
Abstract
We examined the associations of male depression and psychotropic medication use with fecundability in a North American preconception cohort study (2013–2020). Men aged ≥21 years completed a baseline questionnaire with questions on history of diagnosed depression, the Major Depression Inventory (MDI), and psychotropic medication use. Pregnancy status was updated via bimonthly female follow-up questionnaires until pregnancy or 12 menstrual cycles, whichever occurred first. Analyses were restricted to 2,398 couples attempting conception for ≤6 menstrual cycles at entry. We fit proportional probabilities models to estimate fecundability ratios (FRs) and 95% confidence intervals (CIs), adjusting for age (male and female), education, (male and female), race/ethnicity, physical activity, alcohol intake, body mass index, smoking, and having previously impregnated a partner. Nearly 12% of participants reported a depression diagnosis; 90.6% had low depressive symptoms (MDI <20), 3.5% had mild symptoms (MDI: 20–24), 2.7% had moderate symptoms (MDI: 25–29), and 3.3% had severe symptoms (MDI: ≥30). A total of 8.8% of participants reported current use of psychotropic medications. History of depression was associated with slightly reduced fecundability, although this result was also reasonably compatible with chance (FR = 0.89; 95% CI: [0.76, 1.04]). FRs for mild, moderate, and severe compared with low depressive symptoms were 0.89 (95% CI: [0.66, 1.21]), 0.90 (95% CI: [0.62, 1.31]), and 0.88 (95% CI: [0.65, 1.20]), respectively. This indicates little evidence of a dose–response relationship for depressive symptoms with fecundability, although estimates were imprecise. Current psychotropic medication use mediated 44% of the association between depressive symptoms and fecundability.
Introduction
Major depressive disorder (depression) is the leading cause of disability worldwide, with more than 300 million individuals affected (World Health Organization, 2018). In the Unites States, depression affects about 15% of males (Kessler et al., 1994). Depression is a well-established consequence of infertility (Ahmadi et al., 2011; Babore et al., 2017; Drosdzol & Skrzypulec, 2009; Folkvord et al., 2005; Klemetti et al., 2010; Martins et al., 2016; Ozkan et al., 2015; Yang et al., 2017). The extent to which depression is a cause of infertility is unclear. Male depression has been associated with reduced fecundability in multiple studies (Cserepes & Bugan, 2015; Evans-Hoeker et al., 2018; Jacobson, 2016; Kravdal et al., 2017; Power et al., 2013; Tondo et al., 2011). All but one study have been conducted among couples seeking infertility treatment or have been retrospective in design. One prospective cohort study that matched male siblings with and without depression reported an association between depression and reduced fecundability (Power et al., 2013). Another cohort study, conducted within two randomized trials for non–in vitro fertilization (IVF) treatment of infertility, reported an association between baseline depressive symptoms among men (measured using the Patient Health Questionnaire [PHQ-9]; Kroenke et al., 2001) and decreased fecundability (Evans-Hoeker et al., 2018). There have been no other prospective studies of the association between male depression and fecundability.
Treatment for depression often involves the use of psychotropic medications. In North America, approximately 29% of depressed individuals use psychotropic medications (Beck et al., 2005), and the overall use of psychotropics has grown steadily in recent years (Helgason et al., 2004; Kantor et al., 2015; Middleton et al., 2001; Paulose-Ram et al., 2007). There have been no studies of the association between male psychotropic medication use and directly measured fertility outcomes (e.g., fecundability or live birth rates), but several studies have evaluated effects on semen quality. The majority of published studies have examined selective serotonin reuptake inhibitors (SSRIs), which have been associated with reduced semen quality in in vitro studies (Davidson et al., 1983; Kumar et al., 2006), animal studies (Alzahrani, 2012; Bataineh & Daradka, 2007), and epidemiologic studies (Koyuncu et al., 2011; Relwani et al., 2011; Tanrikut et al., 2010; Yland et al., 2021). Studies of other psychotropic medications such as serotonin-norepinephrine reuptake inhibitors (SNRIs) (Borges et al., 2013), norepinephrine-dopamine reuptake inhibitors, and tricyclic antidepressants (Levin et al., 1981; Maier & Koinig, 1994) report inconsistent results, but several (Beeder & Samplaski, 2020; Borges et al., 2013; Milosavljević et al., 2021) have reported adverse effects on semen volume and sperm motility that were reversible after discontinuation of medication use.
In the present study, we prospectively investigated the association of fecundability with depression history, current depressive symptoms, and psychotropic medication use among men participating in a North American preconception cohort study. Depression may influence fecundability via use of antidepressants and sexual dysfunction (Ferguson, 2001; La Torre et al., 2013; Montgomery et al., 2002; Ozkan et al., 2015; Rothschild, 2000), reduced sleep quality or duration (Wise et al., 2018), or reduced testosterone levels (Gettler & Oka, 2016; Johnson et al., 2013; Khera, 2016). We evaluated the extent to which the current use of psychotropics, intercourse frequency, and hours of sleep per night were mediators of the relationship between current depressive symptoms and fecundability. Finally, we examined the extent to which erectile dysfunction mediated the relationship between psychotropic medication use and fecundability.
Methods
Study Population
Pregnancy Study Online (PRESTO) is an ongoing web-based preconception cohort study. The study methods have been described previously (Wise et al., 2015). Briefly, women aged 21 to 45 years residing in the United States or Canada, and who are not using contraception or receiving fertility treatment are eligible for participation. Female participants complete an online baseline questionnaire with items on demographics, behavioral factors, medical and reproductive history, and medication use. After completion of the baseline questionnaire, female participants are given the option to invite their male partners to participate. Men aged ≥21 years are eligible. Male participation involves completion of a baseline questionnaire similar to the female baseline questionnaire. Female participants complete follow-up questionnaires every 8 weeks for 12 months or until reported pregnancy, whichever occurs first. The study was approved by the Institutional Review Board at Boston University Medical Campus, and informed consent was obtained from all participants.
From June 2013 through October 2020, 12,436 eligible women completed the baseline questionnaire. We excluded 142 women whose baseline date of last menstrual period (LMP) was >6 months before study entry and 29 women with missing or implausible LMP data. We then excluded 2,546 women who had been trying to conceive for more than six cycles at enrollment, to reduce potential for recall bias and reverse causation (i.e., subfertility causing changes in behavior). Of the 9,719 remaining female participants, 5,182 (53%) invited their male partners to participate, and 2,398 males (46%) enrolled.
Assessment of Exposure
On the male baseline questionnaire, participants were asked whether they had ever been diagnosed with depression, the year they were first diagnosed, whether they had ever taken any medication for depression or anxiety, whether they had taken any prescribed medication for depression or anxiety within the last 4 weeks, and the name of the prescribed medication. In addition, participants were asked whether they had taken any other medication for other medical conditions (ever and within the last 4 weeks) and the name of the medication. These other medication variables were also considered to identify psychotropic medication use. We used self-reported medication names to identify current users of psychotropic medications. We further classified these individuals as current users of SSRIs, other antidepressants (SNRIs, atypical, tetracyclic, and tricyclic antidepressants), and non-antidepressant psychotropics. Participants could be classified as taking more than a single type of psychotropic medication, although only 18 (0.8%) men reported using more than one medication.
Each participant filled out the Major Depression Inventory (MDI), reporting depressive symptoms experienced during the previous 2 weeks, comprising 12 questions with a possible range of scores of 0 to 50. The MDI has been validated in multiple studies, including both population-based and patient-based studies (Bech, 1997; Bech et al., 2001; Bech & Wermuth, 1998). It has high sensitivity (0.86) and specificity (0.86) compared with clinician-diagnosed major depressive disorder (Bech et al., 2001). We used standard criteria to categorize MDI scores as low (MDI <20), mild (MDI 20–24), moderate (MDI 25–29), and severe (MDI ≥30) (Olsen et al., 2003) and defined “current depressive symptoms” as MDI ≥25.
Assessment of Fecundability
Fecundability is defined as the average probability of pregnancy during a single menstrual cycle for a couple engaging in regular intercourse without contraception. At baseline, female participants reported their date of LMP, their usual menstrual cycle length, and the number of cycles they had been attempting conception. On each follow-up questionnaire, they reported their most recent LMP date, whether they had become pregnant since the previous questionnaire, and whether they had initiated fertility treatment. Total discrete menstrual cycles at risk were calculated as follows: menstrual cycles of attempt at study entry + [(LMP from most recent follow-up questionnaire—date of baseline questionnaire completion)/usual menstrual cycle length] +1.
Assessment of Covariates
On the baseline questionnaire, both partners reported their age, race/ethnicity, education, height, and weight. On the male baseline questionnaire, participants reported data on physical activity, alcohol intake, smoking history, sleep duration, erectile dysfunction, history of infertility (defined as having tried to conceive for >12 months without success), and whether they had previously impregnated a female partner. The female baseline questionnaire additionally collected data on sexual intercourse frequency. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. Total metabolic equivalents of task (METs) of physical activity were calculated by multiplying the average number of hours per week engaged in various activities by metabolic equivalents estimated from the Compendium of Physical Activities (Ainsworth et al., 2000; McKinnon et al., 2016).
Statistical Analysis
Couples contributed observed cycles of attempt time to the analysis from baseline until reported conception, loss to follow-up, withdrawal, initiation of fertility treatment, or 12 cycles, whichever came first. We used an Andersen-Gill data structure, with one row per at-risk menstrual cycle under observation, to account for variation in attempt time at study entry and reduce bias from left truncation (Therneau & Grambsch, 2000). We used proportional probabilities regression models (Weinberg et al., 1989) to estimate fecundability ratios (FRs) and 95% confidence intervals (CIs) for the association between a history of diagnosed depression, current depressive symptoms, psychotropic medication use, and fecundability. The FR represents the ratio of the per-cycle probability of conception in each exposure category compared with the reference category.
We conducted three sets of primary analyses to evaluate the association between fecundability and depression, psychotropic medication use, and a combined exposure of depression and psychotropics. For the analysis of depression and fecundability, we estimated the FRs associated with (1) a history of diagnosed depression (ever vs. never), (2) a 5-unit increase in MDI score, and (3) current depressive symptoms (MDI score <25 vs. ≥25). We also fit restricted cubic splines to allow for a smoothed fit of the relation between MDI score and fecundability, with three knot points at MDI scores of 20, 25, and 30 (Durrleman & Simon, 1989). For the analysis of psychotropic medication use and fecundability, we estimated the FRs associated with the use of (1) non-antidepressant psychotropics, (2) SSRIs, and (3) other antidepressants. To evaluate a combined exposure of depression and psychotropics, we estimated the FRs for (1) current psychotropic medication users with MDI ≥25, (2) current psychotropic medication users with MDI <25, and (3) non-users of psychotropic medications with MDI ≥25, all relative to non-users of psychotropic medications with MDI <25.
Potential confounders were selected a priori based on the available literature and assessment of a directed acyclic graph (Online Appendix A). Results were adjusted for covariates ascertained at baseline, including male and female age (<25, 25–29, 30–34, ≥35 years), race/ethnicity (non-Hispanic White vs. other race/ethnicity), highest level of male and female education (high school or less, some college, college graduate, graduate school), total METs (continuous), alcohol consumption (0, 1–6, 7–13, and ≥14 drinks/week), BMI (<25, 25–29, ≥30 kg/m2), cigarette smoking (never, current, and past), and having previously impregnated a female partner (yes vs. no). Because the Spearman correlation coefficient between male and female depressive symptoms was low (r = .28), we did not adjust for female MDI score. All analyses of psychotropic medications were adjusted for other current and former use of psychotropic medications.
We conducted several sensitivity analyses to evaluate the robustness of our results. Given that exposure data were collected only at baseline from males, but follow-up could continue for up to 12 total menstrual cycles, we performed a sensitivity analysis restricted to the first three cycles of follow-up (i.e., the approximate duration of spermatogenesis) (Misell et al., 2006). In addition to reducing exposure misclassification, truncating follow-up time may reduce attenuation of FRs in time to pregnancy studies (Eijkemans et al., 2019). We also conducted two analyses to limit potential reverse causation (i.e., to ensure that we estimated the effect of pre-existing depression on subsequent fecundability). First, we restricted analyses to participants with less than three cycles of attempt time at enrollment. Second, we performed an analysis restricted to men without a history of infertility.
Mediation Analysis
We performed mediation analyses to evaluate the extent to which the association between current depressive symptoms and fecundability may be mediated by current use of any psychotropic medication, current SSRI use, intercourse frequency, or sleep duration. In addition, we estimated the mediating effects of erectile dysfunction on the relationship between current psychotropic medication use and fecundability. Mediation analysis decomposes the relationship between exposure (depressive symptoms or use of psychotropics) and fecundability into natural direct and indirect, or mediated, effects. The natural direct effect represents the effect of the exposure on outcome that is independent of the potential mediator, whereas the natural indirect effect represents the effect of the exposure that acts through the mediator. The proportion mediated can then be calculated as (FRNDE × [FRNIE − 1])/(FRNDE × FRNIE − 1), such that FRNDE is the natural direct effect and FRNIE is the natural indirect effect (VanderWeele, 2009, 2011, 2016).
For psychotropic medication use, SSRI use, and sleep duration, we fit a model with cross-product terms between current depressive symptoms (MDI ≥25) and each of the potential mediators. This allowed for the presence of interaction between the mediator and exposure. For intercourse frequency, we estimated mediation from a model without a product term with current depressive symptoms because there was no evident interaction. To estimate the extent to which erectile dysfunction mediates the relationship between psychotropic medication use and fecundability, we fit a model with a cross-product term between psychotropic medication use and erectile dysfunction. For each analysis, we estimated the natural direct effect of exposure (current depressive symptoms or current psychotropic medication use) on fecundability, the natural indirect effect operating through the mediating variables, and the proportion mediated.
Missing Data
Missing data were handled using multiple imputation. Specifically, we used fully conditional specification to impute missing outcome, exposure, and covariate data (Schafer, 1999; Sterne et al., 2009). We generated 20 imputation data sets and combined point estimates and standard errors across the data sets. For the 166 couples with no follow-up data, we assigned them one cycle of follow-up and imputed their pregnancy status (yes vs. no). Missingness for covariates ranged from <0.1% (education, BMI) to 2.0% (previously impregnated a partner). We used the weighted copy method to improve convergence of the regression models (Deddens & Petersen, 2008). All analyses were performed in SAS version 9.4 (SAS, 2014).
Results
A total of 2,398 couples contributed 1,497 pregnancies during 10,498 observed menstrual cycles of attempt time. At baseline, 283 (11.8%) men reported having a history of diagnosed depression. Based on MDI score, 2,173 (90.6%) men were classified as having low depressive symptoms, 83 (3.5%) had mild symptoms, 64 (2.7%) had moderate symptoms, and 78 (3.3%) had severe symptoms (Table 1). A total of 212 men (8.8%) were currently using psychotropic medications (78 [3.3%] used non-antidepressant psychotropics, 104 [4.3%] used SSRIs, and 48 [2.0%] used other antidepressants) (Table 2). Compared with men who had no history of depression, those with a history of depression were more likely to be obese (BMI ≥30 kg/m2) and to report a history of smoking, and they reported less physical activity on average (Table 1). Men with more severe depressive symptoms reported shorter sleep duration and less education on average and were more likely to report erectile dysfunction than those with lower MDI scores (Table 1). SSRI use was positively associated with obesity and low intercourse frequency (Table 2). Patterns of associations for use of other antidepressants were generally similar (Table 2).
Age-Standardized Baseline Characteristics of 2,398 Men According to History of Depression and Current Depressive Symptoms, PRESTO, 2013–2020.

Note. SSRI = selective serotonin reuptake inhibitors; SNRI = serotonin and norepinephrine reuptake inhibitors; MET = metabolic equivalent; BMI = body mass index; MDI = Major Depression Inventory.
Age-Standardized Baseline Characteristics of 2,398 Men According to Selected Psychotropic Medication Use, PRESTO, 2013–2020.
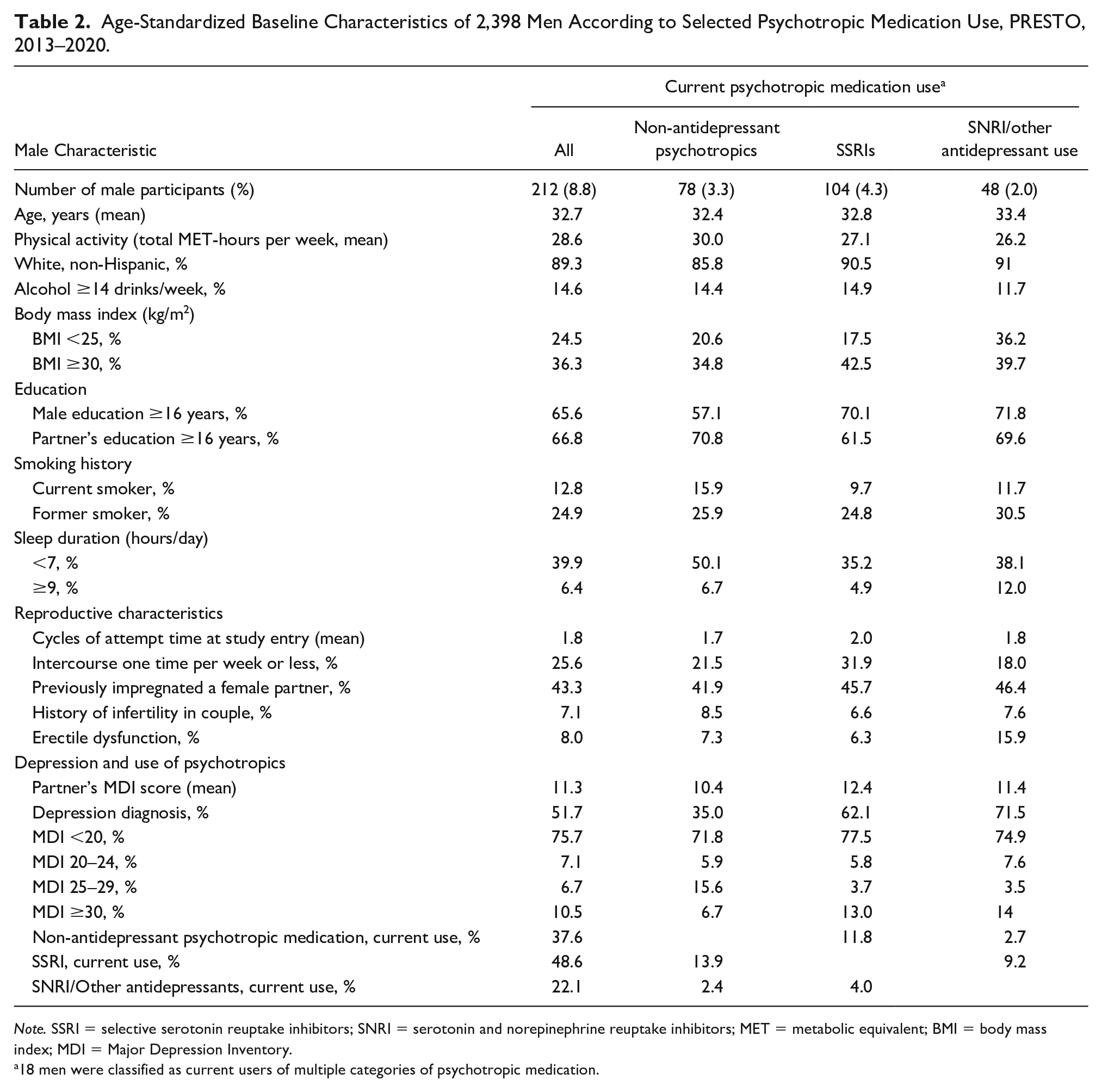
Note. SSRI = selective serotonin reuptake inhibitors; SNRI = serotonin and norepinephrine reuptake inhibitors; MET = metabolic equivalent; BMI = body mass index; MDI = Major Depression Inventory.
18 men were classified as current users of multiple categories of psychotropic medication.
The per-cycle probability of conception for men with a history of diagnosed depression was 0.89 times that of men without a history of diagnosed depression (FR = 0.89; 95% CI: [0.76, 1.04]). FRs for MDI categories of mild, moderate, and severe depressive symptoms were 0.89 (95% CI: [0.66, 1.21], 0.90 (95% CI: [0.62, 1.31]), and 0.88 (95% CI: [0.65, 1.20]) relative to low symptoms. The FR for each 5-unit increase in MDI score was 0.97 (95% CI: [0.94, 1.01]) (Table 3). The FR for current depressive symptoms (MDI score ≥25 vs. <25) was similar to the FR for diagnosed depression (FR = 0.89; 95% CI: [0.70, 1.14]). The restricted cubic spline analysis indicated an inverse association between MDI score and fecundability, but the CIs were wide (Figure 1).
Depression, Depressive Symptoms, Psychotropic Medication Use, and Fecundability, PRESTO, 2013–2020.

Note. SSRI = selective serotonin reuptake inhibitor; PM = psychotropic medication; BMI = body mass index; MDI = major depression inventory.
Adjusted for age, female age, race/ethnicity, education, partner’s education, total METs, alcohol consumption, BMI, current smoker, past smoker, and previously impregnated a female partner.
Additionally adjusted for former PM use, as well as non-antidepressant psychotropic medication, SSRI, SNRI, and other antidepressant use where appropriate.

Restricted Cubic Spline for the Association Between Major Depression Inventory Score and Fecundability
The FRs for current use of non-antidepressant psychotropic medications, SSRIs, and other antidepressants were 0.89 (95% CI: [0.65, 1.23]), 0.85 (95% CI: [0.65, 1.12]), and 1.03 (95% CI: [0.71, 1.48]), respectively (Table 3). Fecundability was 27% lower among current psychotropic medication users with MDI ≥25 compared with non-users of psychotropics with MDI <25 (FR = 0.73, 95% CI: [0.44, 1.22]). FRs for current psychotropic medication users with MDI <25 and for non-users of psychotropics with MDI ≥25, relative to non-users of psychotropics with MDI<25, were 0.90 (95% CI: [0.75, 1.09]) and 0.94 (95% CI: [0.72, 1.22]), respectively (Table 3).
When we restricted the incident period to the first three cycles of follow-up, associations were attenuated for a history of diagnosed depression (FR = 0.97; 95% CI: [0.81, 1.17]) and psychotropic medication use: the FRs for current use of non-antidepressant psychotropics, SSRIs, and other antidepressants were 0.95 (95% CI: [0.65, 1.40]), 0.91 (95% CI: [0.66, 1.26]), and 1.08 (95% CI: [0.71, 1.66]), respectively. Nevertheless, similar associations were observed comparing men with severe versus low depressive symptoms (MDI ≥30 vs. <20: FR = 0.88, 95% CI: [0.62, 1.27]) and comparing psychotropic medication users with MDI ≥25 versus non-users of psychotropics with MDI <25 (FR = 0.72, 95% CI: [0.37, 1.38]) (Online Appendix B).
Among participants with less than three cycles of pregnancy attempt time at enrollment, we observed slightly stronger results for history of diagnosed depression, severe depressive symptoms, non-antidepressant psychotropic medication use, and SSRI use. The results for current psychotropic medication users with MDI ≥25 were similar (FR = 0.74, 95% CI: [0.35, 1.59]) (Online Appendix C). When limiting the analysis to men without a history of infertility, the results were similar to the full analysis (Online Appendix D).
The proportion of the association between current depressive symptoms and fecundability that was mediated by the current use of psychotropics was 0.44 for any psychotropic medication and 0.19 for SSRIs specifically. For intercourse frequency, the proportion mediated was 0.17. Sleep duration was not a mediator of the relationship between current depressive symptoms and fecundability; the proportion mediated could not be estimated because the natural direct and indirect effect estimates were in opposite directions. Erectile dysfunction was not a mediator of the relationship between psychotropic medication use and fecundability (Online Appendix E).
Discussion
In this preconception cohort study, a history of diagnosed depression and greater depressive symptoms (as measured by the MDI) among men were associated with slightly decreased fecundability. These findings were imprecise and consistent with chance, but also with a modest adverse effect. Use of non-antidepressant psychotropics and SSRIs was also associated with slightly reduced fecundability, but estimates were imprecise. Having both a history of depression and current moderate or severe depressive symptoms was associated with a greater reduction in fecundability than these singular exposures, although this association was reasonably consistent with chance. Our findings indicate that current use of psychotropics and intercourse frequency may mediate the association between depressive symptoms and fecundability.
The observed association between history of diagnosed depression and fecundability is consistent with the two other prospective studies on this topic. Among Swedish men with depression who were matched with unaffected siblings, Power et al. reported an FR of 0.93 (95% CI: [0.92, 0.94]), an estimate of effect very similar to the FR of 0.89 in the present study (Power et al., 2013). Our findings for current depressive symptoms were also in the same direction as those reported in a study of couples participating in two randomized trials. The trials were designed to evaluate the comparative effectiveness of several ovulation induction therapies in women with polycystic ovarian syndrome (Pregnancy in Polycystic Ovary Syndrome II [PPCOS II]) and couples with unexplained infertility (Assessment of Multiple Intrauterine Gestations From Ovarian Stimulation [AMIGOS]) (Evans-Hoeker et al., 2018). Current depressive symptoms were assessed at enrollment using the PHQ-9, and the authors reported a 56% lower probability of pregnancy among depressed men relative to non-depressed men (risk ratio = 0.44; 95% CI: [0.20, 0.98]). This is a substantially stronger association than what we observed, which may be due to several factors. First, the trial populations had a low prevalence of major depression (there were only five pregnancies among depressed men). Second, the trials could not determine whether depression was antecedent or subsequent to infertility. Third, the two trials had vastly different conception rates for men with depression (10.5% vs. 20%), which suggests that the two trial populations fundamentally differed in ways which could affect the estimation of the association between depression and fertility. One potential explanation is differences in BMI: the average BMI of female trial participants was approximately 35 kg/m2 in PPCOS II and 27 kg/m2 in AMIGOS.
Our findings indicate that almost half of the effect of current depressive symptoms on fecundability can be explained by the effects of using psychotropic medications. Another potential mechanism linking depression and current depressive symptoms with reduced male fertility is testosterone, which is critical for spermatogenesis, sexual function, and fertility (Singh et al., 1995). Depression in men is associated with low testosterone levels (Gettler & Oka, 2016; Johnson et al., 2013; Khera, 2016). While depression can affect libido, and thereby decrease intercourse frequency, we found evidence that intercourse frequency mediated only 17% of the depression–fecundability association. Although depressive symptoms are associated with poor sleep health, and poor sleep health may influence fecundability, we did not see evidence that sleep mediated the association between depressive symptoms and fecundability.
This is the first study to prospectively examine the relationship between male psychotropic medication use and fecundability in a population not undergoing fertility treatment. In a previous study among a subset of PRESTO participants, use of psychotropic medications was associated with worse semen quality for sperm concentration, sperm motility, total sperm count, and total motile sperm count, although associations were imprecise and confounded by depression diagnosis (Yland et al., 2021). However, the relationship between semen quality parameters and fecundability has been debated (Bonde et al., 1998; Guzick et al., 2001; Zinaman et al., 2000). One study reported that low sperm concentration, but not semen volume or sperm motility, was associated with reduced fecundability (Bonde et al., 1998). In another report, infertility was associated with sperm count, motility, and morphology, but not semen volume or sperm concentration (Zinaman et al., 2000). Thus, it remains important to study both semen quality and fecundability as distinct outcomes.
Our findings are generally consistent with studies that examined psychotropic medication use and semen parameters, which indicated that use of antidepressants, particularly SSRIs, may be associated with lower semen volume (Maier & Koinig, 1994), sperm concentration (Gettler & Oka, 2016; Kumar et al., 2006), and sperm motility (Maier & Koinig, 1994; Relwani et al., 2011), as well as DNA fragmentation (Gettler & Oka, 2016; Tanrikut et al., 2010) and abnormal sperm morphology (Gettler & Oka, 2016; Maier & Koinig, 1994). We found little evidence that erectile dysfunction mediated the association between psychotropic medication use and fecundability, despite consistent associations between psychotropic medication use and erectile dysfunction in the literature.
In the present study, men with moderate or severe depressive symptoms who currently used psychotropic medications had the lowest fecundability of all subgroups examined. Psychotropic medications may interact with depression to cause even greater reductions in fecundability, or this could be a marker of more severe depression (i.e., confounding by indication).
Study limitations include the potential for exposure misclassification. Current depressive symptoms may be misclassified because the MDI was administered only once at baseline. In addition, some men may underreport history of depression diagnosis or use of psychotropic medications. Given the prospective study design, we would expect this misclassification to be non-differential and to attenuate our effect estimates for dichotomous exposures. To address this limitation, we restricted the incident period to the first 3 cycles of follow-up. This method of restriction can reduce attenuation of FRs in time-to-pregnancy studies (Eijkemans et al., 2019). We observed similar results for most associations; however, the association between history of diagnosed depression and fecundability was attenuated. Another limitation of this study is that depression and treatment for depression may have been a consequence of existing fertility problems. To explore potential for reverse causation, we conducted two sensitivity analyses. First, we repeated our analyses among men with fewer than three cycles of attempt time at enrollment and found similar though less precise results. Second, we conducted an analysis among men without a history of infertility; these results were comparable. Our evaluation of treatment for depression was also limited. We did not collect data on non-medication treatments for depression, such as psychotherapy or cognitive behavior therapy, which could have served as a useful comparison group in assessing treatment effects on fecundability (Butler et al., 2006). In addition, we did not collect data on dosage of the studied psychotropic medications.
Our study differs from previous studies in several ways. First, we enrolled couples during the preconception period, soon after discontinuing contraception, which can reduce potential for selection bias, recall bias, and bias due to left truncation (Baird et al., 1994; Joffe et al., 2005; Schisterman et al., 2013; Weinberg et al., 1994). Second, we enrolled couples across the full fertility spectrum, including those who conceived quickly and those who eventually developed infertility, thereby increasing the generalizability of our findings. Third, we prospectively studied depression and psychotropic medication use, and mediation of the depression–fecundability association by use of psychotropics, to distinguish effects of treatment from those of underlying disease. Finally, we assessed fecundability rather than semen quality parameters, as fecundability is a potentially more sensitive and direct measure of fertility (Bonde et al., 1998; Buck Louis et al., 2014; Irvine, 1998; Loft et al., 2003; Slama et al., 2002).
In conclusion, depression, defined via self-reported history of diagnosed depression or current depressive symptoms using the MDI, was associated with slightly decreased fecundability, consistent with previous studies. Psychotropic medication use was also associated with reduced fecundity, particularly among those with current depressive symptoms. Nonetheless, the findings were imprecise and reasonably compatible with chance. Our findings indicate that the current use of psychotropics may mediate almost half of the relationship between current depressive symptoms and fecundability. Reduced intercourse frequency was a less important mediator of this association. This study contributes to our understanding of the potential causes of infertility. The results of our mediation analysis provide insight into what components of these relationships might be effective targets for improving fecundability among couples planning pregnancy.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883221075520 – Supplemental material for A Prospective Study of Male Depression, Psychotropic Medication Use, and Fecundability
Supplemental material, sj-docx-1-jmh-10.1177_15579883221075520 for A Prospective Study of Male Depression, Psychotropic Medication Use, and Fecundability by Jennifer J. Yland, Craig J. McKinnon, Elizabeth E. Hatch, Michael L. Eisenberg, Yael I. Nillni, Kenneth J. Rothman and Lauren A. Wise in American Journal of Men's Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.L.E. is an advisor for Roman, Sandstone, Dadi, Hannah, and Underdog. K.J.R. is an employee of RTI Health Solutions, an independent non-profit research organization that does work for government agencies and pharmaceutical companies. L.A.W. does consultancy for AbbVie Inc. In the last 3 years, Pregnancy Study Online has accepted in-kind donations from Sandstone Diagnostics, Swiss Precision Diagnostics, ![]() , and FertilityFriend.com. None of these studies has any relation to the present study. The authors report no other relationships or activities that could appear to have influenced the submitted work.
, and FertilityFriend.com. None of these studies has any relation to the present study. The authors report no other relationships or activities that could appear to have influenced the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health (R01 HD086742, R03 HD090315, R01 HD105863). The funders had no role in the study design, data collection, analysis and interpretation of data, writing of the report, or the decision to submit the paper for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.