
Abstract
Type II diabetes is increasingly becoming a problem in Latin American countries such as Peru. People living with diabetes must incorporate several behavioral changes in their everyday lives, which are done outside the purview of medical professionals. Support from friends and family members is essential to the successful management of any chronic condition. Our study discusses the role of family involvement in supporting the management of diabetes among Peruvian men and examines how masculine norms play a role in the way such support is received and perceived, and their influence in motivation to adhere to treatment recommendations. In-depth interviews with 20 men from a low socioeconomic status, aged 27 to 68 with a diagnosis of Type II diabetes were conducted. Our analysis suggests the importance of the close, complex, and integrated experience that connects family members and patients with a chronic condition. Participant accounts demonstrate they receive multiple forms of support from a diverse range of social relationships. The overwhelming majority of the people giving the support were female and were especially significant in supporting management practices. The participants’ accounts were able to demonstrate how living with a chronic condition, such as diabetes, affects the whole family–physically, mentally, and emotionally–and they experience the disease as one unit. Our study demonstrates the need for a family health experience approach that considers masculine gender norms around health and provides relevant insights to inform family-based treatments and therapies to allow for more and better targeted health care for men.
Keywords
Introduction
There are an estimated 33 million adults, ages 20 to 79, that are living with diabetes within the South and Central American Region, representing a regional prevalence of 9.5% (International Diabetes Federation [IDF], 2021). In Peru, the prevalence of diabetes has been estimated to be 5.91%, by the IDF; however, other studies estimate it at 6.2% (Bernabé-Ortiz et al., 2016) or even 7% (Seclen et al., 2015), and it was the fourth cause of death in Peru between 2014 and 2016 (Ministerio de Salud, 2019). This is the general trend in other low- and middle-income countries where according to the World Health Organization (2022), 77% of all noncommunicable disease deaths occur. However, not much consideration has been given to how these diabetes experiences are framed by gender norms.
New interventions and preventive care strategies need to be designed and implemented in a way that is appropriate to local gender norms and the social and cultural context in which people with diabetes live. This is particularly important given the severity of chronic conditions such as diabetes at the global and local levels. Studies show that men and women experience and respond to a chronic condition in different ways (Wade, 2009), and have different attitudes toward key health promoting and preventive behaviors such as diet (Gough, 2007; Munt et al., 2017) and exercise (Walsh et al., 2009; Young et al., 2012). There is an increased interest in assessing whether interventions targeted at diabetes management should be gender-based to ensure more effectiveness (Sharkey et al., 2020). Our study was particularly interested in documenting men’s experiences with Type II diabetes since there is little information about this specific group in Latin America, and masculine heteronormative gender norms in other regions of the world have shown to promote attitudes and behaviors that are detrimental to health (Courtenay et al., 2002). Although we recognize that there are multiple masculinities that are constantly evolving, the behaviors and attitudes expressed by our participants are aligned with a traditional binary understanding of gender.
In this article, we particularly look at the role masculine norms among employed men involved in heterosexual relationships play in (a) the way support from family and friends are received and perceived by Peruvian men with Type II diabetes and (b) the motivation to adhere to treatment recommendations. Previous studies have shown that men are more hesitant or reluctant than women to seek medical care for various health problems (Hawkins et al., 2015; Pihl et al., 2023) and are raised to be independent, self-reliant, strong, robust, and tough which impact their health beliefs and behaviors (Courtenay, 2000a). Not seeking care when in pain, not caring for one’s health, and not following doctor’s orders in relation to what they should eat or how they should behave often conflicts with cultural beliefs around men’s vulnerability and power, and male body composition—deemed structurally stronger and efficient (Courtenay, 2000b). A study in Brazil identified that diabetes interferes with spheres for enacting male gender identity among Brazilian men and found there is a competition between complying with being a good patient and staying committed to the responsibilities of being a good husband, as there is a conflictual relation between being a man and being ill (Kolling, 2012). In addition to the role of husband, the gendered division of labor plays an important role in the management of diabetes, as our study provides evidence for.
However, in the context of having Type II diabetes, it is essential to incorporate several changes in their everyday lives to successfully manage their condition and avoid complications, all of which might be influenced by gender norms. Life-changing adjustments to ensure proper glycemic control happen outside the purview of a clinical setting, but instead are done within the home, (Wagner et al., 2001) where support from friends/family is essential to incorporate behavioral changes into their everyday lives (Demirkol, 2005; Denham et al., 2007; Epple et al., 2003; Grabowski et al., 2019; Pamungkas et al., 2017). However, little is known about the way men with chronic conditions respond to family support and how such support is interpreted or filtered through gendered expectations.
Family members provide key sources of support that facilitate the introduction and continuation of such changes, which include modifying your diet, increasing your physical activity, taking medications on a regular basis, and attending medical appointments. Support that families provide is diverse: completing tasks such as scheduling appointments, calculating medication dosages, and cooking healthy meals; as well as providing comfort and encouragement (American Diabetes Association, 2014; Baig et al., 2015; Pesantes et al., 2018). Although literature has proved the importance of family involvement in caring for those diagnosed with chronic conditions, the family and social context of the individual are often left out of intervention and care plans. Not only does family and other social support help those suffering from chronic conditions create successful self-care behaviors, but social ties are known to reduce mortality risk among those with documented medical conditions (Umberson & Montez, 2010). Extensive positive health outcomes documented from social relationships has led experts from many disciplines to start viewing chronic conditions, such as diabetes, as a family illness and health experience (Fisher et al., 1998; Umberson & Montez, 2010). The diabetes illness experience is not limited to a single individual, but instead, is deeply connected and interwoven with the experiences of their loved ones as well.
Despite the recognition of the role of family support on diabetes management, there is not much understanding of the role that gender norms play in the way such support is received and perceived by the person living with the chronic condition. Most studies that look at the effect of masculine norms on health have been done in high-income countries, and often focus on the negative impact of masculine ideology on health-seeking behaviors and preventive care (Iwamoto et al., 2012). Recent studies and reviews have pointed to the need to develop health promotion strategies more appropriately designed for men (Doyal, 2001; Oliffe et al., 2020; Robertson et al., 2008). Within in the last decade, there has been little understanding between masculinity and the way family support could be used both as a tool to be successful in managing diabetes and as a motivator for treatment adherence.
Methodology
This was a qualitative study that used in-depth semi-structured interviews to explore the experiences of Peruvian men living with Type II Diabetes (hereafter “diabetes”) in two cities, Lima and Pucallpa. In Lima, participants were recruited as they waited in line for an appointment in two public health posts and one public hospital in the district of San Juan de Miraflores. They were invited to participate after confirming they had a diagnosis of diabetes for more than 2 years. We did not ask them if they self-identified as men, we simply approached them based on the way they outwardly presented. Once they agreed to participate, we asked for their phone number, and we called them to explain in detail the procedure (one 45-minute to 1-hour interview related to their experiences living with diabetes and their interaction with the public health system) and asked for a place we could meet for the interview. All interviews were conducted in a public space, usually in the food court of a mall or park. They received a US$25 compensation for their time. In Pucallpa, the recruitment was by snowball sampling, as one of the researchers knew a man with diabetes through a family contact. He then asked some friends and colleagues who also suffered from diabetes if they would be interested in the study. They then agreed to meet with the interviewer in the plaza or a restaurant where all interviews were conducted (except for one that was conducted at the participants’ home) after the study procedure, compensation, and topics were conveyed and they signed the informed consent form.
All interviews were conducted in-person during the summer of 2022 by MAP. All interviews were recorded, transcribed verbatim, and coded using the qualitative software MAXQDA© V.8.0. Data were initially coded by MAP and IF using a pre-defined codebook which included family support and behavioral changes to manage a chronic condition. Many of the codes were based off the primary thematic guide that was used to structure the interviews with participants. Emerging themes were identified and added to a fluid codebook, including instances of family hindrances and more specific support categories. The interview guide included a section on family involvement in patient care to understand the type of support (emotional, instrumental, financial, etc.) received by participants to manage diabetes. For each type of management practice, we explored how the family was involved with a particular aspect of care. What we learned was there are differences in which men and women provided support for the person with diabetes, as well as how the person with diabetes perceived that support. The analysis allowed us to have a more nuanced understanding of these processes. A third round of coding was conducted by IF with a condensed codebook including both prior and new codes pertaining to family support and hindrances. These codes were split into subcategories based on the participants stated experiences (medications, appointments, diet, physical activity, and advice) and placed within a family health experience and life context theoretical approach.
Results
Participants
All interviewees were over 18 years, had been diagnosed with diabetes for at least 1 year, and were enrolled in the National Health Insurance (Seguro Integral de Salud, SIS) plan which serves poor and extremely poor people. SIS was introduced in 2002 as part of the Peruvian Ministry of Health’s effort to ensure Universal Health Coverage. It offers a variety of services for people with diabetes: pharmaceutical, emergency, inpatient and outpatient primary-level, and specialty care (Cardenas et al., 2016). Ages of participants ranged from 27 to 68 years, most being married (65%) with only five single men (25%), one divorcee (5%), and one widower (5%). Participant occupations consisted of blue- and white-collar jobs and both part- and full-time work: drivers, community leaders, carpenters, fishermen, journalist, lawyer, and electrician, among others. In the following sections, we present the various types of support participants stated they receive from family members. We have grouped the following into categories: drive and motivation, appointments, financial, and behavioral changes at home (Table 1).
Participant Characteristics/Demographics

Drive, Motivation, and Advice
Participants perceive most of this support as helpful and not a hindrance, where the most favorable type of support they receive was emotional. The participants defined emotional support as actions that promoted “drive” and “motivation” to follow treatment protocol and/or live a happy, healthy life. The encouragement received was expressed in different ways: mentions of love, regular check-ins, general concern from family members, and support in familial responsibilities. Love and concern for their health was very important. Victor remembered one occasion in which his wife didn’t care about not receiving a birthday gift if the money was used for covering his medical expenses: “I don’t want anything, I want your health”∼ Victor, 56 (20 years T2D). Arturo’s partner, upon learning about the changes he had to introduce to manage his condition, stated: “we are going to follow to the letter what you have been told because we want to continue living with you, we want to continue being by your side.” Arturo, 34 (2 years T2D).
She shows her support by reiterating that the whole family will ensure his good health by following the doctor’s orders and treatment recommendations. The use of “we” is particularly important as it signifies it is not only up to Arturo to manage his condition alone, but instead, the responsibility of the entire family. Whatever the participant must go through during treatment and management, the family will go through it with him—be it that everyone must change their diet, remind the participant to take their medications, or attend all their medical appointments.
One particular downside of this “family experience” is that participants were consistently aware and worried about the negative implications their poor health could have on their families. As another participant expressed “Well, another thing [I think about] is the fear of being a burden to the family . . . I wouldn’t want to get sick and depend on being taken care of . . .” Giacomo, 59 (2 years T2D). Many participants expressed similar sentiments, specifically focusing on both the perceived and real burden on the family. These participants recognized the consequences of their ill-health not on them, but instead, on their families and immediate social relationships, who would also remind them of their concern: Son, you have to take care of yourself, keep your health stable . . . don’t make me suffer please. You already know what we’ve been through with your dad so please take care of yourself. Make my life happier, don’t complicate it. Brian, 29 (5 years T2D) She would say, “Grandpa, don’t go and die.” Raul, 68 (25 years T2D) Dad, I don’t want you to die, if you die, where am I going to go? Norberto, 40 (10 years T2D)
As these participant narratives demonstrate, the emotional toll of having a chronic condition does not solely fall on the person with the diagnosis but extends to those around them. The family experiences these emotions just as much or even more so. Almost every participant talked about the emotional effect of their diabetes on their loved ones, often depicting family and friends receiving the brunt of this burden. Participants shared stories of family members pleading, crying, and begging for them to care about their health as shown in Table 2:
Participants Expressions Showing Their Concern for Their Families

The display of concern, fear, and, most importantly, love for the participant by the family is what ultimately motivates them to become healthier and manage their diabetes with greater success. Not only are family units and other close social relationships important sources of vital support, but they are also often the sole motivator of the participant’s compliance.
Most of the examples provided by participants about the advice they receive come from friends, although family members were also mentioned as providing suggestions and general advice. Participants receive advice on diet, physical activity, and following doctor’s orders. Interestingly, one of the most common types of advice is related to the consumption of herbal remedies. They would consume herbal and fruit extracts, “natural pills,” and tea infusions made from plants and barks. This is much more common among those men who live in Pucallpa, a more rural city with a high influx of indigenous people who are known for their plant-based medical traditions. Not all of the herbal remedies are used to replace Western medicine, but instead are used to protect the organs, such as the liver and kidneys, and other bodily systems from the side effects associated with diabetes medications. Such side effects were a particular concern for the participants, and it was important to either supplement the Western medicine with more natural remedies or even stop their medications if they felt there was too much damage occurring.
Ensuring Medication Adherence
Taking their medications on a regular basis, as prescribed by the doctors, was a key practice encouraged by family members. Six participants (30%) mentioned their wives played an important role in medication management for their diabetes. The wives would buy the medication, pick it up from the pharmacy, remind them to take it, check that they really do take it, and in one case, they would advocate on their behalf at the doctor’s appointments to ensure a proper prescription: My lady tells me: “yes you are taking the pill, take it every day. You are going to take it right now.” Raul, 68 (25 years T2D)
In one case, a participant referred to his wife as his “personal GP,” as she learned how to inject insulin and then taught her husband how to do it: My wife began to put the insulin in my navel and there I learned until I lost fear . . . Esteban, 47 (8 years T2D)
Even with this ample amount of support, the participants recognize they still forget or don’t want to take the medication. The wives are actively aware of this fact and appear to be constantly revising their support strategies and methods to better suit the participant’s willingness and temperament.
Besides wives, adult (and sometimes young) children play a role in medication support as mentioned by six participants (30%). Children participate in similar ways to the wives; however, participants often reflect on their children’s support with more endearment, pride, and love, as presented in Table 3. In Pucallpa, there were more mentions about visits from their children as it is a smaller city and “dropping in” is still a usual practice. Interestingly, just as one wife was described as a general practitioner, one daughter was described as the participant’s “bedside nurse.” Leandro’s daughter is very actively involved in her father’s care: she will measure his glucose level, before and after he eats, will determine how much insulin to give him, which medications to give and when, and she injects his insulin as well. Family members have to not only provide emotional support but also learn how to provide direct clinical care and understand information about the condition to do so properly.
Participants Sharing Stories of Their Children Providing Medication Support.

Supporting Healthy Diets
Most of the participants in this study hold blue-collar jobs, particularly as mototaxistas (in Pucallpa) and taxi or truck drivers (in Lima). This type of work presents particular challenges surrounding the management of their diets. For some, it is very difficult to return home for healthy meals which leaves many participants left with fast food and street food as their only option. Eighteen out of the twenty (90%) mentioned, often multiple times, a large and vast support system to ensure they followed dietary recommendations. The two participants that did not specifically mention support from family members did so because they had no one at home to cook for them. Teofilo’s mother had passed away and the recommended dietary changes became unobtainable: Because of my mother’s death … I don’t have a mom; I don’t have someone to cook for me at home. I eat street food, I see a place where they make bland food [comida suave], I go to eat bland. But sometimes I find I eat the food in excess as well. Teofilo, 56 (2 years T2D)
In this case, the death of his mother demonstrates the importance of having a support system at home to provide food alternatives and healthy meals. When looking at the people who provided dietary support, 12 participants (60%) mentioned their wives, partners, or girlfriends. They would cook and prepare meals, supplement/revise certain recipes, deliver home-cooked meals to their place of work, and even adapt their own diets to match their husbands: She says: “I can make you a broccoli chaufa [Peruvian fried rice].”“A broccoli chaufa?’ I say, “how is it done?” Don’t worry, I’ll do it for you, she tells me. I brought her the products she asked for: she asked me for broccoli, she asked me for the grilled breast, and she made the chaufa. Arturo, 34 (2 years T2D) My wife dedicated herself to preparing the right food for me. Ignacio, 41 (11 years T2D)
While it is clear the participant’s partners do the majority of the cooking and meal preparation and are dedicated to provide an abundance of support, it is the participant’s children who help enforce the dietary changes. Eight participants (40%) specifically mentioned their daughters as a source of support for their dietary management practices. While the wives had also changed their diets to match the participants, it is especially appreciated when the children comply as well. The participants often felt pride but also guilt, as they believed their children were missing out because of them: My children accompanied me in what I was going through. They said, “Mom, no. If my dad eats that we all eat the same.” Arturo, 34 (2 years T2D) They [the children] used to drink soda, now they don’t drink anymore. They don’t take because they don’t want to, but they do it for me. That is, by taking care of me they no longer drink soda, they have also deprived themselves of many things, right? Facundo, 54 (8 years T2D)
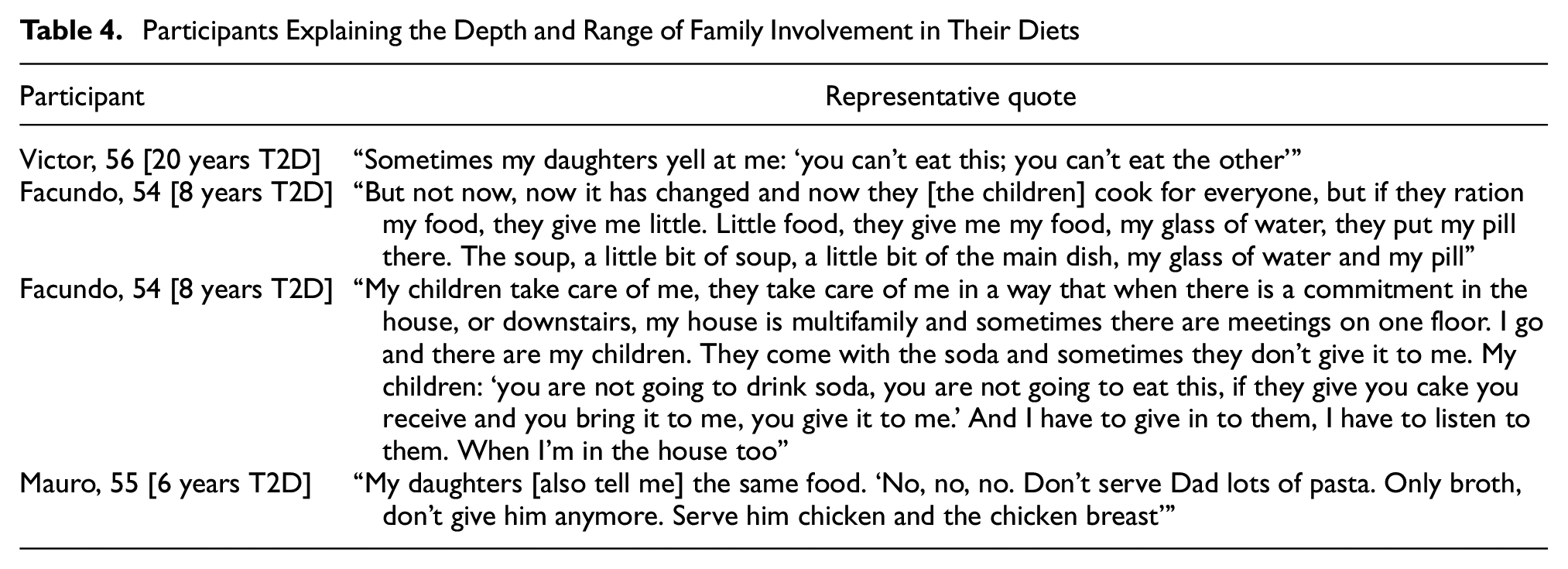
The children, most often daughters, would make sure their fathers were following the proper diet at home and elsewhere. They ration the participant’s food, prepare extra meals on special occasions, and are direct with their demands and expectations of their fathers which can be depicted in Table 4.
Participants Explaining the Depth and Range of Family Involvement in Their Diets
Breakdown of Family/Friend Support Into Pre-Defined Categories, Number of Participant Responses for Each Category, Percentage of Support Types Mentioned, and Support Person(s)


The shaded regions in Table 5 are spaces where there were no mentions of that type of support found in the interviews. The bolded numbers signify the largest amount of mentions for a specific support person - we just wanted to highlight how the majority of mentions of people providing support were about females/wives.
Percentages come from the number of times participants mentioned receiving support from family and/or friends. bThis category includes other kin/family members, such as brothers/sisters, uncles/aunts, in-laws, and so on.
Family gatherings and meals are particularly valued for the participants, as they are important, and common, in Peru. For participants, it is often very difficult to manage their diets during these events. Family members will cook traditional dishes, fried foods, and desserts, all of which are often not part of a sustainable diabetes regimen. As presented in Table 2, Facundo’s children understand how difficult it is to maintain his diet when at these family events, therefore, they come up with a plan beforehand and are sure to remind their father what they can and can’t eat, even going as so far to force their father to give them the unhealthy foods if provided to him. Giacomo’s daughter goes out of her way to prepare something just for him when she knows he has a family gathering to attend where there will most likely be food he can’t eat.
It is important to acknowledge that in three cases (15%) the intensity of the family involvement/support was perceived as a hindrance for participants, especially when the men felt as if they were being controlled by their wives. Despite this fact, the three participants overall appreciate and accept the care and support they receive from their families. Gender is not the only factor that frames support, as there might be other elements which need to be understood. The promotion of diabetes management needs to be tailored by both health care providers and family members.
Financial Support
Despite the fact that all participants have their appointments, exams, and medications covered by the SIS, there are still instances that require them to spend money, either for buying more healthy ingredients, medications when they are out of stock in the public pharmacies, or specialized care they would rather have in a private clinic. Nine participants (45%) mentioned they received some type of financial support from their relatives and friends. This support took many different forms, including cash (gift or loan), buying medical equipment/supplies, money for food, and ensuring in times of need that they had enough supplies to manage their diabetes. Participants noted how intensive and personal the financial support often was, as there were constant check-ins asking if they were okay and if they needed anything more. In one case, Arturo’s mother decided to quit her job to care for her son full-time, and in another case, Norberto’s sister gave him her house in Pucallpa, as she didn’t want him to worry about being able to financially afford somewhere to live. Interestingly, in our study, it was mostly women providing the brunt of the financial support for those with diabetes. However, the financial support was identified to be less about gender and more about who within the family had the capacity to provide the funding.
Appointments
Eleven participants (55%) mentioned the involvement of family and friends with either taking them to appointments, suggesting to seek medical care, encouraging regular/routine medical appointments, or forcing them to see a doctor. This was particularly important when the participants first started experiencing unmanaged diabetes symptoms. Although all participants mentioned they had public health insurance, which should cover all medications, appointments, and exams, for critical situations, five participants (25%) used private services for medical emergencies and diagnoses. The decision to use the private medical services almost always came from the family member prompting, assisting, and even covering the expenses associated with the necessary care. For example, the daughter of one participant, Leandro, decided to take him to a private doctor when a foot injury became critical due to the neuropathy and slower rate of healing often caused by diabetes.
Discussion
Our study has analyzed the perspectives of Peruvian men with diabetes and showed the intense and diverse support they receive from various family members and friends, and the role masculine gender norms play in the way support is interpreted. Similar to other studies (Fisher et al., 1998), we argue that a chronic condition is experienced by the whole familial unit. This is particularly relevant in Latin American culture, where other studies (Becker et al., 1998) have reported diabetes management is conceptualized as a family responsibility—mothers, spouses, children, aunts, and uncles are all expected to help aid in assuring proper and consistent diabetes management. Our study furthers such findings as it highlights the relevance of understanding the way family support is received and interpreted by male patients.
In other studies (August & Sorkin, 2010; Cherrington et al., 2011; Pihl et al., 2023; Sandberg et al., 2006), it has been reported that men receive greater support from their spouse and other members of a social network, as well as being more likely to perceive the support in a more positive light than women with a chronic condition. In addition, it has been identified that utilizing spousal control is more effective for men when compared with women (Westmaas et al., 2002). Research has demonstrated that male patients received more spousal dietary support,—specifically planning meals, buying food, and cooking—which highlights both a gendered division of labor within the household and an implied traditional feminine expectation of caregiving (August et al., 2021; August & Sorkin, 2010; Flagg et al., 2014; Pihl et al., 2023; Sandberg et al., 2006). Furthermore, Sandberg et al. (2006) identified that, in contrast to male spouses supporting women with diabetes, female spouses used more accommodating or collaborative language, such as helpful questions, reminders, or advice.
Tailoring the style and shape of support to male patients is particularly important. Female spouses in Sandberg’s study, found that their “nagging” was a threat to their partners sense of control and autonomy, and they modified their behavior to best suit their partner (Sandberg et al., 2006)—this resembles our findings, as spouses tended to adapt their support. Tucker and Mueller (2000) in August and Sorkin (2010) reported that married diabetes patients might be less likely to respond to pressure, not only due to psychological/physiological stress, but because the assumed intent behind these techniques are perceived as more focused on controlling the patient’s behavior, rather than promoting good health and wellness. This technique is known as “positive social control,” where others utilize expressions of worry, reminders, and other attempts at influence to elicit positive emotions in the recipient (August et al., 2021)—our study population was most responsive to this type of persuasion. While this study did not investigate women’s experiences with diabetes, and thus cannot compare results, our findings demonstrate a seemingly large proclivity toward men both accepting and acknowledging the support of their female spouses and other family members within the social network. Future studies should interview both men with diabetes and their female caregivers.
Participants in our study were willing to accept the help offered by their family and friends because they saw it as an expression of love as well as concern for the potential negative implications of poor health in their capacity to fulfill their (male) role as parents and providers. In Brazil, DaMatta (1997a, 1997b) argues that the sphere of the street and home are gendered and tied to the public world of men and the domestic world of women. In a study investigating the barriers for men and women with diabetes, Cherrington et al. (2011) reported that both men and women discussed physical activity/exercise in relation to work; however, for women, this was associated with housework and traditional gatekeeping roles, and for men, physical exertion almost always referred to manual labor. In terms of medication adherence, men cited barriers relating to long, static work hours that interfered with meals, therefore, leading to most instances of eating out at restaurants and fast-food establishments for the sake of convenience (Cherrington et al., 2011). Our study mirrored such findings, as well as identifying that women were more attentive and concerned for their spouse’s diet and ability to access healthy food options in the home and workplace.
Studies on men’s health experiences (Novak et al., 2019; O’Brien et al., 2005) have identified that men weigh their health care decisions (such as taking time off from work) vis-a-vis the financial implications for their families, while also taking actions to preserve or restore more valued masculine role (such as sexual life). When successful diabetes management conflicts with the obligations men have as providers for the family, work is often prioritized (Kolling, 2012). Men with diabetes in Brazil are reported to not follow doctor’s orders because it required them to stay at home and it affected their responsibilities as a husband—work obligations tend to organize their lives and are inextricably connected to expectations of being a provider for the family (Kolling, 2012). While our study primarily analyzed the various ways in which family members supported diabetes management, we found that the kinds of jobs held by the participants interacted with the type of help they received from family. Thus, future studies could emphasize the interplay between family involvement and working responsibilities of the person with diabetes, which are affected by one’s occupation.
While our study findings echo this phenomenon, Cherrington et al. (2011) suggest that even though men with diabetes are aware of the factors inconveniencing their management, they lack the necessary tools or confidence to overcome these barriers. Williams (2003) reports that those dealing with extensive or unusually high levels of stress often do not make prevention and disease management a priority. The men in our study had consistently fragile working statuses, which is known to increase or heighten levels of worry. While this was true for the current study’s participants, they were able to overcome multiple barriers with the help of family and friends—as well as prioritize disease management and treatment adherence—when they were reminded of their role as a father, husband, or son (Pesantes et al., 2023). Family members helped men realize their inability to successfully manage their disease might translate into them becoming an even bigger, tangible burden on the family. The real consequences of inadequate management of their diabetes became a motivator for men to accept assistance from others.
Similar to other studies (Samuel-Hodge et al., 2000), our results show that those providing care are mostly female family members. Norcross et al. (1996) reported in his study on health-seeking behaviors in California that women are more likely than men to encourage their spouses to seek health care, monitor their health, and utilize health services. Our study furthers such findings as the way support was provided by family members differed depending on who was providing it. Overall, wives/female partners were more “intrusive” in their support while children, especially daughters, would also motivate their parents using the love for them as a way of cajoling their fathers to control their diets or take their medications. Medication adherence was of particular concern for family members and the participants, as they often found it difficult to be consistent with physician recommendations on dosages and frequency. However, one of the main reasons for a lack of adherence to medications, as explained by participants within the study, was due to perceived consequences of long-term use of Western medications on the body. Interestingly, a study in Brazil reported that none of the participants liked to take insulin because the common insulin injection places on the body are readily exposed to the public (Kolling, 2012). Kolling (2012) also reported that being dependent on insulin made the participants feel restricted in their freedom: one participant said the dependency on medication to stay well would make him weak and live as if he was sicker than he actually is: “You need to control diabetes so it will not control you.” Knowing that men were hesitant and oftentimes unwilling to adhere to pharmacological interventions, Brazilian doctors would use the prescribing of injectable insulin as a threat to their male diabetes patients (Kolling, 2012).
Carbone et al. (2007) reported that Hispanic males with diabetes often rely more on women because they hold more central roles in the household, especially for meal preparation. Having their family, particularly their wives and partners, assist them with cooking and recipe adaptation caused a decrease in the emotional impact of diabetes management. This attitude toward ill-members of the family is connected to “familismo” among Latinos, which is a cultural value associated with the expectation on one’s family to provide emotional and instrumental social support, as well as the sense of obligation to take care of one’s family, and to take one’s family into consideration when making decisions (Calzada et al., 2012; Sabogal et al., 1987; Valdivieso-Mora et al., 2016). With this being said, there must be a balance in this relationship of primary caregiver and being a daughter, wife, son, and so on so as to not strain the social relationships in the participant’s life. The responsibility of striking that balance falls on the participant and the caretaker, to not overburden one member involved within the family experience, especially the women.
Although previous studies have proposed that women tend to need more emotional support than men (Choi et al., 2015), our study shows that among Peruvian men, psychological support from family members is also essential for strengthening their ability to successfully and confidently manage their diabetes since this condition is experienced as a family event. Similar to what Sandberg et al. (2006) argue, to improve diabetes management, it is important to assess both patients and spouses. This study suggests the beliefs, attitudes, and knowledge in approaches to support differs by gender, and thus, a discussion with both parties to understand gender styles and expectations will facilitate collaboration and improve support for diabetes management. These results highlight the importance of considering gender differences in the design and content of health education interventions for men with diabetes, as well as the familial, cultural, and social context of the patient in order for treatment plans to be successful.
Limitations
Our study only collected data from male participants which provides only one side of the story. The perspective of caregivers around the support they provide was not included in the interview process; therefore, their insights and experiences could not be shared in detail and would have complemented men’s views.
Conclusion
Family support is a fluid endeavor, as family members experience and accompany patients in various ways and adapt to the needs of their loved ones as they navigate their chronic condition. Just as families learn to provide targeted support for treatment management, they also learn to provide targeted motivation and drive for the patient—health education programs could benefit from such an approach. For future research and practice, a life course approach should be used, as a person’s support system, priorities/values, and responsibilities change over time. In Latin America, family and a man’s role, responsibility, and purpose within the family comprise of key cultural factors in a person’s ability to successfully manage their chronic condition. People diagnosed with diabetes must be given the tools and resources to successfully revise and adapt their behaviors given the fluidity of their life, cultural family ideals, and support systems.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883241239552 – Supplemental material for Men With Type II Diabetes in Peru: The Role of Masculine Gender Norms in the Perception of Family Support
Supplemental material, sj-docx-1-jmh-10.1177_15579883241239552 for Men With Type II Diabetes in Peru: The Role of Masculine Gender Norms in the Perception of Family Support by Isabella Ferrazza and M. Amalia Pesantes in American Journal of Men's Health
Footnotes
Acknowledgements
Our gratitude and utmost appreciation goes to the men who agreed to participant in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was possible thanks to the support of the Dickinson College Research and Development Committee.
Ethics Statement
All procedures were approved by the Dickinson Colleg Institutional Review Board (IRB Study #: 1051).
Informed Consent
Written informed consent was obtained from all participants included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.