
Abstract
Disparities in prostate cancer incidence and mortality among Black men exist in Suffolk County, New York, indicating a need to provide effective educational interventions about prostate cancer screening for this population. We conducted a mixed-methods study exploring Black men’s knowledge, attitudes, and beliefs about prostate cancer, and how they access health information. Three semi-structured virtual focus groups were conducted by Black male physicians with 18 Black men aged 40 years and over living in Suffolk County, New York. All were recorded, transcribed, and coded to identify key themes. Participants also completed surveys assessing prostate cancer knowledge and information preferences. Quantitative and qualitative results were analyzed using SPSS and NVivo software. Recruitment required extensive outreach. Even among relatively well-educated participants, more prostate cancer knowledge was needed, and 11% had not obtained screening because they were not aware they needed it. Family history prompted prostate cancer concerns, and fear of dying from prostate cancer motivated screening. Health information from reputable website sources was preferred, with social media drawing attention to educational opportunities and education portraying individuals to whom Black men could relate. Participants expressed desire for further engagement between their community, the academic hospital, and physicians. Our results indicated that despite being relatively knowledgeable about prostate cancer, Black men desire stronger ties and trust between their community and health care providers to facilitate screening. These data may assist health care professionals in designing practical educational tools and tailored programs about prostate cancer screening among Black men who are at increased risk of disease.
Keywords
Prostate cancer is the most diagnosed cancer in men in the United States (National Cancer Institute, 2023). When compared with other ethnic groups, Black men are disproportionately affected, with prostate cancer being the leading cancer diagnosed in Black males in New York State. In comparison with White and Hispanic men, Black men have the highest incidence of prostate cancer (Jones et al., 2009). Black men are more likely to be diagnosed with late-stage cancer and twice as likely to die from prostate cancer compared with White men (Roberts et al., 2018; The National Cancer Institute, 2019). These inequities are evident in Suffolk County, New York, as well, with age-adjusted prostate cancer incidence of 230.5 per 100,000 (2016–2020) in non-Hispanic Black persons, and 135.9 in non-Hispanic White persons. Mortality rates also demonstrate a disparity in Suffolk County, with age-adjusted prostate cancer mortality of 36.3 per 100,000 (2016–2020) in non-Hispanic Black persons and 15.9 in non-Hispanic White persons (National Cancer Institute & Centers for Disease Control and Prevention [CDC], 2023).
Studies have shown a need for educational interventions to encourage Black men to participate in prostate cancer screening and engage in informed decision-making with health care professionals (Ogunsanya et al., 2017; Oliver et al., 2018; Woods et al., 2004). These studies revealed low knowledge scores for overall prostate cancer knowledge, risk factors, and prostate cancer screening. A review of a national survey revealed that respondents who were Black, younger, and had lower levels of education were less likely to receive information from their doctor required for shared decision-making (SDM) about prostate-specific antigen (PSA) testing (Leyva et al., 2016). These findings suggest a need for additional research to understand the noted disparities among these groups.
A systematic review of interventions to improve decision-making and reduce racial and ethnic disparities in the management of prostate cancer concluded that educational programs were the most effective intervention for improving knowledge among screening-eligible minority men (Sajid et al., 2012). Muvuka et al. (2020) explored health literacy barriers and strategies among African Americans and concluded that research on effective approaches for improving health literacy in populations that experience health disparities should be prioritized due to gaps in the literature, and that the health information delivery preferences of African Americans in diverse settings specifically warrants further exploration. Focusing on studying community-based health literacy interventions was emphasized (Muvuka et al., 2020).
Interventions designed to address the complex causes of these disparities must be informed by the opinions and perspectives of the target population to be effective and beneficial. The current study used a “person-based approach” to assess and enhance the acceptability and feasibility of an intervention during the early stages of development and evaluation (Yardley et al., 2015) to conduct a community needs assessment to (a) learn where and how Black men in Suffolk County get their health information regarding prostate cancer; (b) assess their knowledge, attitudes, and beliefs about prostate cancer; and (c) understand how those beliefs and attitudes impact their behaviors regarding prostate cancer screening to better learn how to effectively educate and serve them.
Method
Semi-structured focus groups were conducted virtually in Spring and Summer 2022. Three focus groups were held with seven, six, and five individuals, respectively, all from Suffolk County. The inclusion criteria for participation were being a person with a prostate, being above 40 years of age, not having had or currently having prostate cancer, identifying as Black, African American, or Afro-Caribbean, residing in Suffolk County, being fluent in English, and being able to join the meeting via Zoom (Zoom Video Communications, Inc., 2022). Prior to the study, recruitment scripts and a flyer, consents, demographic questionnaires, and a focus group discussion guide were developed de novo by the research team. A knowledge assessment, which was previously used in a similar group of participants but not validated, was adapted from Carter et al. (2010) to gauge the participants’ level of knowledge about prostate cancer. A variety of recruitment strategies were used including referrals from community group leaders, recruitment tables set up at community events, flyers, social media promotion, and word of mouth. Our health education specialists partnered with various community group leaders to introduce the initiative to the community and encouraged those who were interested in participating to call to sign up. Overall, the study team outreached to 109 community-based organizations (Caravella et al., 2024). Three community “champions” were enlisted to assist with recruitment. Screening for eligibility was done over the phone or in person. A telephone script was used to sign people up for the focus groups when calls were received from potential participants. For in-person recruitment, interested subjects meeting inclusion criteria were asked to sign up. Screening questions were asked to determine eligibility but were not recorded or used as part of the data. Telephone calls and email correspondence were used to contact the participants regarding the focus group or interview logistics, but otherwise no private information was collected. Only those who met the inclusion criteria participated in the focus groups.
Participants were informed that the goal of the focus group was to hear their thoughts and opinions about issues such as health information and cancer screening, with the intent of using the information to create an educational program about prostate cancer and prostate cancer screening. Prior to the focus group meetings, which were held remotely via Zoom, participants completed a survey designed to collect demographic information, background knowledge, and preferred sources of health information. In addition to the open-ended questions that were posed during the focus group discussion, online polls were launched that were used to collect closed-ended responses.
Quantitative survey responses were summarized with descriptive statistics using SPSS Version 26 (IBM Corp, 2019). The survey was completed before the focus groups took place. It consisted of questions regarding prostate cancer screening, experience with health care appointments, trusting providers, medical advice seeking, and prostate cancer knowledge. The focus group interviews were automatically transcribed, reviewed for accuracy, and subjected to qualitative thematic analyses based upon a set of a priori and emergent codes determined by the focus group discussion topics, using NVivo (Release 1.0) software (QSR International Pty Ltd, 2020). The semi-structured focus group guide was developed based on previous literature and our patient advocacy, clinical, and qualitative expertise. The research team met frequently to discuss coding and theme development, contributing to the reliability and validity of the data analysis. A codebook was developed based on inductive and deductive code commonalities observed in the transcripts. Deductive codes were based on topics included in the guide. Inductive codes were developed from participant responses. Codes were analyzed for frequency and developed into major themes.
In addition to the open-ended questions that were posed during the focus group discussion, online polls were launched that were used to collect closed-ended responses and the duration of the focus group spanned an hour in length. The polls were answered within the focus group meetings and were based on how participants obtain health care information and their format preferences. During the focus group session, participants were educated on the correct answers to the knowledge assessment questions. At the conclusion of the session, participants were thanked for their time, provided with resources about prostate cancer and counseling, and were compensated with a one-time $20 gift card for their participation.
This work did not include informed consent, as it was a focus group study that was deemed exempt by the Institution’s Committee on Research Involving Human Subjects (Institutional Review Board).
Results
Recruitment
Study team staff members outreached to 109 community-based organizations and 18 participants agreed to participate and attended the focus group sessions. This included emails, phone calls, and street outreach. During the outreach effort, three “community champions” emerged and were the most effective resource in facilitating recruitment. The “cold” outreach was not as effective, but rather the referrals made by community champions led to greater turnout.
Demographics
The demographic characteristics of the 18 focus group participants are listed in Table 1. All had completed high school or had higher education. Thirteen (72%) were married or in a committed relationship. While all participants were Black men, 5.6% were Hispanic, Latino, or Spanish.
Demographic Characteristics of Study Participants—Survey Results.
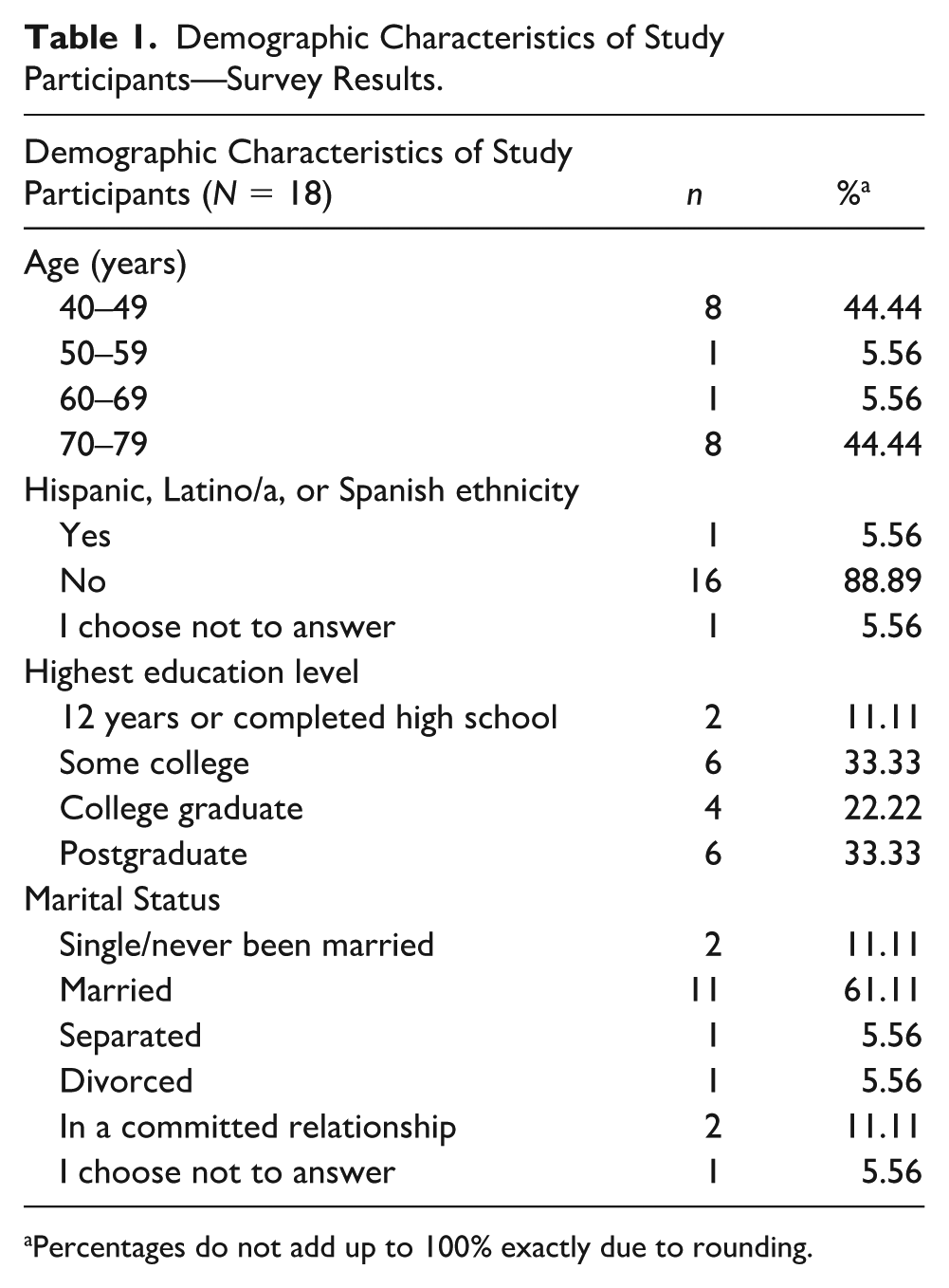
Percentages do not add up to 100% exactly due to rounding.
Quantitative Results
Prostate Cancer Knowledge
Tables 2 and 3 outline the quantitative results of the written surveys and the results of the individual knowledge questionnaires. The number of correctly answered knowledge questions ranged from 1 to 9 (out of 10), with a mean of 6. The number of “I don’t know” responses to the knowledge questions ranged from 0 to 9, with a mean of 3. The question that most participants correctly answered was “A man’s chances of getting prostate cancer increase as he gets older” with all but one respondent answering this correctly as true. All respondents incorrectly endorsed the question “Prostate cancer is the number one cause of cancer deaths in African American men” as true. Several other incorrect responses were received for various knowledge questions related to prostate cancer symptoms, racial disparity among Black men, screening recommendations, what PSA testing and digital rectal exams (DREs) are for, benefits of early detection, and Medicare coverage for screening, indicating deficits in education about prostate cancer among some of the participants.
Health Care Information Seeking, Health Care Experiences, and Attitude Toward Health Care Reported by Study Participants—Survey Results.

Focus Group Participants’ Responses to Knowledge Questions—Knowledge Questions.

One response is missing.
Preferred Source of Medical Information
Figures 1 through 5 outline responses to the source of medical information, including to whom participants would go for medical advice and the preferred sources for receiving such information. The greatest number for each of these questions included a health care provider. With regard to the mode of delivery, the responses were fairly well distributed, with one-on-one or group setting being the largest along with electronic communication.

Sources Participants Would Go for Medical Advice

Where Participants Would Wish to Receive Information if They Had a Specific Health Care Concern

Participants’ Preference in Receiving Health Information

Participants’ Preference in Different Examples of Educational Websites

Participants’ Preference in Social Media Platforms
Qualitative Results: Major Themes
Beliefs About Cancer, Prostate Cancer, and Prostate Cancer Screening
Participants wanted to become more knowledgeable (and be able to apply their knowledge) about prostate cancer and gather more information to share with other community members. Further discussion indicated that this desire was partially driven by friends’ and family members’ struggles with cancer and concerns regarding their own health. Table 4 includes illustrative quotes for each of the theme areas below that were covered in the focus group discussions.
Themes Identified From Focus Groups.
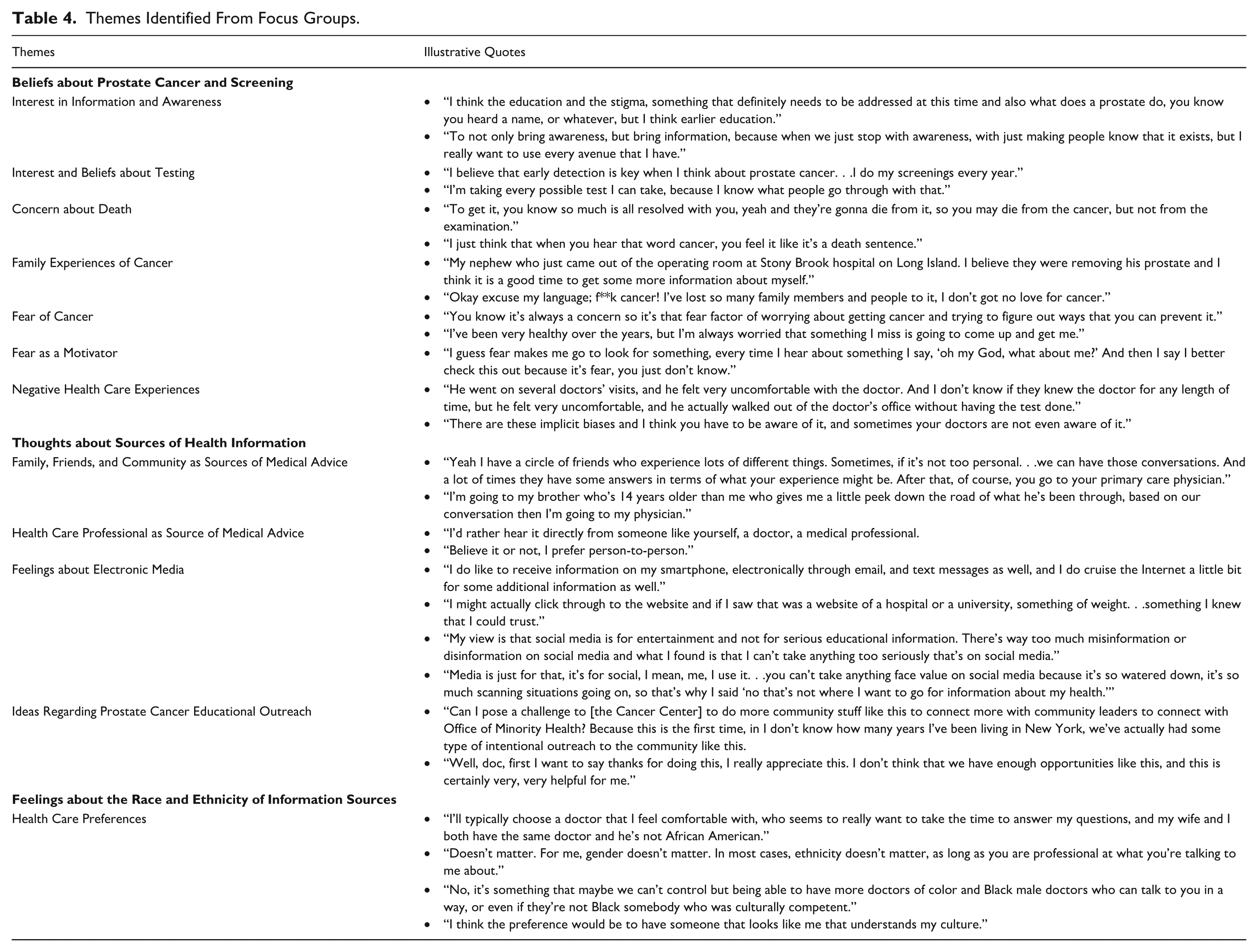
Interest in Information and Awareness
Participants mentioned that they were interested in seeking further information about prostate cancer to become more aware of the risks for themselves and their community members.
Interest and Beliefs About Testing
Most of the participants had already been screened for prostate cancer. They were interested in having these screenings for purposes of early detection and prevention.
Concern About Death
Many of the reasons for participation in this study included concern about the dire outcomes of prostate cancer.
Family Experiences of Cancer
Participants mentioned that they witnessed family members go through hardships due to cancer and wanted to spread awareness and take preventive measures so that they do not have to go through similar experiences.
Fear of Cancer
Due to cancer’s adverse effects, participants reported fear of developing cancer which motivated screenings. Participants regularly reported a preference for seeking professional medical attention, often after facing health concerns or being encouraged to do so by friends and family. There was no agreement among participants if their medical provider needed to be the same gender or ethnicity to receive adequate health care; most were satisfied with professional, competent, and compassionate treatment from any qualified individual. However, those who did report a preference usually also mentioned negative experiences they or someone they know has had within the health care system.
Fear as a Motivator
Participants sought health care treatment due to fear of health complications.
Negative Health Care Experiences
Participants reported negative interactions or negative perceptions regarding health care providers. This could also be a reason for them preferring to have a health care provider that was similar to them.
Thoughts About Sources of Health Information
During the discussion related to what participants look for in terms of receiving health care information, a common trend arose, suggesting they were open to receiving information via social media, but the account itself had to be a verified reputable source or the provided link was to a reputable site. In addition, they mentioned that they would be more likely to engage if the educational material portrayed individuals they could relate to or was being presented by someone they trust.
Family, Friends, and Community as Sources of Medical Advice
Participants mentioned how they sought medical advice from members of their communities, including friends and family, which ultimately leads them to seek professional medical care.
Health Care Professional as Source of Medical Advice
Participants indicated that they sought one-on-one medical care from reputable health care professionals.
Feelings About Electronic Media
Participants indicated they would be receptive to receiving health information from various sources of electronic media. Some participants felt that social media should not be used as a platform to receive medical information. They felt that it is not a professional outlet and not as reliable as other sources.
Ideas Regarding Prostate Cancer Educational Outreach
An overarching theme found in every focus group was the pleasant surprise that the Cancer Center was taking the initiative to hold these focus groups and working to connect with the community. Participants had suggestions for additional community outreach activities and welcomed the Cancer Center’s efforts to become more engaged with the community.
Feelings About the Race and Ethnicity of Information Sources
The participants reported that they would want to receive information from someone of the same race or ethnicity as them; however, that is not always possible as there are not always Black health care givers available. The more important aspect was that they felt comfortable with their health care provider.
Health Care Preferences
Many of the participants did not have a preference for what their health care provider looks like in regard to age, gender, race, and so on, as long as they were professional and treated them with respect. Some of the participants did have a desire for the health care provider to look like them with regard to gender, race, and so on.
Discussion
Through the use of focus groups, this mixed-methods survey study was able to assess knowledge, attitudes and behaviors toward prostate cancer screening among Black men in Suffolk County and to identify effective ways to educate this population. Despite encountering inherent challenges with recruitment, over time and with extensive community outreach and engagement, the study team was able to recruit 18 participants. The information collected during the group discussion indicated a relatively robust knowledge about prostate cancer, but a need and desire for more education, in particular about screening and risk factors that could be shared with the community. In addition, an interest in more educational interactions with the academic health care institution was expressed along with a need to increase the screening rates, as 11.1% stated that they did not know they needed to be screened.
Recruitment
In this study, the first observation noted by the research team was the difficulty in recruiting African American community members to participate in the project. It took extensive engagement efforts which included making contacts with 109 organizations to recruit the 18 people who ultimately participated in the study.
The difficulties in recruitment are not wholly unexpected, given that past research has shown lower participation of Black men compared with White men in cancer research. Black men are less likely to participate in clinical trials compared with White men (Lillard et al., 2022). A focus group study that assessed attitudes toward genomic testing and prostate cancer research among Black men found that mistrust in the health care system was the most common reason for lack of participation in research related to prostate cancer. Additional concerns among participants in that study included historic abuses of Black men in research, namely, the Tuskegee experiments, and feelings of fear and distrust extending from research to general mistrust of the medical system (Rogers et al., 2018).
A phone survey evaluating the legacy of Tuskegee and trust in medical care revealed significant race differences in medical care mistrust, with Black race being predictive of mistrust of medical care (Brandon et al., 2005).
A national telephone survey on participation in clinical research published in 2002 revealed that African American respondents were more likely than White respondents not to trust that their physicians would fully explain research participation and to state that they believed their physicians exposed them to unnecessary risks. African American respondents had a significantly higher mean distrust index score than White respondents. After controlling for other sociodemographic variables in a logistic regression model, race remained strongly associated with a higher distrust score (Corbie-Smith et al., 2002).
Knowledge
Those who were recruited for this study included individuals who were educated (>89% beyond high school), the majority (>50%) were between 40 and 60 years of age, were married or in a committed relationship (72.2%), and had some knowledge about prostate cancer screening (72.2%). Despite this, there were still topics related to prostate cancer in which knowledge could be improved, such as frequency, symptoms and risk factors, as well as information pertaining to screening. For example, opportunities for education might include some of the following elements: PSA is for screening (72.2% correct), DRE is for screening (61.1% correct), early detection improves survival (83.3% correct), and Medicare covers screening (33.3% correct). A majority of participants (61.1%) reported not having exposure to educational materials about prostate cancer, and more than a quarter (27.8%) did not feel at risk for prostate cancer. There was desire expressed in becoming more aware about prostate cancer and gathering more information to share with other community members. Efforts to identify opportunities for empowerment and promote collaborative learning could serve to promote SDM about prostate cancer screening among Black men and improve understanding as those discussions with health care providers take place.
These findings are consistent with past studies that have also demonstrated a reduced level of knowledge about prostate cancer among Black men, especially with regard to risk factors, screening age guidelines, and limitations (Ogunsanya et al., 2017). In addition, Black men may not receive all of the information needed to make informed decisions about prostate cancer screening (Leyva et al., 2016). Limited health literacy may contribute to poorer health outcomes (Muvuka et al., 2020), and higher percentages of Black and Hispanic adults than White, Asian/Pacific Islander, or Multiracial adults had Below Basic health literacy in a 2003 National Assessment of Adult Literacy (Kutner et al., 2006).
Attitudes
Participants expressed fear, experience with cancer in families, and concerns about death from cancer as motivators for screening. Almost all expressed trust in their health care giver and most were confident about talking to their health care giver about prostate cancer. Slightly less than three fourths believed they were at risk for prostate cancer, some because they had already had a screening. There was an expressed interest in becoming more aware of the risks for themselves and their community members.
The findings in this study of a relatively high level of trust in health care givers reveal a slight contrast to the literature that indicates a lower trust in the health care system among African Americans (Lillard et al., 2022). With regard to risk perceptions, our findings are consistent, in that a quarter of those surveyed did not feel they were at risk for the disease and participants voiced an interest in learning more about their individual and community risk factors. The finding related to risk perception may be somewhat confounded by those who felt they had low risk because they had already been screened.
While most of the focus group participants indicated that they trusted their providers, there is a difference between that type of trust with an individual versus trust of the institution as a whole. Participant comments such as a request for the institution to provide more educational and outreach activities in the community, similar to the focus groups being held, indicate a need for more institutional exposure in the community as a way to establish more trust.
Behaviors
About 72% of participants had already been screened, 11.1% did not know they needed it, 11.2% had decided against it after discussion with their provider, and 5.6% did not get screened for some other reason.
A 2022 literature review on racial disparities in men with prostate cancer described that Black men are less likely to get screened or receive treatment for prostate cancer, and nearly half of Black men reported being uneducated about prostate cancer screening (Lillard et al., 2022). In our study, 11% of participants reported that they were unaware of the need for screening, a finding lower than what is reported in the literature, but nevertheless, a barrier that might be overcome with education and community awareness interventions.
Participants mentioned that they sought medical advice from members of their communities, including friends and family, and the majority of participants indicated that they made their own doctor’s appointments. A 2019 focus group study identified that three broad types of social/cultural influence on motivation to seek health care services were identified: family, culture and upbringing, and peers (Eley et al., 2019).
Preferred Methods of Education that Would be Effective
Participants expressed an interest in having the Cancer Center engage more with the community and provide education. There was mention of advice-seeking for health care among family members and friends in the community, which ultimately leads to them seeking professional medical care. This is consistent with the three broad types of social/cultural influences on motivation to seek health care services that were identified in another focus group study and included: family, culture and upbringing, and peers. These social relationships are important in influencing African American men’s health-seeking behaviors (Eley et al., 2019). Despite expression of negative health care experiences among friends, families, and themselves, most expressed a preference for hearing from medical professionals to learn about prostate cancer, and more specifically Black male doctors. Increasing access to African American primary care providers has been shown to be associated with an increase in life expectancy among African American community residents (Snyder et al., 2023). There was also a preference for reputable health information sources, such as the CDC or a hospital website and acknowledgment that social media was more for entertainment than a way to obtain information. It was suggested that social media could be used to draw attention to educational opportunities. Preferences for website formats and sources of social media were varied for the most part, although engagement would likely be improved if educational material portrayed individuals to whom they could relate.
Limitations
The most important limitation of the current study is the generalizability based on the small sample size and the background of the participants. Although the study was performed to specifically understand the knowledge, behaviors, attitudes, and most effective tools for learning among Black men in Suffolk County, New York, the difficulty in recruiting participants makes it difficult to generalize the findings. The 18 participants were largely well educated, knowledgeable, and able to access Zoom, and a large percent had already been screened for prostate cancer. Thus, the participants may not represent those in the community who have not been screened and require the education to get screened. Among individuals with less education, or lower socioeconomic status, differing priorities, such as basic social determinants of health may impact effectiveness of the education strategies assessed in the focus groups. Individuals with lack of access to digital resources would require different educational strategies than were tested in the focus groups.
The originally intended size of each focus group was estimated at eight to 12 participants, which is noted in the literature as the ideal size (Halliday et al., 2021). Participant dropout rates as high as 50% are common barriers to hosting focus groups. It is suggested to over-recruit by five additional participants to account for no shows. These participation goals, however, proved difficult to achieve. The attrition rate for this focus group was 33%. There also may be a bias issue due to recruitment methods. Halliday et al theorize that high dropout rates are due to inconvenience, personal traits such as shyness, and location difficulties (Halliday et al., 2021).
Self-selection bias, in which participants self-elect to participate in a study, is another limitation. The participants who signed up for the study could have been better informed on prostate cancer and more engaged in health care issues than those in the target population. Respondents expressed being concerned about prostate cancer and felt at risk due to family history, which is what motivated them to get screened, seek out health information, and attend the focus group. Participants also mentioned how they witnessed family members go through hardships due to cancer and that they wanted to spread awareness and take preventive measures because of it. Those who participated may be less embarrassed than nonparticipants about discussing prostate cancer screening. The men not represented in this sample could be more hesitant, less informed, or have greater barriers to access of care. Differences between the two groups could be attributed to the varying levels of knowledge about disease and screening procedures, enhanced access to health promotion activities, being less or more fearful of discovering abnormal results, exposure to more aggressive behavior on the part of the provider with respect to screening, and receiving medical care in an environment that is more respectful toward the consumer.
Prior literature mentioned Black men’s attitudes regarding screening (i.e., they don’t talk about it until it is too late) as a possibility for those who did not participate. The lack of participation could be more nuanced. Masculinity has been found to be a key factor associated with the health behavior of African American men (Atakere & Baker, 2016). African American men could feel pressure to be strong and to not talk about the hardships they are facing or the pain they might experience. Gendered and racialized beliefs and norms have been associated with African American men’s lower medical assistance-seeking rates (Rogers et al., 2018). Generational along with racial/ethnic and gender roles in society play a role in the factors that shape African American men’s health.
Conclusion
The research team was able to characterize the knowledge, attitudes, and behaviors of the study participants, providing the Cancer Center community educators with evidence-based steps to effectively educate about prostate cancer screening among Black men in Suffolk County. While recruitment for the focus groups was challenging, opportunities to collaboratively increase knowledge about risk factors and screening, even among this generally well-educated study group who chose to participate, were identified. In addition, there was a need for raising awareness within the community both by health care providers and the health care institution. Educational opportunities may be enhanced by enlisting the aid of family and community members in transmitting messaging to influence screening behavior, utilizing Black health care givers whenever possible, and introducing reputable websites portraying relatable individuals furthere complemented by social media messaging.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883251377306 – Supplemental material for Black Men’s Prostate Cancer Knowledge, Attitudes, Beliefs, and Access to Health Information
Supplemental material, sj-docx-1-jmh-10.1177_15579883251377306 for Black Men’s Prostate Cancer Knowledge, Attitudes, Beliefs, and Access to Health Information by Linda Mermelstein, Jackelyn B. Payne, Rose Martillotti, K. Olivia Mock, Anne E. Moyer, Linda Bily, Giuseppina Caravella, Jaclyn M. Grimaldi, Yuri T. Jadotte, Jedan P. Phillips, Kathleen H. Scarbrough, Jenna Francois and Barbara D. Nemesure in American Journal of Men's Health
Footnotes
Acknowledgements
Katie Houghton, MA, MBA, Office of Community Outreach and Engagement, Stony Brook Cancer Center, Stony Brook Medicine provided administrative support for the study.
ORCID iDs
Author Contributions
Jackelyn B. Payne, PhD, is currently a Cancer Prevention Fellow in the Office of the Associate Director of the Behavioral Research Program, Division of Cancer Control and Population Sciences at the National Cancer Institute of the National Institutes of Health (NIH).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by IRG-21-143-01 from the American Cancer Society and an award from the Miriam & David Donoho Academy of Clinical and Educational Scholars (ACES).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.