
Abstract
Cardiovascular health (CVH) is both a concept and a measure that refers to health behaviors and clinical factors that help prevent cardiovascular disease (CVD). The neighborhood environment is increasingly recognized as a crucial social determinant of CVH, especially for Black populations. The purpose of this participatory concept mapping (CM) study was to (1) understand perspectives on neighborhood features that influence health and (2) identify which features are most important to achieving CVH behaviors for young Black men. We conducted CM with Black men (n = 30), ages 18 to 34, living in two majority Black communities in one southeastern state. The CM process included three sequential phases—brainstorming, structuring, and interpretation. We defined CVH behaviors as having a healthy diet, healthy weight, engaging in sufficient physical activity, and no tobacco use. Participants depicted neighborhood characteristics across 45 statements that were grouped into eight conceptual clusters. Clusters were rated in terms of relative importance to achieving CVH behaviors. Participants ranked the Economic Opportunity and Health Choices clusters as the most important to achieving CVH behaviors. Conversely, Economic Stressors and Environmental Stressors had the lowest rating of relative importance to achieving CVH behaviors. Pattern matching revealed that average cluster ratings of importance to CVH behaviors achievement were ranked similarly across city type (metropolitan vs. small city) and neighborhood racial composition (most Black vs. racially diverse), but with some nuance. This participant-driven process highlights the neighborhood environment as a meaningful social determinant of fostering or undermining CVH behaviors for young Black men.
Keywords
Introduction
In 2010, the American Heart Association (AHA) introduced Life’s Simple 7 to promote seven modifiable behavioral and clinical factors that prevent CVD and stroke morbidity and mortality (Lloyd-Jones et al., 2010). Life’s Simple 7 health metrics comprise four behaviors: diet, physical activity, smoking status, and body mass index (BMI); and three clinical factors: cholesterol, blood pressure, and fasting glucose. These metrics are used to evaluate cardiovascular health (CVH). CVH, measured both overall and by metric, is categorized as ideal, intermediate, and poor. As overall CVH worsens, the risk of current and future CVD increases. Ideal CVH is characterized by the absence of clinically manifested CVD and the simultaneous presence of a healthy diet, sufficient physical activity, not smoking, healthy weight (i.e., BMI < 25), and optimal cholesterol, blood pressure, and fasting glucose levels without assistance from medication treatment (Lloyd-Jones et al., 2010; Shay et al., 2015). Multiple studies demonstrate that higher attainment of more ideal CVH components is inversely associated with mortality, CVD, stroke, heart failure, cancer, depression, and cognitive decline in U.S. populations (Brewer et al., 2018; Cleary et al., 2023; Guo & Zhang, 2017; Hornbuckle et al., 2024; Kronish et al., 2012; Ogunmoroti et al., 2017; Wang et al., 2023; Yang et al., 2012).
Disparities in CVH exist across race-ethnicity categories. In the United States, Black populations compared to non-Hispanic Asian (hereafter “Asian”) and non-Hispanic White (hereafter White) populations have the lowest attainment of ideal CVH metrics (Benjamin et al., 2019; Martin et al., 2024). Racial status is a social construct, typically measured by physical characteristics (Committee on the Use of Race and Ethnicity in Biomedical Research et al., 2025; Lee et al., 2023). Race is an imperfect risk marker of exposure to racism, which is the primary mechanism through which individuals with less privileged racial statuses disproportionately experience structural barriers that produce observable race differences in well-being, morbidity, and mortality (Cerdeña et al., 2024; LaVeist, 2000; Mayne et al., 2023). Although much of the literature on race and CVH has focused on individual determinants, the neighborhood environment is increasingly recognized as a crucial social determinant of CVH for Black populations, largely due to the impacts of institutional and structural racism (Javed et al., 2022; Powell-Wiley et al., 2022; Yearby, 2020). The majority of current literature has shown that neighborhood built, social, and economic conditions, and racial residential segregation undermine the CVH of Black Americans (Carnethon et al., 2017; Diez Roux et al., 2016; Fullin et al., 2023; Kershaw & Albrecht, 2015). In contrast, cohort studies have shown that favorable features within neighborhood built, social, and economic environments positively influence CVH for Black Americans. For instance, the CARDIA (Coronary Artery Risk Development in Young Adults) study, REGARDS (Reasons for Geographic and Racial Differences in Stroke) study, JHS (Jackson Heart Study), MESA (Multi-Ethnic Study of Atherosclerosis), and MECA (Morehouse-Emory Cardiovascular Center for Health Equity) have shown that access to physical activity resources, healthy food environments, higher neighborhood socioeconomic status (SES), neighborhood safety, and social cohesion are linked to better CVH among Black Americans (Dulin et al., 2022; Foraker et al., 2019; Hines et al., 2023; Islam et al., 2022; Whitaker et al., 2018).
Research has increasingly examined the relationship between neighborhood context and CVH at the intersections of gender and race. A national cohort study on cardiovascular outcomes among middle-aged and older adults examined neighborhood characteristics associated with ideal CVH at the intersection of race and gender (Hines et al., 2023). The authors found that Black-White differences in ideal CVH were partially explained by neighborhood safety (12%) and problems (e.g., violence, heavy or speeding traffic, inadequate food shopping, no or poorly maintained sidewalks) (6%) among men, and discrimination (14%) and neighborhood problems (5%) among women. A cohort study of US Black adults in the South documented a positive association between neighborhood social cohesion and ideal CVH behavior metrics—in particular diet, physical activity, and healthy weight—was more pronounced in Black women compared to men (Islam et al., 2022). A nationally cohort study on health among youth and young adults found that Black-White differences in achieving ≥ 4 ideal CVH metrics among young adult men were not evident when both groups lived in majority-nonwhite residential contexts (Baxter et al., 2021). A limitation of this evidence is its overemphasis on the neighborhood social environment with insufficient consideration of the built environment and their co-occurrence.
While evidence shows that 60% of young adults who maintain at least five ideal CVH metrics significantly reduce their CVD risk in middle age (Diaz et al., 2021; Liu et al., 2012), Young Black men continue to face disproportionately higher risks of developing and dying from CVD prematurely (Benjamin et al., 2019; Curtin et al., 2024). This underscores the importance of including young Black men in place-based health research on CVH and disease. This work is particularly needed in the southern U.S. region, often referred to as the “Stroke Belt” due to its high rates of heart disease and stroke, where more than half of Black men in the U.S. reside (Carnethon et al., 2017; Der Ananian et al., 2018). Black men are also underrepresented in research processes (Nolan et al., 2023; Randolph et al., 2018). Their involvement in health research is hindered by rational distrust of mainstream institutions, disproportionate incarceration rates, limited cultural humility among researchers, lack of cultural and gender sensitivity, and poor recruitment methods (Enyia et al., 2016; Griffith, 2018; Randolph et al., 2018). Community-engaged and participatory approaches to research can mitigate these barriers by fostering mutual trust and redirecting power. In this way, knowledge production shifts from researchers conducting research on or about populations to conducting research with or in service to populations (Randolph et al., 2018; Vaughn et al., 2017). This study used concept mapping (CM), a participatory research method, to conceptualize how the neighborhood environment influences CVH behaviors with young Black men living in two majority Black communities in one southeastern state. Study objectives included (1) understanding young Black men’s perspectives of their neighborhood contexts with respect to health, and (2) identifying aspects of their neighborhood context that were most important to achieve CVH behaviors. In this study, we focused on behavioral components of CVH (diet, physical activity, smoking status, and BMI) rather than clinical factors (cholesterol, blood pressure, and fasting glucose) because these behaviors are foundational to well-being, support attaining clinical factors of CVH, and can be externally observed.
Method
As a structured mixed-methods participatory research approach, CM combines qualitative and quantitative data to visualize conceptual domains for a topic of interest (Burke et al., 2005; Kane & Trochim, 2007). In particular, CM was chosen for its ability to generate rich data and demonstrated success of engaging populations underrepresented in research processes. Our CM effort included three sequential phases—brainstorming, structuring, and interpretation—and took place between February and June 2020. While brainstorming occurred in person (February), the onset of the COVID-19 pandemic required the structuring and interpretation phases to be completed virtually (April-June). For each phase of completion, participants received a $25 VISA gift card. Participants selected an electronic or mailed gift card for their participation in virtual phases. Prior to study initiation, the research team, composed of the lead author (S.L.K.B.) and two graduate research assistants, were trained in the CM process and how to review consent forms (written and electronic versions) with participants. The lead author facilitated each phase and audio-recorded sessions. The structuring and interpretation phases were conducted online using Concept System® groupwisdom™ software and Zoom. This study was approved to conduct human subjects research by the University of North Carolina at Chapel Hill Institutional Review Board (19-2337).
Setting, Recruitment, Eligibility
We conducted CM with young Black men living in two communities, Durham and Rocky Mount, North Carolina (NC). Durham is a metropolitan area located within the urbanized region of Durham County or central NC. Rocky Mount is a small city that uniquely straddles two rural counties, Edgecombe and Nash, in eastern NC. According to the 2020 Census, Durham had a population of 283,506, and Rocky Mount had a population of 54,341. Durham and Rocky Mount are characterized by their high prevalence of Black residents (34% and 63% respectively), which exceeds the state average (22%) (U.S. Census Bureau, 2023). These cities have notable connections to Black history and culture. Durham ranks above state and national averages on various socioeconomic indicators, such as education, household income, poverty rates, and employment (U.S. Census Bureau, 2023). In contrast, Rocky Mount falls below these averages on the same indicators.
Participants were recruited through directed flyers posted on social media platforms, listservs of male-centered organizations, health organizations, and in publicly accessible locations where young Black men coalesce. Eligible participants were residents of Durham or Rocky Mount, self-identified as Black/African American, male, aged 18 to 34 years old, and English-speaking. Participant eligibility was confirmed through a baseline demographic survey that assessed inclusion criteria, demographics, and health profiles. From this survey, 65 individuals met inclusion criteria and were invited to participate in the study. Of those invited, 30 participants provided written consent for this study (46.2% response rate).
Community Advisory Board
A Community Advisory Board (CAB) was assembled to facilitate young Black men’s engagement in health research and maintain community perspectives throughout the research process (Enyia et al., 2016; Randolph et al., 2018). The CAB was composed of one Black woman and five Black men who were identified and selected based on their residence in cities of interest, public health knowledge, and willingness to engage young Black men in health research. Prior to the study’s launch, the CAB helped refine the research focal question and recruitment plan. During the study, the CAB assisted in participant recruitment, refining the list of brainstormed statements, and interpretation of the concept map with participants. CAB members were offered compensation for study-related efforts.
Concept Mapping Procedures
There was overlap in participation across the three CM phases; some participants engaged in only one phase, while others participated in multiple phases. This is consistent with CM procedures that allow flexible involvement, even if just one phase, as long as participants represent the same population pool (Kane & Trochim, 2007). Of the 30 study participants, 11 participated in the initial brainstorming phase. Five participants from this phase, along with 19 new participants, completed the structuring phase. Seven participants from the structuring phase completed the interpretation phase.
Phase 1—Brainstorming
We hosted two in-person brainstorming group discussions, one in each community, with a total of 11 participants. Each session lasted 60 to 80 min. During this phase, participants generated a list of statements in response to a focal question: “What are some features of your neighborhood that could relate in any way to Black men’s health and well-being?” Participants were given 5 min to individually respond to the focal question on an index card and then the group discussion began. To ensure participants across sessions had a similar understanding of the focal question, the research team and CAB presented lay definitions of neighborhood, health, and well-being at the beginning of the brainstorming sessions. The phrase “your neighborhood” was included rather than “Black neighborhoods” to contextualize this study within the selected geographic contexts and counter dominant negative narratives about majority Black neighborhoods. The phrase “in any way” was added to the prompt to allow responses that were positive, negative, or otherwise salient to participant lived experiences. Importantly, the word “well-being” was added to encourage holistic views on health that go beyond illness and the physical health domain. Participants were not provided with the list of statements generated from either session. As participants offered statements, they were written on a board in real-time for others to see. Study investigators (S.L.K.B. and A.J.N.) monitored this growing list of statements, probed for diverse responses, and asked for clarification when needed. All 91 responses from both sessions were compiled in a spreadsheet. Discussions were audio-recorded and used by the research team to understand the nuances of statements. The research team and CAB members individually reviewed these statements and identified ones that were redundant, lacked clarity, or were out of the study’s scope. Statements were removed if three or more reviewers flagged them. Statements flagged by two reviewers were brought to the group to reach consensus on their inclusion or exclusion. This process produced a final list of 45 statements for use in the structuring phase.
Phase 2—Structuring
The structuring phase involved two activities—sorting and rating—where participants individually organized and then prioritized the final list of statements from the brainstorming phase. Twenty-four participants individually completed the structuring phase online with sessions lasting approximately 40 to 60 min in total. For the sorting activity, participants were instructed to independently organize all statements into piles based on conceptual similarity in ways that made sense to them. During this task, participants adhered to the following rules: (1) all statements must be assigned to a pile, (2) piles must contain statements that align with a similar theme, construct, or concept, and (3) create at least two piles (Kane & Trochim, 2007). Participants then labeled piles with a word or short phrase that described perspectives on why the statements were related to each other. Study investigators reviewed piles to confirm that participants sorted every statement into one pile. After completing sorting, participants immediately began the rating activity. For this task, participants independently rated each statement in response to a rating prompt about achieving four CVH behaviors. This prompt asked participants to “rate the relative importance of each statement to Black men having a healthy diet, healthy weight, engaging in physical activity, and no tobacco use.” These ideal levels of diet, physical activity, smoking status, and BMI (weight) were selected among the seven metrics because these behaviors are foundational to attaining CVH (Martin et al., 2024; Whitaker et al., 2018). These behaviors are more easily observed and practically measured by non-health professionals, which makes them less difficult to recall and interpret than cholesterol, blood pressure, and fasting glucose. No standardized definitions or criteria were provided to operationalize healthy diet, healthy weight, physical activity, and tobacco abstinence. This decision was made for two reasons. First, to minimize participant burden that would come from applying formulas or criteria to assess diet, weight, and physical activity, which were more complex than assessing tobacco abstinence. Second, this decision allowed participants to share perspectives grounded in Black men’s shared experiences, which was the study’s focus, not their individual realities. Ratings were based on a five-point Likert-type scale with response anchors of 1 (not at all important) and 5 (essential). Participants were encouraged to use the full range of the scale. Study investigators reviewed participant rating data to ensure participants rated all statements and did not provide the same rating for all statements. Researchers (S.L.K.B. and A.J.N.) were on standby (via Zoom) to support participants during these activities and to review participant work.
Using Concept System® groupwisdom™ software, Participant structuring phase data were converted into individual similarity matrices containing cells that represented the number of times two statements were sorted together. Participant matrices were then aggregated to structure a group similarity matrix that represented the number of times two statements were sorted together across all participants (Kane & Trochim, 2007). Multidimensional scaling (MDS) was used to visualize the group similarity matrix by assigning x, y coordinates to each statement for placement on a concept map. Statements are represented as points on the map; statements that were sorted together more often appear closer together on the map. To evaluate how well the MDS model represents this data, we assessed the stress value, a goodness-of-fit indicator. Optimal stress values range from 0.17 to 0.34 (Kane & Trochim, 2007; Rosas & Kane, 2012). Our map had a stress value of 0.22, indicating a good fit. Next, hierarchical cluster analysis (HCA) was applied to group statements into non-overlapping clusters in terms of similarity based on sorting data (Kane & Trochim, 2007). Concept System® groupwisdom™ software generated several maps, known as cluster maps, which displayed different options for the number of clusters on the map, known as cluster solutions. The research team reviewed all cluster solutions and identified three cluster solutions that we felt displayed a reasonable number of clusters that portrayed distinct concepts.
Phase 3—Interpretation
In a Zoom session, we employed Kane and Trochim’s (2007) protocol with two CAB members and seven willing participants from past phases to review three cluster map solutions and decide which one would be our cluster map. Participation in this phase took approximately 60 min. First, the lead author (S.L.K.B.) re-presented the study’s focal question and made connections between the sorting and rating activities (Phase 2) and points and clusters would appear on the cluster maps. Next, cluster map solutions depicting six, seven, and eight clusters on a map were shared with the group. For each cluster solution, participants were instructed to compare how statements (points on the map) were grouped within clusters and reach consensus on a final cluster map solution that best displayed a distribution of themes or clusters that validated their views toward the focal question—neighborhood features associated with Black men’s health and well-being. Next, the lead author (S.L.K.B.) presented software-generated labels for each conceptual cluster of the final cluster map to the group. These labels were derived from a pool of labels participants contributed during sorting. Short group discussions were held to collaboratively confirm or rename each cluster label. Discussions were audio-recorded and used by the research team to understand the nuances of the chosen cluster map.
After choosing the cluster map, post hoc analyses produced a cluster rating map that depicted the relative importance of each conceptual cluster to key factors that promote CVH behaviors for Black men. In a cluster rating map, each layer beneath a cluster signifies its relative importance compared to other conceptual clusters. Average cluster rating values are used to establish thresholds of relative importance that are then displayed as layers. These values are calculated by averaging the rating scores of all statements within each cluster (Kane & Trochim, 2007).
Results
The distribution of participant characteristics in the CM study is displayed in Table 1. The 30 Black men had an average age of 25.8 (4.6) years old. Most Black men had attained education beyond high school, with 30% (n = 9) reporting no college but high school completion, 23% (n = 7) reporting some college, and 37% (n = 11) reporting a college degree. Most Black men were employed (63%; n = 19), while 17% (n = 5) were unemployed, and 20% (n = 6) were students enrolled in higher education. Most Black men described their neighborhood racial composition as mostly Black residents (57%; n = 17), followed by a good mixture of Black and White residents (33%; n = 10), and mostly White residents (10%; n = 3). Most Black men lived in their respective cities for at least five years (60%; n = 18). Regarding self-reported health characteristics, approximately one-third of the Black men self-reported recent use of tobacco products (37%; n = 11), being overweight or obese (37%; n = 11), and being told by a doctor that they had hypertension or high blood pressure (27%; n = 8). Approximately half (53%; n = 16) of the Black men reported having a routine checkup in the past year.
Distribution of Demographic and Health Characteristics of Black Men Participating in the Concept Mapping Study (N = 30).

Note. Tobacco use was described as smoking a cigarette, e-cigarette, cigar, vaping, or chewing tobacco.
Neighborhood Influences by Cluster
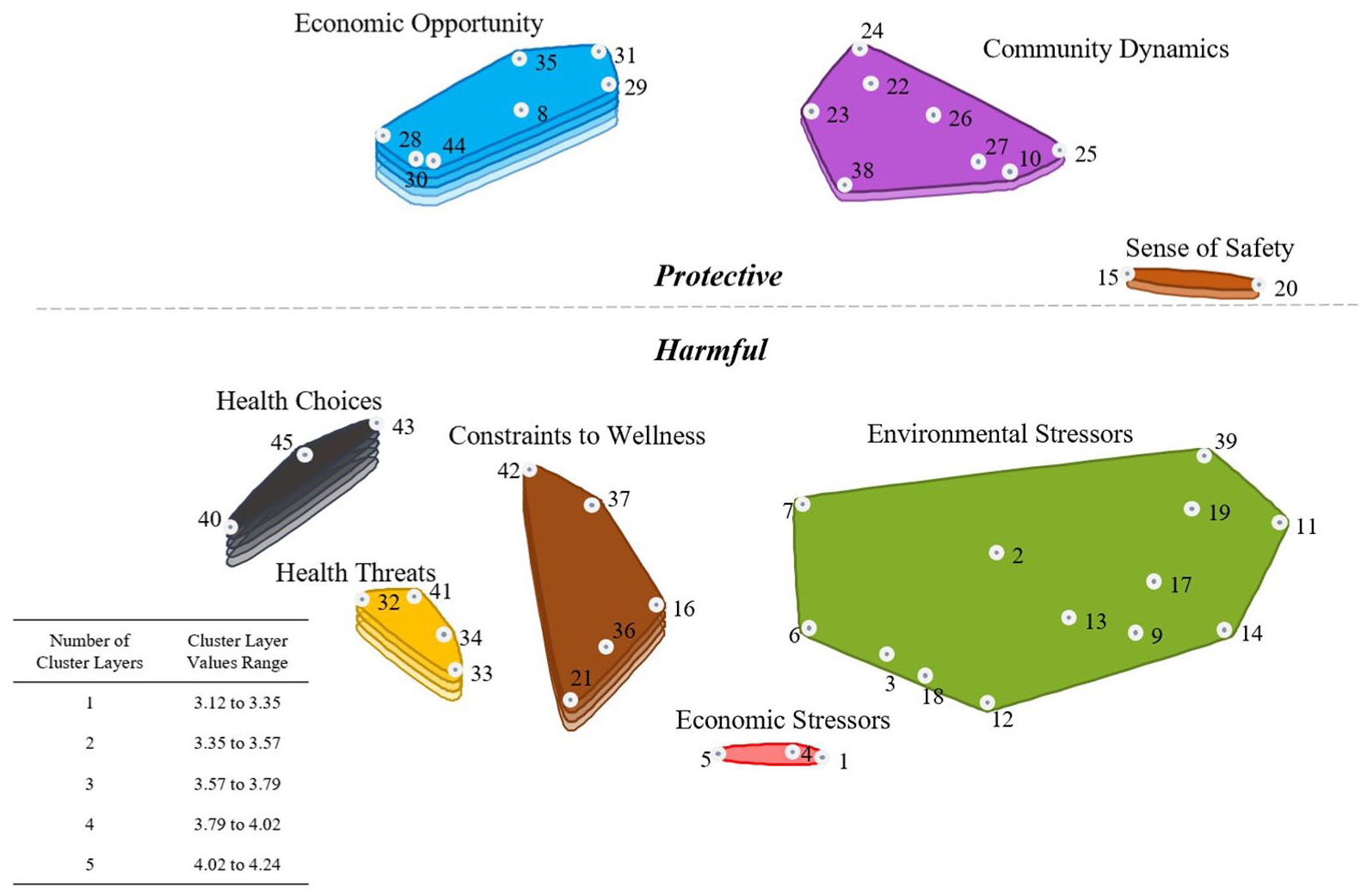
During the interpretation phase, cluster map solutions were reviewed, and the group preferred an 8-cluster solution. This produced a cluster map, Figure 1, that shows how participants conceptualized neighborhood features that influence health and well-being for Black men. During the naming of clusters, the chosen cluster labels were Community Dynamics, Sense of Safety, Environmental Stressors, Economic Stressors, Constraints to Wellness, Health Threats, Health Choices, and Economic Opportunity. The numbered points within clusters indicate each statement’s location on the map. Clusters contain between 2 and 13 statements. Table 2 presents the 45 statements organized within these clusters and the average ratings for clusters and statements.

Final 8-Cluster Map.
Cluster Labels, Numbered Statements, and Average Cluster Rating of Importance to Achieving Cardiovascular Health Behaviors in the Concept Mapping Study.

Note. Clusters are represented according to their average cluster rating of relative importance to achieving cardiovascular health. Numbered statements correspond to the dotted points in Figures 1 and 2. Average cluster ratings correspond to Figure 2.
Likert-type scale values 1 = not important, 2 = somewhat important, 3 = average level of importance, 4 = very important, 5 = essential.
The Community Dynamics cluster depicts aspects of community life and social values that are integral to Black men’s social health. Sense of Safety, the smallest cluster, portrays the precarious link between Black men’s mobility and policing. The Economic Stressors and Environmental Stressors clusters described adverse economic, social, and built environment characteristics, such as financial hardship, neighborhood disorder, and lacking infrastructure. Some Black men wanted to combine these two stressor clusters, but there was no consensus from the group. In Constraints to Wellness, participants highlighted factors that limit Black men’s ability to thrive. Health Threats captured perceptions of obstacles to health care utilization and participation in adverse health behaviors that undermine Black men’s well-being. Health Choices described community conditions that shape health opportunities and behaviors. Finally, the Economic Opportunity cluster reflects key factors that contribute to overall well-being and become more accessible when Black men achieve higher SES individually or within their community.
Near the end of the interpretation phase, some participants noticed a large amount of white space on the cluster map. This observation prompted a group discussion with participants and CAB members that resulted in annotating the cluster map with a dotted line that horizontally partitioned it into two regions. Clusters above the dotted line (Economic Opportunity, Community Dynamics, and Sense of Safety) represent concepts that may protect Black men’s health if maintained or achieved. In contrast, clusters below the dotted line (Health Choices, Health Threats, Constraints to Wellness, Economic Stress, and Environmental Stressors) represent concepts on the map that were deemed harmful to Black men’s health and warrant intervention. For this interpretive element, some Black men were intent that the partition line touch the Sense of Safety cluster, highlighting the precariousness of safety to health for young Black men. Notably, this reflects strong and varied perspectives on the statement “Black police officer living in the neighborhood.” When discussed, some participants resounded Black communities are over-policed and do not need police officers living in them. Others thought both Black residents and police officers may benefit from living among one another. A minority opinion was that community benefits to health should not depend on an officer’s race because officers should protect and serve everyone equally.
Relative Importance to Cardiovascular Health
Figure 2 presents the rating activity results about the relative importance of each cluster to Black men achieving four CVH behaviors—healthy diet, healthy weight, sufficient physical activity, and no tobacco use. On this map, a cluster’s layer(s) depicts its importance in relation to the other clusters, such that more layers signify greater importance than a cluster with fewer layers. Economic Opportunity [4.24] and Health Choices [4.21] were rated as most important for Black men achieving these behaviors, relative to other clusters (Figure 2; 5 layers). The top-rated statements within Economic Opportunity, and among all of the mapped statements, were “access to health care” [4.88] and “practicing good health habits” [4.88]. In Health Choices, the highest-rated statements were “smoking cigarettes” [4.54] and “distance to affordable healthy food” [4.21].
8-Cluster Rating Map.
Health Threats [3.98] and Constraints to Wellness [3.81] were identified as the second most important factors for Black men achieving CVH behaviors, relative to other clusters (Figure 2; 4 layers). The top-rated statements in Health Threats were “not getting enough sleep” [4.22] and “Black men are uninsured in our community” [4.21]. In Constraints to Wellness, the highest-rated statements were “suffering from daily trauma” [4.21] and “distance to grocery stores” [4.21]. Participants rated Community Dynamics [3.55] and Sense of Safety [3.54] as the third most important factors for Black men achieving these behaviors, relative to other clusters (Figure 2; 2 layers). In Community Dynamics, the top-rated statements were “living in a safe neighborhood” [4.46] and “caring about our families” [4.21]. As the smallest cluster, Sense of Safety encompasses two statements. “Being able to walk around” [4.54] was rated as more important to Black men’s attainment of CVH behaviors than “Black police living in neighborhood” [2.54]. Economic Stressors [3.13] and Environmental Stressors [3.12] were rated as the least important factors for Black men achieving these behaviors, relative to other clusters (Figure 2; 1 layer). In Economic Stressors, the top-rated statement was living paycheck to paycheck [4.38]. In Environmental Stressors, the highest-rated statements were “crime rate in area” [4.17] and “parks are not places to play” [4.04].
Figure 3 illustrates two examples of descriptive pattern matching, which compares the agreement of cluster ratings across participant subgroups. Pattern matching is a visual and descriptive technique rather than an inferential test. When comparing Black men living in metropolitan (n = 15; 62%) and small city (n = 9; 38%) areas (Figure 3A), the pattern match showed broadly similar perceptions of cluster importance, but with some nuanced differences. Both groups consistently ranked Economic Stressors and Environmental Stressors as low contributors to achieving CVH behaviors on the pattern match scale. Average cluster ratings were higher among participants from small city areas (3.22–4.37) compared to metropolitan areas (3.05–4.22). Black men from metropolitan areas ranked Economic Opportunity as most important for achieving these behaviors, whereas Black men from small city areas prioritized Health Choices. The Pearson product-moment correlation (r = 0.93) implied an overall strong agreement between how city subgroups rated thematic clusters.

Pattern Matches Across Subgroups.
When we compared participants who described their neighborhood as racially homogeneous or mostly Black (n = 11; 45%) to those who described their neighborhood as more racially diverse (n = 13; 54%) (Figure 3B), the pattern match showed similar perceptions of cluster importance to achieving CVH behaviors, but with slight variations in average cluster ratings. When comparing perceptions across neighborhood racial composition, both subgroups ranked Economic Stressors and Environmental Stressors as least important and Economic Opportunity and Health Choices as most important to achieving these behaviors on the pattern match scale. We observed more dispersion in average cluster ratings among Black men living in mostly Black neighborhoods compared to those living in more racially diverse neighborhoods. This is evidenced by a wider range of average cluster rating ranges among Black men living in mostly Black (3.03–4.38) compared to more racially diverse (3.21–4.13) neighborhoods. Notably, the horizontal line connecting Sense of Safety and Environmental Stressors between groups indicates nearly identical perceptions of importance. The Pearson product-moment correlation (r = 0.97) implied an overall strong agreement between how neighborhood subgroups rated thematic clusters. Neighborhood types were similarly distributed across metropolitian and small city participant subgroups. Among metropolitan participants (n = 15), 46% (n = 7) lived in mostly Black neighborhoods and 54% (n = 8) in racially diverse neighborhoods. Among small city participants (n = 9), 44% (n = 4) lived in mostly Black neighborhoods and 56% (n = 5) in racially diverse neighborhoods.
Discussion
Our study used CM and involved a CAB to conceptualize perspectives on the ways that neighborhood features influence health and well-being, and CVH for young Black men residing in two majority Black southern communities. Our central goal was to prioritize the neighborhood aspects they felt were most important to their achievement of four CVH behaviors: healthy diet, healthy weight, sufficient physical activity, and no tobacco use. The CM process resulted in a map containing eight conceptual clusters—Community Dynamics, Sense of Safety, Environmental Stressors, Economic Stressors, Constraints to Wellness, Health Threats, Health Choices, and Economic Opportunity. Participants characterized these clusters as being either protective or harmful to Black men’s health. They identified Economic Opportunity and Health Choices, originally described as very important, as the most important factors for achieving CVH behaviors. Conversely, Economic Stressors and Environmental Stressors were viewed as having the lowest relative importance, despite being originally described at an average level of importance. While most of these concepts are recognized in literature on the relationship between place, race, and CVD risk and prevention, they are rarely examined together. The study findings collectively illustrate the need for systems thinking and structural interventions to support overall CVH achievement and maintenance among young Black men.
Young Black men recognized Economic Opportunity as the most important to Black men achieving CVH behaviors. Statements within this cluster described positive health behaviors, healthier food options, health care access, and time for leisure activities. The label they gave this cluster demonstrated group consensus around the need for better opportunities for economic advancement that could enable them to live in higher SES communities that would facilitate better opportunities for health and wellness. Americans of lower SES have a higher prevalence of CVD risk factors and poor CVH relative to other SES groups (Bell et al., 2018; Foraker et al., 2019). The widely used theory of fundamental causes supports an understanding of how and why health inequities persist over time through social conditions (Link & Phelan, 1995). In this way, individual SES embodies access to resources, such as money, knowledge, power, and social capital. As an individual’s SES increases, their access to these resources may increase, thus minimizing or altogether avoiding the social consequences of disease and health risks (Link & Phelan, 1995; Phelan et al., 2010). Evidence suggests that higher SES does not confer better health for Black men (Bell et al., 2018; Williams, 2003). This is because racism is a fundamental cause of racial inequities in health and intertwines with SES (Dennis et al., 2021; Phelan & Link, 2015; Williams & Collins, 2001). In health research, race has often been used as an imperfect proxy for racism (Bailey et al., 2017; Fashaw-Walters & McGuire, 2023). Treating race and SES as if they do not simultaneously coexist in spatial and social contexts limits researchers’ ability to effectively understand health inequities. Some research addresses the confounding effects of race and SES by analyzing a range of joint race and SES health differences within various geographic locales (Bell et al., 2018; Hale et al., 2019; Hargrove et al., 2022; Thorpe, Kelley, et al., 2015; Thorpe, Kennedy-Hendricks, et al., 2015). Few studies have assessed the relationship between neighborhood-level SES and CVH (Diez Roux et al., 2016; Foraker et al., 2019; Gebreab et al., 2015). Among the studies that observed a relationship, a cohort study of Black Americans living in the South found that higher levels of individual- and neighborhood-level SES (operationalized as income and education categories) are associated with better CVH (Foraker et al., 2019). Our findings on CVH behaviors align with this emergent line of inquiry and displays the potential interrelated effect of individual and neighborhood SES on CVH among Black men, in particular in the South, as a critical area warranting further exploration.
Health Choices was prioritized as the most important harmful neighborhood factor for achieving CVH behaviors. Participant statements in this cluster emphasized the distance to food that is both affordable and healthy as well as the saturation of fast-food outlets. The rating of this cluster suggests that young Black men perceived their local food environment as a key neighborhood characteristic that structures food choices related to CVH behavior attainment. Two statements, “limited access to, availability, affordability of healthy food” and “an abundance of fast food and convenience stores,” reflect the concept of food apartheid, which refers to the ways racist structures restrict Black communities’ access to healthy, affordable food (Gripper et al., 2022; Nicholson-Robinson et al., 2025; Sherman & Griffith, 2018). Moreover, young Black men residing in the small city and predominantly Black neighborhoods ranked Health Choices as a greater concern for CVH behaviors compared to their counterparts residing in a metropolitan area and more racially diverse neighborhoods. These illustrative differences align with existing literature that shows structural inequalities drive associations between living in community contexts characterized by rurality, low SES, or racial residential segregation and exposure to poor food environments (Baxter et al., 2023; Bell et al., 2019; Goodman et al., 2020; Havewala, 2021; Hines et al., 2022; Jiang et al., 2023; Koob et al., 2023). This finding may support future work that will add to the limited research focused on the relationship between the food environment and eating practices among Black men (Griffith et al., 2016; Sherman & Griffith, 2018). In addition, cigarette smoking was the highest-rated statement in the Health Choices cluster. This may reflect perceptions of cigarette smoking as a means of coping with psychosocial stressors in one’s neighborhood. While often perceived as maladaptive, for some Black men, cigarette smoking and use of other substances are means of coping with racism and other racialized psychosocial stressors (e.g., child hood trauma, community violence, work stress) which may indicate that their CVH behaviors are doubly impacted by such stressors and maladaptive coping strategies (Hicks & Kogan, 2020; Parker et al., 2017; Webb Hooper et al., 2013).
The positioning of Environmental Stressors and Economic Stressors on the cluster rating map and descriptive pattern matches suggests that participants viewed these clusters as related and the least important for achieving CVH behaviors. The consensus of perceptions evident in these ratings reflects an adaptation to the environmental and economic disadvantages associated with living in racially and economically segregated neighborhood contexts that systematically undermine health. Participants’ interpretation of these clusters as least important for CVH behaviors may stem from the perceived normalcy of concentrated exposure to adverse economic, social, and built environment characteristics that perpetuate health disadvantages in non-White communities. These structural arrangements may have shaped participants’ perspectives on health priorities and led them to emphasize neighborhood factors perceived as more immediate or malleable, unlike Environmental Stressors and Economic Stressors that may be viewed as neighborhood conditions that are beyond their influence and “just the way it is” (Shakur, 1998). On the other hand, participants may have rated the Environmental Stressors and Economic Stressors clusters as least relevant to CVH behaviors because the link between the long-standing, adverse conditions and positive health outcomes (i.e., CVH behaviors) may seem more distant in comparison to other clusters. This mirrors tendencies in health research, education, and funding to prioritize poor over positive health outcomes and emphasize investigating short-term determinants over upstream structural influences (e.g., racism and capitalism). Future studies should explore these perspectives.
While the CM study was not designed to test mechanisms of structural racism or segregation, participant-generated data align with previous research on the ways that racial residential segregation is a mechanism through which structural racism functions as a fundamental cause of health inequities (Phelan & Link, 2015; Powell-Wiley et al., 2022; Williams & Collins, 2001). The perceived ordinariness with which participants described Environ-mental Stressors and Economic Stressors reflects the persistence of racial residential segregation, a product of structural racism, that is entrenched in American society and life (Massey, 2012; Williams & Collins, 2001). This normalization is neither random nor incidental; it is a common mechanism that makes systematic disadvantage appear common and inevitable, leaving inequities embedded within neighborhoods and other social determinants unnamed and unquestioned in society (Ford & Airhihenbuwa, 2010a, 2010b; Jones, 2018; Powell-Wiley et al., 2022; Yearby, 2020). In this way, health advantages disproportionately accrue to White individuals because racial residential segregation grants majority White neighborhoods greater access to social and built environment features that promote health. Conversely, people living in neighborhoods with fewer White residents have less access to such features and a greater risk of worse health outcomes. Research suggests that the built, social, and economic environments of neighborhoods are critical social determinants of health that facilitate race disparities in CVH and CVD risk (Baxter et al., 2021; Carnethon et al., 2017; Hines et al., 2023; Whitaker et al., 2018). Relatedly, the Program for Men’s Health Research at Johns Hopkins University has published comparative studies showing that no differences in depression or CVD risk were observed among Black and White men living in racially integrated urban communities with similar income levels (Hale et al., 2019; Thorpe, Kelley, et al., 2015; Thorpe, Kennedy-Hendricks, et al., 2015). This work strengthens the argument that neighborhood environments characterized by racial and economic integration, where White and non-White residents are exposed to the same resources and risk features, are critical social determinants of men’s health outcomes.
As an interpretive element, the dotted line dividing the clusters into regions of protective and harmful neighborhood factors on the map touched the Sense of Safety cluster, which reflects varied perspectives to the statement “Black police officer living in the neighborhood.” The historical legacy and daily experiences of police encounters and violence in the United States elicited varied reactions to this statement (Alexander, 2020; Gilbert & Ray, 2016; Gordon, 2020; Pinckney et al., 2018). When probed to relate police officer presence in the community to CVH behaviors, participant responses indicated that police officer presence in the community may be a neighborhood stressor that both promotes and undermines CVH behaviors. For example, the presence of police officers may promote abstaining from tobacco use (a CVH behavior) by discouraging smoking outdoors to avoid suspicion of marijuana use in places where it is not fully legalized. Conversely, police officer presence may undermine physical activity (another CVH behavior) by discouraging outdoor exercise for fear of harassment and violence. Recent literature has increasingly examined police encounters within studies on the relationship between community violence and cardiovascular outcomes, with mixed findings among Black adults (Allgood et al., 2024; Bey et al., 2020; Hines et al., 2023; Walker et al., 2024). Hines et al. (2023) observed that neighborhood safety and problems in the physical environment, partly defined as violence, were the largest contributors to differences in CVH between Black and White men. Looking across the life course, Bey et al. (2020) observed no association between discrimination by the police or courts during young adulthood and CVH two decades later for Black men or women. In contrast, Allgood et al. (2024) observed that higher police encounters were associated with lower CVD risk scores among Black men, but not among White men. Taken together, these findings call attention to the importance of how police encounters are perceived and the health effects of coping strategies enacted to address this stressor. More research is needed to understand how coping strategies to police presence and encounters in community settings affect CVH and disease risks.
Several study limitations warrant cautious interpretation of the findings presented. First, generalizability is limited to young Black men residing in similar southern environments due to purposive sampling in one state in the southeastern region of the United States. The findings reflect the sample and moment of data collection, so generalizability over time or other contexts is limited. Second, for the rating prompt related to CVH behaviors, participants were not given formal definitions of healthy diet, healthy weight, physical activity, or no tobacco use. This was done to minimize respondent burden and center participant perspectives on the experiences of Black men and not their own. Young Black men may have drawn on their general knowledge and self-report of weight status and tobacco use (see Table 1) to discern what “healthy” meant for other Black men in these categories. Still, this may have introduced some bias in the statement rating activity. Results from the cluster rating map and pattern matching focused on neighborhood influences should be interpreted with this in mind. Here, we clarify that the interpretation of descriptive pattern matching results is primarily visual and qualitative. The Pearson correlation coefficient reflects the degree of agreement in cluster ratings between subgroups and is not an inferential test. In this mixed-methods approach, pattern matching is an illustrative technique to explore consistency in perceived cluster importance across subgroups. Subgroup comparisons should be interpreted cautiously and are intended to highlight alignment in agreement and nuance rather than support statistical inference.
Despite these limitations, this CM study has several strengths. First, CM effectively centered the perspectives and lived experiences of young Black men, an understudied population enduring inequities in CVH that is seldom engaged in health research (Adams et al., 2021; Enyia et al., 2016; Griffith, 2018; Joseph et al., 2022). Second, the study’s sample size of 30 participants fit well within the recommended range of 10 to 40 to establish a robust analysis, as evidenced by the low stress value (Kane & Trochim, 2007). Third, although the sample focused on young Black men, it was heterogeneous in terms of educational attainment, health status, and neighborhood racial composition.
Implications
Dominant narratives and interventions on CVD prevention or CVH promotion typically focus on lifestyle changes without addressing the role that social and structural determinants, such as neighborhood context, play in promoting a healthy lifestyle. The insights gained from this study underscore the importance of adopting a systems thinking approach to address CVH behaviors among young Black men living in predominantly Black and southern communities. The prioritization of Economic Opportunity (i.e., the need for better opportunities for economic advancement) and Health Choices (i.e., community conditions that shape health opportunities and behaviors) as critical factors for CVH suggest that structural interventions targeting these areas could yield substantial benefits. Conversely, the identification of Economic Stressors and Environmental Stressors as less salient highlights the need for implementing comprehensive strategies that are based on assessing the relevance and importance of various social determinants of CVH. Structural interventions are a public health strategy designed to address the structural contexts in which health is produced and reproduced (Blankenship et al., 2006). In turn, structural interventions may address the political, social, and economic factors that are the root causes of CVH disparities. This approach requires collaborative efforts across sections to dismantle structural barriers and promote environments conducive to positive health outcomes. Systems thinking is a useful tool to effectively understand these barriers and design structural interventions. Systems thinking integrates perspectives from multiple disciplines to emphasize how a system’s structure, existing interconnections, and understandings of behavior drive or delay behavior change (Arnold & Wade, 2015; Matson et al., 2022). In viewing neighborhoods as systems, systems thinking models may be useful for unpacking the complex and multilevel pathways that influence CVH behaviors among young Black men.
Conclusion
CM is a useful tool to explore and visualize a group’s ideas about a topic. This study used CM to conceptualize and prioritize the influence of neighborhood features on behavioral components of CVH for young Black men living in majority Black and southern communities in the United States. Participant-driven results identified 45 statements grouped within eight conceptual clusters to describe a range of neighborhood features that affect health and well-being, and the achievement of four CVH behaviors. Participants perceived three clusters as fostering and five clusters as undermining Black men’s CVH behavior achievement. These findings contribute to the growing body of evidence investigating the effects of neighborhood environments on structuring CVD risk, specifically among Black populations. The understanding gained from this CM study provides support for hypotheses and future systems thinking approaches and structural interventions that address young Black men’s ability to engage in CVH behaviors and health longevity where they reside.
Footnotes
Acknowledgements
We are grateful to the community advisory board members who provided guidance and support for this research. In addition, we appreciate the graduate students who worked on this research with the lead author. Finally, we thank the anonymous reviewers for their input on the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Baxter was supported by the Health Policy Research Scholars, a program of the Robert Wood Johnson Foundation. Dr. Thorpe Jr.’s contribution was supported by NIH Grants: K02AG059140 and U54MD000214.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Study participants in this study were assured that raw data would remain confidential and would not be shared.