
Abstract
Observational studies have identified a significant co-morbidity between urinary tract infections (UTIs) and psychiatric disorders, yet the causal relationship remains uncertain. We conducted a bidirectional Mendelian randomization (MR) analysis to evaluate the causal relationship between psychiatric disorders (schizophrenia [SC], bipolar disorder [BD], major depressive disorder [MDD], autism spectrum disorder [ASD], attention-deficit/hyperactivity disorder [ADHD], obsessive-compulsive disorder [OCD], anorexia nervosa [AN]) and UTIs using data from the Psychiatric Genomics Consortium and UK Biobank. To account for potential confounding factors and investigate the independent effects of multiple psychiatric disorders, we further employed multivariable Mendelian randomization (MVMR). Inverse variance weighted analysis demonstrated that genetic susceptibilities of MDD and ASD increased UTI risk with odds ratios (ORs) of 1.31 (95% CI: 1.15–1.48, p < .001) and 1.08 (95% CI: 1.03–1.15, p = .004), respectively. UTIs were associated with a slight increase in the risk of MDD, evidenced by an OR of 1.061 (95% CI: 1.01–1.12, p = .019). Multivariate MR analysis revealed that MDD, after adjusting for type 2 diabetes mellitus and urinary stones, increased UTI risk (OR = 1.25, 95% CI: 1.08–1.45, p = .002), with smoking mediating 13.6% (p = .006) of MDD’s effect on UTIs. Our study establishes a causal relationship between psychiatric disorders and UTIs, identifying smoking as a mediator. These findings provide valuable guidance for clinicians to develop effective prevention and management strategies for patients with coexisting mental disorders and UTIs.
Introduction
Urinary tract infections (UTIs) are a pervasive problem that affects individuals of all ages, from infants to the elderly (Curns et al., 2005). These infections can range from mild to severe and profoundly impact an individual’s health and quality of life. The frequency of UTIs and their recurrent nature make them one of the most common bacterial pathogenic infections, leading to a significant number of hospitalizations each year. In the elderly population, UTIs are a leading cause of hospitalization for infections. The vulnerability of this demographic to UTIs highlights the importance of preventive measures and effective treatment options. In addition, UTIs are a major concern for those who have undergone a renal transplant, as more than 30% of all infectious complications in this population are caused by UTIs (Alangaden et al., 2006). The global emergence of antibiotic resistance complicates diagnosing and treating UTIs effectively (Masajtis-Zagajewska & Nowicki, 2017).
Psychiatric Disorders pose a significant threat to global public health, with millions of individuals affected worldwide. These disorders, led by major depressive disorder (MDD), are a primary cause of nonfatal burden with a far-reaching impact on individuals and society (“Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016,” 2017). Despite extensive research on psychiatric disorders, the underlying causes and mechanisms remain largely unknown. Chronic and recurrent stress is widely considered a significant contributing factor to developing psychiatric disorders (Campbell et al., 2014). Its impact on mental health is multifaceted, manifesting through several pathways, such as disturbances in neurotransmitter balance, activation of abnormal immune system responses, and exacerbation of psychological stress (Cohen et al., 2007). Numerous clinical studies have revealed a significant co-occurrence of UTIs and psychiatric disorders (Fraguas et al., 2019; Tsugawa et al., 2019; Zhang et al., 2010).
Some studies have suggested that UTIs are associated with the pathophysiology of psychiatric relapse and may increase the risk of premature death (Graham et al., 2014). In previous studies, researchers found that more than one in four acutely psychotic patients with schizophrenia had UTIs at the time of hospitalization (Graham et al., 2014; Laney et al., 2015; Miller, Graham, et al., 2013). After controlling for potential confounders, adult patients with nonemotional psychosis were almost 11 times more likely to have UTIs than controls. In contrast, adult patients with MDD with psychotic features were almost nine times more likely to have UTIs than controls (Graham et al., 2014). Similarly, UTIs are higher in the child and adolescent population of patients with psychiatric disorders (Carson et al., 2017). With the growing body of evidence highlighting the relationship between UTIs and psychiatric disorders, further research must be conducted to understand this complex relationship better and develop appropriate intervention strategies.
Despite the numerous studies exploring the relationship between UTIs and psychiatric disorders, the causal relationship remains uncertain. This is primarily due to the limitations of observational studies, which often suffer from confounding variables, limited follow-up time, and small sample sizes. These factors can all lead to significant bias in the results and make it difficult to confirm the causal relationship between UTIs exposure and psychiatric disorders. This study utilized a cutting-edge research method called Mendelian randomization (MR) to address this issue. This approach leverages genetic variants from genome-wide association studies as instrumental variables (IVs) to make causal inferences about the outcome (Lawlor et al., 2008). The bidirectional MR study conducted in this study aimed to clarify the relationship between UTIs and psychiatric disorders by eliminating the influence of confounding factors and providing a more robust estimation of causality. By using MR, the study aimed to shed light on the complex interplay between UTIs and psychiatric disorders and clarify this relationship’s direction.
Materials and Methods
Study Design
This study utilized published genome-wide association study (GWAS) pooled data for two-sample and multivariate MR (MVMR) analyses to assess the causal relationship between psychiatric disorders and UTIs (Figure 1).

The Whole Workflow of MR Analysis.
Our MR analysis satisfies all three assumptions: (i) association assumption: single nucleotide polymorphisms (SNPs) are highly associated with predicted exposures, (ii) independence assumption: SNPs are independent of known potential confounders, and (iii) exclusivity assumption: SNPs influence the outcome through exposure factors and are not directly related to the outcome.
To ensure that the results of this study were robust, the selection of IVs was made with great care, taking into account the criteria outlined in the MR literature. Only genetic variants that met the stringent criteria of a GWAS-correlated P-value of <5 × 10−8 or <5 × 10−6 and a linkage disequilibrium (LD) r2 of < 0.001, as well as being less than 1 MB from the index variant were considered for use as IVs (Chen et al., 2024; Davies et al., 2018; Kwok & Schooling, 2021). The threshold for GWAS-correlated P-values was initially set at 5 × 10−8. However, if an insufficient number of SNPs were available for the final MR analysis, this threshold was relaxed to 5 × 10−6. For assessing IVs strength, the following formula was used to calculate F-statistics: F=β2/SE2 (Bowden et al., 2019). The SNPs with F <10 were removed. Furthermore, we integrated the MR Steiger test into our analysis to enhance the credibility of our results. The MR Steiger directionality test determines the validity of the chosen SNPs as IVs (Hemani et al., 2017). A “TRUE” MR Steiger result implies causality in the anticipated direction.
In this study, we employed bidirectional MR analysis, using genetic variants associated with psychiatric disorders and UTIs as IVs. This approach leveraged the genetic instruments to statistically test for causal effects in both directions, thus assessing not only the influence of psychiatric disorders on the incidence of UTIs but also whether UTIs might contribute to the onset of psychiatric disorders. This bidirectional assessment provided a comprehensive evaluation of the potential causal relationships between these conditions.
A series of sensitivity analyses were conducted to validate our results. Five MR methods—
Data Sources
Databases generated by GWAS were searched, and eligible datasets were extracted. To reduce bias caused by race-related confounding factors, the genetic background of the study population was restricted to European ancestry.
Genetic associations of psychiatric disorders from the Psychiatric Genomics Consortium (PGC) (“Biological insights from 108 schizophrenia-associated genetic loci,” 2014; Duncan et al., 2017; Grove et al., 2019; Howard et al., 2019; “Revealing the complex genetic architecture of obsessive-compulsive disorder using meta-analysis,” 2018; Stahl et al., 2019): Schizophrenia (SC) data (n = 82,315); Bipolar Disorder (BD) (n = 51,710); MDD (n = 503,199); Autism Spectrum Disorder (ASD) (n = 46,351); Attention-Deficit/Hyperactivity Disorder (ADHD) (n = 55,374); Obsessive-Compulsive Disorder (OCD) (n = 33,925); Anorexia Nervosa (AN) (n = 14,477). Summary data of Urinary Tract Infections (UTIs) from the UK Biobank. This study included 486,214 European males (21,958 cases and 464,256 controls) (Supplementary Table 1).
Statistical Analysis
Among the causality testing methods used—including IVW, weighted median, weighted mode, contamination mixture method, and RAPS—IVW is recognized as the primary approach. It provides efficient statistical efficacy by assuming that all variables are valid, disregarding the presence of intercept terms in the analysis, and using the inverse of the variance of the outcomes as fitting weights (Burgess et al., 2013). The weighted median method adjusts for the effect of invalid IVs and yields a robust assessment, even in the presence of 50% invalid IVs (Bowden et al., 2016). Compared to the IVW method, the weighted mode method offers greater robustness, delivering reliable estimates under more lenient assumptions about instrumental variables (Hartwig et al., 2017). The contamination mixture method performs MR robustly and efficiently in the presence of invalid IVs (Burgess et al., 2020). And RAPS accounts for systematic and idiosyncratic pleiotropy and can provide a robust inference for MR analysis with many weak instruments (Zhao et al., 2020).
For the sensitivity analysis, the MR-Egger intercept test was used to assess horizontal pleiotropy. Based on the assumption that instrument strength is independent of direct effects (InSIDE), the intercept term can be used to measure pleiotropy in the MR-Egger regression. Horizontal pleiotropy does not exist when the intercept term is zero (Bowden et al., 2015). Cochran’s Q test was used to identify heterogeneity (Cohen et al., 2015), and MR-PRESSO was used to evaluate the pleiotropy (Verbanck et al., 2018). We also employed the CAUSE method, which handles both correlated and uncorrelated horizontal pleiotropic effects (Morrison et al., 2020). This approach reduces the number of false positives that are typically caused by correlated horizontal pleiotropy, compared to other methods.
In order to reduce the false positive rate, we applied the Bonferroni correction method for multiple testing across all five MR methods used to explore causal effects. The threshold for statistical significance was defined as a p-value <7.14 × 10−3 (p = .05 / [seven exposures × one outcome]) adjusted for seven exposures and one outcome using the Bonferroni method. A p-value ranging from 7.14 × 10−3 to 5 × 10−2 was deemed to indicate suggestive significance.
In addition, we employed MVMR analysis, which is an extension of univariable MR that uses multiple genetic variants associated with multiple exposures to estimate the direct causal effect of each risk factor on an outcome (Burgess & Thompson, 2015). In the MVMR analysis, instrumental variables associated with at least one exposure were included, and the multivariate IVW approach was used to estimate causality. We also aimed to assess a potential mediator between psychiatric disorders and UTIs. We decomposed the total effect of the psychiatric disorder on UTIs into direct and indirect effects [36], with the latter mediated by the potential factor. The product of coefficients method was used to estimate the indirect effect (β1 × β2), with β1 representing the effect of the psychiatric disorder on the mediator, and β2 representing the effect of the mediator on UTIs. The direct effect (β3) was calculated after adjusting for the mediator. The total effect was the sum of the direct and indirect effects, and the proportion mediated was calculated as (β1 × β2 / [β3 + β1 × β2]).
All of the statistical analyses were accomplished based on R (version 4.3.0) and the R packages of “TwoSampleMR” and “Mendelian Randomization.” The study results are reported according to the standards of Strengthening the Reporting of Observational Studies in Epidemiology-Mendelian Randomization (STROBE-MR) (Skrivankova et al., 2021).
Results
Instrument and Correlations of Genetics
Supplementary Table 1 presents the exposure and outcome characteristics of SNPs. Supplementary Tables 2–3 provide summary statistics of SNPs as IVs.
Univariate MR Analysis
Causal Effect of Psychiatric Disorders on UTIs
For the forward analyses, psychiatric disorders were used as the exposure factor and UTIs was used as the outcome variable (Figure 2). According to primary IVW estimates, genetically predicted MDD (odds ratio [OR] = 1.31, 95 % confidence interval [CI]: 1.15–1.48, p = 2.66 × 10−5) and ASD (OR = 1.08, 95% CI: 1.03–1.15, p = 3.97 × 10−3) was positively associated with the risk of UTIs. In MR analyses exploring the relationship between MDD and UTIs, significant associations were observed in several methods. The weighted median and contamination mixture methods, along with the RAPS, all reported notable positive associations. Specifically, the contamination mixture method revealed a particularly strong linkage (OR = 1.48, 95% CI: 1.23–1.78, p = 8.82 × 10−6) and RAPS also supported a robust positive association (OR = 1.36, 95% CI: 1.20–1.55, p = 1.10 × 10−6), underscoring consistency even under conditions of robust error variance. Conversely, ASD did not exhibit significant associations with UTIs in any method except for the IVW analysis. Importantly, across all other MR methods, the direction was consistent with the IVW findings for both MDD and ASD. Furthermore, the average F-statistic exceeded 10, indicating that weak instrumental variables were absent (Supplementary Table 2). In addition, according to the results of the MR analysis, there was no significant association between the risk of UTIs and various psychiatric disorders including SC, BD, ADHD, OCD, and AN, with all p-values greater than 7.14 × 10−3.

Effect of Psychiatric Disorders on Odds of Urinary Tract Infections in the Univariable Model.
Causal Effects of UTIs on Psychiatric Disorders
The potential causal effect of UTIs on psychiatric disorders was investigated by reverse MR analysis (Figure 3). However, according to the results from the IVW method, UTIs did not significantly increase the risk of any psychiatric disorders under the adjusted P-value threshold, although the effect of UTIs on MDD was nominally significant (OR = 1.06, 95% CI: 1.01–1.12, p = 1.91 × 10−2 < 0.05). In MR analyses exploring the relationship between UTIs and MDD, the RAPS demonstrated statistically significant results (OR = 1.07, 95% CI: 1.02–1.12, p = 6.88 × 10−3), indicating a possible positive causal relationship where UTIs may increase the risk of MDD. And the average value of F-statistic is >10 ( Supplementary Table 3 ). Although the other methods suggested a positive association, they did not achieve statistical significance under the adjusted threshold.

Effect of Urinary Tract Infections on Odds of Psychiatric Disorders in the Univariable Model.
Sensitivity Analysis
All MR Steiger tests associated with the positive results mentioned above returned TRUE, confirming that the IVs used are valid. The detailed results of these analyses are presented in Supplementary Table 4 . To further validate the positive findings reported above, we performed sensitivity analyses using different MR methodologies. The Cochran Q test for IVW revealed no heterogeneity between MDD and UTI in either direction of the MR analysis, with p > .05 ( Supplementary Table 5 ). In addition, both directions demonstrated high stability and lacked significant pleiotropic effects, as confirmed by the MR-Egger intercept test results ( Supplementary Table 6 ). The MR-PRESSO results for the associations between MDD and UTIs, as well as ASD and UTIs, were largely consistent with the findings from the IVW analysis ( Supplementary Table 7 ). Funnel plots from the MR analysis were used to assess heterogeneity visually (Figure 4). The leave-one-out sensitivity analysis results showed that the IVW analysis of the remaining SNPs was similar to those of the analysis, including all SNPs in turn, and no SNPs were found to have a significant effect on the causal association estimates (Figure 5).
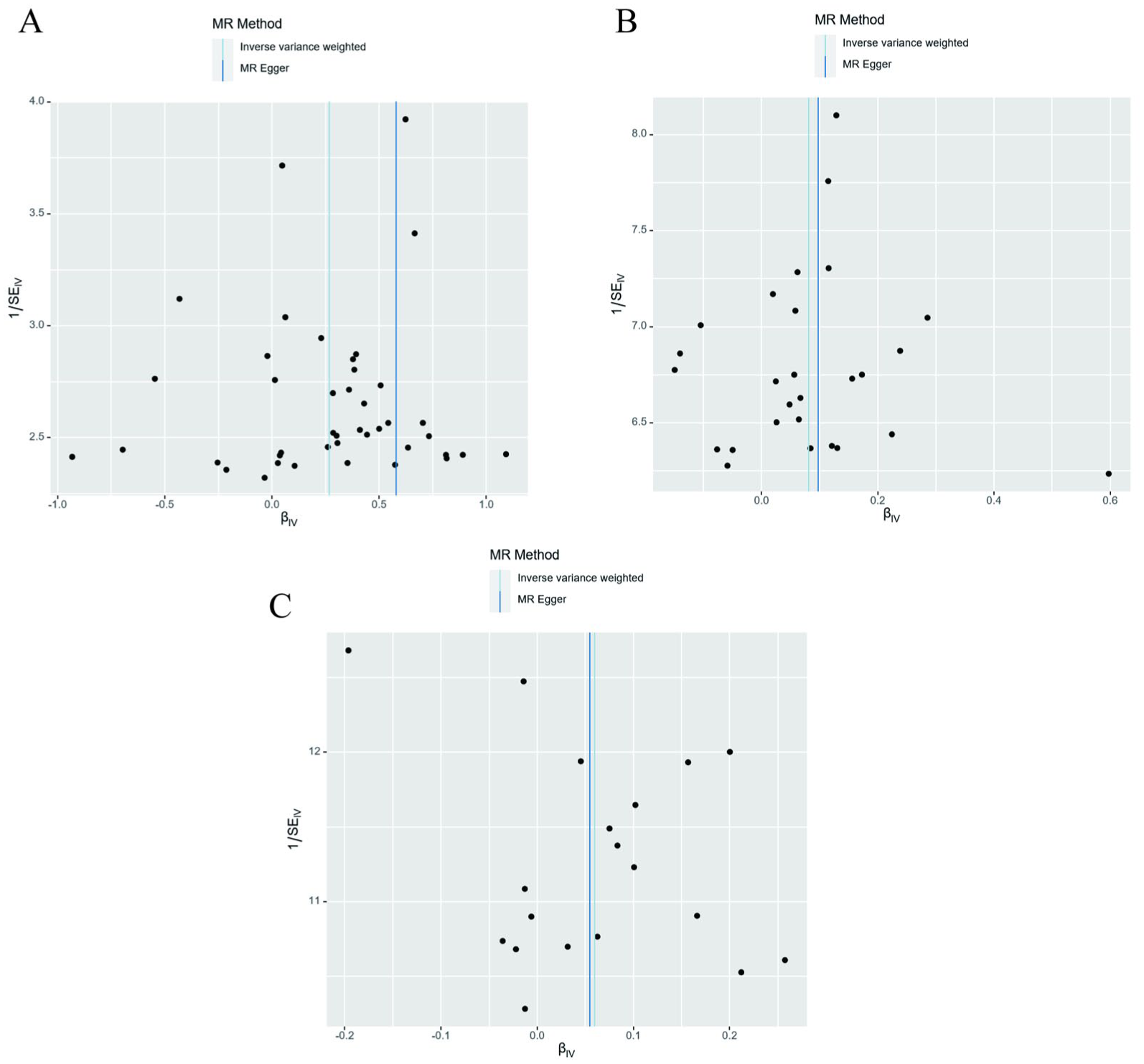
Funnel Plots for Sensitivity Analysis of Psychiatric Disorders and Urinary Tract Infections Associations. (A) Funnel Plot of the Causal Effect of Major Depressive Disorder on Urinary Tract Infections. (B) Funnel Plot of the Causal Effect of Autism Spectrum Disorder on Urinary Tract Infections. (C) Funnel Plot of the Causal Effect of Urinary Tract Infections on Major Depressive Disorder.

Leave-One-Out Plots for Sensitivity Analysis of Psychiatric Disorders and Urinary Tract Infections Associations. (A) Leave-One-Out Plots for the Causal Association Between Major Depressive Disorder on Urinary Tract Infections. (B) Leave-One-Out Plots for the Causal Association Between Autism Spectrum Disorder on Urinary Tract Infections. (C) Leave-One-Out Plots for the Causal Association Between Urinary Tract Infections on Major Depressive Disorders.
In the forward-direction CAUSE analyses investigating the impact of various psychiatric disorders on UTIs, MDD demonstrated a positive association (p = 2.19 × 10−2) ( Supplementary Table 8 ). This significant result was obtained specifically under the CAUSE method causal model. Conversely, the reverse analysis from UTIs to MDD did not yield any positive results. These findings highlight a potential unique causal link between MDD and the risk of UTIs.
Multivariate MR and Mediation Analysis
Given the significant association identified in our previous analyses, and considering that diabetes mellitus type 2 (T2DM) and Urolithiasis are common confounders of UTIs (Hsiao et al., 2019; Luk et al., 2021), we included MDD and ASD along with T2DM and Urolithiasis in MVMR analyses. This approach allowed us to further explore the relationship between psychiatric disorders and UTIs. The MVMR results confirmed that MDD remains significantly associated with the risk of developing UTIs, even after adjusting for T2DM and Urolithiasis (OR = 1.25, 95% CI: 1.08–1.45, p = 2.74 × 10−3) (Figure 6, Supplementary Table 9 ).

Effect of Each Exposure on Odds of Urinary Tract Infections in the Multivariable Model.
The total effect of MDD on UTIs risk is decomposed into (i) the direct effect of MDD on UTIs and (ii) the indirect effect of MDD through mediators individually. The indirect effect of intermediation was derived using the product method (Carter et al., 2021). We investigated the relationships between MDD and smoking, as well as smoking and UTIs, using the IVW method ( Supplementary Table 10 ). study showed a causal association between MDD and smoking (OR = 1.22, 95% CI: 1.14–1.30, p = 1.44 × 10−9). There was also a causal association between smoking and UTIs (OR = 1.20, 95% CI: 1.07–1.35, p = 2.25 × 10−3). The proportion of the effect of smoking on MDD-mediated outcomes was further calculated using mediation analysis. The results showed that the effect of MDD on UTIs was partially mediated by smoking, with the proportion of mediation ranging from 13.6% (95% CI: 0.04–0.24, p = 6.39 × 10−3; Figure 7).

Illustration of the Total Effect and Direct Effect of Psychiatric Disorders on Urinary Tract Infections.
Discussion
Psychiatric disorders represent a significant public health challenge, affecting more than one billion people worldwide (Rehm & Shield, 2019). Given this challenge, several observational epidemiological studies have explored the link between UTIs and psychiatric disorders (Hufschmidt et al., 2010; Ketcham & Miller, 2022). However, due to limitations inherent in observational study designs, the reliability of these findings is often questioned. The present study used the MR analysis approach to overcome these limitations and evaluate the causal relationship between UTIs and seven psychiatric disorders. The results of this study offer novel insights into the complex interplay between UTIs and psychiatric disorders, specifically in the context of MDD. Using the MR analysis, the study demonstrates a causal relationship between MDD and UTIs, providing direct evidence of a link between these conditions. Further, the results suggest that smoking may mediate this causal relationship, implying that smoking cessation or reduction may reduce the risk of MDD and UTIs.
To our knowledge, this is the first systematic study to investigate the causal relationship between psychiatric disorders and UTIs by MR analysis and the mediating role of smoking in this relationship. Previous observational studies have suggested an association between psychiatric disorders and UTIs. In a Danish registry study, the risk of psychiatric disorders was increased by more than 50% in the presence of genitourinary infections compared with the absence of such infections (hazard ratio[HR]: 2.30, 95% CI: 1.91–2.76, p < .001) (Hjorthøj et al., 2020). A study based in Taiwan, China, found an association between postpartum depression and antenatal UTIs, with an adjusted OR of 1.27 (95% CI: 1.07–1.65). Furthermore, compared to women with lower UTIs, those with upper UTIs had a higher risk of PPD, with an adjusted OR of 2.97 (95% CI: 1.31–6.77), while lower UTIs had an adjusted OR of 1.21 (95% CI: 1.02–1.58). This suggests that health care professionals should pay more attention to the mental health of patients with such conditions (Lee et al., 2017). At the same time, depression is associated with a chronic low-grade inflammatory response, cell-mediated immunity activation, and the compensatory anti-inflammatory reflex system. This chronic inflammatory activation may have a beneficial effect on UTIs.
In assessing the association between psychiatric disorders and UTIs, T2DM and urinary stones were confounding factors. With MVMR, we corrected the bias due to T2DM with urinary stones and found that MDD still leads to an increased risk of the prevalence of UTIs. The mediator analysis revealed that smoking played a mediating role in the increased risk of UTIs caused by MDD, and the proportion of this role was 13.6%, indicating that smoking is important in participating in the effect of MDD on UTIs, which deserves further in-depth study.
The mechanisms underlying the association of psychiatric disorders with UTIs remain unknown. One view is that psychiatric disorders induce physiological changes in the urinary system and lead to various behavioral alterations in patients, such as impaired personal hygiene or impulsive conduct (Eriksson et al., 2010), all of which elevate the susceptibility to UTIs. In addition, adverse effects brought on by antipsychotic medications, such as urinary retention, are also recognized as significant risk factors for UTIs (Miller, Graham, et al., 2013). An alternative perspective posits that in cases of chronic inflammation resulting from UTIs, a persistent release of cytokines may directly impact dopaminergic neurotransmission. Moreover, this peripheral inflammation may cause decreased proliferation of BrdU-positive neural stem cells in the hippocampal dentate gyrus, potentially leading to psychiatric disorders and depression (Darwish et al., 2022; Miller, Bodenheimer, et al., 2013).
Neither observational nor MR studies can make precise inferences about the mechanisms. In this study, we found the importance of smoking as a mediating factor in the causal relationship between MDD and UTIs by mediation MR analysis. Smoking, recognized as a significant global public health concern, has attracted substantial attention (Goodchild et al., 2018). Among individuals with mental disorders, it is strongly associated with increased levels of anxiety and depression (Jamal et al., 2012). In previous research, a diminished capacity for positive affect has been linked to attenuation of the mesolimbic system, which is responsible for reward processing in the brain. Notably, the self-administration of nicotine, a dopamine agonist, has been found to enhance the ability to experience pleasurable mental states in smokers diagnosed with depression (Cook et al., 2007; Rubin et al., 2020). Individuals with anhedonia/depressive tendencies may enhance positive emotional states by engaging in compensatory behaviors like smoking. Smoking is thought to have adverse effects on almost all organs (National Center for Chronic Disease et al., 2014) and is considered an independent risk factor for UTIs (Wallin et al., 2020). Previous studies have shown that maternal smoking during pregnancy increases the risk of UTIs. In contrast, smokers have a greater need for antibiotic treatment of UTIs during pregnancy and more frequent self-reported genitourinary symptoms (Gilstrap & Ramin, 2001; Wallin et al., 2020). In addition, the duration of smoking significantly affects the appearance of UTIs, as those who continue to smoke throughout pregnancy are more likely to develop UTIs compared to those who quit smoking in the first trimester (Wallin et al., 2023). The causal relationship between smoking and UTIs was also verified in the present study, but the specific mechanism by which it causes UTIs is poorly understood. From a clinical perspective, this result highlights smoking cessation as a potential intervention to help reduce UTI risk in patients with MDD, alongside other preventive strategies. In addition to behavioral factors like smoking, there may be microbiome and immunological pathways underlying the relationship between psychiatric disorders and UTIs. Chronic mental stress can disrupt neuroimmune regulatory mechanisms, alter the gut microbiota composition, and increase systemic inflammatory responses (Petakh et al., 2024). Such perturbations may weaken host defense in the urinary tract, thereby elevating the risk of infection. Future research would benefit from longitudinal designs and integrative multi-omics approaches to unravel these complex interactions.
Although MR is a valid method for causal inference using pooled GWAS data, caution should be exercised when interpreting the results of this study due to several limitations. First, the primary databases employed are sourced from the PGC, which stands as the largest and most reputable genetic repository in the field of psychiatry. Notwithstanding, there exists a potential for sample overlap, which could introduce bias into the results. Nevertheless, in this investigation, the exposure, mediators, and outcomes were derived from distinct databases, with no observed evidence of sample overlap or horizontal pleiotropy. Second, to reduce ethnic bias, the GWAS data in this study were exclusively obtained from individuals of European descent. This selection criterion, while minimizing bias, may constrain the extrapolation of our findings to the global population (Wang et al., 2022).
Conclusions
The present Mendelian randomization analysis indicates a positive causal relationship between MDD and UTIs, with a potential for a reverse causal relationship as well. As such, preventive measures aimed at reducing the incidence of MDD could prove beneficial in mitigating the risk of UTIs, while preventing UTIs may also have added health benefits by lowering the incidence of MDD. Our findings suggest that smoking may function as a crucial mediator of UTIs linked to MDD, indicating that reducing or ceasing smoking habits may lower the risk of UTIs in individuals with MDD. By taking a comprehensive approach to patient care, health care providers can help improve these patients’ overall health and well-being, leading to better outcomes and a higher quality of life.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883251400693 – Supplemental material for Mendelian Randomization Analyses Support Causal Relationships Between Psychiatric Disorders and Risk of Urinary Tract Infections
Supplemental material, sj-docx-1-jmh-10.1177_15579883251400693 for Mendelian Randomization Analyses Support Causal Relationships Between Psychiatric Disorders and Risk of Urinary Tract Infections by Minghui Ke, Haolang Wen, Binghao Bao, Yuan Liu, Lei Zhang, Chenglong Zheng and Baoxing Liu in American Journal of Men's Health
Footnotes
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Authors’ Contributions
Ming-hui Ke: Analyzed the data and revised the report. Haolang Wen: Wrote and revised the report. Bing-hao Bao: Conceived the study. Yuan Liu and Lei Zhang: Assisted in the study’s implementation. Cheng-long Zheng and Bao-xing Liu: Modified the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.