
Abstract
Numerous case reports exist on penile strangulation injuries and extrication methods; however, the care and long-term consequences of penile strangulation injuries have been under-reported. Our aim is to investigate the long-term outcomes and sequalae following penile strangulation injuries. The PubMed Medline database was searched using the keyword string “penile strangulation,” “penis strangulation,” and “constriction” for all studies reporting outcomes of published penile strangulation injuries. Articles were evaluated for follow-up after strangulation injury, strangulating agent, extricating agent, and sequelae of injury. Fifty-six studies resulted with reports of 100 cases of penile strangulation and extrication from January 2000 to December 2019. The mean patient age was 41 (range: 3–86) years. Twenty-four (24/100) cases reported sequalae following extrication. Follow-up ranged from 2 weeks to 7 years with median follow-up time in the 7- to 12-month grouping. Metal rings comprised 36% (36/100) of strangulation agents and 50% of reported incidents were attributed to sexual activity. To our knowledge, this is the only study focusing on long-term outcomes after penile strangulation. This review provides a summary of 56 studies that document penile strangulation injuries over the last 20 years. Although a wide array of penile strangulation injuries have been documented in the literature, reports lack secondary management and long-term outcomes after removal of the strangulation device. We recommend that providers report long-term penile strangulation outcomes for future urologic evaluations after extrication.
Introduction
Penile strangulation is a rare urological emergency requiring prompt evaluation and treatment. Entrapment of the penis by a foreign object causes blockage of vascular and lymphatic channels leading to inflammation, edema, and ultimately necrosis (Ivanovski et al., 2007). Resulting injuries can vary from mild edema to gangrene, necrosis, or sepsis depending on the timing of injury recognition and subsequent extrication (Bhat et al., 1991).
Although the incidence of penile strangulation is unknown, these injuries have been reported in males of all ages. In the pediatric population, genital examinations for evaluation of penile edema have revealed hair tourniquets. Self-applied objects ranging from metallic objects to plastic bottles have been reported in the adult population. This practice is often attributed to sexual curiosity in male adolescents, while a desire to increase sexual performance or autoerotic behavior has been reported in middle-aged and elderly men (Ivanovski et al., 2007; Perabo et al., 2002). Regardless of the reason for placement, each strangulation agent can pose unique challenges to the treating urologist (Noh et al., 2004).
Penile constriction is frequently reported as a case report or limited case series that focuses on the offending agent and the physician’s approach to removing the foreign body. The first case in the literature was reported by Gauthier in 1755, in which he used clamps to free the penis and testicles of a 16-year-old from a steel lighter (Gauthier, 1755). In 1991, Bhat et al. introduced a 5-point grading scale for penile strangulation injuries based on their experiences treating eight patients (Bhat et al., 1991). The scale ranged from grade 1 edema of the distal penis with no evidence of skin ulceration or urethral injury to grade 5 with gangrene, necrosis, or complete amputation of the distal penis (Bhat et al., 1991). This grading scale has not been widely popularized, possibly due to the low sample size.
Although various methods and approaches to removal of the strangulation agent have been reported in detail, few reports have focused on secondary management of strangulation injuries and long-term outcomes for assessment of sequelae that may arise from the initial insult (Schellhammer & Donnelly, 1973; B. B. Sinha, 1988; Vähäsarja et al., 1993).
Thus, in the present treatise, we sought to evaluate the current body of contemporary literature involving penile strangulation and extrication. Our primary objective was to evaluate long-term outcomes of strangulation injury after extrication. Our secondary objectives were to characterize the incidence of individual strangulation agents, methods of removal, reason for placement, and patient demographics. To our knowledge, this is the first systematic review to analyze the literature regarding this topic.
Materials and Methods
In December 2019, a literature search of PubMed MEDLINE for all studies published between January 2000 and December 2019 was performed using a predefined search strategy. Database query was performed using the following search terms: “penile strangulation,” “penis strangulation,” and “constriction” as the main search term. All identified studies were screened by title and abstract for initial review (e.g., first level assessment). Eligibility criteria were applied to full text articles (e.g., second-level assessment) using predefined parameters. Studies in English reporting outcomes were considered if they were published in a peer-reviewed journal. Focus was placed on studies reporting secondary management after initial extrication of penile injury. When possible, we extracted primary outcome data regarding the long-term sequelae after the inciting agent was extracted. Patient age, strangulation agent, reason for strangulation, extrication agent, and length of follow-up data were also extracted. Excluded from consideration were studies not available in English, strangulation not involving the penis, and cases based on animal models. In cases of duplicate studies or studies reporting outcomes from the same cases, the most recently published study was assessed. References of all full-text articles assessed as part of the second-level assessment were reviewed to ensure all relevant articles had been surveyed. Two reviewers independently performed two separate searches before developing a finalized list. Disagreements were resolved by a third independent reviewer. Of the 173 yielded publications, there were no duplicate studies found. After abstract and title review of the studies, 105 studies were not relevant to the study. Ultimately, full-text review yielded 56 studies which were included in the final analysis (Figure 1). Given the retrospective nature of this work and review of prior published manuscripts, ethics committee approval nor informed consent from the study population was not required.

Article Inclusion Selection Criteria
The categorical variables were reported as proportions, and age was reported as mean, median, and range. We compared age across different groups using Kruskal–Wallis test. The categorical variables were compared across different groups using Fisher’s exact test. All significance tests were two-sided, with a p value <.05 considered statistically significant. Statistical analyses were performed using Statistical Analysis Software (SAS) version 9.4 (SAS Institute Inc, Cary, North Carolina).
Results
In total, 56 studies with a total of 100 patients treated for penile strangulation were included in our analysis (Table 1). The average patient age was 41 (range: 3–86) years. Of the 100 cases reviewed: 24% (24/100) of cases reported some degree of adverse sequelae from the initial injury. Follow-up care ranged from 1 week to 7 years, with median follow-up time in the 7- to 12-month grouping. The 7-year follow-up was attributed to penile strangulation by hair on a 13-year-old boy. Fifty percent of injuries (50/100) occurred during sexual activity with metal rings and polyethylene terephthalate (PET)-based substances (e.g., plastic bottle) being the main causative agent for strangulation 36% (36/100) and 13% (13/100), respectively. For statistical analysis, we grouped clinically similar strangulation agents together (Figure 2). Metal rings included ball bearing rings, bronze, bull ring, iron, steel, wedding rings, and metal hoops. Metal tubes included metal pipes as well as a metal axtree. Threads included hair, cotton, and polyester mesh. Bottles included all plastic and glass bottles. The reported reasons for strangulation agent placement are shown in Figure 3.
Penile strangulation reported presentation and follow-up from 2000–2019

NR = Not reported.

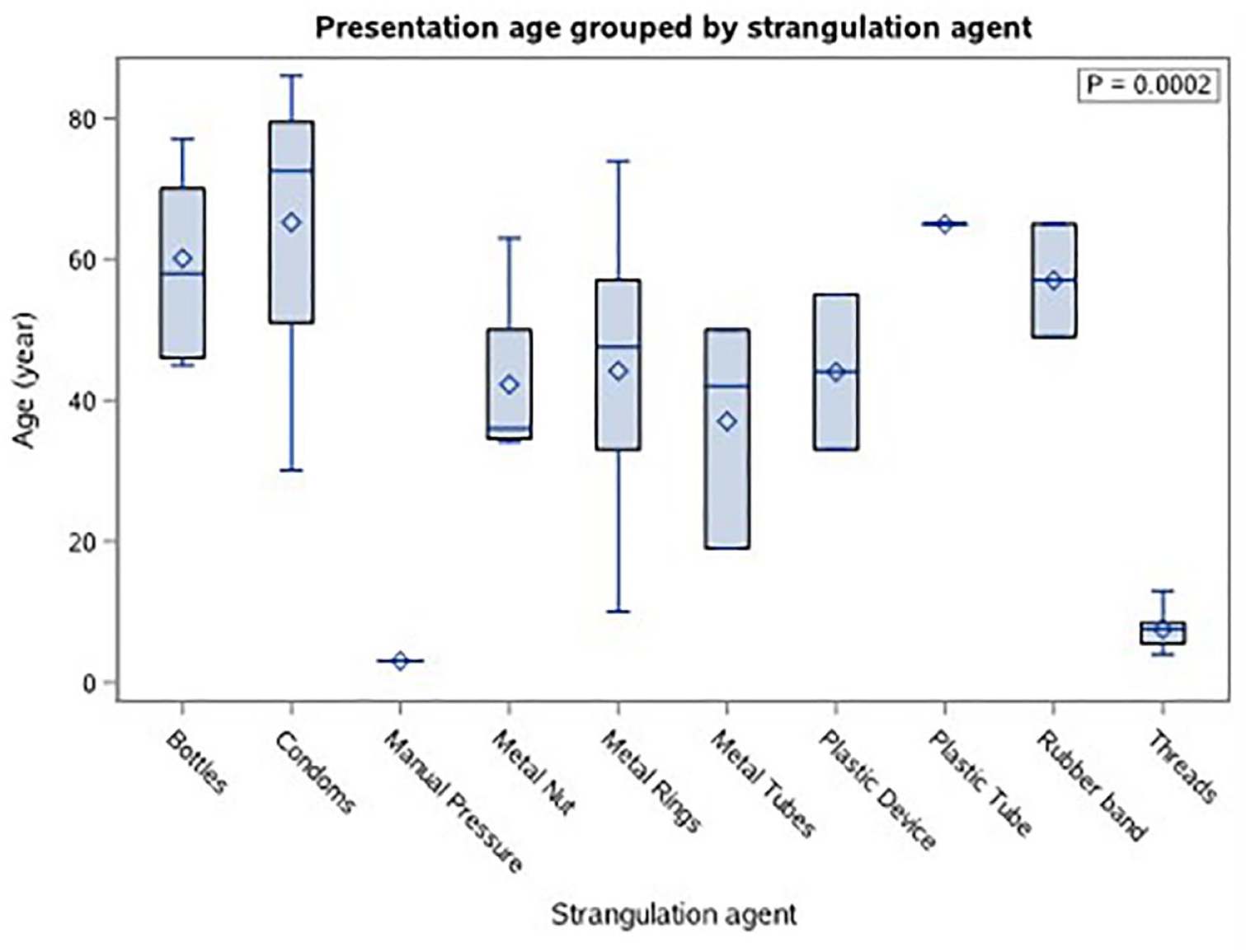
Presentation Age Grouped by Strangulation Agent

Presentation Age Grouped by Reason for Placement
Extrication methods varied widely; however, manual removal, Ortho pliers, and Gigli saws were the most common methods for removal of the strangulation agent. Metal rings had the highest variety of agents used for extrication n = 16, but the silk method accounted for the most common method in for extrication of this agent. All metal hoops reported in the surveyed literature were removed by saw (n = 6).
There was a significant age difference between groups when stratified by strangulation agents (Figure 4). Metal rings displayed the greatest presenting age range (range: 10–74, median 47.5). Threads were limited to the pediatric population (range: 4–13, median 7.5).
Presentation Age Grouped by Strangulation Sequelae
There was also a significant age difference between groups when stratified by reason for strangulation (Figure 5). Sexual activity showed the widest presenting age range (range: 14–77, median 48.0). Incontinence was prevalent in the senior population (range: 65–86, median 72.5). Curiosity (range: 7–10, median 8.5) and incidental reasons (range: 4–13, median 8.0) were limited to the pediatric population.

Presentation Age Grouped by Reported Follow-Up
There was no statistically significant difference between age groups when stratified by sequelae (Figure 6) or follow-up (Figure 7).

Cases

Presentation age at time of strangulation grouped by reported follow-up
For cases reporting follow-up outcomes, the most common sequela was the need for skin grafting 25% (6/24) followed by need for urethroplasty 21% (5/24) (Figure 6). Seventy- six cases did not include information about long-term side effects or complications (Table 1).
Discussion
In the earliest publication on this condition, Gauthier noted that after extrication, he soaked the patient’s testicles in a saline solution and applied benzoin ointment (Gauthier, 1755). Afterwards his patient was allegedly cured in “one month and several days.” Although the initial presentation seemed to be alleviated, Gauthier and many authors following him, did not report objective follow-up assessments which might have revealed delayed or long-term effects. Our results show that sequelae were reported in 24% of patients who presented with strangulation injuries. Additional sequelae may be under-represented because objective follow-up data, such as evaluation of voiding with the American Urological Association Symptom Score (AUASS) questionnaires, postvoid residual, or uroflow studies, and evaluation of sexual function, were not uniformly reported. We would recommend follow-up visits to discuss surveillance with consideration of postvoid residual urine (PVR) measurement, uroflow studies, and cystoscopy as suspicion dictates.
It was noted that follow-up was not limited to a particular age group. The larger Koifman et al. (2019) and Li et al. (2013) studies were excluded from this stratification as they reported patients based on mean age without individual patient data points (Koifman et al., 2019; Li et al., 2013).
The majority of patients followed longer than 2 years 75% (3/4) were in the pediatric population. This finding may be provider dependent; specifically, if these patients are followed in pediatric urology clinics compared to adult urology clinics where follow-up may be more patient driven than provider driven.
When grouped into broader categories, we found that threads were the most common strangulation agents in the pediatric population with a mean age of 7.5 years. The mean age of metal ring placement was 44.2 years, and the majority of these were attributable to sexual activity 91% (31/34) and ranged from the teenage to senior population (>65 years). Strangulation agent placement performed incidentally or by curiosity were limited to the pediatric population. Strangulation agent placement for incontinence was limited to the senior population.
The depth of reporting and implied significance of individual sequalae was variable throughout the literature. Several reports listed patient symptoms present without individualizing the data. This posed a challenge when trying to draw correlations since multiple symptoms could be attributed to single patients while others remained without morbidity. In addition, several large case series had discrepancies in the number of extricating agents and strangulation agents, calling the validity of the results into question. Ultimately, we chose to report sequelae by interventions performed as this was the most uniform and objectively quantifiable method to characterize the data throughout all reported results. In addition, these reported sequelae highlight findings that were bothersome or morbid enough to warrant patient or provider intervention.
It is indeed possible that many of these patients lack long-term sequelae and our critique might not be applicable to these case presentations whose main focus is to add to the urologist’s armamentarium for intervention in a urological emergency. These emergencies are sparse enough that it would be even more rare to find a urologist with an extensive case log totaling more than a few cases. We speculate the actual prevalence of penile strangulation injuries is unknown, in part due to the rarity of the presentation and that prior to the emergence of ICD-10 S30.842A code for penile constriction in 2016; the ICD-9 code 607.89 which encompassed strangulation, also included “sebaceous cyst,” “fistula,” and “hemorrhage” of the penis among others. In addition, some patients can remove these agents after multiple attempts at home.
Prevention
Metal rings were the most commonly presenting strangulation agent, and the most common reason for placement was attributable to sexual interest. Agents reported as “metal rings” accounted for 38% (19/50) of sexually placed strangulation agents and up to 62% (31/50) when combined with the addition of all types of metal rings. The reported data do not specify whether or not the intended uses of grouped rings were for sexual activity. However, given these findings, we would encourage providers to present penile strangulation as a possible complication of metal ring erection devices and to consider informing patients of other alternatives such as elastic bands, though all constriction bands should be used with caution and removed within a reasonable timeframe.
Any agent that leads to constriction of the penis should be expeditiously extricated as unrecognized complications may lead to sepsis and death as reported in at least four cases. Penile constriction by hair tourniquets may not be immediately evident on exam and should be on the provider’s differential diagnosis, especially in pediatric patients presenting with penile edema, as this may be a red flag for potential child abuse.
Limitations
Our search criteria may not have included all available data because subtle changes in word choice such as “constricting device” from “constriction device” may limit the number of return articles.
Many outcome pathways that were described, such as “urethroplasty,” have no additional information provided. Was the outcome the result of urethral stricture or urethral erosion? How long after the strangulation was the stricture noted? Timeframes such as time from strangulation placement to extrication and exact dates of follow-up were often reported as vague ranges. In multiple reports, demographic data such as age were presented as a range, precluding the ability for a more in-depth analysis. These questions in turn point to the necessity of better documentation and reporting to characterize outcomes of these strangulation injuries.
In addition, terminology is not conserved among the reported cases examined. This precluded granular accuracy in identifying strangulation agents, extrication agents, and similarly descriptive categories. Thus, an effort was made to maintain the original reported terminology to avoid inappropriate regrouping. Reported strangulation and extrication agents were left as initially reported to not cause bias into the nuance between the agents as either understood by the original reporters or with the current investigators. The strangulation agents were then consolidated into associative groups to evaluate for any meaningful correlations as seen in Figure 2. The grouping may reflect improper consolidation based on this study’s authors understanding of the reported strangulation agents. This may have led to an inherent lack of consolidation of what may indeed be similar agents by different reported names.
Conclusion
Penile strangulation is a urologic emergency requiring emergent extrication. Our review highlights the array of resources urologists may employ as interventions when confronted with such cases. Although there are many case studies and case series detailing extrication of the foreign object as well as reason for strangulation, there lacks a standardized protocol for assessment of the injury, data on long-term outcomes, and standardized treatment stages after removal of the offending agent. Adding a standardized protocol for long-term care based on the severity of the injury (edema vs. sepsis), strangulation agent (metal ring vs. hair tourniquet), or required interventions (urethroplasty vs. amputation) may aid in further expanding the tools available to urologists faced with this emergency. This review describes the differences in follow-up care and the need for more literature regarding this topic. Future studies should seek to detail secondary management protocols in these patients. Reporting on the long-term outcomes after removal of strangulating agents is necessary to better understand the natural history of these injuries so that follow-up protocols can be developed to monitor for complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.