
Abstract
This study aimed to investigate the effects of Tai Chi Softball (TCSB) training on the physical health of older men, with a focus on improvements in muscle strength, flexibility, balance, and blood lipid profiles. A 12-week randomized controlled trial was conducted, recruiting 140 men aged 55–65 years. Participants were randomly assigned to either a Tai Chi Softball group (TCSBG, N = 70) or a control group (CG, N = 70). The TCSBG engaged in TCSB training sessions 4 to 5 times per week, with each session lasting 70 to 90 min, while the CG maintained their usual daily routines without any additional interventions. Measurements were taken before and after the intervention and included waist-to-hip ratio (WHR), handgrip strength (HS), sit-and-reach (SAR), single-leg stance (SLS), vital capacity (VC), heart rate, systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol. The results revealed that after 12 weeks of TCSB training, participants in the TCSBG showed significant improvements (p < .05) in HS, SAR, and SLS, indicating enhanced muscle strength, flexibility, and balance, respectively. The VC also increased significantly, while both SBP and DBP decreased notably (p < .05). Moreover, significant reductions were observed in TC, TG, and LDL-C levels p < .05). In conclusion, TCSB training demonstrated efficacy in improving muscle strength, flexibility, balance, cardiorespiratory fitness, and blood lipid profiles in older men. These findings suggest that TCSB training can mitigate age-related declines in physical function and reduce cardiovascular risk in older men.
Introduction
As the global population continues to age, the health and well-being of older populations have become increasingly critical (Partridge et al., 2018). By 2050, the global population aged 60 and above is projected to double (Naja et al., 2017), presenting significant challenges for individuals, families, and public health systems (Prince et al., 2015). Among the aging population, the health of older men deserves particular attention. Aging is associated with a gradual decline in physical functioning, especially in muscle mass and strength (Papadopoulou, 2020), which directly impacts mobility and independence in daily life (Dos Santos et al, 2017). Research indicates that reduced muscle mass in older men substantially increases the risk of falls, which often result in fractures, prolonged immobility, and even long-term health and financial burdens (Benichou & Lord, 2016; Kirwan et al., 2020). Additionally, aging in men is frequently accompanied by rising lipid levels, including total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG), which are key risk factors for atherosclerosis (Mortensen & Nordestgaard, 2020). These lipid changes further heighten the risk of coronary heart disease and other cardiovascular diseases (Upadhyay, 2015). Addressing these health challenges requires identifying effective strategies to improve the physical health of older men through targeted interventions.
Physical activity, as a cost-effective, non-pharmacological intervention, offers significant benefits in addressing health concerns among older men (Rodrigues et al., 2021). Studies have demonstrated that moderate exercise slows muscle loss, reduces blood lipid levels, enhances cardiovascular health, and lowers the risk of age-related diseases (Cartee et al., 2016). In particular, exercise regimens combining aerobic activities with strength training have been shown to improve physical fitness, enhance balance, and boost cardiovascular function in older men (Seco et al., 2013). Among these, Tai Chi Softball (TCSB) is a modern adaptation of traditional Tai Chi principles combined with elements of racket sports. It involves using a lightweight racket to control a softball in smooth, continuous movements that emphasize coordination, balance, flexibility, and mindfulness. The practice is rooted in Tai Chi’s philosophy of balance and fluid motion, integrating gentle yet controlled swings, rotations, and weight shifts that promote both physical and cognitive well-being. TCSB has emerged as an innovative form of exercise that integrates the traditional principles of Tai Chi with the dynamic characteristics of softball. This low-impact and comprehensive exercise approach incorporates balanced, weight-bearing, and coordinated movements, potentially offering benefits such as improved muscle strength, better balance, and a reduced risk of falls (Zhong et al., 2020). Moreover, the gentle, mind-body nature of TCSB may help regulate lipid metabolism, improve cholesterol levels, and reduce the risk of cardiovascular diseases (Zou et al., 2017).
In recent years, studies have confirmed that TCSB has significant effects in improving bone mineral density (Xin & Guo, 2024), lower limb strength (Lou et al., 2017), balance (Lam et al., 2011), blood pressure regulation (Zou et al., 2017), and blood lipid profiles (Zou et al., 2017) in elderly women. However, most of this research has focused on perimenopausal or postmenopausal female populations, with limited attention paid to older men. Men and women exhibit significant differences in body composition, physiological metabolism, and health needs (Gordon & Hubbard, 2020). For example, men typically have higher muscle mass but experience a more rapid decline in muscle strength with age (Wilkinson et al., 2018). Furthermore, men are at a higher risk of cardiovascular diseases and dyslipidemia (Liu & Li, 2015). These distinctions highlight the necessity of tailored studies to address the specific health needs of older men and validate the effectiveness of TCSB for this population. Currently, systematic research is lacking on the role of TCSB in improving muscle strength, balance, and lipid profiles in older men. Exercise interventions that address the specific health challenges faced by older men play a crucial role in promoting their overall well-being, as highlighted in this study.
Overall, this study aims to explore the effects of TCSB on the health of older men, focusing on its potential to enhance muscle strength, flexibility, and balance, lower blood lipid levels, and reduce the risk of cardiovascular diseases. It is expected to provide a valuable theoretical basis and practical guidance for effective exercise interventions targeting the health needs of older men.
Methods
Research Design
This 12-week randomized controlled trial investigated the effects of TCSB exercise on health-related indicators in older men. Participants were recruited from the local community and randomly assigned to either the TCSB group (TCSBG), which underwent TCSB training, or the control group (CG), with 70 individuals in each group.
Randomization was conducted using the randomization function in Excel 2019 (Microsoft, Redmond, WA, USA). The TCSBG participated in TCSB training 4 to 5 times per week, with each session lasting 70 min and consisting of a 10-min warm-up, 50 min of practice, and a 10-min relaxation phase. Meanwhile, the CG continued their usual daily routines without any additional exercise interventions. Health-related indicators such as height, weight, waist circumference, hip circumference, waist-to-hip ratio (WHR), handgrip strength (HS), sit-and-reach (SAR), single leg stance (SLS), vital capacity (VC), heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DPB), TC, TG, LDL-C, high-density lipoprotein cholesterol (HDL-C) were assessed at baseline (week 0) and after the intervention (week 12). All assessments were performed by professional staff using a standardized protocol in a controlled environment to ensure consistency and reliability.
Participants
All participants were recruited from the LianHu elderly community in Xi’an. The sample size was determined using G*Power software (Version 3.1.9.7, Franz Faul, University of Kiel, Germany) (Faul et al., 2007), with the following parameters: α = .05, power = 0.85, effect size = 0.15, and a statistical test involving repeated measures with group interaction. Based on a design involving two groups and two measurement points, the required sample size was determined to be 51 participants per group. To account for potential dropouts, a total of 150 participants were initially recruited, and 140 participants successfully completed the study. The baseline characteristics of the participants are summarized in Table 1. Informed consent was obtained from all participants prior to enrollment. The study protocols were approved by the Institutional Ethics Committee of Xi’an Medical University (Number XYLS2025129) and adhered to the principles outlined in the Declaration of Helsinki.
Basic Participant Information.

Note. TCSBG = Tai Chi Softball group; CG = control group; BMI = body mass index.
The inclusion criteria for participant recruitment were as follows: individuals aged 55–65 years; no significant motor dysfunction, with the ability to independently perform daily activities; no prior systematic experience with TCSB exercise but a willingness to learn; no evidence of cognitive impairment, with the ability to understand and follow instructions; and voluntary participation confirmed by signing an informed consent form. Exclusion criteria included: a body mass index (BMI) exceeding 27; a history of cardiovascular disease; inability to adhere to the exercise intervention or follow-up schedule; participation in other exercise-related interventional studies that could affect the study outcomes; or a diagnosis of mild cognitive impairment.
Measurement of Health-Related Indicators
WHR = Waist Circumference/Hip Circumference
Measurements were obtained using a standard tape measure equipped with a tensiometer. Waist circumference was measured at the level of the navel, while hip circumference was measured at the widest part of the hips (above the transverse gluteal crease), with measurements accurate to 1 mm (Quintanilla, 2014). WHR = Waist circumference/Hip circumference (Wu, 2022). WHR ≥0.9 for men and ≥0.85 for women were considered abnormal (Ibrahim & Ahsan, 2019), and WHR ≥0.5 was considered abnormal (Nevill et al., 2020).
Handgrip Strength
The maximum isometric strength of the hand and forearm muscles was measured using a dynamometer (Mathiowetz, 2002). Participants were instructed to hold the dynamometer in their dominant hand, keeping their arm at a right angle with the elbow resting at their side. The middle phalanx of the fingers was positioned at the front end of the dynamometer handle to ensure proper placement. When ready, participants squeezed the dynamometer with maximum isometric strength and maintained this effort for approximately 5 s (Roberts et al., 2011). Each participant completed two grip strength tests, and the best result was recorded.
Vital Capacity
The participants stand facing the spirometer and begin with preparatory actions, such as chest expansion or deep breathing (Song et al., 2014). Next, they hold the mouthpiece of the device, position it correctly, and exhale as forcefully as possible into the spirometer. The exhalation force and rhythm should be moderate—neither too fast nor too slow—and continue until the participant can no longer exhale. At this point, the spirometer reading is taken and recorded.
Heart Rate
Measurements were conducted using a standardized electronic sphygmomanometer by trained investigators (Xue, 2003). Participants were instructed to avoid strenuous exercise, workouts, eating, or consuming caffeinated beverages for at least 1 hr prior to the measurement. During the measurement, participants were instructed to relax mentally and avoid exertion, talking, or movement. They were required to maintain a standard measurement posture, ensure the cuff’s center was at heart level, and leave enough space to slide a finger between the cuff and the arm. Two consecutive measurements were taken with a 1-min interval, and the average of the readings was recorded.
Sit-and-Reach
The tester instructs the participant to sit barefoot with legs extended straight on the board, ensuring both feet are firmly placed against the stop board (B. X. Zhang & Li, 2012). The participant is then instructed to bend their upper body forward while extending their arms, using the fingertips of both hands to push the measuring ruler forward until the maximum possible reach is achieved. During the test, the knees must remain straight, and both hands must stay in contact with the measuring ruler. Participants are required to perform the task to the best of their ability. The reading on the measuring ruler is recorded accurately. Each participant is given two test attempts, and the highest value is recorded.
Single Leg Stance
Participants stand naturally with both feet placed firmly on the ground to ensure proper leg support (Yao, 2008). Once the participant is ready, they close their eyes and lift one foot, at which point the tester begins timing. If the participant’s supporting foot shifts or if they place the lifted foot back on the ground, the timing stops, and the score is recorded to one decimal place. Each participant performs the test twice, and the highest score from the two attempts is recorded as the final score.
Blood Pressure
Blood pressure was measured using a mercury sphygmomanometer (Wei, 2012). Each participant’s blood pressure was measured three times after a 30-min rest, and the average of the three readings was recorded as the final blood pressure value (Wang et al., 2022).
Blood Lipid Metabolism Test
A 3 mL sample of fasting venous blood was collected, and TC, TG, serum HDL-C, and serum LDL-C were analyzed using an automated biochemical analyzer (Wang et al., 2018; Wen & Su, 2021).
Exercise Protocol
Before the intervention began, all participants underwent baseline testing for WHR, HS, SAR, SLS, VC, HR, SBP, DBP, TC, TG, LDL-C, and HDL-C. All assessments were conducted in an indoor gym at the community center under the supervision of an experienced researcher. Each test was performed twice, with a 3-min recovery interval between trials, and the best result was used for data analysis. Ethical protocols were strictly followed to ensure participant privacy and data security. Participants retained the right to withdraw from the study at any point without facing any negative consequences.
The TCSB training program was conducted over a 12-week period at the Xi’an LianHu Community Senior Center under the supervision of a certified Tai Chi instructor. Each training session was divided into three phases: warm-up, formal training, and recovery (Lou et al., 2017). The program was designed in two stages: an adaptation phase during the first 4 weeks and an intensive phase during the following 8 weeks, with progressive adjustments in training frequency, duration, and intensity. In the adaptation phase, participants trained 4 times per week for 1 hr per session. Each session began with a 10-min warm-up, which included dynamic stretching and simple Tai Chi movements to mobilize joints and prepare muscles for physical activity. This was followed by a 40-min formal training phase, during which participants learned the basic movements and the first section of the TCSB routine. Finally, a 10-min recovery phase involved static stretching and breathing exercises to promote relaxation and recovery. In the intensive phase, participants trained 5 times per week, with each session lasting 1.5 hr. The warm-up phase was extended to 20 min and included dynamic stretching along with a review of the basic movements learned in the adaptation phase. The formal training phase was increased to 70 min, focusing on learning more complex movements and the second section of the TCSB routine. Partner coordination and group exercises were incorporated to enhance interaction and improve participants’ coordination. The recovery phase was also extended to 20 min, with participants performing static stretching, breathing adjustments, and relaxation meditation to facilitate physical recovery and alleviate fatigue. This progressive structure was designed to gradually adapt participants to the exercise regimen, ensuring safety while maximizing both physical and cognitive benefits.
At the conclusion of the 12-week intervention, all participants will complete a post-test assessment following the same procedures as those used during the baseline testing. These assessments will once again be conducted in the indoor gym of the community center to ensure consistency in testing conditions.
Statistics and Analysis
All statistical analyses were performed using SPSS 26.0 (IBM, Armonk, NY, USA). The Kolmogorov–Smirnov test was applied to assess the normality of data distribution, while Levene’s test was used to evaluate the homogeneity of variances. Inter-group differences in baseline data were analyzed using independent samples t-tests, and within-group changes before and after the intervention were assessed with paired samples t-tests. Interaction effects between time and group were evaluated using repeated measures ANOVA. Results were expressed as mean ± standard deviation (Mean ± SD), and significant differences are indicated by p < .05, whereby * represents p < .05 and ** represents p < .01. For variables that showed significant intervention effects, post-hoc analysis was conducted to identify the specific sources of between-group differences.
Results
Baseline Differential Test
The baseline differential test results for participants in both the TCSBG and CG are presented in Table 2.
Differential Test of Participants at Baseline.
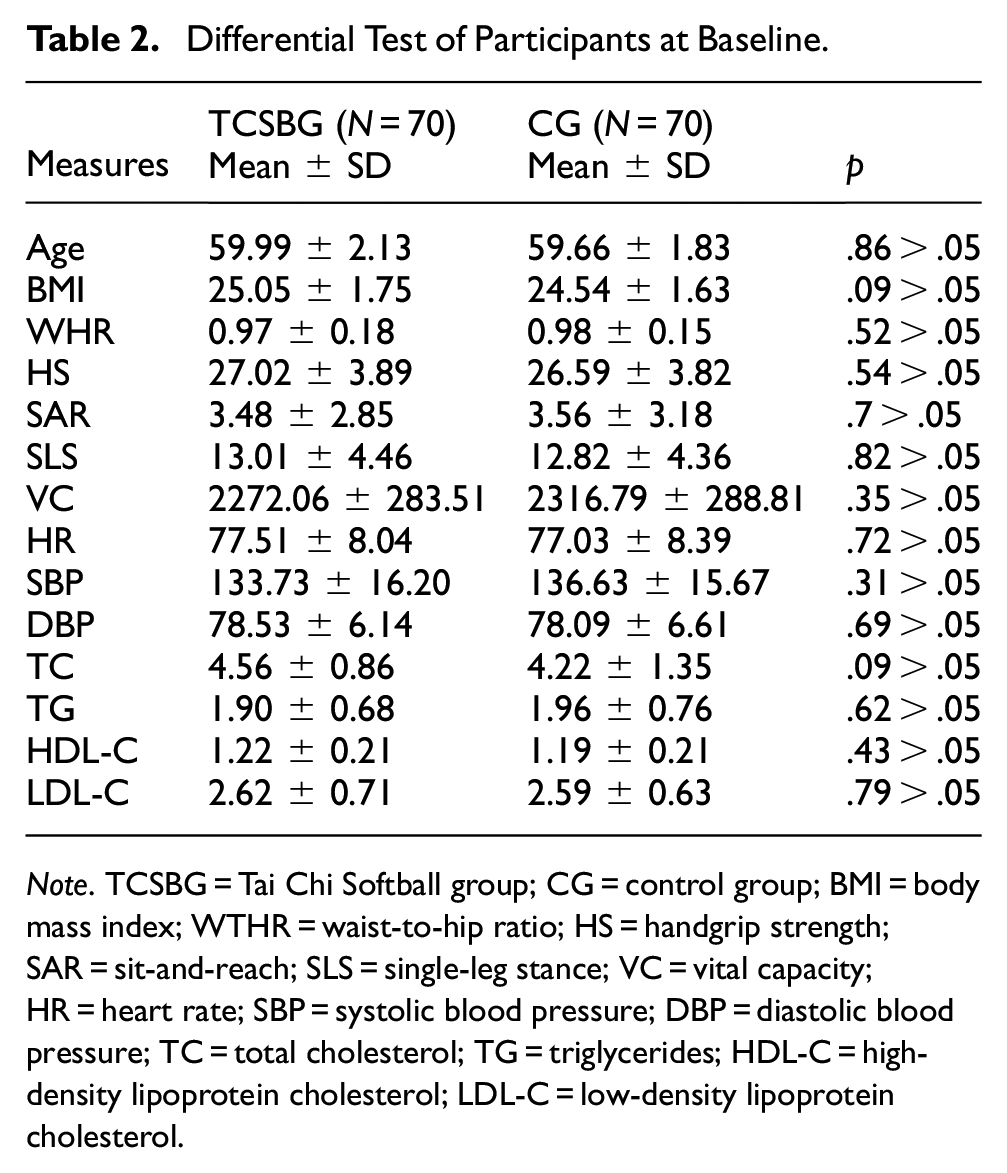
Note. TCSBG = Tai Chi Softball group; CG = control group; BMI = body mass index; WTHR = waist-to-hip ratio; HS = handgrip strength; SAR = sit-and-reach; SLS = single-leg stance; VC = vital capacity; HR = heart rate; SBP = systolic blood pressure; DBP = diastolic blood pressure; TC = total cholesterol; TG = triglycerides; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol.
The baseline results of the differential test between the TCSBG and CG are summarized in Table 2. The mean age of participants was 59.99 ± 2.13 years in the TCSBG and 59.66 ± 1.83 years in the CG. The BMI values were 25.05 ± 1.75 in the TCSBG and 24.54 ± 1.63 in the CG. For WHR, the mean was 0.97 ± 0.18 in the TCSBG and 0.98 ± 0.15 in the CG. Regarding HS, the TCSBG recorded a mean of 27.02 ± 3.89 kg, compared to 26.59 ± 3.82 kg in the CG.
Flexibility, as measured by the SAR test, averaged 3.48 ± 2.85 cm in the TCSBG and 3.56 ± 3.18 cm in the CG. Balance performance, assessed through the SLS test, was 13.01 ± 4.46 s in the TCSBG and 12.82 ± 4.36 s in the CG. VC values were 2272.06 ± 283.51 mL in the TCSBG and 2316.79 ± 288.81 mL in the CG.
For HR, the mean was 77.51 ± 8.04 bpm in the TCSBG, compared to 77.03 ± 8.39 bpm in the CG. SBP was 133.73 ± 16.20 mmHg in the TCSBG and 136.63 ± 15.67 mmHg in the CG, while DBP was 78.53 ± 6.14 mmHg in the TCSBG and 78.09 ± 6.61 mmHg in the CG.
Lipid profiles were similar across groups. TC levels were 4.56 ± 0.86 mmol/L in the TCSBG and 4.22 ± 1.35 mmol/L in the CG. TG levels were 1.90 ± 0.68 mmol/L in the TCSBG and 1.96 ± 0.76 mmol/L in the CG. HDL-C levels were 1.22 ± 0.21 mmol/L in the TCSBG and 1.19 ± 0.21 mmol/L in the CG, while LDL-C levels were 2.62 ± 0.71 mmol/L in the TCSBG and 2.59 ± 0.63 mmol/L in the CG.
Overall, the p-values for the comparisons between the two groups were >.05, indicating no statistically significant differences between the TCSBG and CG at baseline.
Effects of Intervention
Table 3 demonstrates within- and between-group comparisons of various measures, including WHR, HS, SAR, SLS, VC, HR, SBP, DBP, TC, TG, HDL-C, and LDL-C, which were assessed at baseline and week 12 using repeated measures ANOVA. At baseline, there was no significant difference between the TCSBG and CG on all measures (p > .05).
Within-Group and Between-Group Comparisons for Outcome Measures at Baseline and Week 12 (N = 140) Using Repeated Measures ANOVA.

Note. TCSBG = Tai Chi Softball group; CG = control group; WTHR = waist-to-hip ratio; HS = handgrip strength; SAR = sit-and-reach; SLS = single-leg stance; VC = vital capacity; HR = heart rate; SBP = systolic blood pressure; DBP = diastolic blood pressure; TC = total cholesterol; TG = triglycerides; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol.
p < .05. **p < .01.
By week 12, the TCSBG demonstrated statistically significant improvements in several health indicators, including HS, SAR, SLS, VC, SBP, DBP, TC, TG, and LDL-C, compared to the CG (p < .05). Specifically, HS in the TCSBG increased by 3.31 kg, rising from 27.02 ± 3.89 kg at baseline to 30.33 ± 4.11 kg. SAR performance improved by 0.74 cm, increasing from 3.48 ± 2.85 to 4.21 ± 3.15 cm. SLS duration also showed a significant increase of 4.62 s, from 13.01 ± 4.46 s to 14.44 ± 4.73 s. Additionally, VC in the TCSBG increased by 112 mL, from 2272.06 ± 283.51 mL at baseline to 2383.57 ± 288.59 mL. In terms of blood pressure, SBP decreased by 5.9 mmHg, from 133.73 ± 16.20 mmHg to 127.86 ± 16.01 mmHg, while DBP dropped by 3.76 mmHg, from 78.53 ± 6.14 mmHg to 74.77 ± 6.66 mmHg. Regarding blood lipid levels, TC decreased by 0.38 mmol/L, from 4.56 ± 0.86 mmol/L to 4.19 ± 1.14 mmol/L. TG levels showed a notable reduction of 0.47 mmol/L, declining from 1.90 ± 0.68 mmol/L to 1.42 ± 0.54 mmol/L. Similarly, LDL-C levels decreased significantly by 0.29 mmol/L, from 2.62 ± 0.71 mmol/L to 2.33 ± 0.70 mmol/L. In contrast, minimal changes were observed in WHR, HR, and HDL-C in the TCSBG by week 12. WHR decreased slightly from 0.97 ± 0.18 to 0.97 ± 0.17, while HR showed a small reduction from77.51 ± 8.04 bpm to 77.50 ± 8.98 bpm. HDL-C levels increased marginally, rising from 1.22 ± 0.21 mmol/L to 1.22 ± 0.21 mmol/L. Meanwhile, the CG exhibited no statistically significant changes in WHR, HS, SAR, SLS, VC, HR, SBP, DBP, TC, TG, HDL-C, or LDL-C by week 12 (p > .05).
The interaction effects of time and group were further analyzed, revealing significant main effects for both time and group in several key variables, including HS, SLS, DBP, and TG. Specifically, the following results were observed: HS: F(1,138) = 10.30, p = .002 < .01; SLS: F(1,138) = 17.13, p = .000 < .01; DBP: F(1,138) = 5.93, p = .02 < .05; TG: F(1,138) = 8.19, p = .005 < .01. Post hoc multiple comparisons confirmed that the main effect of time was significant for these variables, indicating notable improvements during the intervention period. However, no significant differences were observed between groups over the course of the intervention.
Discussion
This randomized controlled trial aimed to examine the effects of a 12-week TCSB training program on the health of older men. The findings revealed that participants in the TCSBG training experienced significant improvements in physical function (evidenced by enhanced HS, SAR, and SLS), cardiovascular function (increased VC and reduced SBP and DBP), and lipid profiles (reduced TC, TG, and LDL-C levels).
Physical Function
The study revealed significant improvements in strength, flexibility, and balance among older men following 12 weeks of TCSB training HS, as one of the primary indicators of upper extremity strength is widely recognized as an important predictor of various health outcomes (Bohannon, 2008). Numerous studies have shown that HS reflects the degree of aging in the body, with a tendency to decline sharply in populations that engage in little physical activity. Peolsson et al (2001) stated that maximum grip strength is reached between the ages of 30 and 35 years, after which it decreases by 0.5% per year between 35 and 45 years and by 1% annually after the age of 75. Goodpaster et al. (2006) similarly reported that muscle strength declines with age, particularly in men undergoing age-related hormonal changes, such as during menopause. In addition to biological aging and tissue atrophy, grip strength in older adults is closely linked to lifestyle changes, such as reduced physical activity, limited participation in sports, and less frequent engagement in physical exercise. This study demonstrated that TCSB training could effectively enhance muscular strength in older adults, a finding consistent with previous research (Lou et al., 2017). The observed improvement in HS can be attributed to the repetitive gripping and controlled softball movements in TCSB training, which strengthen the hand and forearm muscles and improve muscular endurance. Additionally, TCSB training enhances hand dexterity, coordination, and neuromuscular control, further contributing to the increase in HS.
SAR performance that reflects flexibility, agility, and the range of motion of the trunk, waist, and hip joints (B. X. Zhang & Li, 2012) also improved significantly in this study. Flexibility is influenced by the structural characteristics of joints, the volume of surrounding tissues, and the extensibility of ligaments, tendons, muscles, and skin (Behm, 2024). Children and adolescents are typically the most flexible, but flexibility tends to decrease with age (Gopnik et al., 2017). During aging, the joint capsules, ligaments, tendons, and surrounding structures undergo degenerative changes, reducing the body’s ability to stretch (Chhajer, 2016). The findings of this study align with previous research demonstrating improvements in flexibility following TCSB training (B. X. Zhang & Li, 2012). Similar studies have also shown that 24 weeks of Tai Chi training can enhance flexibility (Yu & Yang, 2012). Notably, TCSB training, which involves waist-centered movements such as figure-eight rotations, swinging, flipping, and side rotations, effectively engages the waist muscles and promotes flexibility in the waist joints.
An intriguing finding of this study was the significant improvement in balance after 12 weeks of TCSB training. SLS, a measure of balance ability, is an essential and simple indicator of the coordination and balance controlled by the brain’s right hemisphere (Goble et al., 2011). Among the most significant aspects of aging are the degenerative changes in lower extremity motor function and balance coordination (Lou et al., 2017). Waters et al. (2000) found that skeletal muscle loss begins at age 40 and intensifies after age 65, with more pronounced muscle loss in the lower extremities compared to the upper body. This loss of muscle strength and balance can significantly affect the functional independence of older adults. Previous research has demonstrated that 4 months of TCSB training can improve balance in older adults (Lai, 2011), consistent with the findings of this study. TCSB exercises, such as left and right swings, forward and backward circular motions, and rotational movements, require semi-flexed knee positions and constant weight shifting between the legs. Additionally, actions such as single-leg clockwise or counterclockwise rotations (180° or 360°) help strengthen the lower limb muscles and improve balance. These dynamic movements contribute to enhanced balance and coordination in older adults.
Cardiovascular Function
VC represents the maximum functional activity of the lungs and is an important physiological indicator reflecting chest development, lung function, respiratory muscle strength, and overall physical fitness levels (Cotes et al., 2009). As individuals age, elderly people experience progressive atrophy of respiratory muscles, rib calcification, spinal kyphosis, pleural thickening, and other factors that contribute to reduced chest size (Bonomo et al., 2008). In addition, increased fibrous tissue, decreased lung elasticity, alveolar atrophy, and reduced gas exchange capacity in lung tissue lead to a decline in respiratory function (Gea et al., 2020). In line with these age-related changes, the results of this study demonstrate that 12 weeks of TCSB training significantly improved lung capacity in older men. This finding is consistent with results from previous studies (Lai, 2011). Furthermore, research suggests that strengthening respiratory muscles and expanding chest cavity volume are primary mechanisms by which aerobic exercises enhance lung capacity (Aliverti, 2016). Specifically, during TCSB training, movements such as turning, drawing arcs, and tapping involve a wide range of motion, maximizing chest expansion and thereby contributing to the observed improvements in VC. The main reason is that during the practice of TCSB, the range of movements such as turning, drawing arcs, and tapping is relatively large, which can maximize chest volume and greatly improve lung capacity.
Beyond improvements in lung function, a large body of research has demonstrated that aerobic exercise can reduce SBP by 2% or 4–13 mmHg and DBP by 1% or 3–18 mmHg (Wang et al., 2022; Wei, 2012; Wen & Su, 2021; P. Zhang et al., 2024). For individuals with hypertension, many scholars argue that exercise therapy offers advantages over traditional medication. Unlike pharmacological treatments, exercise therapy avoids reliance on antihypertensive drugs and reduces associated side effects (Ozemek et al., 2020). Furthermore, studies have shown that exercise interventions in middle-aged and elderly individuals with hypertension lead to significant reductions in both SBP and DBP (Wei, 2012; Wen & Su, 2021). However, the effectiveness of exercise interventions in treating hypertension depends heavily on the design and implementation of exercise intensity, frequency, and duration (Alpsoy, 2020). Research confirms that mild to moderate-intensity training has a particularly significant antihypertensive effect in elderly patients with hypertension (Ghobadi et al., 2016). As a form of low-intensity aerobic exercise, TCSB has demonstrated positive effects in stabilizing and controlling blood pressure in older adults through consistent, long-term practice. This reduces the risk of hypertension and aligns with the findings of this study. Moreover, these results corroborate findings from previous research (Wei, 2012; Wen & Su, 2021), further emphasizing that long-term participation in aerobic exercise can effectively lower blood pressure in elderly populations.
Lipid Profiles
Hyperlipidemia is one of the major risk factors for atherosclerosis and coronary heart disease (CHD), both of which pose significant threats to human health (Cheung, 2005). The incidence of CHD is particularly high among individuals over the age of 45 (Madhavan et al., 2018). Numerous studies have confirmed that lowering blood lipid levels can significantly reduce the risk of CHD (Ference et al., 2019). The two key lipoproteins closely associated with CHD are LDL and HDL. High levels of LDL and low levels of HDL are strongly linked to an increased risk of CHD. Conversely, low LDL and high HDL levels can significantly reduce the risk of developing CHD. For instance, Tokmakidis and Volaklis (2003) demonstrated in a study on CHD patients that after 8 months of combined strength and aerobic exercise training, TC and TG levels decreased by 9.4% and 18.6%, respectively, while HDL-C levels increased by 5.2%. However, after discontinuing exercise for 3 months, TC and TG levels increased by 3.7% and 16.1%, respectively, and HDL-C levels decreased by 3.6%. These findings highlight that the beneficial effects of exercise on blood lipid metabolism are not sustained in the absence of consistent physical activity, emphasizing the importance of long-term exercise adherence. Relatedly, studies have shown that Tai Chi training effectively reduces TG, TC, and LDL-C levels while increasing HDL-C levels in middle-aged and elderly populations (Yin et al., 2023). The findings of this study further confirm that TCSB training produces similar effects. As an extension of Tai Chi, TCSB incorporates the principles of “hardness within softness” and “softness within hardness,” blending gentle and controlled movements with coherent and uniform force.
During TCSB training, the whole body engages in coordinated, relaxed exercises. These movements promote the opening and smoothness of microvessels, significantly increasing the number of open microvessels in the muscles and expanding the cross-sectional area of vascular communication. This improvement in microcirculation enhances the self-repair, self-protection, and efficiency of various organ systems, further contributing to overall health benefits (Bai, 2008).
Although this study demonstrates that TCSB training positively impacts muscle strength, flexibility, balance, cardiorespiratory fitness, and blood lipid levels in older men, several limitations should be acknowledged. First, the relatively small sample size of 170 participants may constrain the generalizability of the findings. Second, the study was conducted within a single LianHu elderly community, China, which may limit the applicability of the results to broader populations due to geographical and cultural factors. Lastly, this study did not include mental health indicators, despite evidence suggesting that Tai Chi exercises contribute to psychological well-being. Future research should incorporate a more diverse sample, extend to multiple locations, and evaluate mental health outcomes to provide a more comprehensive assessment of TCSB’s benefits.
Conclusion
TCSB training demonstrated efficacy in improving muscle strength, flexibility, balance, cardiorespiratory fitness, and blood lipid profiles in older men. These findings suggest that TCSB training can mitigate age-related declines in physical function and reduce cardiovascular risk in older men.
Footnotes
Ethical Considerations
The study protocols were approved by the Institutional Ethics Committee of Xi’an Medical University (Number XYLS2025060) and adhered to the principles outlined in the Declaration of Helsinki.
Consent to Participate
Informed consent was obtained from all participants prior to enrollment.
Funding
The study was supported by the Ministry of Education's Humanities and Social Sciences Research Fund under the project “Collaborative Research on Applied University Physical Health Education and Health Endowment” (Project No. 24YJA890004).
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.