
Abstract
Expectant fathers who struggle to cope with the fear of childbirth often develop negative attitudes toward attending birth. This study aimed to compare fear of childbirth and attitudes toward participation in birth among expectant fathers with primiparous and multiparous partners. The researchers conducted this prospective comparative study with 142 expectant fathers, including 70 fathers with primiparous partners and 72 fathers with multiparous partners. The study used a Personal Information Form, the Fathers’ Fear of Childbirth Scale (FFCS), and the Attitude Scale Toward Participation in Birth for Father Candidates (ASTPBFC) to collect data. Fathers with primiparous partners reported significantly higher levels of fear of childbirth than fathers with multiparous partners
Introduction
Labor is a physiological event that brings about numerous changes in the lives of expectant mothers and expectant fathers (Bruno et al., 2020; Vischer et al., 2020). Although labor represents a natural process, it often causes stress, anxiety, and fear in mothers. Physiological, mental, and psychological factors affecting mothers may also lead to emotional distress in expectant fathers (Sercekus et al., 2020). Psychological stress experienced by expectant fathers can negatively affect their ability to provide emotional and physical support to their partners during pregnancy (Johansson et al., 2021).
Researchers define fear of childbirth as a negative cognitive, emotional, and psychological evaluation of labor or as perceiving labor with anxiety and fear (Hofberg & Brockington, 2000; Stoll & Hall, 2013). In clinical practice, clinicians generally classify fear levels as low, moderate, severe, or phobic fear (Larsson, 2017). Numerous studies have examined the prevalence of fear of childbirth among mothers (Gokce Isbir et al., 2024; Ilska et al., 2021; Nasr et al., 2020; Onchonga et al., 2020). In contrast, researchers have reported inconsistent findings regarding the prevalence of fear of childbirth among expectant fathers (Hildingsson et al., 2014; Sahin et al., 2023). However, a limited number of studies indicate that approximately 32% of expectant fathers experience moderate fear of childbirth (Xue et al., 2024). Expectant fathers often report fear related to potential threats to the health of the mother and infant, possible birth complications, the unpredictability of the labor process, and concerns about fulfilling the paternal role. Evidence shows that men, particularly first-time expectant fathers, experience a sense of unreality upon learning about the pregnancy, along with excitement and fear related to the birth process. They also report anxiety, inadequacy, and powerlessness when facing new roles and responsibilities associated with fatherhood (Colciago et al., 2022; Poh et al., 2014). Studies indicate that 13%–80% of first-time expectant fathers experience these emotions, which often become more pronounced during the third trimester of pregnancy (Escott et al., 2009; Labrague & McEnroe-Petitte, 2016). Fear of childbirth may lead expectant fathers to perceive the upcoming birth negatively and to favor cesarean birth (Sercekus et al., 2020).
Factors such as expectant fathers’ fear of the birth process, uncertainty, and lack of information influence not only birth preferences but also participation in childbirth. In Sweden, health care systems first allowed fathers to participate in childbirth in the late 1950s, and other European countries addressed this issue in subsequent years (Davran, 2019). In developing countries, the rate of expectant fathers’ participation in childbirth has gradually increased (Darwin et al., 2017; Poh et al., 2014). Karacam and Karatepe (2020) reported that men wish to actively participate in their partners’ births.
Research demonstrates that expectant fathers’ participation in childbirth increases maternal satisfaction with the birth experience, reduces obstetric interventions, strengthens mother–infant and father–infant attachment, and enhances spousal harmony (Darwin et al., 2017; Maken et al., 2018). Women whose partners participate in childbirth report greater satisfaction with the birth experience, show a stronger preference for vaginal birth, and demonstrate higher breastfeeding rates and longer breastfeeding duration. Spousal support plays a critical role in helping women feel supported and experience pregnancy, childbirth, and the postpartum period more positively and healthily (Royal College of Midwives, 2015).
In Türkiye, no study has directly examined the prevalence of expectant fathers’ attendance at childbirth; however, Timur Tashan and Duru (2018) found that 34.5% of fathers expressed a desire to attend childbirth. Expectant fathers in Türkiye began participating in childbirth later than those in many other countries, primarily because sociocultural norms discouraged the presence of companions during birth and because of restrictive institutional policies (Karacam & Karatepe, 2020; Sercekus Ak et al., 2018). Traditionally, health care systems excluded fathers from the birthing process; however, recent initiatives have aimed to increase expectant fathers’ involvement in childbirth (Timur Tashan & Duru, 2018). Currently, expectant fathers can attend births primarily in private hospitals and in state hospitals designated as mother-friendly hospitals. Türkiye launched the Mother-Friendly Hospital Program in 2011, and the program became more widespread after 2015. This initiative enabled expectant fathers to participate in childbirth and provide support to their partners (Sercekus Ak et al., 2018). To ensure a positive birth experience, especially for first-time expectant fathers, preparation for the childbirth process remains essential. The first step involves identifying expectant fathers’ fear of childbirth and their attitudes toward participation in birth. Therefore, health care providers should assess expectant fathers’ fear of childbirth and attitudes toward attending birth during pregnancy and plan appropriate interventions accordingly. Accordingly, this study aimed to compare fear of childbirth and attitudes toward participation in childbirth among expectant fathers with primiparous and multiparous partners.
Methods
Study Design
The researchers designed this study as a prospective study. They conducted it between June 1 and September 1, 2024, with expectant fathers whose partners were primiparous or multiparous pregnant women attending the obstetrics and gynecology outpatient clinic of a private LIV hospital in Türkiye. The department secretary provided information about expectant mothers who attended the clinic with their spouses and whose gestational age was ≤36 weeks. After the obstetric examinations, the researchers conducted face-to-face interviews with expectant fathers in a private and suitable room within the maternity ward. The study hospital (Private LIV Hospital) had an obstetrics and gynecology outpatient clinic staffed by seven physicians, a delivery unit with 20 delivery rooms, a family planning outpatient clinic, and an in vitro fertilization center. The institution did not offer antenatal education classes, and none of the expectant fathers participating in the study had received prenatal education. The hospital records approximately 1,200 births annually.
Sample
The study population consisted of all expectant fathers whose primiparous or multiparous partners attended the obstetrics and gynecology outpatient clinic of the private LIV hospital. The researchers calculated the sample size using power analysis based on previous studies (Mortazavi et al., 2023; Rashidi et al., 2023). They performed the analysis using G*Power version 3.9.1 and determined that a minimum sample size of 140 participants was required for the two groups combined (α = .05, 1 − β = .95), assuming a large effect size (d = 0.61) for differences in fear of childbirth between expectant fathers with primiparous and multiparous partners (Cohen’s d = 0.6119848).
During data collection, the researchers approached 76 expectant fathers with primiparous partners and 74 expectant fathers with multiparous partners. Six expectant fathers with primiparous partners withdrew from the study because of difficulties related to work schedules or time constraints and two expectant fathers with multiparous partners transferred to a higher-level health care facility. Consequently, the final sample included 142 participants: 70 expectant fathers with primiparous partners and 72 expectant fathers with multiparous partners (see Figure 1). The researchers did not follow expectant fathers during the postpartum period. Because the study included only expectant fathers whose partners had a gestational age of ≤36 weeks, the planned mode of delivery was known; however, the researchers could not determine emergency cesarean delivery rates.

Flow Plan of the Expectant Fathers Participating in the Study.
The study included expectant fathers who volunteered to participate, had no communication barriers, whose partners had no pregnancy-related complications, and whose partners were ≤36 weeks of gestation. The researchers excluded expectant fathers who declined participation, and whose partners experienced pregnancy complications or were ≥36 weeks of gestation.
Data Collection
Before data collection, the researchers informed expectant fathers about the purpose of the study and emphasized that participation was entirely voluntary and that they could withdraw at any time without consequences. The researchers obtained written and verbal informed consent from all participants using the Informed Voluntary Consent Form. They prepared all consent forms and data collection tools in Turkish. Expectant fathers who agreed to participate completed the data collection forms individually.
Data Collection Tools
Personal Information Form
The Personal Information Form included questions related to the sociodemographic characteristics (e.g., age, educational level) of expectant fathers and pregnancy-related characteristics of their partners (e.g., gestational week, planned mode of delivery).
Fathers’ Fear of Childbirth Scale
Ghaffari et al. (2020) developed the Fathers’ Fear of Childbirth Scale (FFCS) to assess fathers’ fear related to childbirth. The scale evaluates two dimensions: fear related to the birth process (Items 1–12) and hospital-related fear (Items 13–17). The FFCS includes 17 items rated on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). Calpbinici et al. (2024) conducted psychometric analyses of the scale in Turkish culture and demonstrated that the FFCS is a valid and reliable instrument for assessing fear of childbirth among Turkish expectant fathers. Total scores range from 17 to 85, with scores of 17–35 indicating low fear, 36–54 indicating moderate fear, and 55 or higher indicating high fear of childbirth. Higher scores reflect greater fear of childbirth. The original scale demonstrated a Cronbach’s alpha internal consistency coefficient of .93. In the present study, the researchers calculated a Cronbach’s alpha coefficient of .89.
Attitude Scale Toward Participation in Birth for Father Candidates
Cicek Ozdemir and Kan (2022) developed the Attitude Scale Toward Participation in Birth for Father Candidates (ASTPBFC). The scale consists of 26 items rated on a 5-point Likert-type scale ranging from 1 (completely disagree) to 5 (completely agree). The scale includes 18 positively worded items and 8 negatively worded items. The positively worded items include M1, M2, M3, M6, M8, M14, M19, M20, M26, M33, M35, M40, M44, M13, M16, M25, M30, and M36, whereas the negatively worded items include M10, M23, M29, M32, M34, M37, M38, and M42. The scale comprises three subscales: the first subscale includes Items M1, M2, M3, M6, M8, M14, M19, M20, M26, M33, M35, M40, and M44; the second subscale includes Items M10, M23, M29, M32, M34, M37, M38, and M42; and the third subscale includes Items M13, M16, M25, M30, and M36. Total scores range from 26 to 130, with higher scores indicating more positive attitudes toward participation in childbirth among expectant fathers. The original scale demonstrated a Cronbach’s alpha internal consistency coefficient of .96. In this study, the researchers calculated a Cronbach’s alpha coefficient of .90.
Data Analysis
The researchers entered all data into SPSS for Windows (IBM Corp., Armonk, NY, USA) and conducted the analyses using this software. They used descriptive statistics, including percentages, mean values, and standard deviations, to summarize participants’ characteristics. To compare expectant fathers’ descriptive characteristics and mean scale scores, the researchers applied independent-samples t-tests. They used the chi-square test to assess group similarity with respect to control variables. The researchers examined the moderating effect of age to determine whether expectant fathers’ age influenced the relationships examined in the study. To assess multicollinearity, they calculated variance inflation factor (VIF) values. VIF values greater than 5 indicate potential concern, whereas values above 10 represent a critical threshold (Menard, 2010).
Ethics
The researchers obtained written approval for the study from the Gaziantep University Clinical Research Ethics Committee (May 2, 2024; No. 2024/139) and from Private LIV Hospital. They obtained both verbal and written informed consent from all participants after providing detailed information about the study. The researchers conducted the study in accordance with the principles of the Declaration of Helsinki, as revised in Brazil in 2013.
Results
Table 1 presents the descriptive characteristics of the 142 expectant fathers, including 70 fathers with primiparous partners and 72 fathers with multiparous partners. The mean age of expectant fathers with primiparous partners was 30.17 ± 3.63 years, whereas the mean age of expectant fathers with multiparous partners was 33.82 ± 5.10 years. None of the expectant fathers in either group had attended antenatal classes (100%). The analyses revealed no statistically significant differences between expectant fathers with primiparous and multiparous partners in terms of demographic characteristics, indicating that the groups were comparable (p > .05; Table 1).
Descriptive Characteristics of the Expectant Fathers.

Note.
None of the expectant fathers in either group had attended antenatal classes (100%).
Expectant fathers with primiparous partners reported a higher mean total score on the FFCS; 52.24 ± 12.74) than expectant fathers with multiparous partners (42.50 ± 13.16). The results indicated that fear of childbirth was significantly higher among expectant fathers with primiparous partners (p < .05). Analysis of the FFCS subdimensions showed that expectant fathers with primiparous partners scored higher on the birth process subdimension (42.32 ± 12.62) than those with multiparous partners (31.22 ± 10.71; p < .05). The groups did not differ significantly in terms of the hospital fear subdimension (p > .05). Regarding attitudes toward participation in childbirth, expectant fathers with primiparous partners had a lower mean total score on the Attitude Scale toward Participation in Birth for Father Candidates (ASTPBFC; 62.35 ± 14.91) than expectant fathers with multiparous partners (74.54 ± 19.82). Expectant fathers with multiparous partners demonstrated significantly more positive attitudes toward attending birth (p < .05). Subdimension analyses revealed that expectant fathers with multiparous partners scored higher on the positive emotions subdimension (38.23 ± 12.87) than expectant fathers with primiparous partners (29.12 ± 8.59; p < .05). The groups did not differ significantly in the negative emotions subdimension (p > .05). However, expectant fathers with multiparous partners reported higher scores on the actions toward attending birth subdimension (18.69 ± 4.79) compared with expectant fathers with primiparous partners (14.34 ± 3.54; p < .05; Table 2).
Comparison of the Mean Scores of Fear of Childbirth and Attitudes Toward Participation in Birth Scales and Their Subdimensions.

Note. t: Independent sample t-test.
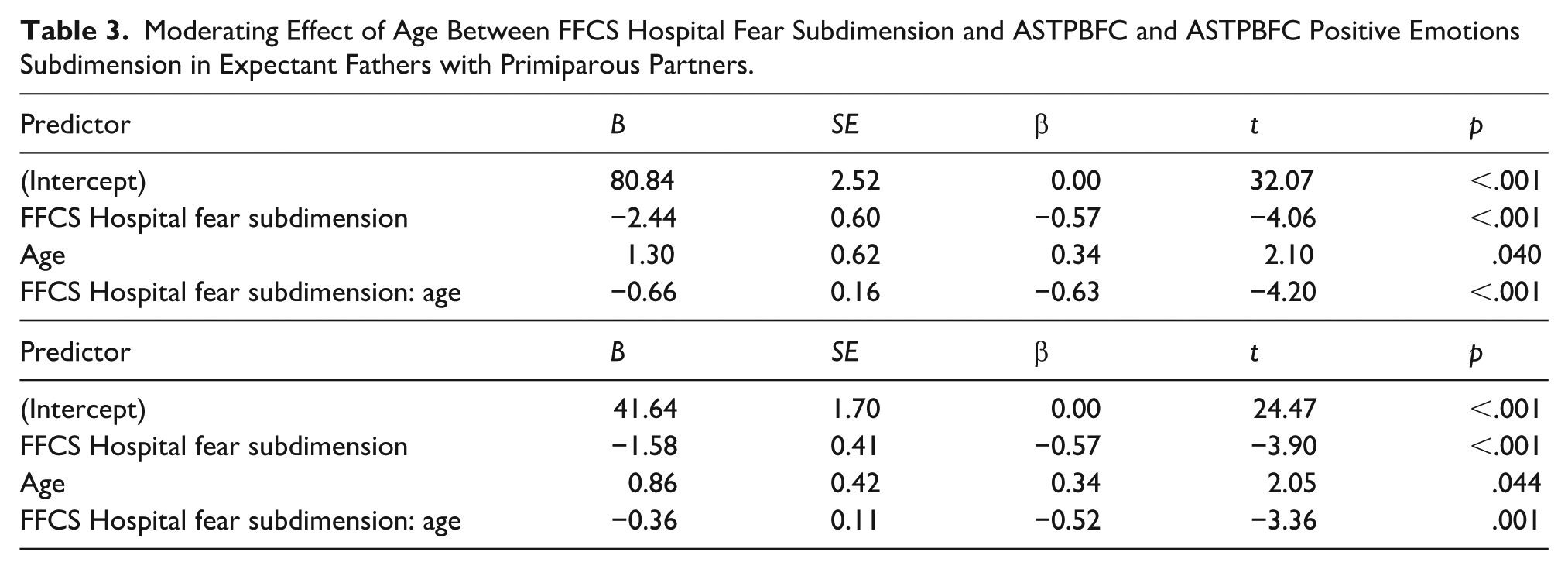
Among expectant fathers with primiparous partners, age demonstrated a significant main effect, B = 1.30, t(68) = 2.10, p = .040. When age was fixed at zero, a one-unit increase in the FFCS hospital fear subdimension predicted a decrease of 2.44 units in the ASTPBFC score. The interaction between age and the FFCS hospital fear subdimension was significant, B = −0.66, t(68) = −4.20, p < .001, indicating that the effect of hospital-related fear on attitudes toward participation in childbirth weakened as age increased. Age explained 22.20% of the variance in the ASTPBFC positive emotions subdimension among expectant fathers with primiparous partners. The interaction between age and the FFCS hospital fear subdimension also significantly predicted positive emotions, B = −0.36, t(68) = −3.36, p = .001, further indicating a diminishing effect of fear as age increased (Table 3).
Moderating Effect of Age Between FFCS Hospital Fear Subdimension and ASTPBFC and ASTPBFC Positive Emotions Subdimension in Expectant Fathers with Primiparous Partners.
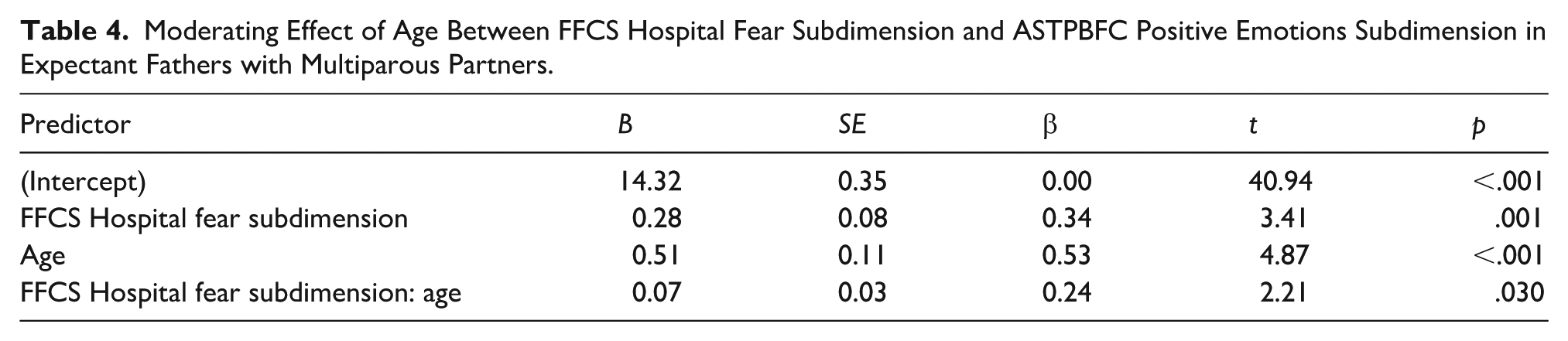
Among expectant fathers with multiparous partners, age explained 34.99% of the variance in the ASTPBFC positive emotions subdimension. The interaction between age and the FFCS hospital fear subdimension was significant, B = 0.07, t(66) = 2.21, p = .030, suggesting that the effect of hospital-related fear on positive emotions toward participation in childbirth strengthened as age increased. When age was fixed at zero, a one-unit increase in the FFCS hospital fear subdimension predicted an average increase of 0.28 units in the ASTPBFC positive emotions subdimension (Table 4).
Moderating Effect of Age Between FFCS Hospital Fear Subdimension and ASTPBFC Positive Emotions Subdimension in Expectant Fathers with Multiparous Partners.
Discussion
Expectant fathers who experience fear of childbirth often prefer medical interventions, particularly cesarean birth, as a strategy to cope with the uncertainty associated with labor and birth (Moran et al., 2021). In addition, expectant fathers who struggle to manage the fear of childbirth tend to develop negative attitudes toward attending birth. For this reason, fear of childbirth represents an important issue that requires attention, particularly in countries with high birth rates. Previous studies have examined expectant fathers’ fear of childbirth (Rashidi et al., 2023; Sercekus et al., 2020; Xue et al., 2024) as well as their attitudes toward participation in childbirth (Cicek Ozdemir & Kan, 2022; Karacam & Karatepe, 2020). However, to the best of our knowledge, no previous study has directly compared fear of childbirth and attitudes toward participation in childbirth between expectant fathers with primiparous and multiparous partners. In this respect, the present study contributes novel findings to the literature.
The study included a total of 142 expectant fathers, 70 with primiparous partners, and 72 with multiparous partners, with a mean age of 32.02 ± 4.78 years. Most participants had a university-level education, worked in private-sector positions, reported adequate income levels, and lived in nuclear families. These characteristics may have influenced participants’ perceptions of childbirth and their attitudes toward participation in the birth process.
Fear of Childbirth in Expectant Fathers
In this study, expectant fathers reported a moderate level of fear of childbirth, and expectant fathers with primiparous partners (52.24 ± 12.74) experienced higher levels of fear than those with multiparous partners (42.50 ± 13.16). Previous research suggests that first-time expectant fathers often experience heightened fear because of concerns about fulfilling the paternal role, limited knowledge of the birth process, lack of prior parenting experience, younger age, and unresolved fear experienced by their partners (Hildingsson et al., 2014). In Türkiye, Sercekus et al. (2020) reported that 54.3% of expectant fathers experienced fear of childbirth, supporting the findings of the present study. Consistent with our results, studies conducted in developing countries indicate that expectant fathers frequently experience moderate to high levels of fear of childbirth. For example, Rashidi et al. (2023) reported that Azerbaijani expectant fathers experienced moderate fear of childbirth (mean score = 48.39 ± 14.10), which significantly increased anxiety and depression levels. Similarly, Ghaffari et al. (2020) found that expectant fathers in Iran reported high levels of fear of childbirth. In China, Xue et al. (2024) reported a fear of childbirth prevalence of 32.1% among expectant fathers. In Kenya, Onchonga et al. (2020) found that fear of childbirth occurred more frequently among expectant fathers with primiparous partners (13.8%) than among those with multiparous partners (8%). In contrast, studies conducted in developed countries such as Germany, Sweden, and the United States have reported relatively low levels of fear of childbirth among expectant fathers (Hildingsson et al., 2014; Hunter et al., 2011; Kannenberg et al., 2016). Several studies have also examined the relationship between age and fear of childbirth among expectant fathers. Sercekus et al. (2020) reported significantly higher fear levels among expectant fathers aged 25–35 years compared with those older than 35 years. In contrast, Schytt and Bergström (2014) observed higher fear levels among fathers aged 43 years and older (29%) than among those aged 42 years (27%) and 38 years (17%).
Analysis of the FFCS subdimensions revealed that expectant fathers with primiparous partners scored higher on the birth process subdimension than those with multiparous partners. For first-time expectant fathers, the birth process often represents an unfamiliar experience characterized by uncertainty, excitement, anxiety, and concern about their partner’s pain and well-being (Colciago et al., 2022). Therefore, first-time expectant fathers may experience greater fear related to the birth process than fathers who have previously experienced childbirth. Regarding the hospital fear subdimension, expectant fathers with primiparous and multiparous partners reported moderate levels of fear, with no significant difference between the groups. Concerns about the competence of health care professionals, anxiety related to the hygiene and safety of the birth environment, and fear of medical errors or malpractice may contribute to hospital-related fear among expectant fathers (Colciago et al., 2022; Moran et al., 2021).
Attitudes Toward Participation in Birth Among Expectant Fathers
In this study, expectant fathers generally demonstrated positive attitudes toward attending childbirth. The positive attitudes observed may relate to the study sample characteristics, as participants received care at a private hospital, had relatively high educational attainment, and reported adequate income levels. These factors may increase awareness of paternal involvement and facilitate more supportive attitudes toward participation in childbirth. However, expectant fathers with primiparous partners (62.35 ± 14.91) demonstrated more negative attitudes toward attending birth than expectant fathers with multiparous partners (74.54 ± 19.82). In addition, expectant fathers with multiparous partners reported more positive emotions related to participation in childbirth. Limited knowledge of the birth process, heightened fear of childbirth, anxiety related to hospital procedures, and prevailing cultural beliefs that discourage fathers’ presence during labor may explain the more negative attitudes observed among expectant fathers with primiparous partners. In contrast, prior parenting experience among expectant fathers with multiparous partners may contribute to greater confidence and more positive attitudes toward participation in childbirth (Cicek Ozdemir & Kan, 2022). Furthermore, some expectant fathers may avoid participation in childbirth because of concerns about experiencing psychological distress or trauma during the birth process. Numerous studies have examined expectant fathers’ views on participation in childbirth. In Türkiye, Duru (2014) found that 71.8% of first-time expectant fathers expressed a desire to attend childbirth. Similarly, Davran (2019) reported that although expectant fathers wished to attend childbirth, hospital policies often prevented their participation in Türkiye. In Australia, Kothari et al. (2023) reported that 99% of expectant fathers wanted to attend childbirth, and the study also showed that positive attitudes toward participation increased with age. In contrast, a study conducted in developed countries such as France and Switzerland indicated that expectant fathers perceived participation in childbirth as a significantly anxiety-provoking experience (Franzen et al., 2021).
The Relationship Between Fear of Childbirth and Attitudes Toward Participating in Birth
The present study also revealed a negative relationship between expectant fathers’ fear of childbirth and their attitudes toward attending birth. As the fear of childbirth increased, positive attitudes toward participation in childbirth decreased. Factors such as fear of the birth process, uncertainty, and lack of information may contribute to this relationship. To the best of our knowledge, no previous study has directly examined the effect of expectant fathers’ fear of childbirth on their attitudes toward attending birth, highlighting the originality of the present findings.
Furthermore, the findings indicated that the effect of hospital-related fear on positive attitudes toward attending birth weakened with increasing age among expectant fathers with primiparous partners, whereas this effect strengthened with age among expectant fathers with multiparous partners. Previous studies have suggested that as fathers age, they may develop more negative expectations about childbirth and perceive labor as more challenging or distressing (Bergström et al., 2013; Schytt & Bergström, 2014). In addition, the sources of fear appear to change with age: younger expectant fathers tend to experience fear related to socioeconomic concerns, whereas older expectant fathers more frequently report fear related to the moment of birth and the responsibilities of parenthood (Bergström et al., 2013). Although no previous studies have examined the moderating role of age in the relationship between fear of childbirth and attitudes toward attending birth, research investigating age-related differences in fear of childbirth among expectant fathers has produced mixed findings. Some studies have reported increased fear with advancing age (Eriksson et al., 2005; Schytt & Bergström, 2014), whereas others have shown that fear decreases as age increases (Franzen et al., 2021; Sercekus et al., 2020).
Clinical Implications
To enable expectant fathers to effectively support their partners during the sensitive transition to parenthood, midwives and nurses should actively include expectant fathers, along with expectant mothers, throughout the childbirth process. Health care professionals should engage directly with expectant fathers to understand their preferences and perspectives regarding participation in childbirth, listen to their concerns and fears, and provide encouragement. In addition, health care providers should invite expectant fathers to participate in childbirth preparation classes together with their partners (Schobinger et al., 2024). This inclusive approach may help reduce expectant fathers’ fear of childbirth (Souza Vidal Lima et al., 2021), enhance their ability to support their partners (Anjum et al., 2023), facilitate a smoother transition to fatherhood (Noh, 2021), and contribute to a more positive birth experience with fewer medical interventions (Wynter et al., 2021).
Conclusion
This study demonstrated that expectant fathers experienced a moderate level of fear of childbirth, with higher fear levels observed among expectant fathers with primiparous partners. Expectant fathers with multiparous partners reported more positive attitudes toward participation in childbirth. The findings also indicated that expectant fathers’ age played an important role in moderating the relationship between fear of childbirth and attitudes toward attending birth. Based on these results, increasing the number of mother-friendly hospitals and expanding opportunities for expectant fathers to participate in antenatal education programs is recommended. In addition, future research should include samples from state hospitals and incorporate participants from diverse cultural backgrounds.
Limitations of the study
Although no precise data exist regarding the prevalence of expectant fathers’ attendance at childbirth in Türkiye, estimates suggest that participation remains below desired levels because of institutional policies and traditional practices (Cicek Ozdemir & Kan, 2022). The relatively positive attitudes toward participation in childbirth observed in this study may reflect the characteristics of the sample, which consisted primarily of expectant fathers with higher income and education levels who received care at a private hospital. These factors limit the generalizability of the findings.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883251414637 – Supplemental material for A Comparison of Fear of Childbirth and Attitudes Toward Participation in Birth in Expectant Fathers With Primiparous and Multiparous Partners
Supplemental material, sj-docx-1-jmh-10.1177_15579883251414637 for A Comparison of Fear of Childbirth and Attitudes Toward Participation in Birth in Expectant Fathers With Primiparous and Multiparous Partners by Kaplan Dogan E in American Journal of Men's Health
Supplemental Material
sj-docx-2-jmh-10.1177_15579883251414637 – Supplemental material for A Comparison of Fear of Childbirth and Attitudes Toward Participation in Birth in Expectant Fathers With Primiparous and Multiparous Partners
Supplemental material, sj-docx-2-jmh-10.1177_15579883251414637 for A Comparison of Fear of Childbirth and Attitudes Toward Participation in Birth in Expectant Fathers With Primiparous and Multiparous Partners by Kaplan Dogan E in American Journal of Men's Health
Footnotes
Acknowledgements
The researcher thanks all fathers participating in this research project.
Ethical Consideration
Written permission for this study was obtained from Gaziantep University Clinical Research Ethics Committee (Date: 02.05.2024 no: 2024/139) and Private LIV Hospital. Verbal consent and written consent forms were obtained from the participants. All participants were informed about the study. This study was conducted in accordance with the provisions of the Declaration of Helsinki as revised in Brazil in 2013.
Author Contribution
EKD; concept, design of the study, collection, analysis and interpretation of data, writing and revision.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The dataset of this study is available corresponded author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.