
Abstract
Mindfulness (Mind) intervention as a psychological treatment is adopted in the sports field, its effect during competition has not been fully explored yet. This study examined the impact on cognitive performance following laboratory-controlled mindfulness intervention lasting 16 weeks. In a single-blind randomized crossover design, 90 college table tennis athletes meeting inclusion criteria were randomly assigned to either a control (Con) group or a mindfulness (Mind) group. The Mind group underwent a 16-week mindfulness intervention (8 minutes/session, 4 sessions/week) after training, while the Con group continued with life-as-usual at that time. Cognition, cerebral oxygenation, emotion state, salivary cortisol, and mental fatigue were measured at baseline (pretest) and post-intervention (posttest). Long-term mindfulness intervention significantly improved cognitive performance, e.g., attention concentrativeness, attention span, distractibility, instantaneous memory, short-term memory, long-term memory, supported by eliciting increased oxyhemoglobin concentration in the left and right medial prefrontal cortex (mPFC). A better emotional state and a lower mental fatigue level as well as lower cortisol concentration were observed in the Mind group than in the Con group after the intervention at posttest. A 16-week mindfulness intervention can improve emotional state, reduce subjective fatigue, improve cognition and increase cerebral oxygenation. In general, mindfulness training is recommended for table tennis athletes during competition.
Introduction
Contemporary sport psychology underscores the cognitive-emotional synergy in athletic performance, particularly among college athletes (Weber et al., 2023). While facing shared mental health challenges (e.g., anxiety/depression) with non-athletes (Edwards & Froehle, 2023; Pluhar et al., 2019), college athletes experience heightened stress from academic demands and rigorous training pressures, requiring superior emotional regulation for competitive success (Lopes Dos Santos et al., 2020). In addition, they required greater cognitive flexibility, especially in open-skill sports like table tennis (Lai et al., 2024) and volleyball (Montuori et al., 2019), to adapt to dynamic competitive environments. Therefore, developing cost-effective interventions has become a research priority in athlete development.
Mindfulness has emerged as a noninvasive, present-focused cognitive training method gaining prominence in sport psychology (Bühlmayer et al., 2017). This practice cultivates nonjudgmental present-moment awareness through experiential acceptance protocols, demonstrating efficacy in reducing stress/anxiety among adolescent-to-young adult populations (Jones et al., 2020; Lin et al., 2019). Its nonclinical modality offers particular advantages for implementation in college athletic. Importantly, table tennis is characterized by its fast pace and open-skill nature, requiring rapid decision-making, refined perceptual-motor integration, and maintained emotional control under competitive pressure (Liu, 2025). These specific demands thus render its practitioners an exemplary cohort for investigating the enhancement of core neural and psychological processes through mindfulness training.
Research on athletes has shown that mindfulness-based interventions enhance athletes’ (1) Sport performance. Improved performance in shooting (Josefsson et al., 2021), basketball, table tennis (Tebourski et al., 2022), and rowing (Sparks & Ring, 2022), with higher levels of awareness, refocusing, and awareness being related to better sport performance in competitions. (2) Cognition & mental health. Reductions in performance anxiety and enhancements in executive function have been observed (Beenen et al., 2025; Chen et al., 2018; Myall et al., 2023). An event-related potential study revealed that mindfulness program positively affected the participating athletes’ cognitive functions, including executive functions, while also increasing the efficiency of conflict resolution in neural processes (Nien et al., 2020). Research incorporating functional near-infrared spectroscopy (fNIRS) has demonstrated that enhanced cognitive function following mindfulness practice is underpinned by increased prefrontal cortex activation and heightened cerebral oxygenation (Mohanty et al., 2024). (3) Physiological markers. Changes in prefrontal hemodynamics response, glucose/lactate levels, and muscle pain perception have been documented (Adachi & Takizawa, 2024; Zhu et al., 2020). While existing research has established links between mindfulness interventions and cognitive/mental health in athletes, the neurological processes driving these effects are still not fully understood.
While mindfulness studies in athletes are growing, few have simultaneously examined its effects on cognitive, emotional, and neurophysiological outcomes within the same cohort. Furthermore, we note a scarcity of research focusing on the unique cognitive demands of racket sports like table tennis using functional neuroimaging. This study examined the effects of extended mindfulness-based training on athletes’ emotional regulation and cognitive functioning. Participants in the experimental condition completed 8-minute mindfulness practice sessions. Using near-infrared spectroscopy (NIRS), we compared prefrontal cortical hemodynamic patterns during cognitive tasks to assess how sustained mindfulness practice influences neurophysiological and psychological outcomes. Drawing upon existing literature, we hypothesized that compared with the Con group, the Mind group would (1) exhibit a better cognitive performance and emotional regulation, supported by increased oxyhemoglobin concentration in the bilateral mPFC; (2) show reduced mental fatigue and hypothalamic-pituitary-adrenal (HPA) axis activation, as indicated by lower cortisol secretion.
Methods
Study Design
This randomized controlled trial adopted a crossover design, implemented at Beijing, China between March and August 2024. Following eligibility assessment through screening procedures, subjects underwent randomization into either the experimental intervention group or the normal group. Prior to baseline assessments, participants were randomly assigned using a 1:1 allocation scheme. To maintain probably-blinded ratings, all participants received explicit directives to refrain from discussing their group assignments throughout the study duration.
Participants
We recruited table tennis athletes from a public university in Beijing, China. Eligibility was determined based on the following inclusion criteria: (a) age between 19 and 26 years; (b) willingness to accept random allocation; (c) right-hand dominance; and (d) normal communication abilities and normal or corrected-to-normal vision. Exclusion criteria were as follows: (a) history of serious injuries in the past six months; (b) cardiovascular or other medical conditions that could interfere with physical exercise interventions; (c) current diagnoses of psychosis, bipolar disorder, active suicidality, untreated post-traumatic stress disorder, or substance use disorder within the previous three months; (d) presence of cognitive, physical, or visual impairments; (e) prior participation in a mindfulness-based course lasting two weeks or longer; or (f) current involvement in another intervention study. The physical education teacher, physician, and principal investigator were collectively responsible for developing the eligibility criteria and implementing the screening process.
The screening process initially involved 100 participants, with 10 meeting exclusion criteria. The reasons for exclusion were as follows: one participant were left-handed; three declined random allocation; two reported a history of injury in the past six months; and four were concurrently participating in other sports intervention studies. Of these eligible candidates, 90 underwent stratified randomization (intervention group: n=45; normal group: n=45). Final analysis included 71 participants (intervention group: n=39; normal group: n=32) completed the study, as described in the diagram of participation flow in Figure 1. In addition, The participant was required to sign written informed consent for their participation, and all procedures were in accordance with the institutional ethical standards, which was in accordance with the 1964 Declaration of Helsinki.

The Diagram of Participation Flow of This Study.
Treatment
The experimental group received a mindfulness-based training program. The intervention was delivered four times per week over 16 weeks. Each session comprised an 8-minute mindfulness induction using a guided audio recording, which consisted of two sequential components: (1) Mindfulness breathing stage. Mindfulness breathing was played at the beginning and the end of the audio for about 2 min, respectively, e.g., focus on your body and pay attention to your breathing; slowly, take a deep breath and breathe in, breathe out. (2) Body scan meditation. In body scan meditation, the audio’s core segment comprised a 4-minute body scan meditation, such as: feel the weight or pressure on the soles of the feet, the slight tremor of the muscles. The practice is fundamentally characterized by cultivating a nonjudgmental, accepting attitude to consciously attend to present-moment experiences (Zhu et al., 2022). The intervention was delivered by a research assistant who underwent a specialized training program for this study. The training included: (a) a thorough review of the intervention manual; (b) 20 hours of didactic sessions on the principles and techniques of mindfulness; (c) multiple role-playing sessions; and (d) piloting the entire protocol with non-participants. Fidelity to the protocol was monitored throughout the study by the principal investigator. The time of the control group is the same as that of the experimental group (6 min), and life as usual.
Treatment Compliance and Fidelity. To monitor participant compliance, we implemented a multi-faceted approach: (1) Attendance records were meticulously maintained for all intervention sessions, with a predefined adherence criterion of ≥85% attendance for inclusion in the per-protocol analysis; (2) Daily practice logs were provided to participants, who were instructed to record the duration and frequency of their home-based mindfulness exercises, which were reviewed weekly by the research team to provide reminders and support; and (3) Brief engagement surveys were administered at the mid-point and post-intervention to subjectively assess participants’ adherence to the practice guidelines outside of sessions. To ensure intervention fidelity, the following procedures were established: (1) A manualized protocol was developed prior to the study, specifying the objectives, core components, and time allocation for each session, which was rigorously followed by the instructor; (2) The interventionist, a certified mindfulness practitioner, underwent specific training on this protocol to ensure consistent delivery; and (3) As a key objective fidelity check, approximately 20% of the sessions, selected at random, were audio-recorded and reviewed by an independent research assistant using a standardized fidelity checklist. This checklist confirmed that all key components were delivered as intended, with no major protocol deviations observed.
Measures
A blinded physiotherapist, unaware of treatment group allocations, conducted standardized assessments of all outcome measures at both baseline and post-treatment evaluation phases.
Five facets mindfulness questionnaire To obtain behavioral scores for mindfulness, the Five Facets Mindfulness Questionnaire (FFMQ) was adopted to evaluate mindfulness status. This validated instrument evaluates five core dimensions of mindfulness: (1) Observing, (2) Describing, (3) Acting with Awareness, (4) Nonjudging of Inner Experiences, and (5) Nonreactivity to Inner Experience. Each subscale contains eight items except Nonreactivity (seven items). Participants evaluated each statement using a 5-point Likert-type scale (1 = “Never” to 5 = “Very often”). Dimension-specific scores were calculated by summing the responses within each facet, while comprehensive FFMQ scores represented the aggregate total across all subscales for individual participants (Yue et al., 2023).
Cognition task Cognitive function was assessed using the Jingshiren Psychological Test Software (BRRZ01001, Beijing, China). The assessment comprised four subtests: (1) Attention concentrativeness. The subject needs to focus their attention on the center of the screen, and they were required to remember the number of targets they observed, responding as quickly as possible. Upon completing their response, they should press the spacebar to initiate the next trial. (2) Attention span. A character matrix will be displayed on the screen. The subject is required to systematically scan the matrix row by row from left to right and top to bottom. Whenever a target character is identified, left-click to mark it. Responses should be made as quickly as possible while maintaining accuracy. (3) Distractibility. After the test begins, letters will be displayed in rapid succession. It is critical to memorize all red-letter stimuli and monitor whether the letter X emerges following any red letter presentation. (4) Immediated memory. A character matrix will be centrally displayed on the screen and will disappear after a brief interval. The subject must recall and record the content of the vanished matrix, then press the spacebar to advance to the next set. (5) Short-term memory. A character string will be centrally displayed on the screen. Subjects are required to memorize both the character string and their presentation sequence to the fullest extent. After completing the intervening activity, the subject required to recall the original stimuli in sequential order. (6) Long-term memory. Arrows pointing in four directions (up, down, left, right) with two thickness levels will be serially presented at screen center. Following each stimulus presentation, the subject must immediately recall both the directional orientation and thickness of arrows in sequential order.
fNIRS data The multi-channel fNIRS device was used to monitor changes in oxyhemoglobin concentration of the dorsolateral prefrontal cortex at all times during a cognitive task. As previously described (Izzetoglu & Holtzer, 2020; Vitorio et al., 2017), the study employed an fNIRS Imager 1100 system (Sampling rate: 2Hz) with integrated anti-aliasing filters to monitor the dorsal and anterior prefrontal cortical hemodynamics. The fNIRS sensor comprised four LED light sources ((peak wavelengths was 730, 805, and 850 nm) and 10 photodetectors arranged in a eight-channel covering the frontal region. The head cap has light sources secured 30 mm apart, with each detection point centered in the detection area, and the device includes specific brain area markers to guarantee precise monitoring. fNIRS data were processed in MATLAB 2021Ra with the DOT-HUB and Homer2 toolboxes. During preprocessing, channels were excluded if the source–detector distance exceeded 50 mm or the coefficient of variation surpassed 10%, thereby reducing data dimensionality. Motion correction was subsequently applied via spline interpolation (p = .99) to remove movement artifacts and maintain signal continuity. A bandpass filter (0.01–0.1 Hz) was then used to suppress slow drifts, high-frequency oscillations, and cardiac interference. Group-level hemodynamic responses were obtained by averaging the time courses across participants, and these analyses were performed in OriginPro 2021b. The tissue saturation index (TSI) in the frontal cortex is operationally defined as [oxy-Hb][Total-Hb] × 100% and reflects the dynamic equilibrium between cerebral oxygen delivery suppl and metabolic consumption (Song et al., 2024).
Emotional evaluation Emotional status was measured at baseline and post-intervention. The primary outcome was anxiety symptoms measured with the State-Trait Anxiety Inventory (STAI). This questionnaire comprises two parts of 40 items, utilizing a 4-point Likert-type-scale (1 = Strongly Disagree, 2 = Disagree, 3 = Agree, 4 = Strongly Agree). The STAI-State quantifies the severity of acute anxiety symptoms, while the STAI-Trait operationalizes baseline anxiety characteristics (Esteves et al., 2021). The total score was calculated as the sum of all 40 items, ranging from 20 to 80 points, with higher scores indicating greater severity of anxiety symptoms. The Cronbach’s alpha reliability coefficient for the STAI in our study was 0.83. Depress were a secondary outcome assessed using the Beck Depression Inventory (BDI). The BDI comprises 21 self-rated items assessing four symptom domains: cognitive, affective, conative, and somatic. Total scores ranged from 0 to 63 points and were stratified as: 0-4 (asymptomatic), 5-7 (mild), 8-15 (moderate), and ≥16 (severe), with higher values demonstrating increased depressive symptom severity. This self-rating scales for depression exhibited internal consistency and validity in non-psychiatric patient populations (Guo et al., 2024). The Cronbach’s alpha reliability coefficient for the BDI in our study was 0.86. The Subjective Happiness Scale (SHS) is a psychometric instrument that quantify self-reported perceptions of global life satisfaction and hedonic well-being (Zhang et al., 2024). The scale consists of four items, each scored on a 7-point Likert-type scale. The sum of these items yields a possible total score ranging from 4 to 28, with higher scores denoting elevated perceptions of subjective happiness. The Cronbach’s alpha reliability coefficient for the SHS in our study was 0.80.
Mental fatigue evaluation The Rating of Perceived Exertion (RPE) scale were used to evaluate athlete’s mental fatigue. The subject was instructed to self-report numerical values from 0 (complete rest) to 10 (maximal exertion) based on their instantaneous physiological state (Table 1). An increased RPE rating corresponds to elevated perceived exercise intensity (Shen et al., 2022).
Borg’s RPE-10 Scale.

Cortisol Determinations Salivary cortisol level was collected by salivary collection kits to obtain the required specimen and accomplished through the ELISA procedure. Briefly, participants deposited 1-2 mL of saliva into a sterile saliva collector, which was then transferred to a centrifuge tube (5ml) preloaded with nucleic acid stabilization buffer. Following vortex homogenization, samples were cryopreserved at 4°C. The determinations of salivary cortisol were accomplished through the ELISA procedure, using the cortisol assay kit (H094-1-2, Nanjingjiancheng, China) (Honceriu et al., 2023).
Statistical Analyses
Power analyses were based on the assumption that mindfulness-based training, relative to control, will lead to improvement in cognition, emotion and fNIRS with an effect size of 0.69 (power of 83%, two-tailed α = .05). A total of 71 participants were included in the analysis: 39 in the intervention group and 32 in the control group. Before analysis, the experimental raw data for all variables will be assessed for normality. Subsequently, statistical analyses were performed using SPSS 22.0 and GraphPad Prism 8.0. The primary analytical approach involved repeated-measures analysis of variance (ANOVA) with mixed models, followed by Tukey’s Honestly Significant Difference (HSD) post hoc, with statistical significance set at p < .05.
Results
Effects of Interventions on Mindfulness Measures
Notably, analysis of the observing subscale revealed a significant interaction, with scores demonstrating exclusive improvement in the mindfulness group, indicating that the time-dependent changes on this subscale were specifically attributable to the mindfulness intervention Figure 2. This was supported by the following results for the Time × Group interaction: FFMQ Total, F(1, 69) = 8.56, p < .05, partial η2 = 0.06, 95% confidence interval (CI) [0.01, 0.14]; FFMQ Observing, F(1, 69) = 4.00, p < .05, partial η2 = 0.03, 95% CI [0.02, 0.09]. The interaction for FFMQ Awareness was also significant, F(1, 69) = 22.10, p < .05, partial η2 = 0.14, 95% CI [0.05, 0.24]. Thus, the meditation intervention was successful.
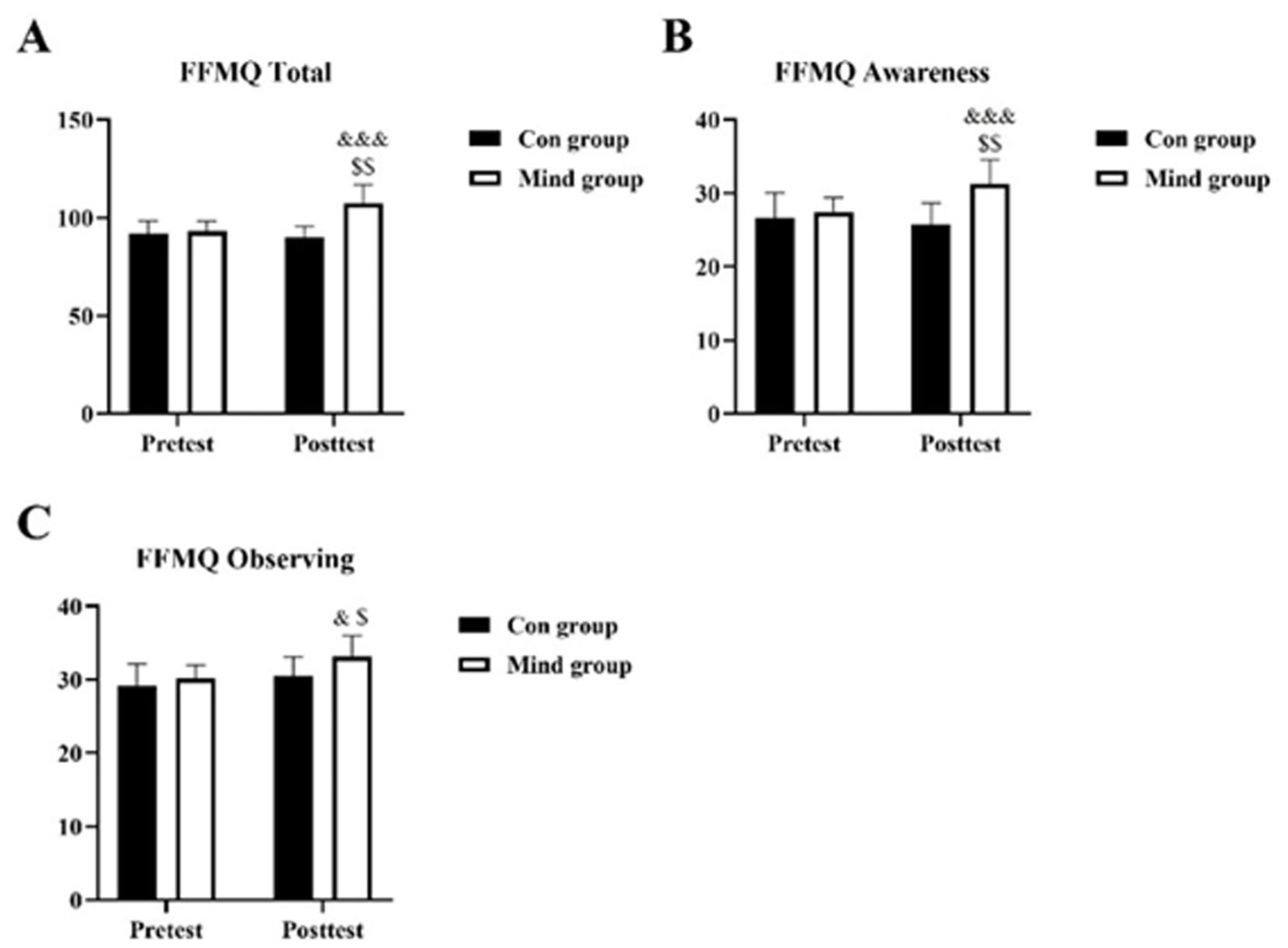
Self-Reported Mindfulness Measures Improved After Intervention.
Effects of Interventions on Cognition Outcomes
On cognition outcomes, the main effect of time was significant: Attention concentrativeness, F(1, 69) = 9.201, p < .05, partial η2 = 0.09, 95% CI [0.02, 0.20]; Attention span, F(1, 69) = 19.21, p < .05, partial η2 = 0.18, 95% CI [0.06, 0.31]; Distractibility, F(1, 69) = 3.62, p < .05, partial η2 = 0.04, 95% CI [0.00, 0.12]; Instantaneous memory, F(1, 69) = 9.36, p < .05, partial η2 = 0.09, 95% CI [0.02, 0.20]; Short-term memory, F(1, 69) = 5.46, p < .05, partial η2 = 0.06, 95% CI [0.01, 0.16]; Long-term memory, F(1, 69) = 4.749, p < .05, partial η2 = 0.05, 95% CI [0.01, 0.14]. The main effect of intervention mode was significant: Attention concentrativeness, F(1, 69) = 9.201, p < .05, partial η2 = 0.09, 95% CI [0.02, 0.20]; Attention span, F(1, 69) = 3.838, p < .05, partial η2 = 0.04, 95% CI [0.02, 0.12]; Distractibility, F(1, 69) = 19.21, p < .05, partial η2 = 0.18, 95% CI [0.06, 0.31]; Instantaneous memory, F(1, 69) = 2.724, p < .05, partial η2 = 0.03, 95% CI [0.00, 0.10]; Short-term memory, F(1, 69) = 9.363, p < .05, partial η2 = 0.09, 95% CI [0.02, 0.20]; Long-term memory, F(1, 69) = 23.55, p < .05, partial η2 = 0.21, 95% CI [0.08, 0.34]. Furthermore, there was a significant interaction between time and intervention mode: Attention concentrativeness, F(1, 69) = 16.87, p < .05, partial η2 = 0.16, 95% CI [0.05, 0.28]; Attention span, F(1, 69) = 9.201, p < .05, partial η2 = 0.09, 95% CI [0.02, 0.20]; Distractibility, F(1, 69) = 19.21, p < .05, partial η2 = 0.18, 95% CI [0.06, 0.31]; Instantaneous memory, F(1, 69) = 2.724, p < .05, partial η2 = 0.03, 95% CI [0.00, 0.10]; Short-term memory, F(1, 69) = 9.363, p < .05, partial η2 = 0.09, 95% CI [0.02, 0.20]; Long-term memory, F(1, 69) = 12.72, p < .05, partial η2 = 0.12, 95% CI [0.03, 0.24].
From Figure 3, it can be found that in preintervention, the cognition outcomes were no significantly difference both the Con and Mind groups (p > .05). At poststage, all the cognition subscale score showed intervention effect and increased after intervention for Mind groups than that Con group (p < .05). In addition, the cognition subscale results showed a time effect, with an increase in subscale score only in the mindfulness intervention group but not the Con group (p < .05).
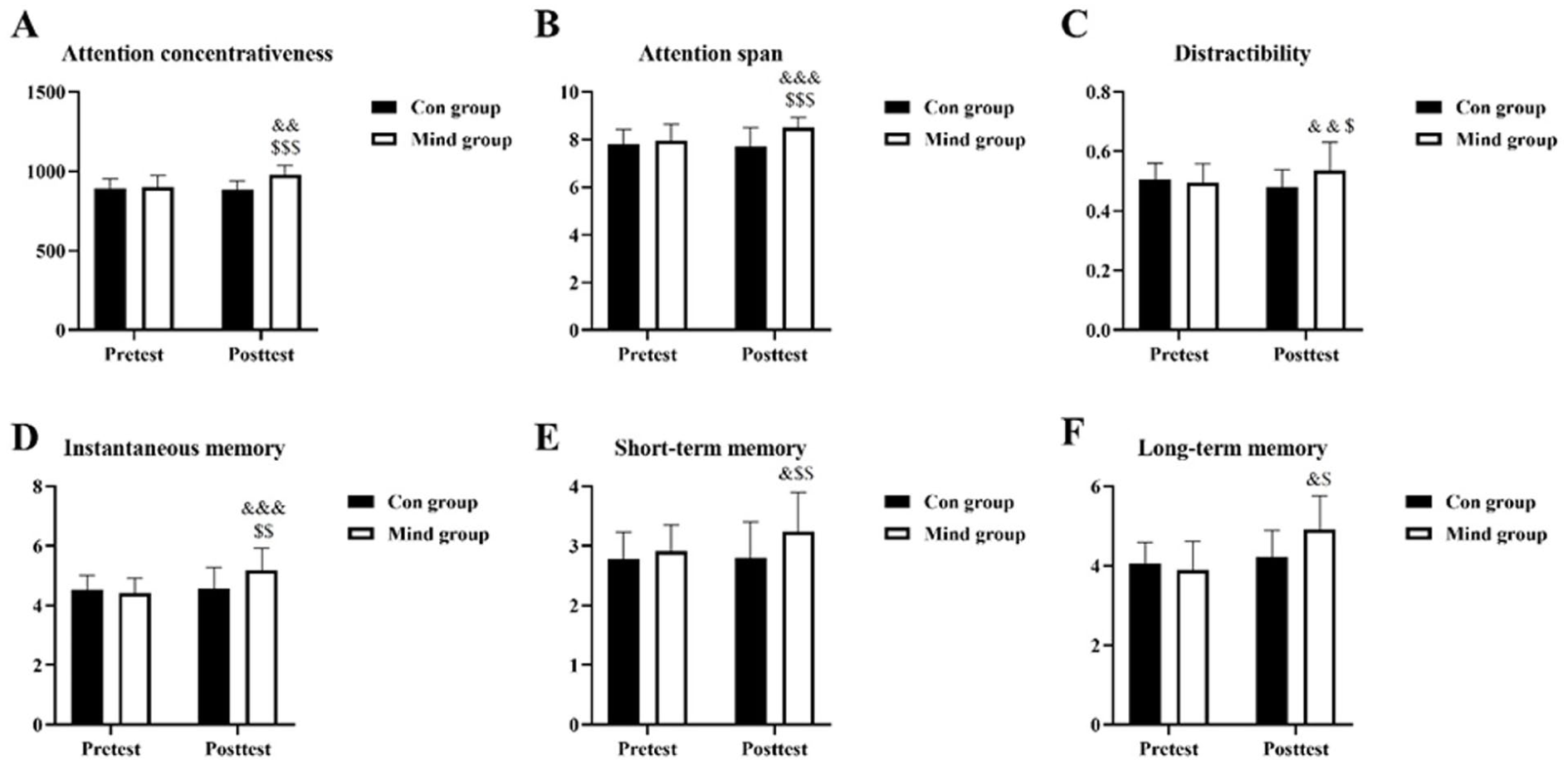
Cognition Results in Each Group after intervention.
Effects of Interventions on fNIRS Results
We conducted an analysis of variance to compare the HbO concentration in different mPFC regions between the two groups during the cognition test (Figure 4A). The effect of time was significant for the left mPFC, F(1, 69) = 37.23, p < .05, η2 = 0.29, 95% CI [0.15, 0.41], and the right mPFC, F(1, 69) = 13.90, p < .05, η2 = 0.13, 95% CI [0.04, 0.25], the TSI, F(1, 69) = 12.80, p < .05, η2 = 0.03, 95% CI [0.12, 0.30]. The main effect of intervention method was significant for the left mPFC, F(1, 69) = 13.90, p < .05, η2 = 0.13, 95% CI [0.04, 0.25], and the right mPFC, F(1, 69) = 11.10, p < .05, η2 = 0.11, 95% CI [0.02, 0.22], but not for the TSI, F(1, 69) = 10.40, p < .05, η2 = 0.17, 95% CI [0.02, 0.335]. The interaction was significant for the left mPFC, F(1, 69) = 15.07, p < .05, η2 = 0.14, 95% CI [0.04, 0.26], and the TSI, F(1, 69) = 6.53, p < .05, η2 = 0.07, 95% CI [0.03, 0.16], the right mPFC, F(1, 69) = 13.03, p < .05, η2 = 0.03, 95% CI [0.01, 0.10].

Average Concentration of (A) Left mPFC HbO; (B) Right mPFC HbO; (C) Tissue Saturation Index (%HbO2) on the Ranking Screen and the Target in the Cognition Test. $p < 0.05 represent between comparison on posttest. &p < 0.05 for pretest vs. posttest comparison.
There was no significant difference between the two groups in terms of [HbO] in the left and right mPFC regions at pretest stage (p > .05). However, compared with the Con group, the Mind group showed significantly greater mean HbO in the left mPFC and right mPFC as well as TSI, as shown in Figure 4. Statistical analysis of the main effect of time showed that the content of HbO2 in the left and right mPFC regions as well as TSI were significantly higher after mindfulness intervention than before training (p < .05); however, the HbO concentration and TSI had no significant differences in the Con group at pre-to-post stage (p > .05).
Effects of Interventions on Emotion Outcomes
Figure 5 presents mean emotion outcomes for the three dependent variables (STAI, BDI, and SHS) at pretest and posttest. The main effect of time was significant for STAI, F(1, 69) = 4.76, p < 0.05, η2 = 0.05, 95% CI [0.00, 0.14], and SHS, F(1, 69) = 5.58, p < 0.05, η2 = 0.06, 95% CI [0.01, 0.16], and BDI: F(1, 69) = 0.19, p < 0.05, η2 = 0.05, 95% CI [0.11, 0.32]. The main effect of intervention mode was significant for STAI, F(1, 69) = 5.58, p < 0.05, η2 = 0.06, 95% CI [0.02, 0.16], and BDI, F(1, 69) = 1.23, p < 0.05, η2 = 0.01, 95% CI [0.02, 0.33], and SHS, F(1, 69) = 17.28, p < 0.05, η2 = 0.16, 95% CI [0.05, 0.28]. The interaction effect between time and intervention mode was significant for STAI, F(1, 69) = 7.49, p < 0.05, η2 = 0.08, 95% CI [0.01, 0.19], and BDI, F(1, 69) = 4.98, p < 0.05, η2 = 0.05, 95% CI [0.01, 0.14], and SHS, F(1, 69) = 4.98, p < 0.05η2 = 0.06, 95% CI [0.02, 0.27].

Differences between the Con group and the Mind group in terms of
Post hoc Tukey test analyses (Figure 5) exhibited that there was no significant difference in emotion outcomes between the two groups at pretest stage (p > .05). Nevertheless, after mindfulness intervention, the emotion outcomes in the Mind group were significantly higher than those in the Con group (p < .05). Before and after training, the emotion outcomes had no significant differences in the Con group (p > .05), while the Mind group exhibited a significant difference in emotion outcomes scores before and after training (p < .05).
Effects of Interventions on Mental Fatigue
The mental fatigue results for each group are presented in Figure 6. The result revealed a significant main effect of intervention, F(1, 69) = 21.63, p < .05, η2 = 0.19, 95% CI [0.07, 0.32], a significant main effect of time, F(1, 69) = 15.80, p < .05, η2 = 0.15, 95% CI [0.04, 0.27], and a significant interaction between intervention and time, F(1, 69) = 33.41, p < .05, η2 = 0.27, 95% CI [0.13, 0.40].

Subjective report results of Mindfulness on athletic mental fatigue. $p < 0.05 representbetween comparison on posttest. &p < 0.05 for pretest vs. posttest comparison.
Post hoc test analyses (Figure 6) showed that there was no significant difference in RPE scores between the two groups before training (p > .05), but the RPE scores of the Mind group were significantly lower than those of the Con group (p < .05). The results by within-group comparison demonstrated that the RPE scores of Mind group was significantly higher after training than before training (p < .05). In the Con group, mental fatigue scores had no significant difference before and after training (p > .05).
Effects of Interventions on Salivary Cortisol Level
As shown in Figure 7, the result of salivary cortisol level revealed significant main effect of time, F(1, 69) = 3.55, p < .05, η2 < 0.01, 95% CI [0.01, 0.16], the main effect of intervention mode was significant, F(1, 69) = 4.15, p < .05, η2 = 0.04, 95% CI [0.01, 0.13], as was the interaction between time and intervention mode, F(1, 69) = 8.07, p < .05, η2 = 0.08, 95% CI [0.01, 0.18].
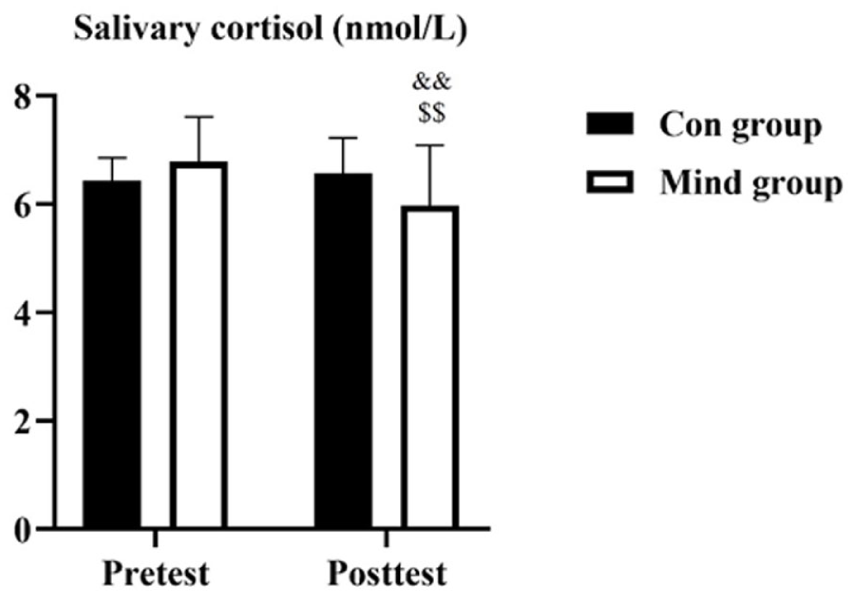
Graph Reporting Salivary Cortisol levels in nmol/L at Pretest and Posttest. $p < 0.05 represent between comparison on posttest. &p < 0.05 for pretest vs. posttest comparison.
The results of Figure 7 showed no significant difference in salivary cortisol level between the two groups before training (p > .05). After training, the salivary cortisol in the Mind group was significantly decreased than the Con group (p < .05). We also learn by within-group comparison that the scores after training were significantly decreased in the Mind group than those before training (p = .001). In the Con group, salivary cortisol had no significant difference before and after training (p > .05).
Discussion
This investigation examined the effects of a 16-week mindfulness intervention on cognitive functions and perceptual abilities in table tennis athletes. The results demonstrated that implementing mindfulness practices after training enhanced athletes’ cognitive performance and emotion state, particularly in domains of attention and memory. These improvements were supported by fNIRS data showing notable alterations in oxygenated hemoglobin (HbO) levels within targeted cerebral regions. Furthermore, compared with the control group, the Mind group exhibited reduced salivary cortisol levels, decreased mental fatigue, and enhanced emotional regulation.
Our results corroborate previous research that enhanced mindfulness status following a 16-week training regimen, while FFMQ proving useful for assessing effects of mindfulness intervention. Notably, comparative analysis revealed statistically significant improvements in FFMQ observing and awareness subscale score in the Mind group, and not the control group, indicating that mindfulness interventions did contribute to improvements in mindfulness over the control intervention. These findings are further reinforced by observed Group × Time interaction patterns within our data, primarily attributable to the increase of FFMQ scores in the Mind group (Perini et al., 2023).
As hypothesized, the current results are consistent with previous research (Zhong et al., 2025), which suggests that participants who received long-term mindfulness interventions exhibited better cognitive function when compared with control participants. Moore and Malinowski (2009) in the experimental research demonstrated a significant positive correlation between mindfulness levels and cognitive function. Tingaz (2020) further pointed out that, as a key element of mindfulness, non-judgment demonstrated partial mediation in shaping cognitive outcomes. The reason for the observed improvement in cognition parameters after mindfulness interventions is that it might be affected by cerebral oxygenation, which is related to the prefrontal cortex (Kojima et al., 2020). The fNIRS results showed that the intervention group exhibited higher oxyhemoglobin concentration after mindfulness interventions (Ding et al., 2025). It is known that mPFC is a key structure that facilitates sustained cognition by modulating activity in task-related and task-unrelated regions of the brain (Gao & Zhang, 2023). As stated above, the impacts of mindfulness on cognition are mainly reflected in increased cerebral oxygenation in the prefrontal lobe, especially in the left and right mPFC.
Further, our findings demonstrate that mindfulness practice can modulate health status, including anxiety, depression, subjective happiness, indicating that mindfulness meditation enables emotional status. This may be explained that mindfulness interventions can ameliorate emotional disorders (Ortner et al., 2007) and negative mood (Jha et al., 2010). Interestingly, mindfulness is a skill, and the emotional regulation mechanism it employs seems to depend on the degree of meditation practice. The study by Grecucci et al. revealed that mindfulness novices are more prone to using cognitive-based top-down emotional regulation, in contrast to advanced practitioners, who favor perceptual-driven bottom-up regulation mechanisms (Grecucci et al., 2015). Therefore, mindfulness meditation enables emotional regulation.
Our findings also indicate that participants undergoing 16-week mindfulness intervention exhibited therapeutic efficacy in facilitating recovery from mental fatigue and modulating salivary cortisol levels. This is in line with a previous experiment study concluded that a lower mental fatigue level and lower cortisol concentration were observed in the mindfulness interventions trial than in the control trial after the intervention (Ding et al., 2025). Consistent with established neuroscientific evidence indicating that non-judgmental and accepting awareness mechanisms exert beneficial effects on the brain, mindfulness’s potential to enhance non-judgmental and accepting awareness appears to interact with biological system underlying the development of mental fatigue (Cao et al., 2022). This may be explained that the causation of mental fatigue is influenced by the anterior cingulate cortex after competition (Darnai et al., 2023), while stronger anterior cingulate cortex activity accompanied by decreased mental fatigue after mindfulness interventions (Tang et al., 2020; Zsadanyi et al., 2021). Tang et al. (2009) revealed that even short-term mindfulness interventions can increase anterior cingulate cortex activity by enhancing attention and self-regulation via altering the interaction of the central (brain) and autonomic (body) systems (Tang et al., 2009). Thus, mindfulness interventions appear to be associated with improved regulation of the sympathetic nervous system and hypothalamic-pituitary-adrenal system, particularly in reduced mental fatigue and salivary cortisol.
This study has several limitations. First, the sample consisted of ordinary college athletes, who differ from elite athletes in sports proficiency, training intensity, and competitive experience; thus, the generalizability of the mindfulness effects to elite athletic populations remains uncertain. Second, the use of an eight-channel fNIRS system restricted our coverage to specific regions of interest, precluding whole-brain analysis. Future research would benefit from high-density arrays to comprehensively track hemodynamic changes across broader cortical networks. Third, the region-specific oxygenation changes observed here may be dependent on the particular cognitive demands of the mindfulness task employed. Investigating whether these patterns vary across different mindfulness-based activities represents an important direction for future work. Finally, limitations such as the small sample size for neuroimaging analyses, the potential for participant expectancy effects, and the restricted generalizability beyond collegiate table tennis players should also be acknowledged.
This study has several limitations. First, the use of an eight-channel fNIRS system limited cortical coverage to specific regions of interest, preventing whole-brain analysis. Future studies should employ high-density arrays to monitor hemodynamic changes across broader brain networks. Second, the observed region-specific changes in cerebral oxygenation may have been influenced by the cognitive demands of the mindfulness task used. Further research is needed to examine how these activation patterns vary across different mindfulness practices. Third, limitations such as the small neuroimaging sample size, potential expectancy effects, and restricted generalizability beyond collegiate table tennis players should also be explicitly considered. Finally, future studies should also include performance measures, given the focus on competition-related cognitive and emotional variables.
Conclusion
The 16-week mindfulness intervention may positively influence cognitive performance, with cerebral oxygenation fluctuations in prefrontal cortical regions partially mediating these functional alterations. Furthermore, this investigation demonstrated the advantageous impacts of mindfulness intervention on emotional regulation and mental fatigue mitigation as well as salivary cortisol level modulation in table tennis athletes.
Footnotes
Acknowledgements
We would like to thank all participants for their participation in this study.
Ethical Considerations
All participants gave written informed consent. This study received institutional ethical approval, which was conducted in accordance with the 1964 Helsinki Declaration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.