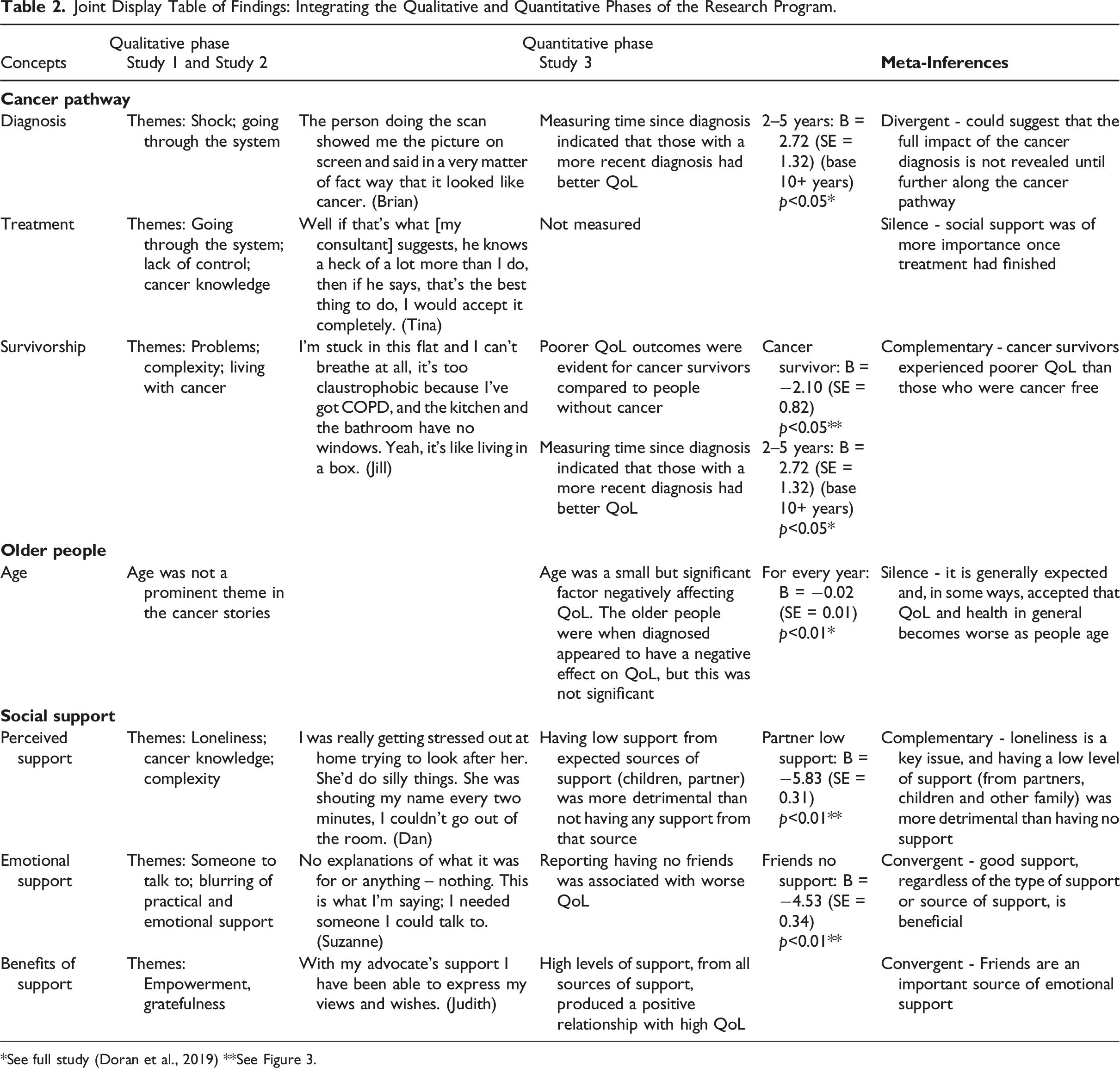
*See full study (Doran et al., 2019) **See Figure 3.
The diagnosis stage, although not specifically explored in the studies, was included in the Joint Display Table as it represented the beginning of the cancer pathway. Interestingly, divergent findings emerge when exploring the concept of diagnosis. The qualitative phase of the research highlighted the negative themes of shock and going through the system, both of which relate to initial cancer diagnosis (as well as further along on the cancer pathway). It is suggested that the themes from the qualitative studies are divergent with the quantitative finding that QoL was higher on average for people with a more recent cancer diagnosis. One possible explanation for higher QoL could be the potential increase of social support offered at the time of cancer diagnosis. Therefore, while there may be negative themes of shock and being a cog in the system, one potentially positive outcome for many people was an increase in support. Perhaps initially after a cancer diagnosis, the shock effect inhibits reflections on and assessment of other factors, such as QoL. Both findings could suggest that the full impact of the cancer diagnosis is not revealed until further along the cancer pathway.
Silence was evident when comparing findings in relation to the treatment stage of the cancer pathway. While treatment and treatment decisions were central areas of interest in Phase 1 of the research, the findings from these studies that suggested social support was of more importance once treatment had finished led to a focus on QoL and survivorship in Phase 2. Therefore, no measure of treatment or treatment decisions was used in the Living Well Beyond Cancer Study (and currently there is no appropriate measure in the ELSA dataset), and study was silent on the theme of treatment.
The concept of survivorship was met with complementary findings. Survivorship and QoL were investigated in the Living Well Beyond Cancer Study because of the prominent themes of support needs post-cancer from the qualitative phase of the research; therefore, it is not unexpected that the findings complemented each other. The qualitative findings were reinforced by the quantitative findings that suggested cancer survivors experienced poorer QoL than those who were cancer free. The findings highlight the complexity of being a cancer survivor, on-going support needs, and the potential impact on QoL when those support needs are not adequately met. In particular, it was interesting that QoL deteriorated as the number of years post-diagnosis increased, perhaps a sign of the impact of late effects of cancer treatments.
The silence in relation to the concept of older people and age is interesting. Questions around age were not included in the story template used for collecting the narratives analyzed in the Every Step of the Way study or the interview discussion guide in the Advocacy and Cancer Study. However, age was considered in these studies by sampling older people. Yet when telling their stories, old age (or even age in general) was not an issue that was explicitly highlighted by the older people with cancer. In contrast, age was included in the models used in the analysis for the Living Well Beyond Cancer Study, and as would be expected, increasing age had a negative effect on QoL. Perhaps, it is generally expected and, in some ways, accepted that QoL and health in general becomes worse as people age. Therefore, it was potentially an unspoken assumption in the qualitative studies that age impacted on their lives.
Social support was explored by focusing on perceived support, emotional support, and the benefits of support. Perceived support relates to an individual’s perceptions and feelings about of their general level of support (Cattan et al., 2003). Emotional support reflects having access to functional support, for example, someone to talk to; therefore, the availability, as well as the receiving, of support was examined (Tardy, 1985). The measure of benefits of support reflects reported positive outcomes.
The social support findings were not linked to the study design in the same way as survivorship. In relation to perceived support, themes around loneliness and complexity (often expressed during discussions of caring responsibilities) that arose in the qualitative studies were independent to the quantitative findings that suggested that having a low level of support (from partners, children, and other family) was more detrimental than having no support. However, although the findings are independent, they are clearly complementary; therefore, the findings from the Living Well Beyond Cancer Study are reinforced by the stories from the Every Step of the Way Study and interviews from the Advocacy and Cancer Study.
Findings converged around the concept of emotional support. The theme of someone to talk to from the Advocacy and Cancer Study converges with the Living Well Beyond Cancer Study finding in relation to the impact of friendship. Older people who were cancer survivors were more likely than older people who were cancer free to report having a lot of support from friends (in bivariate analysis); however, reporting no friends had a strong relationship with poor QoL (in the regression models). The findings perhaps suggest that the need to talk after a cancer diagnosis makes friendships stronger. However, if you have no emotional support from friends, this was shown to be detrimental to QoL.
In relation to the concept of benefits of support, the prominent themes from the Every Step of the Way Study of empowerment and gratefulness reflect that many of the stories involved the older person moving from a position of no support and no friends to a position where advocates filled the role of a supportive friend. It was at this point that the outlook improved: “With my advocate’s support I have been able to express my views and wishes.” (Judith)
Therefore, convergence is reported with the finding from the Living Well Beyond Cancer Study that showed a general positive relationship between emotional support and QoL. High support regardless of the type of support, or source of support, produced equally high QoL.
Discussion
The methodological problem posed at the start of this article was how to integrate narratives into mixed methods studies in a way that uses the participant’s voice, their story, to truly guide the research. The example study described in this article demonstrated how a narrative MMR methodology can be applied to fully integrate narratives into a multiphase MMR study. Cancer as a topic is well suited to a mixed methods approach. Research into cancer is dominated by the medical and biological sciences; however, by approaching the topic from an applied social research perspective, the stories and experiences of older people living with cancer are given more prevalence. The multiphase study followed an exploratory sequential MMR design (Creswell & Plano Clark, 2018). Through a narrative mixed methods methodology, the stories and shared experiences of older people living with cancer influenced the design of the quantitative phase of the research.
Secondary data analysis was carried out using ELSA data, a survey that to date has had little interrogation in relation to investigating outcomes for cancer survivors. While ELSA data has been used to measure cancer screening update (Beeken et al., 2014), and investigate health behaviors and cancer (Grimmett et al., 2009; Jackson et al., 2014; Rouxel et al., 2015), ELSA has not previously been used to measure the impact of social support along the cancer pathway.
Key to the methodological approach was the final integration of outcomes from all three studies. Rigor and full integration of methods was achieved by using integration strategies established in the mixed methods field (Creswell & Plano Clark, 2018; Moran-Ellis et al., 2006; O’Cathain et al., 2008, 2010). The application of a mixed methods approach helped overcome some of the limitations of separate qualitative or quantitative methods and the integrated results produced an outcome greater than the sum of the parts. Using mixed methods enabled the blending of narratives with the wider social context and the richness of the results add to the impact potential of the research.
The exploration of the integrated mixed methods process (following the thread) and the integration of outcomes from the three studies (final joint display table) demonstrated that social support does have an impact on older people along the cancer pathway. The cancer stories in particular reveal that older people with cancer positively receive social support. However, older people with cancer who have low levels of social support are likely to report isolation and experience poor QoL, and there is a reported need for social support beyond the active cancer treatment stage (Kroenke et al., 2013). To be considered is that the sampling design of quantitative studies (that is, asking for volunteers to be interviewed) is likely to overrepresent people with better support networks, as they are the respondents more likely to participate in research studies (Marmot et al., 2003); therefore, findings may be underestimated. In our research, survivorship and emotional support were the key topics of interest highlighted by the integration of findings. More needs to be done to ensure the provision of social support to cancer survivors.
Limitations
The narrative mixed methods process dictated the focus of the quantitative study in the second phase of the research. Therefore, if the stories had been different, the focus of the quantitative study could have changed. As it was, the stories in the qualitative phase of the research all came from a very specific sample, users of advocacy services. The sample of advocacy users limited the scope of the findings. However, as the stories were generally complex they provided richer data compared to that which is often gained from homogeneous groups of participants in qualitative research (Bamidele et al., 2019).
The quantitative phase of the research was limited by the data available in ELSA. As mentioned, if the stories had been different, then the focus on the ELSA data would have been different, but alternative analysis would have only been possible if the ELSA data contained relevant variables. Although large social surveys offer a wealth of detail, there is little scope to change the data that is collected to suit changing research needs. The variables used in the current research enabled the creation of a good indicator of emotional support, and the indicator was able to be modeled with different sources of support (partner, children, other family, and friends). However, support from perhaps more professional sources, such as advocates and clinical staff, was not captured in the modeling as the data is not available through ELSA. Therefore, the research was limited by the individual methods and data used across the different research phases.
Qualitative studies tend to have small samples. A total of 17 stories were analyzed across Phase 1, the sampling was not random, and the findings are not easily generalizable. In contrast, the data used in Phase 2 (ELSA) was a very large sample that reflects the general population. The differences in samples almost certainly explain to some degree the divergent findings highlighted in the final Joint Display Table (Table 2) in relation to the diagnosis stage of the cancer pathway. The results from the Advocacy and Cancer Study confirmed that most of the older population, including those diagnosed with cancer, felt well supported. The participants in Phase 1 were purposively recruited; they had low levels of support and had found it necessary to access support through the advocacy services. Additionally, the ELSA data was collected some years apart from the narratives, it follows that the data does not reflect the exact same social contexts. Therefore, the qualitative and quantitative studies had very different samples.
Contribution to the Mixed Methods Literature
There is a growing interest in the explicit combining of established research methodologies with MMR, and each approach offers different contributions to the MMR literature. For example, mixed methods–grounded theory is a popular approach for both generating and testing theory (Guetterman et al., 2019), mixed methods phenomenological research has been defined as “research that combines phenomenological methods with methods grounded in an alternative paradigm within a single study” (Mayoh and Onwuegbuzie, 2015, p. 98), and mixed methods case studies has been developed as a useful framework for understanding complex social problems (Mason et al., 2020). However, there is limited literature on the combination of narrative methodology and MMR methodology. This article contributes to the MMR literature by addressing this gap.
The research example in this paper followed a narrative MMR methodology and has proposed to our knowledge the first definition of this approach, that is, a MMR approach that is shaped by stories about the phenomenon under investigation. In this example, the stories of older people living with cancer marked the starting point for the research. Through this approach, narrative MMR aids understanding of complex research problems by integrating narratives into mixed methods studies in a way that situates the participant at the center of the research, and using their story to truly guide the research.
Applying a narrative mixed methods methodology is beneficial when the quantitative phase of the research is able to be adapted. The ELSA study, from which our quantitative data was drawn, contains many hundreds of variables offering the opportunity to explore a wide range of research questions. In our research, we set out to explore cancer treatment experiences; however, after first listening to the stories, we instead explored the long-term well-being and QoL of older people living with cancer. The narrative mixed methods methodology helped focus the quantitative research design.
Through the use of joint display tables, we aligned narrative data with regression models and demonstrated an innovative method of integration. It is not common to find mixed methods studies that have used independent qualitative study alongside secondary analysis of a large-scale social survey. The use of a narrative MMR methodology to integrate narratives into quantitative research offers a new area of potential development, particularly in relation to secondary analysis of survey data. The methodology will be of interest to social statisticians who are seeking to explore large datasets, but who want to integrate the stories behind the numbers in their research design (Pluye & Hong, 2014).
Conclusion
Narrative MMR can be used to provide insight into complex social questions by using stories to guide the research. The study reported in this article demonstrated how a narrative MMR methodology could be used to produce new knowledge about the interplay between cancer, emotional support, and older people. It was found that older people with complex needs and low levels of social support can have their situations compounded by a cancer diagnosis. As the population ages, we are going to witness a rapid increase in the number of older cancer survivors. Many of the older cancer survivors will be relatively healthy, but this research has highlighted the complexity of the lives of older people living with cancer and their associated support needs.
The narrative MMR methodology offers researchers interested in a range of topics, including inequalities, social justice, and diversity, a tool for putting the experiences of people we are interested in learning more about at the center of the research process. Narrative MMR will appeal to researchers from a range of disciplines who want to integrate stories into the analysis of large quantitative datasets. Further research that utilizes a narrative MMR approach and draws on both stories and the wealth of secondary social survey data available is warranted.
Footnotes
Acknowledgments
We gratefully acknowledge the help of the anonymous referees and journal editors in the preparation of this manuscript. The research on which the paper is based was supported by a Research Impact Scholarship from the University of Manchester, we thank all the participants who contributed to the research. The writing of this article was supported by funding from the Leverhulme Trust.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.