
Abstract
Despite recent emphasis on couples-based HIV prevention interventions, efficacious interventions for Latino male couples have yet to be tested. The study examined the feasibility and acceptability of the Connecting Latinos en Pareja (CLP) intervention, a couples-based HIV prevention intervention for Latino male couples. This pilot demonstrated high feasibility, meeting targets for recruitment, retention, and intervention completion. We recruited a diverse cohort of 46 individuals/23 couples with a retention rate of 80% over 6 months and a 100% intervention completion rate in both conditions (four structured couple sessions in each condition). This pilot RCT was not powered to detect significant intervention impact on the primary outcome; however, there was a significant increase in relationship functioning among couples in the intervention group relative to controls and promising trends in changes in several key outcome and mediating variables. Secondary analysis documented trends in the expected directions for several other key hypothesized mechanisms of action (stimulant use, psychological symptoms, quality of life) as well as the primary outcome of proportion of protected sex acts (overall and broken out by main vs. outside partners). Qualitative exit interviews revealed high levels of acceptability of the CLP intervention. Participants highlighted affective component of the intervention and perceived effectiveness in improving dyadic communication skills and safer sex practices. Our findings show that a pilot trial of CLP is highly feasible and acceptable, with CLP demonstrating promising evidence of changes in key intervention mechanisms.
Introduction
Since early in the HIV epidemic, Latinos, particularly sexual and gender minority Latinos, have been impacted disproportionally. A study conducted in 2020 revealed an urgent national emergency as “The Invisible US Hispanic/Latino HIV Crisis” (Guilamo-Ramos et al., 2020). While the number of new cases decreased slightly from 9,000 in 2010 to 8,900 in 2019 for gay and bisexual Black men and gay and bisexual White men experienced a decrease in rates of new HIV cases from 7,500 in 2010 to 5,100 in 2019, HIV infection rates in gay and bisexual Latino men increased from 6,800 new cases in 2010 to 7,900 new cases in 2019 (Centers for Disease Control and Prevention, 2021). Increase is notable even when taking into account increases in the overall Latino population in the United States over the same time period.
Social and structural conditions continue to drive HIV cases among Latino men who have sex with men (LMSM). Discrimination, structural stigma, social isolation, migration experiences, and cultural factors contribute to an elevated risk for many LMSM (Andriano et al., 2022; Hoebbel & Fals-Stewart, 2003; Rodriguez-Diaz et al., 2021; Shorrock et al., 2022; Stappenbeck et al., 2004; Watson et al., 2022). For instance, “machismo” norms prescribe that men must avoid feminine behaviors (e.g., being penetrated), be perceived as powerful and prove their manhood by having multiple partners and unprotected sex (Noyola et al., 2020; Rhodes et al., 2009; Robles et al., 2022; Royster et al., 2006). LMSM may feel further compelled to engage in risk behaviors to compensate for real or perceived negative perceptions about their sexual orientation as well as internalized heterosexism (Rhodes et al., 2006; Sandfort et al., 2007). For many, the stress of not having legal U.S. residency status, the challenges of navigating different cultural contexts (mainstream U.S. culture, White gay community culture, Hispanic culture) and the loneliness, isolation, and depression that arise through concealing their sexual identity and being estranged from their families can lead LMSM to have unprotected sex as a source of comfort and relief (Diaz & Ayala, 1999; Shedlin et al., 2005). Directing HIV prevention efforts to LMSM is critical.
There is strong evidence from White male couples that HIV infection often occurs within primary relationships (Mitchell et al., 2012; Starks et al., 2016). MSM are more likely to engage in condomless anal intercourse with primary partners than with outside partners (Frost et al., 2008; Jin et al., 2009). In our preliminary work with Latino male couples, we found that being in a couple was associated with a higher frequency of condomless anal sex as well as increased alcohol consumption (Martinez et al., 2017). Among those in relationships, 68% reported engaging in condomless anal sex acts in the past 3 months, and almost half (49%) reported having more than one partner in this period. The majority (58%) screened for high-risk alcohol consumption in the past month. Given the clear significance of couple relationships for HIV prevention and transmission, and that HIV risk within primary relationships is driven by factors unique to each couple, there is a pressing need for flexible, couple-based interventions that can be tailored to specific relationship characteristics/dynamics.
There is a growing body of research supporting the effectiveness and escalating promise of couple-based approaches for HIV prevention and care (Darbes et al., 2019; El-Bassel, Gilbert, et al., 2010; El-Bassel, Jemmott, & Landis, 2010; Hoebbel & Fals-Stewart, 2003; Jiwatram-Negrón & El-Bassel, 2014; Newcomb et al., 2017; Robert et al., 2005). Intervening with the couple offers many advantages over individual interventions, including engendering a sense of mutual responsibility and support for the partners to remain healthy, using health promotion and risk reduction as strategies to strengthen a valuable relationship, building the couple’s communication and problem-solving skills, strengthening sexual agreements within the dyad and partners, and helping them to set and achieve goals that promote health and reduce risk (Wu et al., 2010, 2011). Couple-level interventions have the potential for lasting impact, as partners adopt elements of the intervention that continue to be implemented after the formal intervention has ended. Furthermore, the impact can extend to future relationships, as individuals implement skills and strategies with new partners. In addition to the exemplar completed and published couple-based HIV-related intervention studies referenced above, there are a number of HIV-related couples interventions being implemented, including for male couples in the United States (Kim et al., 2021; Newcomb et al., 2022; Starks et al., 2021), sexual and gender minority couples in the United States (Tabrisky et al., 2021), young heterosexual couples in the United States (Trent et al., 2022), and several interventions at various stages of evaluation among heterosexual couples in South Africa (Clinicaltrials.gov: NCT03809364, NCT05231707, and NCT05310773), Malawi (Clinicaltrials.gov: NCT04906616), Mozambique (Clinicaltrials.gov: NCT03149237 and NCT04071470), Kenya (Kwena et al., 2021), Zambia (Clinicaltrials.gov: NCT04729413), and Kazakhstan (Clinicaltrials.gov: NCT03555396). None have centered the unique context facing Latino men and their same sex partners.
Although interventions for male couples exist (Frye et al., 2021; Mitchell, 2015; National Institutes of Health RePORT, 2015; Starks et al., 2022; Stephenson et al., 2011, 2021), none have been developed and evaluated within a Latino cultural context focused on the unique constellation of factors salient to Latino male couples. With the exception of a small number focused on Black/African American men (Clinicaltrials.gov: NCT01394900 and NCT04951544; Kim et al., 2021), dyadic interventions have sampled predominantly White, sexual minority men who reported high levels of education and employment; thus, the generalizability of these interventions to communities most disproportionately impacted by the epidemic is unknown (Gamarel et al., 2022).
Studies comparing culturally sensitive interventions to those that do not incorporate culture-specific components report that the former have greater efficacy (Scott D. Rhodes et al., 2015). Our own work and that of others indicate that there are distinct differences in the factors associated with HIV risk and protection among White, Black, and Latino sexual minority men [anonymized for peer review]. Because interventions must address psychosocial, cultural, relational, and contextual factors that impact people’s lives and mediate or moderate HIV risk behaviors to be maximally effective (Stall & Purcell, 2000), it is imperative that interventions are responsive to these differences. Yet, despite the promise of couples-based interventions, and the push to develop and test couple-based interventions for MSM more broadly, this approach has yet to be applied to Latino male couples. The formative work described in this paper and the planned follow-up research will address this substantial gap in the U.S. public health response to the shifting HIV epidemic.
In this article, we (a) describe the development and refinement of Connecting Latinos en Parejas (CLP), a couples-based biobehavioral intervention for Latino male couples and the subsequent pilot randomized controlled trial (RCT), (b) evaluate feasibility and acceptability of the intervention, and (c) explore trends in hypothesized mechanisms of action as an early indication of its potential efficacy leading into a fully powered RCT.
Methods
Phase 1: Intervention Refinement
Intervention Refinement
The CLP intervention was adapted from Connect n’ Unite, a couples-based HIV prevention intervention for Black male couples (Wu et al., 2010). Connect n’ Unite is a couples-based intervention targeting the intersection of stimulant use and sexual risk behavior among racial/ethnic and sexual minorities, with the ultimate goal providing an evidence-based intervention that can be delivered in drug treatment and other service settings to reduce the spread of HIV among stimulant-using, African American/Black MSM.
Details on the adaptation process and results have been published elsewhere [anonymized for peer review]. Briefly, there were five steps: (a) engaging community stakeholders (e.g., sexual minority Latino men living with HIV, providers in Latino AIDS service organizations), (b) capturing the lived experiences of Latino gay couples, (c) identifying intervention priorities, (d) integrating the original intervention’s social cognitive theory into a relationship-oriented, ecological framework for Latino gay couples, and (e) adapting intervention activities and materials. The end product was a manualized intervention called CLP in English and Spanish. The initial adaptation study highlighted three findings of significance to the feasibility and acceptability trial. First, the men screened as well as those enrolled reported high rates of condomless acts of anal intercourse, concurrent sexual partnerships, and substance use. In the past 3 months, 72% screened for problematic alcohol consumption and 42% used club drugs. Thirty-four percent were HIV-positive. Second, in less than 1 month, we recruited 20 Latino male couples indicating that our projected enrollment target is feasible and realistic. Third, Latino male couples highly endorsed the intervention; during the exit interviews, they stated that it was culturally relevant, timely, and filled a void in prevention efforts. In addition to echoing this sentiment, providers spoke to the feasibility of implementing CLP in community agencies and future scale-up potential if our results indicate that CLP is efficacious.
Theoretical Framework of CLP
Both Connect ‘n Unite and CLP are grounded in Social Cognitive Theory (SCT) and a relationship-oriented ecological framework [anonymized for peer review]. Like Connect ‘n Unite’s application of SCT,(Wu et al., 2010) CLP’s activities are designed to (a) provide information and knowledge to promote accurate risk appraisal; (b) build social and self-regulatory skills through problem-solving, role-plays, and other cognitive behavioral strategies; (c) increase self-efficacy to engage in HIV protected sex and reduce risk behaviors; (d) increase positive outcome expectancies regarding HIV protection strategies; and (e) build and sustain social support networks for practicing HIV protected sex. These activities are grounded in the unique cultural context for Latino male couples, as described previously.
The relationship-oriented ecological perspective refines SCT constructs and incorporates contextual, multilevel dynamics that influence risk among intimate partners. The ontogenetic level focuses on each partner’s developmental history and personal attributes (e.g., childhood sexual abuse) and SCT constructs (e.g., PrEP use outcome expectancies). CLP prompts participants to examine how their past experiences influence their current sexual practices and intimate relationships. The microsystem consists of interactional and structural factors that are part of the immediate intimate relationship context in which the couple’s sexual activity and risk/protective behaviors occur. CLP’s activities target communication and negotiation skills related to sexual risk behaviors, protection, and pleasure as well as sexual decision-making power and control. CLP also addresses how the use of alcohol and other substances impairs cognition, which may undermine negotiation and mutual decision-making. The exolevel refers to external factors impinging on the immediate setting by acting as stressors or buffers on the likelihood of engaging in particular behaviors. CLP aims to strengthen social support and peer norms for having HIV protected sex and use of alcohol and/or other drugs in sexual contexts. The macrosystem encompasses broad cultural values and belief systems (i.e., the “man” is the penetrator, if you disclose your sexuality or HIV status your family will reject you) and stereotypes of Latino men (i.e., hot, desirable lovers; sex objects in the sexual marketplace). CLP prompts participants to examine how these cultural values, beliefs, and stereotypes influence the couples’ sexual practices. It helps to build internal resources and external social support networks to reverse the objectification, rejection, and/or disfranchisement that have been linked to HIV risk behaviors (Roque Ramírez, 2007). We provide a summary of the sessions in the next section. Figure 1 shows moderators, mediators, and outcomes.

Moderators, Mediators, and Outcomes
Pre-Piloting
We engaged six Latino male couples in an initial refinement process of the intervention, in which all partners were at least 18 years old and at least one identified as Latino. Couples were engaged in collaboration with a local Latino AIDS service organization. Flyers were distributed with information about the intervention and how key informants could help inform the refinement of the intervention. The four sessions were presented to the six couples followed by a reflection and feedback consultation.
During each session, the interventionists presented drafts of the intervention modules, including activities and exercises, and requested feedback regarding module content, design, accessibility, interactivity, and delivery. Changes resulting from this feedback process were presented to a Community Advisory Board and further evaluated by the core research team.
Following the development work, including the adaptation and pre-piloting described above, the pilot intervention protocol was finalized.
CLP
CLP consists of four sessions whose content, scenarios, and examples can be adapted to each couple’s unique circumstances and relative HIV statuses. It incorporates behavioral risk reduction (e.g., condom use), biomedical prevention methods such as pre-exposure prophylaxes (PrEP); promotes engagement in care, adherence to treatment regimens and viral suppression; and encourages routine HIV testing as indicated by each partner’s serostatus. In delivering the core conceptual components, the interventionist tailor the content to reflect the couples’ life situation using their own words, concerns, and priorities; also, activities and accompanying materials were designed to accommodate each couple’s unique circumstances and relative HIV statuses (e.g., couples’ mixed immigration status and how it impacts access to comprehensive care, HIV status-neutral approaches designed to address HIV prevention and care needs among seroconcordant [positive and negative] and serodiscordant couples).
Session 1 focuses on the personal, cultural, and contextual factors that influence risk and protection among couples. Through exercises and activities, couples examine how cultural values (e.g., machismo), relationship dynamics and context, substance use (e.g., alcohol consumption, heroin, street fentanyl, other illicit opioids), and social and structural factors (e.g., immigration status, discrimination), impact sexual risks and health behaviors. In addition to providing basic information about HIV/AIDS, STIs, and substance use, couples are introduced to problem-solving, the concept of couple self-care and new prevention methods stressing those most relevant given a couple’s HIV status. The session ends with an assignment designed to enhance personal and couple-oriented self-care. See Figure 2 with the Who’s in Mi Casa activity designed for the dyad to identify individual and social/structural conditions influencing risk. Session 2 consists of developing effective communication and goal setting skills, developing couple sexual health plans, and increasing the couple’s motivation to use different prevention technologies. Using examples relevant to the couple, the interventionist uses problem-solving to help the couple evaluate different prevention approaches and determine the most appropriate ones for the couple to incorporate into their risk reduction plan. As part of their homework assignment, they are encouraged to practice using at least one option from the problem-solving exercise in the subsequent week. A key component of this session is a focus on communication using a structured framework (GIVE, Figure 3). Session 3 applies the problem-solving and communication skills to a focus on relationship strengthening, identifying and defining unwritten rules, exploring couples’ power and decision-making process, examining triggers to risky sex, and developing action plans. It includes skills-building role-plays for negotiating HIV protected sex and exploring different prevention alternatives. The homework assignment involves understanding the couple’s own triggers around risky sex, developing alternatives, and coming up with a couple-oriented relationship strengthening plan that includes safe and fun sex. In Session 4, couples identify social support networks and resources within and outside the Latino community that could help them sustain their goals. Couples also review and refine their plans for engaging in HIV protected sex and in the HIV prevention and care continuum, including continued HIV testing within the dyad as relevant and with outside partners. Couples learn strategies for dealing with “slips” and review key skills developed during the sessions. The session concludes with a “graduation ceremony” during which couples make a commitment to follow their plan.
Who’s in Mi Casa? Activity

Role-Play
Wellness Promotion
The Wellness Promotion (WP) attention control condition was previously adapted to a Latino cultural context and served as the time and attention matched comparison condition in the feasibility and acceptability RCT previously described. WP comprises four sessions and focuses on nutrition, fitness, health care, health and internet literacy, including assessing the quality of information/sites on the web and the dangers of misinformation, and stress management and emphasizes adherence to medical regimens and medication management. It is informational, less interactive than CLP, and does not include problem-solving, communication exercises, or the development of sexual protection plans. It does, however, include basic information regarding HIV/STI prevention, including information and referral for PrEP, HIV testing recommendations, as well as engagement in care and the importance of treatment adherence for HIV+ participants. CLP and WP have the same number of sessions and time allocated for each session, making the WP an ideal time and attention matched control for CLP.
Phase 2: Pilot Feasibility and Acceptability Study
Design
We conducted a feasibility and acceptability pilot RCT of CLP compared with a time and attention matched Wellness Promotion (WP) control intervention (1:1 couple-level randomization). For this pilot RCT, we did not set out to conduct outcome analyzes to determine an effect size. This decision was guided by the literature (Arain et al., 2010; Becker, 2008; Eldridge et al., 2016; Kistin & Silverstein, 2015; Kraemer et al., 2006; Lancaster, 2015; Lancaster et al., 2004; Leon et al., 2011; Thabane et al., 2010, 2016) and the NIH (National Center for Complementary and Integrative Health [NCCIH], 2017) highlighting the inherent instability of effect size estimates derived from small pilot studies and reinforcing the value of pilot RCTs in establishing feasibility and acceptability and for informing operational refinement in study protocols (Eldridge et al., 2016).
Sample Size
As the primary aim of this pilot study was to assess feasibility and acceptability of the research protocol for a future clinical trial, the sample size of N = 20 couples/40 individuals (10 couples/20 individuals in each condition) was set primarily for practical reasons and not driven by hypothesis testing or estimating precision of effect size estimates. The target sample of 20 couples was set to provide a sufficiently large number of couples to obtain reasonable descriptive estimates and to enable us to test our data collection instruments and procedures and recruitment methods with a sufficiently large sample supplying a variety of responses as well as to obtain a rich set of qualitative exit interview data.
Inclusion and Exclusion Criteria
Participants were included if they (a) reported being at least 18 years; (b) resided in the Philadelphia Metropolitan Area; (c) identified as Latinx/Hispanic/Afro-Latino or reported having a main partner who identifies as Latino/Hispanic/Afro-Latino; (d) reported having a main/primary male partner operationalized as a man with whom he has a primary ongoing sexual relationship, for at least 3 months; (e) at least one member of the dyad reported three acts of unprotected of anal sex (with main or other partners); and (f) able to speak English and/or Spanish. Unprotected anal sex was defined as reporting condomless anal sex in the absence of reporting adherence to PrEP (for HIV-negative MSM) or full adherence to ART (for HIV-positive MSM) as measured using a validated adherence rating scale (Lu et al., 2008) and the 3-item adherence assessment developed and validated by Wilson et al. (2016). Participants were excluded if they (a) reported severe intimate partner violence (IPV) within the dyad during the past year on the Revised Conflict Tactic Scale (Greenwood et al., 2002; Tjaden et al., 1999; Waldner-Haugrud et al., 1997; Waterman et al., 1989) or (b) had a language or cognitive impairment that could prevent informed consent.
Recruitment
We implemented a multipronged recruitment strategy to identify, recruit and enroll Latino male couples. First, based from our work with Latino male couples, four factors were considered when developing recruitment materials: (a) racial, gender, and relationship inclusivity (including nonmonogamous couples); (b) language considerations; (c) visual appeal; and (d) responsiveness to social and contextual factors. Our previous work highlights the importance of using simple, direct, and concise messages; reinforcing gain frames (“increasing safety”) rather than loss frame (“reducing HIV risk”); and being aware of how societal portrayals of sexual minority Latino men, including the hypersexualization of Latino men, contributes to further stigmatization and marginalization of this group. Second, we established a robust online recruitment strategy to recruit study participants (e.g., social networking apps including Grindr, Jack’d and Scruff; Facebook, Twitter, and Instagram accounts). In particular, we identified convenient days, times, and locations to post on social networking apps. We have found these strategies have yielded successful recruitment of Latinos in Grindr (e.g., posting Grindr adds between 6 p.m. and 10 p.m. in predominantly Latino communities, to recruit sexual minority men). Third, we worked with Latino-serving organizations to post recruitment flyers and promote study. We sent letters to trusted community organizations with information about the study and highlighted significant given the disproportionate impact of HIV among sexual minority Latinos. Fourth, we emphasized study uniqueness in all of our recruitment and engagement strategies. In particular, we emphasized and shed light on the invisible HIV epidemic among Latinos and the opportunities to intervene within dyads. Fifth, we adapted to potential participants’ changing schedules and offer assistance to overcome challenges. Sixth, potential participants were not be pressured to enroll in the study. Recruiters did not focus exclusively on the study and their recruitment numbers. Instead, they shared local resources and made referrals based on participants’ needs (e.g., support related to immigration issues, mental health, or homelessness). This respectfulness and awareness of participants’ competing needs and priorities have helped build trust with Latino communities in our previous studies. Seventh, once dyads completed the intervention sessions, we gave them framed graduation certificates. See Figure 4 for an example of a recruitment flyer.

Recruitment Material
Intervention Procedures
Research Assistants (RAs) were crossed so that each one delivers both interventions. Crossing RAs controls for interventionist characteristics and strengthens internal validity. Nesting the RAs within conditions reduced the chance for bleeding (e.g., contamination) between conditions that could lead a type II error, but increased the likelihood of making the more serious type I error. We employed strict quality assurance procedures to minimize the potential for “bleeding” and will conduct fidelity evaluations to monitor adherence. We systematically assigned RAs to couples in the order in which they are enrolled in the study. We also ensured that the RA who served as the couple’s interventionist was different than the one who conducts the assessments.
The protocol called for couples to complete eight study visits during the 6-month study period. Intervention sessions were administered weekly, but we made reasonable adjustments to maximize participation. Intervention sessions were conducted at a local Latino AIDS service organization, at Temple University’s School of Social Work, and/or at couples’ preferred location (e.g., private room in local library). Assessments were scheduled ±1 week from their target dates. In our tracking database, we recorded the date in which each couple completed each study activity.
Self-administered REDCap assessments were conducted at baseline, 3 and 6 months and included demographic variables, HIV-specific information (e.g., HIV status, PreP, and HIV treatment history), sexual behaviors within and outside of the dyad, and validated scales for relationship functioning (Busby et al., 1995), psychological symptoms (Brief Symptom Inventory; Asner-Self et al., 2006) quality of life, alcohol and other substance use (Dawson et al., 2005; Group et al., 2016), and other domains as shown in Figure 1.
Randomization
We randomly assigned couples to the two conditions 1:1 following collection of all baseline data at the beginning of the second study visit, which is when they were scheduled to receive their first intervention session. This approach minimizes potential biases in treatment effect estimates due to differential attrition between randomization and the first session. It also ensures that all participants receive at least 1 intervention session. We used randomized permuted blocks with randomly varying block lengths to assign couples to CLP or WP with equal probability.
Tracking and Retention
We maintained regular contact with participants via e-mail, text, and phone throughout the study. We sent participants birthday, holiday or other special occasion cards to maintain relationships and collected comprehensive locator information that included the names, telephone and addresses of at least three persons we could contact in the event we could not find the participants. Other approaches to promote retention included a graduated incentive payment structure and the provision of study-branded swag at key timepoints during the study (e.g., tote bags, water bottles, and keychains).
Ethical Considerations
We secured approval from [anonymized for peer review]. All participants provided written informed consent prior to enrolment in the study. No study-related serious adverse events were detected. Several procedures were implemented to minimize risk:
All study staff went through a comprehensive training that included the impetus, goals, organization, and rules/regulations under which the study operates; this training also covered: (a) ethical issues in research; (b) establishing and maintaining rapport with participants; (c) obtaining informed consent; (d) addressing participants‘ concerns with confidentiality and handling sensitive situations; (e) obtaining accurate tracking information; (f) managing distress and conducting crisis and enhanced referrals; and (g) detecting, handling, and reporting adverse events. This common, general training was supplemented with more specialized topics and scenarios during trainings dedicated to specific roles/tasks (e.g., Research Assistants and Project Coordinator) as appropriate.
A Certificate of Confidentiality issued by the federal government was obtained for this study.
All data were de-identified with alphanumeric codes (each individual and couple was assigned a code).
Research assistants were trained to help participants address feelings of discomfort. A comprehensive referral list was provided to those who report emotional distress and/or severe violence. In addition, those who screened positive for HIV or those who are HIV-positive but not in care were linked to HIV care coordination services. We assisted participants in making contact with service providers.
All participants were informed that they did not need to answer questions if they felt uncomfortable doing so during the sessions.
Community Advisory Board
A community advisory board guided all stages of the research process. Community advisory board members included sexual minority Latino men and representatives from local organizations serving sexual minority Latino men. CAB members engaged in conversations and deliberative dialogues, which are undergirded by principles of social justice, local relevance, mutual benefit, and long-term commitment to the community. Deliberative methods seek to obtain rich community insight into health disparities and inequities, allow sharing community-informed solutions, recognize the expertise of each participant, and give underrepresented communities influence over decision-making to guide health equity goals. Deliberations will encompass five key elements: (a) coming together; (b) sharing information; (c) discussing; (d) documenting; and (e) action. CAB contributed to the development of recruitment materials and assessments, and provided recommendations for sustainability and continued engagement of sexual minority Latino men.
Measures
Feasibility
We have relied on our team’s prior experience with pilot and full scale RCTs and guidance from the NIH on appropriate feasibility measures (NCCIH, 2017). Feasibility metrics included details of the success of procedures for recruitment, retention, data completeness, and intervention completion. These metrics, along with acceptability data, were used to guide the procession to a full-scale RCT.
Acceptability
Assessment of acceptability was guided by work by Sekhon and colleagues (Sekhon et al., 2017, 2022). In this Theoretical Framework of Acceptability, acceptability to health care interventions comprises seven components: affective attitude, burden, intervention coherence, ethicality, opportunity costs, perceived effectiveness, and self-efficacy. These domains were assessed primarily though qualitative exit interviews following completion of the pilot study activities.
Behavioral Outcomes and Hypothesized Intervention Mediators/Mechanisms of Action
The ultimate primary outcome for a subsequent planned efficacy trial will be proportion of HIV-protected anal sex acts. Proportion of HIV-protected anal sex acts was assessed using a comprehensive risk behavior assessment that is adapted to the couple’s serostatus and use of prevention tools. The algorithm incorporates three types of protective behaviors: (a) condom use, (b) PrEP utilization and adherence for those who are HIV-negative, and (c) viral suppression and antiretroviral treatment adherence for those who are HIV-positive (i.e., treatment as prevention). We examined proportion of protected sex acts with all partners and separated by main versus non-main partners.
For intervention mediators, we examined available data mapping onto key intervention mechanisms, including relationship functioning (Keown-Belous, 2013), mental health (Derogatis et al., 2018), substance use, and perceived overall health/quality of life (Hanefeld et al., 2017). The relationship functioning scale was designed to assess relationship satisfaction and social support in same gender relationships and was hypothesized one a key mechanism of change of the CLP intervention (Keown-Belous, 2013). Mental health was assessed through the Brief Symptom Inventory-18. Participant selected the option that best describes how much they were distressed within the past 7 days by the following including nervousness or shakiness inside, feeling so restless they couldn’t sit still, and feeling fearful. Substance use was assessed by sequentially asking participants to report whether during the prior 3 months they used methamphetamine, cocaine in various forms, heroin/other opiates, tranquilizers, other club drugs and stimulants, and non-prescribed erectile dysfunction drugs. Quality of health was assessed by asking How would you rate the overall quality of health? Participants were prompted to report the quality of health: poor, fair, good, very good or excellent.
Analysis
We used an intention-to-treat (ITT) design. The primary study endpoint was 6-month follow-up. The two-sided Type I error rate for the primary outcome (proportion HIV protected anal sex acts with main partner) was be set at è =.05. Initial data analysis tasks involved univariate and bivariate statistics to characterize the sample and review the distributional properties of measures across treatment arms; for continuous variables, we calculated means, standard deviations and ranges, and examined boxplots for outliers. For categorical variables, we looked at frequency tables and examine bivariate relationships between dependent and independent variables. The distribution of variables for the two conditions was compared using parallel boxplots for continuous variables and mosaic plots for categorical variables. We used random effect models and/or generalized estimating equations (GEE) modeling 6-month follow-up differences adjusting for characteristics at baseline, 3-months, and treatment arm to increase statistical precision. (Loeys & Molenberghs, 2013).
Results
Participants Characteristics
At baseline, participants’ average age was 32 (range 20–57), 83% (n = 38) born in the United States, 22% (n = 10) with high school diploma/GED or lower education, 50% (n = 23) with yearly income less than US$30K, 15% (n = 7) with experience of homelessness in the past 90 days. Over one-fifth (22%, n = 10) reported living with HIV. Among HIV-negative participants (n = 35), only 14% (n = 5) had taken PrEP in 90 days prior to baseline assessment. See Table 1 with participant characteristics.
Participant Characteristics for Pilot Study (N = 46)

Note. Percent of protected sex = # of protected sex (i.e., condom use from start to finish for column A; taking PrEP & using condom or taking PrEP but not using condom or using condom but not taking PrEP for column B)/total # of anal sex. PrEP = pre-exposure prophylaxes; GED = General Education Development; ART =Antiretroviral therapy.
Participants were HIV-negative and NEVER taken PrEP, HIV non-positive (not tested, unknown, no results, or refused to answer) or HIV-positive. b Participants were HIV-negative and taking PrEP. c Use PrEP, always used condoms, or virally suppressed.
Outcomes
Feasibility
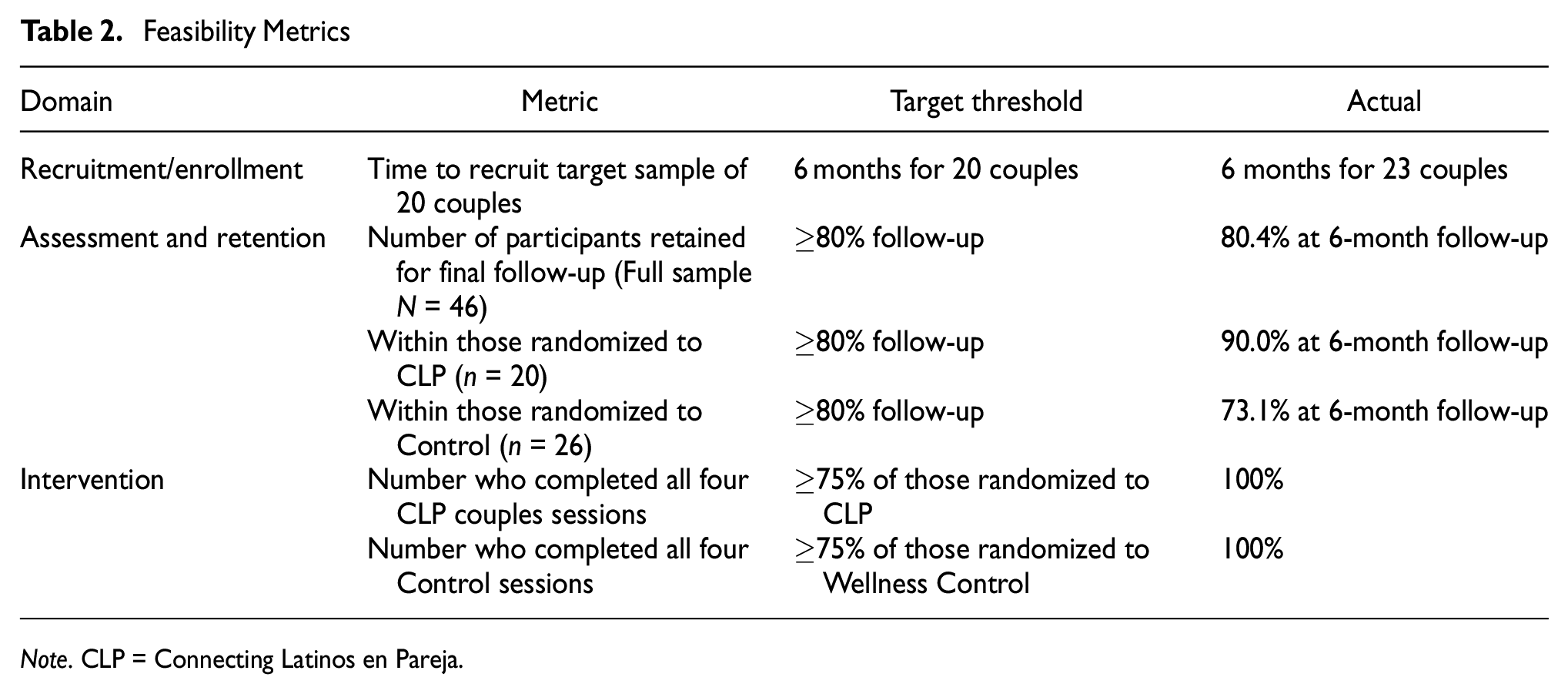
As detailed in Table 2, we achieved satisfactory indicators of feasibility across the domains of recruitment/enrollment, assessment/retention, and intervention completion. Although there was an overall satisfactory retention rate of 80.4% at final follow-up, the level was lower (73.1%) for those randomized to the control intervention. In response, we have modified our retention plan for the planned subsequent trial to include greater contact between visits and an escalating incentive structure that will be finalized with input from our community advisory board for the future randomized controlled trial.
Feasibility Metrics
Note. CLP = Connecting Latinos en Pareja.
Acceptability
Participants indicated a high level of acceptability following completion of the CLP intervention. The 100% intervention completion rates across both randomization arms suggest both feasibility and acceptability. Below, we provide exemplar quotes from the exit interview that map onto domains of acceptability.
Affective Attitude
This intervention has made me think more so about my partner’s feelings, outlook, and needs overall. I value him so much more since the start of this study. I no longer second guess what I feel or why I feel.
Burden
There were no indications of excessive burden from the exit interviews. However, the study team noted challenges with scheduling in-person sessions with couples, which has informed the plan for future sessions to be conducted virtually via video conferencing platforms.
Intervention Coherence
It helped me understand more about HIV and the preventatives to catching HIV and how it spread and what medications there are involved with that. It has helped me to be more open in communication with my partner, and in my life. It definitely has strengthen my relationship. Sin embargo cuando considero que tengo una relacion que funciona, emocional y comunicacionalmente. Nos ha funcionado de manera positiva toda la informacion que nos dieron. Hemos podido monitoriar nuestros objetivos para cumplir nuestras metas con las herramientas que nos dieron. Incluso hemos cambiado algunos objetivos los cuales hemos considerado que es la mejor opcion. Sin duda, cada una de las citas que tuvimos con los chicos de connecting latinos, las hemos aprovechado al maximo.
Ethicality
There were no adverse events documented as part of the study, and no ethical concerns presented by participants during the exit interviews.
Opportunity Costs
There were no indications of important things that were necessary to give up to participate and benefit from the intervention.
Perceived Effectiveness
There were many quotes that were coded as supporting perceived effectiveness of the intervention: Helped me be safer in my sexual life and practice as well as protect those around me. Very helpful in terms of allowing my husband and I to have an open and honest dialogue about all of our options regarding safe and sometimes unsafe sexual practices. In addition, it allowed us the opportunity to realize just how much we really know and understand one another. We learned how to listen and communicate better. I learned to not get offended so quickly, I learned how to calm down and breathe. The reason I know about prep is because of what I learned here.
Self-Efficacy
I implement some of the strategies and skills I have learned in my daily activities. We have been using the communication skills that we worked on during the session and particularly in how to better set and achieve our goals together. The information, strategies, and skills from this intervention have helped me to maintain focus on goals, both set during the intervention and after. My life has moved forward in positive ways.
Furthermore, several participants commented on the importance of relationship function. One noted “This program was extremely helpful in building and strengthening relationships.” Another participant expanded, “Connecting Latinos en Pareja has been an eye opener for not only sex and health education, but for the many ways we can grow as a whole, in community or relationships.”
Quantitative Trends
We documented preliminary evidence of impact on key mediators, including overall quality of health, stimulant use, and mental health. Although not powered to detect differences in outcomes, there was a significant increase in relationship functioning among couples in the intervention group relative to controls. In addition, we documented trends in the expected directions for several other key hypothesized mechanisms of action (stimulant use, psychological symptoms, quality of life) as well as the primary outcome of proportion of protected sex acts (overall and broken out by main vs. outside partners). See Figure 5 with quantitative trends for primary outcome and Figure 6 with trends for other mediators of interest.

Protected Sex Acts for CLP Compared With WP Controls

Mechanism Trends for CLP Compared With WP Controls
Discussion
This pilot RCT showed high levels of feasibility and acceptability across a number of key domains including relationship functioning. Similar to other studies, relationship functioning and strengthening sexual agreements within the dyad and partners help achieve and promote health and HIV sexual risk reduction (Wu et al., 2010, 2011). In addition, there were encouraging qualitative and quantitative findings suggesting that the intervention is affecting hypothesized mechanisms of action.
The pilot experience has provided valuable insights for updating and refining the intervention, including the value of converting to a remote, video format for couples sessions, the need for biomarkers for outcome ascertainment, and the importance of updating the curriculum and assessment measures to capture changes in HIV prevention approaches, including long-acting injectable PrEP and HIV treatment, on-demand dosing for PrEP, and the forthcoming pipeline of longer-term formulations and implants for drug delivery. This work has highlighted the need for subsequent protocols for a full efficacy trial to be nimble to changes in prevention technologies and epidemiological data, shifts in recruitment strategies to reflect trends in the behavior of the target communities, all while being true to the underlying theory-informed and tested mechanisms of change on which the intervention is established.
Our study showed the importance and significance of engaging community stakeholders and the larger scientific community in the refinement and testing of the intervention. Community members were critical in providing community engagement and scientific guidance on methods (e.g., theory/methods, data analysis, recruitment, and engagement of study participants) and recommendations based on study findings.
Building from the findings of the pilot study, leveraging technology to remotely deliver CLP offers promise. New data have pointed to the geographic areas most likely to have impact on the HIV epidemic on Latino persons. The U.S. Ending the HIV Epidemic (EHE) Initiative have identified 50 local priority jurisdictions that accounted for 61% of new HIV diagnoses among Latinos in the United States in 2019. These priority jurisdictions receive funding to develop innovative, locally tailored plans that lay the foundation for scaling up the key strategies of the initiative in a way that will address meets unique local needs, and reduces health disparities, and achieves health equity in each community. However, there are 17 jurisdictions with most new HIV diagnoses among Latinos are not designated EHE priority jurisdictions. These hotspots include Westchester, NY, Nassau, NY, Passaic, NJ, Middlesex, NJ, Union, NJ, Osceola, FL, Cameron, TX, Hidalgo, TX, Galveston, TX, Denver, CO, Pinal, AZ, Pima, AZ, Kern, CA, Fresno, CA, Santa Clara, CA, and Contra Costa, CA (Guilamo-Ramos, 2021). Latinos account roughly one of the 10 new Latino HIV diagnoses nationally. Therefore, future interventions should consider technology and remotely delivered modalities to effectively reach and help fill critical gaps to address the HIV epidemic among sexual minority Latino men (Guilamo-Ramos, 2021).
There are limitations that should be considered that limit generalizability of the findings from this pilot RCT. First, dyads reporting use of on-demand PrEP and long-acting injectable PrEP or ART, in the absence of other risk behaviors, were excluded from the study. While we understand that there is scientific evidence that the “2-1-1” schedule provides effective protection for gay and bisexual men when having anal sex without a condom, it was not part of CDC’s guidelines for PrEP use. Second, we acknowledge that it is not feasible to collect adherence data on outside partners and we relied on self-report from enrolled participants of the HIV status, PrEP and ART use of their outside partners. Future studies should consider the inclusion of biomarkers for adherence. Finally, as previously noted, this pilot RCT was designed to primarily assess feasibility and acceptability and thus not sufficiently powered to detect statistical differences in outcomes. A future full-scale RCT is needed to rigorously evaluate the impact of the CLP intervention.
Overall, CLP has the potential for significant public health impact because it includes couples regardless of serostatus and incorporate PrEP and recommends routine HIV testing for HIV− men and promotes engagement in care, adherence to treatment regimens, and viral suppression for HIV+ men while still emphasizing the importance of condom use.
Conclusion
Sexual minority Latino men continue to be disproportionately impacted by the HIV epidemic. This study assessed the feasibility and acceptability of a couples-based HIV prevention intervention for Latino male couples. The pilot RCT was not powered to detect significant intervention impact on the primary outcome; however, there was a significant increase in relationship functioning among couples in the intervention group relative to controls and promising trends in changes in several key mediating variables. Qualitative exit interviews revealed high levels of acceptability of the CLP intervention. CLP, if efficacious in a full clinical trial, will help advance HIV prevention efforts among Latino men and fill critical knowledge gaps to guide the translation of evidence-based interventions into widespread adoption by community-based organizations and health departments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potentior publ/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention under a grant from the Minority HIV and AIDS Research Initiative (MARI) (1U01PS005124-02; PI: Martinez).