
Abstract
Spindle cell neoplasms of breast comprise both benign and malignant entities. All the soft tissue lesions that comprise spindle cells can be found in the breast. These lesions are rare but their exact diagnosis is of paramount importance in the patient management. Here we present a case of 55 years old female, who presented with complaints of lump in the right breast. On sonomammography, a circumscribed, oval anechoic cystic lesion with eccentric isoechoic soft tissue component was seen in right breast with internal vascularity within the soft tissue component, with a BIRADS 4B score. Fine needle aspiration cytology showed plump to spindle cells in a hemorrhagic background. She underwent right modified radical mastectomy. On gross examination, a gray white well-circumscribed growth with cystic spaces measuring 3.5 × 3.5 × 3.0 cm was seen in upper outer quadrant of right breast. The microscopic examination showed a well-circumscribed lesion with spindle cells arranged in short fascicles and whorls with numerous dilated vascular channels. Spindle cells were seen infiltrating the mammary ducts and adipose tissue, with focal interstitial collagen. Thus a diagnosis of low/intermediate grade of spindle cell lesion of the breast with differential diagnosis of desmoid fibromatosis and pseudoangiomatous stromal hyperplasia was made. On immunohistochemistry, the spindle cells showed diffuse nuclear and cytoplasmic positivity for β catenin, while spindle cells were negative for Pan CK and CD34. Thus a final diagnosis of desmoid fibromatosis of right breast was rendered on immunohistochemistry.
Introduction
Spindle cell lesions of breast cover a wide range of entities. Benign lesions include nodular fasciitis, reactive spindle cell nodule after biopsy, inflammatory pseudotumor/inflammatory myofibroblastic tumor, pseudoangiomatous stromal hyperplasia (PASH), myofibroblastoma, benign fibroblastic spindle cell tumor, leiomyoma, schwannoma, spindle cell lipoma, solitary fibrous tumor and myxoma. 1 It is important to distinguish them from aggressive lesions that show bland appearing spindle cells such as desmoid-type fibromatosis, low-grade (fibromatosis-like) spindle cell carcinoma, low-grade fibrosarcoma/myofibroblastic sarcoma and dermatofibrosarcoma protuberans. 1 Breast fibromatosis is recognized by clonal fibroblastic proliferation. It is a low-grade infiltrative spindle cell neoplasm composed of fibroblasts and myofibroblast. It mimics breast cancer clinically and leads to overdiagnosis and aggressive treatment. Clinical course is variable with high recurrence rates. 2 PASH is a rare benign mesenchymal lesion of the breast commonly seen in premenopausal or perimenopausal women. PASH may present with complaints of breast mass. 3 Microscopic examination generally shows complex, anastomosing, empty, slit like spaces that are lined by spindle cells in a dense collagenous stroma. The recognition of the benign spindle cell tumor-like lesions and tumor is crucial to avoid confusion with morphologically similar lesions.
Case report
A 55 years old female presented to the surgical out-patient department with complaint of lump in right breast which was not increasing in size, not associated with pain or discharge from lump or nipple. There was no history of similar complaint on contralateral side or lump at any other site. There was no history of surgery, trauma or breast implants. On examination, a lump was palpable in upper outer quadrant of her right breast measuring 3 × 3 cm. It was non-mobile and non-tender, with no fixity to chest wall. There was no puckering or dimpling of nipple areola complex. No lymph node was palpable clinically in bilateral axilla. On sonomammography, a circumscribed, oval, anechoic cystic lesion with eccentric isoechoic soft tissue component was seen in upper outer quadrant of right breast measuring 3.5 × 3.3 × 3.1 cm with internal vascularity within the soft tissue component. The lesion had non-parallel orientation to skin and had microlobulated margins in lateral aspect. A grade of BIRAD 4B was given on sonomammography (Figure 1(a)). Computed tomography showed a soft tissue density mass with spiculated margins showing contrast enhancement measuring 31 × 33 × 35 mm in upper outer quadrant of right breast parenchyma. Multiple enlarged lymph nodes were present in right axilla with largest being 11 mm in size. She underwent fine needle aspiration cytology of the mass which showed bland appearing spindle cells with vesicular nuclei against a hemorrhagic background. Spindle cells showed vesicular nuclei and wispy cytoplasm. Few stromal fragments were also seen. (a) Sonomammography showing a circumscribed, oval, anechoic cystic lesion with eccentric isoechoic soft tissue component in right breast with internal vascularity within the soft tissue component. The lesion has non parallel orientation to skin and has microlobulated margins in lateral aspect (BIRADS 4B). (b) Photomicrograph showing a well-circumscribed lesion with spindle cells arranged in short fascicles and whorls with numerous dilated vascular channels (H&E×40). (c) Photomicrograph showing fascicles of spindle cells infiltrating the mammary duct (H&E ×100). (d) Photomicrograph showing fascicles of spindle cells along with interstitial collage (H&E ×100).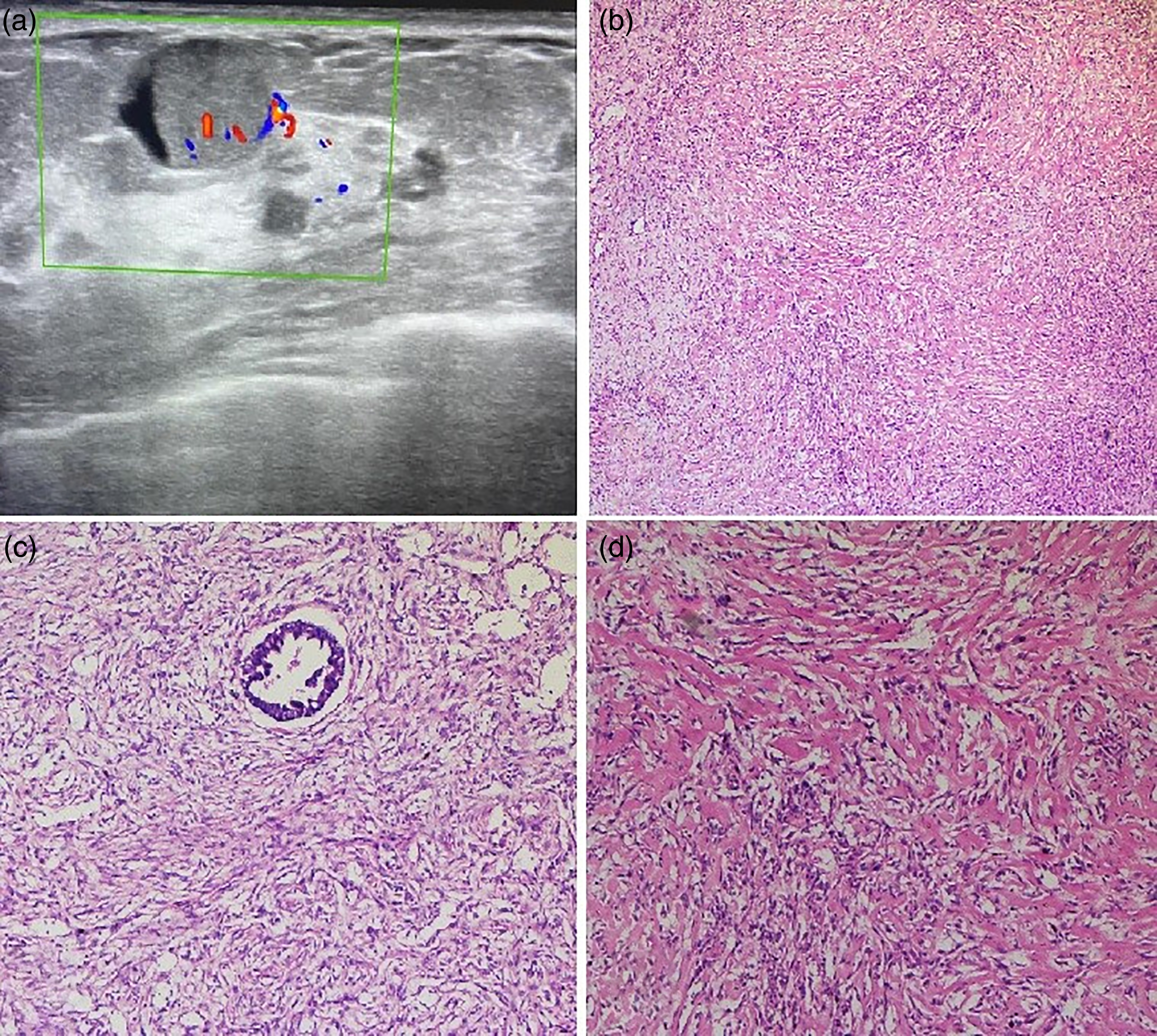
Patient underwent right modified radical mastectomy and on gross examination a gray white well-circumscribed growth with cystic spaces measuring 3.5 × 3.5 × 3.0 cm was seen located in upper outer quadrant. Lesion was not involving nipple areola complex grossly. On microscopic examination, a well-circumscribed lesion with spindle cells arranged in short fascicles and whorls with numerous dilated vascular channels were seen (Figure 1(b)). Slit-like pseudovascular spaces were also seen. Spindle cells were infiltrating the mammary ducts and adipose tissue (Figure 1(c)). Spindle cells were showing mild nuclear pleomorphism with scant cytoplasm. Interstitial collagen was also seen (Figure 1(d)). All the margins and base were free from tumor on microscopic examination. 19 lymph nodes were identified, and all of them showed reactive hyperplasia and were free from tumor deposits. On these morphological findings, diagnosis of low/intermediate grade spindle cell neoplasm of breast was made with desmoid fibromatosis and PASH as the main differential diagnosis. Other differential diagnosis includes fibromatosis-like subtype of metaplastic breast carcinoma, benign phyllodes tumor, nodular fasciitis, myofibroblastoma and solitary fibrous tumor. To confirm the diagnosis, a panel of immunohistochemistry was applied. β-Catenin showed diffuse strong nuclear and cytoplasmic positivity in tumor cells while Pan CK was negative in tumor cells. CD34 was negative in spindle cells; however, normal blood vessels showed CD34 positivity (Figure 2). Pan CK negativity in tumor cells excluded the possibility of metaplastic carcinoma. CD34 negativity in tumor cells excludes the possibility of phyllodes tumor and solitary fibrous tumor. The positivity of β-catenin in tumor cells and negative reactivity for CD34 and Pan CK exclude the possibility of nodular fasciitis and myofibroblastoma. Thus a final diagnosis of desmoid fibromatosis of breast was rendered immunohistochemically. Immunohistochemistry. (a) β-catenin – Spindle cells showed diffuse strong nuclear and cytoplasmic positivity for β-catenin (IHC×100). (b) CD34 – Spindle cells were negative for CD34; however, normal blood vessels showed CD34 positivity (IHC ×100).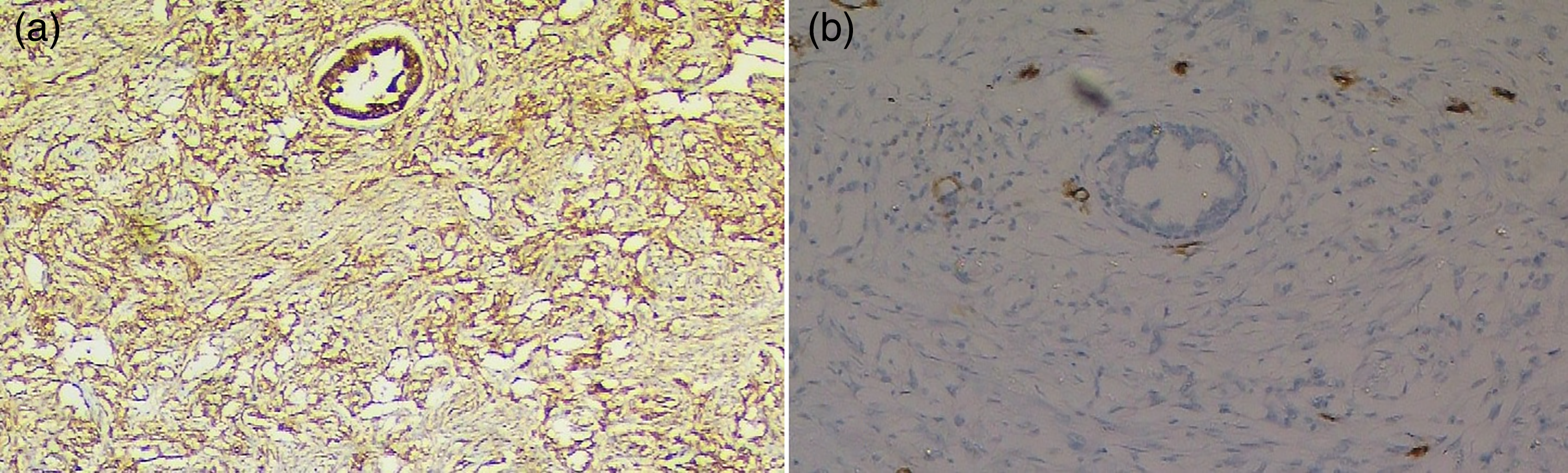
Discussion
Desmoid fibromatosis is a locally aggressive, very rare lesion of the breast, comprising less than 0.2% of all breast tumors.4,5 It presents clonal fibroblastic proliferation. 4 In breast, it arises primary from breast parenchyma; however, they may arise from pectoral fascia of chest wall. 4 It usually presents as ill-defined and irregular mass, with straightening and tethering of cooper ligaments while some cases may show benign appearance. 5 It can be missed on mammography, so combined ultrasound and MRI are preferred radiological investigations, if there is suspicion of fibromatosis. 6 As clinical and radiological findings are often mimic carcinoma breast, fibromatosis is mainly diagnosed on morphological grounds with support of immunohistochemistry. Diagnosis of bland-looking spindle cell lesions of the breast is often challenging because there is a close morphological and immunohistochemical overlap. Most helpful marker is β-catenin which shows aberrant nuclear expression attributed to genetic alteration associated with the lesion. But this finding can be seen in 60–95% cases of phyllodes tumor and sometimes in metaplastic carcinoma. To support the diagnosis, CD34 is helpful as most stromal cell lesions of breast express CD34 except for fibromatosis and nodular fasciitis. Some other markers include SMA and desmin are helpful; however, these markers are non-specific. 7
Pseudoangiomatous stromal hyperplasia (PASH) is a benign proliferative lesion with characteristic slit-like pseudovascular space lined by spindle cells (myofibroblasts). It can also occur in nodular form. 8 If these findings are present, PASH should be kept as one of the differentials. Another differential diagnosis includes nodular fasciitis which is focally infiltrative lesion composed of spindle cells forming short fascicles or storiform pattern with increased mitotic activity and does not display nuclear β-catenin staining. 9
Keeping both the differentials in mind we applied the IHC in present case and final diagnosis of desmoid fibromatosis was given.
Main treatment if diagnosed accurately on radiology and biopsy findings is wide local excision. Since most cases show recurrence within 2 years of surgery, it is of paramount importance to obtain adequate resected margins during surgery. 10 Although negative margins are not reliable indicator to avoid recurrence, some authors have suggested tumor size and negative margins as the factors of recurrence but conclusive evidence is lacking. Many authors have questioned the importance of negative margins as even for benign disease, invasive surgery is required that has a major cosmetic impact on patient. Recently methotrexate based chemotherapy and radiotherapy are being considered as the treatment options. 2 In our case, modified radical mastectomy was performed. Our patient is doing well on 1-year follow-up after surgery.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.