
Abstract
The main objectives of this cross-sectional study were to determine the relationship between socioeconomic status (SES) and depression and to estimate the mediating effects of social network satisfaction, self-esteem, and perceived health status among middle-aged and elderly men living alone, based on the reserve capacity model. Secondary data from a sample of 394 middle-aged and elderly men aged 45 years or older from the 15th Korea Welfare Panel Study (KOWEPS) were analyzed. A path analysis model was constructed to evaluate the relationship among SES, social network satisfaction, self-esteem, perceived health status, and depression. The path analysis exhibited significant direct effects of social network satisfaction, self-esteem, and perceived health status on depression and significant indirect effects of SES on depression. There was no direct effect of SES on depression. Social network satisfaction and self-esteem had significant mediating effects of SES on depression. Among middle-aged and elderly men, intrapersonal reserves, which are psychosocial factors including social network satisfaction, self-esteem, and perceived health status, showed more association with depression than tangible reserves such as SES. This suggests that interventions promoting self-esteem and perceived health status could prevent depression.
Due to the extent of nuclear families and transformed social environments, South Korea is ranked first among the Organisation for Economic Co-operation and Development countries in terms of the growth rate of single-person households. The percentage of single-person households in Korea dramatically increased from 15.7% in 1995 to 30.2% in 2019 (Statistics Korea, 2020). The percentage of older adults (aged 65 years or older) living alone also increased from 6.1% in 2010 to 7.5% in 2019 and is projected to keep rising (Statistics Korea, 2020). In particular, the number of middle-aged and elderly men (aged 45 years or older) among all single-person households is continuously on the rise, from approximately 1.19 million households in 2015 to 1.51 million households in 2019 (Statistics Korea, 2020). While the percentage of adult women, aged 45 years or older, among single-person households, dropped from 58.5% in 2015 to 57.0% in 2019, that of adult men, aged 45 years or older, increased from 41.5% in 2015 to 43.0% in 2019 (Statistics Korea, 2020).
Government statistics indicate that older adults account for a substantial proportion of single-person households in Korea, consequently causing “lonely death” (dying alone) to emerge as an important social issue (Kim, 2019). According to various studies, elderly men who lived alone demonstrated more severe loneliness, depression symptoms, suicidal ideation, and suicide attempts compared with their female counterparts (Joo et al., 2019; Kim, 2017; Ko & Lee, 2015). In addition to elderly men, middle-aged men who live alone have been highlighted as an at-risk group for lonely death (Park & Choi, 2020). Approximately 85% of estimated lonely death cases involve men, and 69.1% have been attributed to middle-aged single-person households, considered socioeconomically disadvantaged (Choi et al., 2019; Song, 2016). Although the vulnerable population is projected to expand if the susceptibility of middle-aged men living alone is not addressed before they become older adults, policy support for middle-aged and elderly men living alone is still lacking (Im & Park, 2018).
Depression is prevalent in all age groups, with the highest prevalence among older adults. However, the prevalence of depression among middle-aged men is continuously increasing (from 320,000 in 2018 to 350,000 in 2020), and depression in this population requires close social attention (Health Insurance Review & Assessment Service, 2020b).Several studies have reported that middle-aged and older single-person households demonstrate a lower socioeconomic status (SES), featuring lower education level and employment and income instability, compared with multiperson households; consequently, the rate of suspected depression is significantly higher in these populations compared with their counterparts in multiperson households (Lee, 2017). Approximately 39% of people who died were reported to have suffered from depression (Song et al., 2018). This corresponds with previous findings stating that gender, age, low education, low income, job instability, absence of a spouse, lack of social support system, physical health factors, mental health factors, and low self-esteem are some of the predictors of depression in single-person households (Jang & Kim, 2020).
A study that examined suicide in middle-aged and older adults, based on data from 15 European countries, reported that middle-aged and elderly men were less educated and were affected by more socioeconomic disparities related to occupation and income compared with their female counterparts (Lorant et al., 2018). Middle-aged and older adults with a low SES demonstrated higher suicide rates and were more vulnerable to mental disorders, such as depression, due to socioeconomic instability (Kessler et al., 2008; Lorant et al., 2018). In particular, middle-aged and elderly men living alone are considered socioeconomically vulnerable due to the risk of social isolation because of retirement or unemployment. Previous studies have reported that the percentage of economically inactive individuals, temporary workers, and manual laborers, such as day laborers, was higher among middle-aged and older adults living alone; consequently, this population had low stability of assets and low public and private pension subscription rates (Lee, 2017). Since middle-aged and older adults living alone are at an elevated risk for income, employment, and residential instability, this leads to a higher incidence of social isolation and mental health problems such as depression and suicide (Ettman et al., 2020; Kang & Lee, 2016; Petrovic et al., 2018). The fact that low SES predicts depression in middle-aged and elderly men has been documented extensively in the literature.
The reserve capacity model (RCM) is one of the most prominent theoretical frameworks for understanding the association between SES and health inequity (Gallo, 2009; Gallo & Matthews, 2003). The RCM suggests that people with a low SES experience more daily difficulties and stressors and have fewer resources to cope with these challenges compared with the middle or upper class (Gallo & Matthews, 2003). The RCM describes three types of reserve capacities: tangible reserves (e.g., money, transportation), intrapersonal reserves (e.g., self-esteem and optimism), and interpersonal reserves (e.g., social support and social networks). According to the RCM, people with low SES deplete such reserves more quickly, have limitations in replenishing these reserves for the future, and are subject to a high level of stress and negative emotions due to the lack of resources, ultimately deteriorating their overall mental and physical health. In essence, this model posits that reserve capacity factors, such as social networks and self-esteem, act as mediators in the relationship between SES and health (Gallo et al., 2005).
Several studies support the idea that SES, intrapersonal reserves, interpersonal reserves, and health are associated based on the RCM. Barger (2006) reported a positive relationship between education and social support and the independent effects of depression on subjective health ratings. Howarter and Bennett (2013) identified that optimism and symptoms of anxiety mediate the relationship between perceived discrimination and health-related quality of life among community-dwelling residents of Hispanic descent. A study on Chinese migrants revealed that subjective social status was positively associated with self-rated health and life satisfaction and that perceived stress significantly mediated this relationship (You et al., 2021). Gallo (2009) identified that low psychosocial resources, including perceptions of control and social support, can be factors that connect low SES with poor health.
Social isolation is a major risk factor for mental health problems such as depression (Noguchi et al., 2021). Middle-aged and elderly men living alone are particularly at risk of shrinking social networks as well as social isolation due to unemployment or retirement (Ko & Lee, 2015). A study that investigated middle-aged and older adults, who are at high risk of lonely death, reported that the level of loneliness and social isolation was higher among the low-income class, day laborers, nonpermanent workers, and individuals with poorer health (Song et al., 2018). The implementation of social distancing practices for preventing the spread of coronavirus has further escalated the risk of social isolation among the vulnerable class, increasing the likelihood of lonely death (Brooke & Jackson, 2020). It is to be noted that middle-aged and older adults with low SES who lived alone demonstrated less social isolation if they were satisfied with their social networks (Song et al., 2018); similarly, the level of depression decreased with increasing perceived social support (Tengku Mohd et al., 2019).
Alongside the abovementioned factors, self-esteem is another classic psychological predictor of depression (Song & Seong, 2021). Rosenberg (1965) defined self-esteem as a feeling of self-acceptance, self-respect, and worthiness, stating that people with high self-esteem are satisfied with their current selves. Studies report that maintaining an appropriate level of or improving self-esteem has positive effects on mental health, while low self-esteem exacerbates depression (Song & Seong, 2021).
Perceived health status is the comprehensive rating of one’s own physical, physiological, psychological, and social status, and represents an individual’s opinion about their health that cannot be medically measured (Kwon & Kim, 2016). Perceived health status is a useful parameter for understanding individuals’ health, and positively perceiving one’s health has been reported to improve mental health (Ko & Lee, 2015). Studies have consistently reported that individuals who rate themselves to be in poor health are more likely to be depressed than those who rate themselves to be in good health (Ko & Lee, 2015), highlighting the fact that perceived health status is an important component in evaluating depression.
Most studies on depression in single-person households have been conducted on older adults, with limited research on male single-person households, including middle-aged men, who are known to be at high risk of lonely death (Lee & Yoon, 2018). Limited studies have examined depression in middle-aged and elderly men living alone in Korea, based on the RCM. Because SES influences health via a number of paths, various mediators must be examined in addition to SES (Gallo & Matthews, 2003).
The main objectives of this study were to determine the relationship between SES and depression and to examine the mediating effects of social network satisfaction, self-esteem, and perceived health status among middle-aged and elderly men living alone, based on the RCM. We hypothesized that SES would be associated with depression and that social network satisfaction, self-esteem, and perceived health status would have mediating effects of SES on the study population (Figure 1).

Conceptual Framework of the Study Based on the Reserve Capacity Model
Methods
Study Design
This cross-sectional study developed and analyzed a path model for depression and its associated factors among community-dwelling middle-aged and elderly men living alone based on empirical data collected by Korea Welfare Panel Study (KOWEPS).
Participants
The researcher collected data from the 2020 outcomes of the 15th KOWEPS, which is a nationwide annual study (Korea Institute for Health and Social Affairs, 2021). The KOWEPS is a nationally representative survey that initially enrolled 7,072 households, 6,029 of which completed the 15th survey in 2020. In this study, the raw data of the most recent survey, the 15th KOWEPS conducted in 2020, were downloaded, from which only data of male single-person households were extracted. Age was calculated using the year of data collection and birth year, after which only those aged 45 years or older were selected. Considering these three criteria (single-person household, male, 45 years or older), the total sample consisted of 403 participants. After excluding nine participants with missing values in any of the independent, mediating, and dependent variables to be used in the study model, 394 participants were finally selected for the study.
In general, the sample size required for the path analysis model is at least 150, and approximately 10 to 20 times the number of observed variables is recommended (Mitchell, 2001; Woo, 2012). In this study, there were six observed variables, which require a minimum sample size of 120. Therefore, the sample size of 394 met the minimum requirement for this model to be analyzed.
This study was approved by the institutional review board (IRB) of the researcher’s institution (IRB no. 2021-1134-0001). All information was downloaded anonymously from the website; therefore, no identification data were included.
Measurements
SES
SES was a composite variable created by summing the scores of education, employment status, and income (Yang et al., 2017). Education (0 = “≤high school,” 1 = “≥college”), employment status (0 = “unemployed,” 1 = “employed”), and income (0 = “<60% median income,” 1 = “≥60% median income”) were dichotomized. The composite SES scores ranged from 0 to 3. Higher scores indicated higher SES levels in this study.
Social Network Satisfaction
Social network satisfaction referred to an individual’s satisfaction with their social relationships. One question (“How much are you satisfied with your social relationships?”) was asked, using a five-point Likert-type scale: (1) very low, (2) low, (3) normal, (4) high, and (5) very high. A higher score indicated greater social network satisfaction.
Self-Esteem
Self-esteem was assessed using the Rosenberg Self-Esteem Scale (Bae et al., 2014; Rosenberg, 1965). This scale contains 10 items, with each item rated on a five-point Likert-type scale (1 = generally not true; 5 = always true). Items 3 (I am inclined to think that I am a failure), 5 (I feel I do not have much to be proud of), 8 (I wish I could have more respect for myself), 9 (I feel that I am not a person of worth), and 10 (I think that I am not a good person) were reverse-coded. A higher total score indicated higher self-esteem. The Cronbach’s alpha of the Korean version of the scale was .82 at the time of development (Bae et al., 2014) and .95 in this study.
Perceived Health Status
Perceived health status was assessed with the question, “How do you rate your own health?” A five-point Likert-type scale was used for the response: 1 = very healthy, 2 = healthy, 3 = neither healthy nor unhealthy, 4 = unhealthy, and 5 = very unhealthy. The question was reverse-coded, where a higher score indicated a better-perceived health status.
Depression
Depression was measured using the Center for Epidemiological Studies-Depression Scale developed by Kohout et al. (1993) and adapted into Korean (K-CESD-11) by Chon et al. (2001). Each item was rated on a four-point Likert-type scale (0 = rarely or none of the time; 3 = most or almost all the time). This tool contains 11 items, and the total score ranges from 0 to 33. Items 2 (I was relatively well) and 7 (I did not have many complaints) were reverse-coded, and the total depression score was calculated. A higher score indicated a higher level of depression, and depression was diagnosed by obtaining CESD-11 scores of ≥16. The Cronbach’s alpha was .91 at the time of the development of the Korean version (Chon et al., 2001) and .96 in this study.
Age
Age was determined by asking the participants to specify their birth year; the true age of the participants was calculated by subtracting their birth year from the year of data collection. Age was used as a control variable to control for the confounding effect of age on depression.
Data Analysis
The raw data of the 15th KOWEPS (Korea Institute for Health and Social Affairs, 2021) were downloaded for use, and the collected data were analyzed using Mplus 8.3 software. SES was entered as the independent variable, social network satisfaction, self-esteem, and perceived health status as the mediators, depression as the dependent variable, and age group as the control variable in the path analysis. Path analysis was performed to identify both direct and indirect relationships between variables, as well as any mediating effects between these variables.
The general characteristics of the participants were analyzed using frequencies, percentages, means, and standard deviations. For checking normality, skewness and kurtosis were examined, and the variable “income” was positively skewed. We, therefore, applied a log transformation; however, income remained non-normal according to the Shapiro–Wilk normality test. All other variables had an absolute skewness of ≤3 and an absolute kurtosis of <10, confirming normality (Kline, 2011).
Bivariate analysis was performed by calculating standardized partial correlation coefficients of each parameter. To analyze the study hypotheses and estimate the relationships among the variables, a path analysis was performed (MacKinnon, 2008). We assessed the goodness-of-fit of the path model by testing the chi-square (χ2), degrees of freedom (df), comparative fit index (CFI), Tucker–Lewis index (TLI), standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA). Standardization coefficient and 95% confidence interval (CI) were calculated with 1,000 nonparametric bootstrapping for the direct and indirect paths. The nonparametric bootstrapping procedure involves repeated estimations of the magnitude and CIs for the effects using a series of random samples (Preacher & Hayes, 2008). An indirect path was considered significant if the computed upper and lower limits of the 95% CI did not include 0.
Results
Participant Characteristics
Table 1 presents the descriptive statistics of the participants. Education level was divided into high school diploma and college degree or higher; 339 (14%) had a college degree or higher. While 170 (43.1%) of the participants were economically active, 251 (63.7%) were in the low-income class (less than 60% of the income median). The mean SES was 0.93. The mean age was 69.29 years, and 248 (62.9%) of participants were aged 65 years or older.
Characteristics of Participants (N = 394).

Note. SES = socioeconomic status.
The mean social network satisfaction and perceived health status scores were 3.45 and 3.07, respectively. The mean self-esteem and depression scores were 28.63 and 5.45, respectively.
Per Kline (2011), skewness and kurtosis were examined to test the normality of variables. Except for income, all variables had an absolute skewness of three or lower and absolute kurtosis of less than 10, confirming normality.
Correlations Among Major Variables and Multicollinearity
Before testing the model, the correlations among the variables were analyzed (Table 2). Depression was significantly negatively correlated with SES (r = −.242), social network satisfaction (r = −.361), self-esteem (r = −.523), and perceived health status (r = −.404), and significantly positively correlated with age (r = .142). The absolute value of the partial correlation coefficients among the major variables was smaller than .6, confirming the absence of multicollinearity.
Correlations of Study Variables.
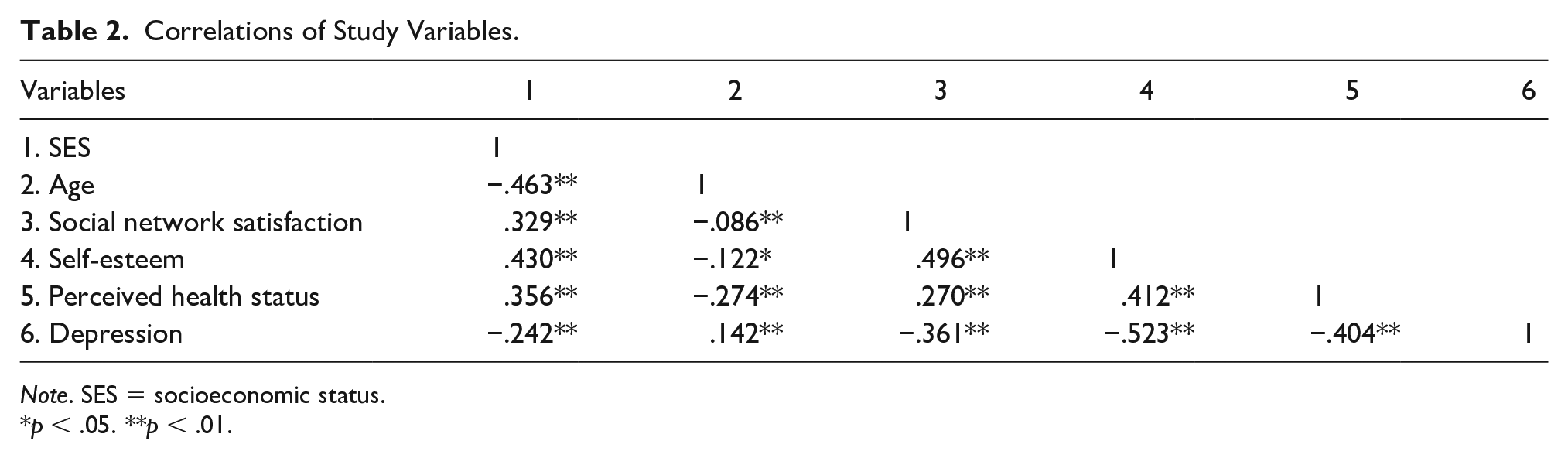
Note. SES = socioeconomic status.
p < .05. **p < .01.
Fit of the Hypothetical Model
The fit indices of the established path model were χ2: 17.263 (df = 12), CFI: .988, TLI: .979, SRMR: .032, and RMSEA: .033. Overall, the fit indices of the path model were acceptable (Anderson & Gerbing, 1984).
Path Model Analysis
Direct Paths
SES, the independent variable, had a significant positive effect on social network satisfaction (β = .329; p < .001), self-esteem (β = .430, p < .001), and perceived health status (β = .211, p < .001; Table 3). There was no significant effect of social network satisfaction on perceived health status, but self-esteem had a significant positive effect on perceived health status (β = .295, p < .001).
Direct and Indirect Path Effect (Standardization; N = 394).

Note. SES = socioeconomic status; SNS = social network satisfaction; PHS = perceived health status; SE = standard error; CI = confidence interval.
SES and age, the control variable, did not significantly influence depression, the dependent variable. However, social network satisfaction (β = −.125, p < .05), self-esteem (β = −.396, p < .001), and perceived health status (β = −.217, p < .001), the mediators, had a significant negative effect on depression (Figure 2).

Study Model Path Analysis
Indirect Paths
The total indirect effect of SES on perceived health status was β = .144 (p < .01). While social network satisfaction did not significantly mediate the effect of SES on perceived health status, self-esteem had a significant positive mediating effect (β = .126, p < .01).
The total indirect effect of SES on depression was β = −.243 (p < .01). Both social network satisfaction (β = −.041, p < .05) and self-esteem (β = −.170, p < .01) were significant negative mediators of the relationship between SES and depression. The mediation path through social network satisfaction and perceived health status in the effect of SES on depression was not significant, but the path through self-esteem and perceived health status had a significant negative mediating effect (β = −.027, p < .05). Bootstrapping confirmed that all these paths were consistent with the t test results for each coefficient.
Discussion
This study explored the effects of SES on depression based on the RCM (Gallo & Matthews, 2003), using path analysis, and analyzed the mediating effects of social network satisfaction, self-esteem, and perceived health status in this relationship. In this study, social network satisfaction, self-esteem, and perceived health status were positively related to depression. Depression decreased with increasing social network satisfaction, self-esteem, and perceived health status. This finding corresponds with the results of Hämmig (2019), where the prevalence of moderate to severe depression was higher among those who felt socially isolated and those with poor perceived health, regardless of age. A study on widowed men who lived alone also reported that social-relational coping resources influenced the level of depression (Lee & Jung, 2021). Self-esteem was significantly associated with depression in middle-aged men (Jo & Seong, 2016) and elderly men (Lee et al., 2019), supporting our results on self-esteem. However, in our study, SES did not have a significant direct effect on depression in middle-aged and elderly men living alone. This was contradictory to previous findings that SES influences depression and an individual’s mental health status because it induces health inequity (Gallo & Matthews, 2003). However, our results were similar to those of many studies that applied the RCM, wherein SES only had a significant indirect effect on depression or mental health, and not a direct effect (Bennett et al., 2015; Chen et al., 2021; Zamora-Racaza et al., 2017). This result may be attributable to the lack of data, as SES was not multidimensionally analyzed with the community poverty rate and social security insurance included (Gallo & Matthews, 2003). Furthermore, it is also attributable to the sociocultural trend in Korea, wherein middle-aged and elderly men feel that they need to take a backseat in society after middle adulthood, as a result of the International Monetary Fund (IMF) crisis in Korea, which eliminated the concept of a job for life (Kim, 2021), resulting in psychological factors having a greater influence on depression than SES.
Taken together, intrapersonal and interpersonal reserves, including social network satisfaction, self-esteem, and perceived health status, have higher mediating effects on depression than do tangible reserves, such as economic activity and income, in middle-aged and elderly men living alone after retirement.
Self-esteem was both directly associated with depression symptoms and indirectly associated with SES. Depression decreased with increasing self-esteem, which was consistent with the model positing that reserve capacity mediates health outcomes (Gallo, 2009); our result also supported previous findings that used the model, in which individuals’ psychosocial variables mediated the effects of SES on health (Azizoddin et al., 2017; Bennett et al., 2015). Particularly, individuals with high self-esteem can protect and defend themselves from psychological difficulties, and do not develop depression owing to their coping skills (Kim, 2020). The results demonstrated that self-esteem—an intrapersonal reserve—had a mediating effect, with the greatest effect on depression. This finding is consistent with the clear association between intrapersonal reserves and health documented in a few studies that also applied the RCM (Gallo et al., 2007; Matthews et al., 2008, 2010; Schnittker, 2004). This result suggests that intervention strategies that promote emotional stability by specifically targeting self-esteem among various coping resources are crucial for preventing depression in middle-aged and elderly men living alone. Regarding the indirect paths of SES on depression, perceived health status had a significant mediating effect only in the path involving the mediation of self-esteem. This finding also supports the notion that self-esteem is a more important intrapersonal reserve in mediating the effect on depression.
The findings demonstrated that the prevalence of depression among middle-aged and elderly men living alone was 6.6%. The percentage of men aged 40 years or older with suspected moderate or more severe depression was 3.6% in the 2019 Korean National Health Examination Statistics, indicating that the prevalence of depression is higher among middle-aged and elderly men living alone (Health Insurance Review & Assessment Service, 2020a). This result is also consistent with previous findings that single-person households have a higher prevalence of depression (Kwon et al., 2018). In the United States, the prevalence of depression was 5.2% among men in their 40s and 50s and 6.1% among men aged 60 years or older (Brody et al., 2018), indicating that middle-aged and elderly men living alone in Korea had a higher prevalence of depression, and therefore, this population should not be overlooked when planning preventive measures.
When developing interventions that effectively prevent depression in middle-aged and elderly men living alone, the target should be to resolve social isolation by achieving stability of SES and promoting self-esteem and perceived health status, as opposed to simply focusing on altering the SES (e.g., stable income and job) or building new social networks, such that individuals can utilize various coping resource dimensions to prevent depression. During this process, depression prevention interventions for middle-aged and elderly men living alone that strengthen individuals’ psychological health, namely intrapersonal reserves like self-esteem and perceived health status, should also be developed to reduce depression.
In this study, social network satisfaction did not have a significant direct effect on perceived health status, contradicting the results of a study that applied RCM, in which social support was associated with perceived health status (Gallo & Matthews, 2003).It seems that social network satisfaction was not significantly related to perceived health status because middle and older adulthood is a period characterized by a natural decline in formal social relationships based on economic activities (Lee & Jung, 2021). Furthermore, similar to SES, which is a tangible reserve, it supports that intrapersonal reserves are more effective than interpersonal reserves (e.g., social network satisfaction) in preventing depression.
This study is significant in that it provides foundational data for depression intervention programs by presenting the links between depression and its associated factors based on the RCM and using a path model in middle-aged and elderly men living alone, who are at high risk for a lonely death. The results of this study indicated that social network satisfaction, self-esteem, and perceived health status had direct effects on depression, while SES had an indirect effect on depression through the mediation of self-esteem and perceived health status. The number of middle-aged and elderly men living alone increases each year, meaning that people at risk of lonely death are on the rise; this calls for society-wide attention on the matter. Particularly, multidisciplinary research interests, as well as practical measures to develop feasible interventions, are essential to establish a social support system and improve people’s self-esteem.
This study has a few limitations that need to be addressed in future research. Because it was a cross-sectional study, we could not establish causality among the study parameters, but only make an inference. Although we used data from a nationally representative survey, a higher number of participants held high school diplomas, had an income less than 60% of the income median, and were aged was over 65 years. This may have resulted in a sampling bias, which is a threat to external validity.
Another limitation was that we could not enter cognitive-emotional factors, such as stress and optimism, as mediators in the model to examine relationships because this was a secondary data analysis, and the original data did not include these parameters. Despite these limitations, this study is significant in that it highlights the direction of depression prevention interventions for middle-aged and elderly men living alone by examining the links of reserve capacities such as social network satisfaction, self-esteem, and perceived health status in the effects of socioeconomic disparity on depression. Another key strength of this study is that nationally representative data (KOWEPS) were used to identify the paths of depression for the relatively neglected population of middle-aged and elderly men living alone. Additional longitudinal studies should be conducted to examine the changes in predictors of depression over time and changes in SES in middle-aged and elderly men living alone. Studies should investigate the causality between depression and its associated factors, including stress and optimism, which could not be examined in this study due to the lack of data, and compare middle-aged and elderly men living alone, with their counterparts living with family.
Footnotes
Data Sharing Statement
We used data from the 15th Korea Welfare Panel Study (KOWEPS) data. The KOWEPS is a nationally representative survey. In this study, the raw data of the most recent survey, the 15th KOWEPS conducted in 2020, were downloaded.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval Statement
This study was approved by the institutional review board (IRB) of the Catholic University of Korea (IRB no. 2021-1134-0001). All information was downloaded anonymously from the website; therefore, no identification data were included.