
Abstract
Higher prevalence of obesity in men compared with women, particularly among those 18 to 40 years of age, has been observed in Singapore. We explored young men’s perceptions of weight change after transiting out of National Service (NS) over a 12-month period and sought to understand the underlying drivers. In-depth interviews, guided by the Health Belief Model (HBM), were conducted with young men 12 months after they had completed full-time NS. Six constructs from the HBM, namely, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and perceived self-efficacy, were utilized to guide the analysis. Thematic analysis revealed that participants generally perceived a gain in body weight after the transition and attributed this to decreased exercise-related physical activity (PA) levels and increased consumption of unhealthy food. However, many did not display immediate concerns nor view leading a healthy lifestyle as priority, citing time constraints, inertia to comply, or lack of access to sports facilities and healthy food options as barriers. Healthy lifestyle behaviors, mainly PA, were mostly pursued for physical health and appearance. Motivators toward a healthy lifestyle tended to be internal factors such as self-motivation, personal preference, and habit, whereas external motivators included peer or familial influence and environmental factors. Our findings align with key concepts of the HBM and suggest a need to educate young men transiting out of NS on lifestyle, weight, and health, in particular addressing their misconceptions.
Background
Obesity is a health condition of rising global concern as it raises the risk of a range of noncommunicable diseases, including hypertension and diabetes mellitus (Rahmouni et al., 2005; Sowers, 2003; Steppan et al., 2001). Globally, overweight and obesity prevalence rates among adults surged by 27.5% over 33 years (Ng et al., 2014). Similarly in Singapore, overweight and obesity rates have increased alarmingly over a 10-year period, from 26.2% in 1997 to 36.2% in 2017 (Epidemiology & Disease Control Division, Ministry of Health, Singapore, 2017). The rise in obesity prevalence can be attributed to countries worldwide, including Singapore, experiencing “nutrition transitions” or a shift from a primarily plant-based diet to a meat and processed foods diet, particularly when foods rich in salt, sugar, and saturated fats have become cheaper and more widely available (Branca et al., 2019). This, combined with the increase in physical inactivity as people have more disposable income, are contributing to weight gain and risk of chronic illnesses (Fox et al., 2019; Health Promotion Board, 2014). Research suggests that weight is ultimately a function of a lack of energy balance, or taking in more calories than are expended through physical activity (PA).
The Singapore Prospective Study Program reported that adult individuals (n = 2,483) who gained the most weight and greatest waist circumference (WC) over a period of 8 to 10 years belonged to the young adults (aged 18–29 years; Ong et al., 2009). This finding concurs with studies in other countries, demonstrating that young adults are the most susceptible to weight gain (Lewis et al., 2000; Nelson et al., 2008; Rissanen et al., 1988; Wardle & Boniface, 2008; Williamson, 1993). Weight gain in young adults has been attributed to major transitions (Lewis et al., 2000; Nelson et al., 2008), such as moving out of family homes and starting university (Laska et al., 2012), that may be associated with poor dietary choices (Li et al., 2012) and sedentary behaviors (Anderson et al., 2009).
Interestingly, local statistics in 2010 revealed that obesity prevalence rates in young men (aged 18–29 years) were 3 times higher than in young women (15.4% vs. 5.8%; Epidemiology & Disease Control Division, Ministry of Health, Singapore, 2010). This is contrary to findings in the United States (Lewis et al., 2000; Williamson et al., 1990), where obesity rates were higher among young women (aged 18–34 years) instead. We speculate that this disparity in obesity rates between genders may be partially due to mandatory full-time National Service (NS), which all Singaporean males are required to undergo for 2 years on completing postsecondary education (The Law Revision & Commission, 2001). The U.S. Millennium Cohort Study (n = 38,686) reported that males were vulnerable to a rapid weight gain at the time of discharge from the military (Littman et al., 2013) and attributed this finding to a high energy consumption despite a decrease in energy expenditure. High overweight and obesity rates were also observed in other conscription cohorts in Germany, Austria, Norway, and Iran (Hermanussen et al., 2001; Salimi et al., 2019). It is unclear whether the same applies to young Singaporean men after a period of transiting out of a highly structured environment characterized by compulsory PA and limited dietary options.
Although interventions have attempted to curtail the rise of obesity among young men, low attendance rates from “not being able to reach, engage and retain young men successfully” have often affected their efficacy and success rates. Another plausible factor is that interventions had been designed without much understanding of young men’s perceptions toward leading a healthy lifestyle (Ashton et al., 2015), hence resulting in a mismatch in design and implementation. Previous research has shown that gender tailored interventions have the potential to address the social diversity and plurality of masculinities in young men, thus being (Ashton et al., 2015; Ashton, Morgan, et al., 2017) more effective in recruiting, retaining, and engaging men and improving their health outcomes (Beck et al., 2010; Kreuter et al., 2013; Morgan et al., 2013). For interventions to be effective in young men, factors such as barriers and motivators driving their lifestyle choices, in the relevant cultural setting, should be elucidated.
Although there has been a steady rise in the number of studies exploring perceived motivators/enablers and barriers in young men in relation to weight management and lifestyle behaviors in Australia (Ashton et al., 2015; Ashton, Hutchesson, et al., 2017; Mendis et al., 2014) and the United States (Greaney et al., 2009; Levi et al., 2006; Walsh et al., 2009), only a few have adopted qualitative approaches (Ashton et al., 2015; Greaney et al., 2009; Mendis et al., 2014; Walsh et al., 2009). Qualitative research is particularly useful for understanding concepts and gathering opinions and experiences, and thus offers in-depth insights into areas less known and explored, like this study (Agius, 2018). It is worth noting that, besides Greaney et al. (2009) who adopted an ecological approach to analyze data collected from focus groups, no other studies have used health behavior theories to guide their qualitative research in this area.
In this study, we adopted the updated Health Behavior Model (HBM; Glanz et al., 2015) to guide our research. Being a value-expectancy model, its constructs will enable us to better understand and interpret the extent to which young men value weight control and health and their expectations of how healthy lifestyle behaviors may achieve this. This model comprises of six constructs: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and perceived self-efficacy. Questions related to these constructs examined participants’ beliefs about their likelihood of getting a condition, that is, weight change (perceived susceptibility), about the seriousness of the condition (e.g., weight gain and obesity) and its consequences (perceived severity), positive aspects of adopting a health behavior to reduce the risk of this condition (perceived benefits), obstacles to performing the health behavior and related negative aspects (perceived barriers), and internal and external factors that trigger the health behavior (cues to action). Self-efficacy, which refers to the confidence that one can perform the recommended health behavior, was also examined.
As it remains unclear whether current findings in Caucasian populations are relevant to young men in an Asian context like Singapore, this study aimed to understand the factors, including barriers and motivators, that drive certain lifestyle choices, particularly in relation to diet and PA, in young men in Singapore (aged 19–25 years) when transiting out of full-time NS. We assessed changes in their body weight and waist circumference 12 months after this transition.
Method
Study Design
This study adopted a qualitative approach in the form of in-depth interviews and was conducted in adherence to the requirements outlined in the consolidated criteria for reporting qualitative research (COREQ) checklist (Tong et al., 2007; Supplementary Material). It was granted ethical approval by the Institutional Review Board at the National University of Singapore.
Participants and Setting
Recruitment was conducted during designated Health and Safety days among six military units with a spectrum of vocations, encompassing participants of diverse backgrounds. This study was advertised to participants as a study by the University to better understand factors influencing weight changes in full-time NS who were transiting out of army training, so that appropriate interventions can be developed for the Singapore population. Interested participants approached a booth with researchers from the University to obtain detailed information of the study and provide their informed written consent. Only full-time NS men in their final 6 months of service and who were between 19 and 25 years of age were included. Those older than 25 years of age were excluded as they were typically military professionals and would not transit out of NS unless retired. Included participants were required to be Singapore citizens or permanent residents of Chinese, Malay, or Indian ethnicity; able to read and understand English; and have internet access on their mobile phones or on a smart device at home.
Data Collection
At the recruitment booth, anthropometric measurements of the participants were taken and recorded by trained personnel. Participants’ height was measured using a stadiometer and recorded to the nearest one decimal place. Participants’ weight and WC were measured in duplicate using a weighing scale and measuring tape, respectively; recorded to the nearest one decimal place; and averaged. Body mass index (BMI; kg/m2) was calculated by taking weight (kg) divided by the square of height (m). In addition, participants were sent an online questionnaire to provide demographic information, including age, ethnicity, household income, residential area, and education level.
The participants visited the study site at the University 12 months from the recruitment visit. Anthropometric measurements of weight, height, and WC were taken, followed by an in-depth interview in a consultation room to ensure confidentiality. The interview sessions were conducted in English, were facilitated by two trained researchers (H.X.L. and J.K.I.) and took approximately 60 min each. An audio recorder and notepad were used to capture the information collected. Field notes was cross-checked by the same two researchers after the interviews and this helped to ensure that data saturation was reached before making the decision to terminate further interviews. Cash reimbursement was issued for the participants’ time and travel.
The questions asked during the interview sessions were modified from and loosely based on the updated Health Belief Model (HBM), a framework explaining and predicting individual health-related behaviors (Glanz et al., 2015). This framework comprises of six constructs: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and perceived self-efficacy (construct included in the updated HBM). Questions related to these constructs examined participants’ beliefs about their likelihood of getting a condition, that is, weight change (perceived susceptibility), about the seriousness of the condition (e.g., weight gain and obesity) and its consequences (perceived severity), positive aspects of adopting a health behavior to reduce the risk of this condition (perceived benefits), obstacles to performing the health behavior and related negative aspects (perceived barriers), and internal and external factors that trigger the health behavior (cues to action). Self-efficacy, which refers to the confidence that one can perform the recommended health behavior, was not directly asked as a question, but emerged as a theme. For the purpose of this study, we developed the interview guide and piloted among male internal staff prior to the study interviews.
Data Analysis
The audio recordings were transferred to a password-protected computer and encrypted hard drive and were transcribed by a company that offers professional transcription services (https://rafflestranslation.com.sg/). Transcripts were then checked against their corresponding audio recordings and imported to NVivo (Version 12, QSR International) to organize the data. Two researchers (H.X.L. and Z.H.C.) conducted the analysis deductively using the HBM and following the six phases of thematic analysis guide by Braun and Clarke (2006). Specifically, the researchers first read the transcripts repeatedly to familiarize with the data and then generated initial codes from the transcripts independently. These codes were next discussed between the researchers and collated into potential themes, with data relevant to each potential theme gathered. To ensure credibility, codes were deliberated between H.X.L., Z.H.C., and M.F.-F.C. and consensus was reached after several iterations. Data saturation was considered to have been achieved when no new themes were identified. Following this, checks were conducted to ensure that the themes work in relation to the coded extracts and then the entire data set, so that a thematic “map” of the analysis can be generated, using the HBM as a guide (Figure 1). The specifics of each theme were refined, such that clear definitions and names for each theme were generated. Finally, compelling extract examples were selected and analyzed in relation to the research question when writing up the manuscript.

Themes and Subthemes Using the HBM
The term army was used colloquially by the young men in reference to full-time NS and is prevalent in some quotes in the “Results” section and in Tables 2 and 3.
Results
Of the 260 participants recruited, 33 (13%) participants returned for the 12-month study visit and 26 (10%) participated in the interview. Participants were predominantly Chinese (n = 23, 88.5%), mostly full-time university students (n = 24, 92.3%), and half (n = 12, 46.2%) were middle-income and below. At recruitment, their mean age was 20.6 ±1.2 years, mean BMI was in a healthy range of 22.7 ± 2.1 kg/m2, and mean WC was 77.1 ± 7.4 cm. At the 12-month study visit, mean BMI was 22.5 ± 2.0 kg/m2 and mean WC was 78.0 ± 6.9 cm. The mean change in weight from the recruitment visit to 12 months post full-time NS was −0.6 kg, whereas the mean change in WC was +0.9 cm (Table 1).
Demographic Characteristics of Young Men (N = 26).

Note. BMI = body mass index; NS = National service; SGD = Singapore dollar.
HDB: Owner-occupied public housing built and sold by the Housing and Development Board Phang and Wong (1997).
Key themes that emerged were aligned with the six constructs of the updated HBM, whereas the subthemes helped provide structure to the larger and complex themes.
Perceived Susceptibility to Weight Change Post-NS
More than half the number of participants (n = 15, 57.7%) reported a perceived gain in weight after the transition, whereas a few (n = 4, 15.4%) reported a perceived loss in weight. Contrary to perceptions, a decrease in actual weight was observed in more than half of the participants (n = 16, 61.5%). The others had some weight gain (n = 6, 23.1%) or had no change in weight (n = 4, 15.4%).
Perceived Factors Influencing Weight Change
When asked about factors contributing to their perceived weight change, participants reported that lifestyle changes after leaving full-time NS, particularly in relation to changes in diet and exercise-related PA levels were primary factors. In line with Caspersen et al.’s (1985) definition, exercise-related PA is a subcomponent of PA.
Changes in Exercise-Related PA
A decrease in PA levels was commonly cited as a key factor. Most participants reported a decrease in PA levels after leaving full-time NS and mentioned that they felt less fit in their current lifestyles compared with during NS. As reported by a participant, “. . . after [transitioning out of full-time NS], I can see my physical fitness drop quite drastically.” Many participants mentioned that their current lack of exercise-related PA contributed to weight gain, as reported by one, “Definitely exercising less as compared to when I was in army” and mentioned by another, “I don’t really exercise anymore—like on a daily basis, but uh I would still like . . . have basketball training twice a week.” Conversely, some participants felt that their lack of exercise-related PA contributed to weight loss instead, as remarked by one participant, “because you don’t workout . . . so like you lose muscle mass, so like you become lighter.”
Participants also reported engaging in different forms of exercise-related PA post full-time NS. These PA were generally of lower intensity and with a greater emphasis on recreational exercises. As mentioned by a participant, “now it’s more of playing games and sports rather than carrying heavy loads.” In contrast, a few reported engaging in higher levels of exercise-related PA, resulting in them gaining weight gain through bulking up: “I was like uh gymming . . . so I like want to gain more muscle all these, yeah so the weight increase lah [sic].”
Changes in Diet
Dietary changes were a common determinant of weight change, with many participants attributing the consumption of unhealthy food to weight gain following their transition out of full-time NS. Several participants reported poorer diet quality with the inclusion of “more processed foods” and “more fatty foods” in their diets. As described by one participant, “now it’s like a lot of potato chips, a lot of maybe ice cream . . ., and then if it’s at home then it’s easy to grab . . . it’s very easy to uh gain.” Another participant described, “Definitely more processed food, yeah. For example, mala (chilli) then they will use all the Maggie noodles (instant noodles) those type of things and luncheon meat (sic).” Furthermore, a few mentioned that they had less restriction on their food choices, with the freedom to “just eat anything [they] want.” Some suggested that an increased in food intake caused their weight gain, as reported by one participant, “I gain a bit of weight because I was eating a lot more.” A few attributed a decrease in their food intake to weight loss. Interestingly, several participants highlighted the idea of energy input versus output in influencing weight change. They emphasized that a delicate balance was required between one’s diet and PA level, and consuming more than the amount one was expending would lead to weight gain. As explained by one participant, “I eat more than like the amount that I exercise so of course, that would lead to me gaining weight.”
Other Factors
Stress was also reported to play a secondary role in affecting both PA levels and diet. Some felt that stress in their lives led them to “eat more food,” while a few mentioned that stress lowered their motivation “to do anything.” Some participants reported that the higher stress levels came from their studies, for example, having to meet assignment timelines, post full-time NS, while a few cited that their current stress took a different form from that during full-time NS. As reported by a participant, “this stress is different lah [sic]. It’s more self, there’s more independency.” It appeared that to some, the stress came from having to take responsibility of certain life choices instead of depending on instructions from an authoritative figure.
Perceived Severity and Consequences of Weight Change
When asked whether weight changes would affect or had affected them, most participants were indifferent about the consequences of their weight change, saying that they had “never really thought about it” or that it was “not really a concern.” Some participants felt that the effects of their current lifestyle were still reversible, as noted by a participant, “I lose and gain weight quite easily so I am not overly concerned.” A few considered future health repercussions from excessive weight gain but were currently not too concerned, “maybe when I get older, probably all the health problems start to creep in.” Surprisingly, one individual perceived that the consequences of weight change was a necessary and acceptable trade-off with achieving academic goals: “I feel that the trade-off was necessary with um decrease in time span and exercising and the intensity of physical training, so I can fully focus on my studies.”
Perceived Benefits and Barriers to Adopting a Healthy Lifestyle
We explored participants’ perceived benefits and barriers to adopting a healthy lifestyle. The barriers were generally classified into three subthemes: (a) personal factors, (b) social factors, and (c) environmental factors (Tables 2 and 3).
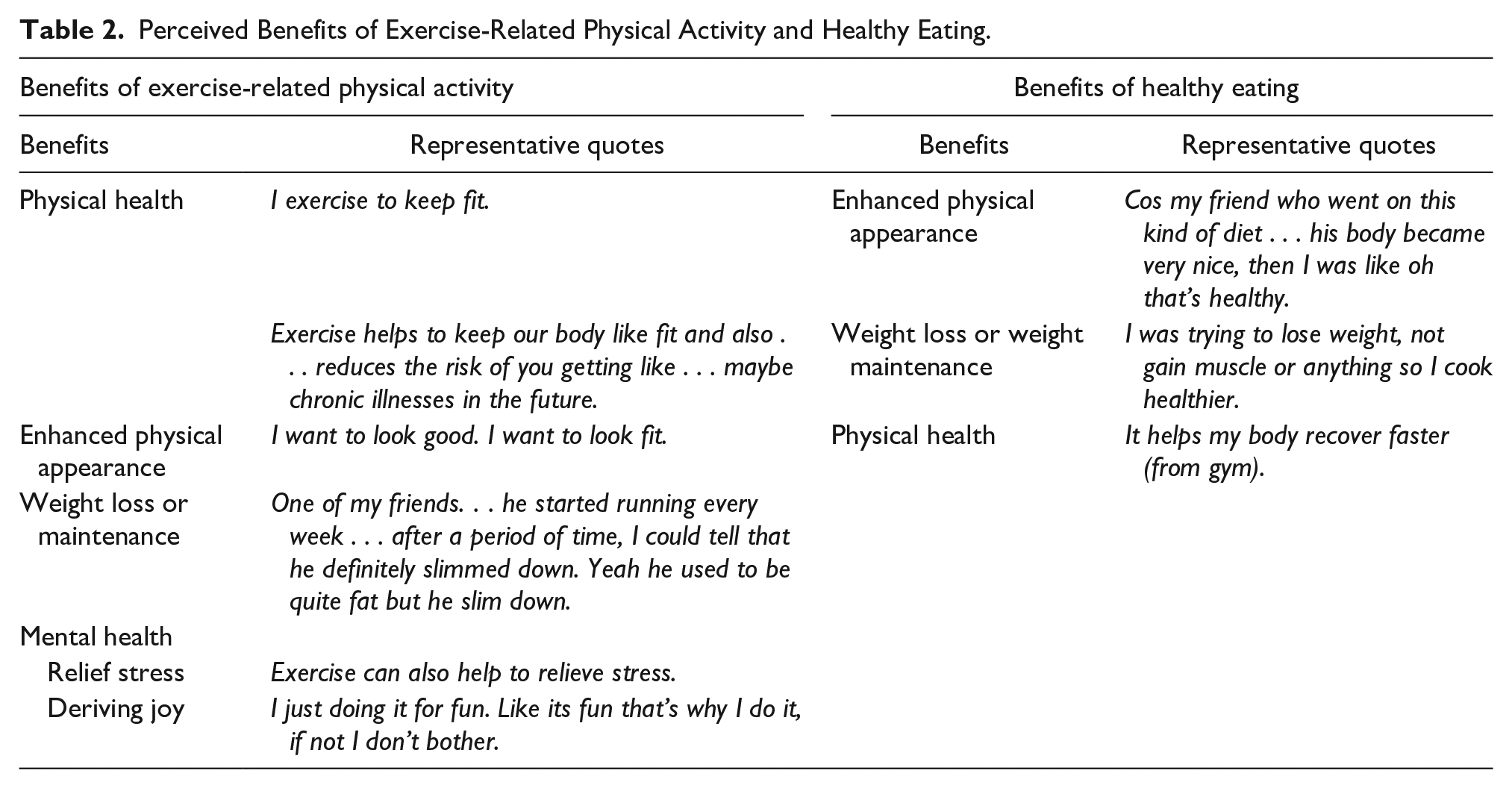
Perceived Benefits of Exercise-Related Physical Activity and Healthy Eating.
Barriers and Motivators of Exercise-Related Physical Activity and Healthy Eating.

Condos refer to condominiums, a form of private housing.
Perceived Benefits of Exercise-Related Physical Activity and Healthy Eating
Most participants were aware of the benefits of regular exercise and were able to list several of them (Table 2). Of these, the beneficial impact on physical health and on physical appearance was most commonly reported. Weight loss or weight maintenance, as well as mental health benefits, such as relieving stress and finding joy in the sport, were other benefits mentioned.
In contrast to PA, fewer participants reported the benefits of healthy eating and fewer benefits were mentioned. Reported benefits centered on enhancing physical appearance, aiding weight loss and/or weight maintenance, and providing physical health benefits.
Perceived Barriers to Exercise-Related Physical Activity and Healthy Eating
Personal Factors
Regarding barriers, personal factors were most frequently mentioned. A substantial number reported that exercise was not a current priority or they found no reason to exercise at this stage in life. As mentioned by a participant, “Like if I have free time, I don’t mind doing it.” Most participants reported having time constraints due to academic work taking precedence over exercising. Some participants reported feelings of “laziness” and tiredness from school or working life, which hindered their motivation to exercise. This was contrasted to time during full-time NS, when physical training was mandatory. As depicted by a participant, “just the motivation (to exercise) not there anymore compared during the (full-time) NS life.”
Similarly, for healthy eating, a number of participants did not view healthy eating to be a priority or need, prioritizing taste over nutritional value. Several participants reported a lack of time to prepare, plan, and cook healthy foods or eat regularly due to the busyness of school. Several participants also reported feeling “lazy” to adhere to healthy eating habits, while a few mentioned that they were unable to curb their cravings for unhealthy food options.
Social Factors
Social factors were also mentioned by some participants to be barriers to exercising and healthy eating. Finding friends with common interests or finding a common time to exercise together was reported to be challenging for several participants. In parallel, a handful of participants mentioned that peer pressure and being compelled to follow their friends’ unhealthy food choices were impediments to healthy eating.
Environment Factors
Environmental barriers also played a role. A few participants cited a lack of convenience in accessing sports facilities, while several reported limited availability of healthy food options when dining out, easy access to unhealthy food options, and higher prices of healthy foods as barriers to healthy eating (refer to Table 3 for related quotes).
Cues to Action
There were internal and external factors that triggered behaviors related to exercise-related PA and healthy eating and they were generally classified into three subthemes: (a) personal factors, (b) social factors, and (c) environmental factors. Related quotes can be found in Table 3.
Personal Factors
A majority of participants cited intrinsic motivators such as taking genuine interest in a sport and achieving their goal of passing mandatory fitness tests as internal factors that drive their exercise-related PA. Personal factors also motivated healthy eating in some participants such as an individual’s habit of cooking healthy foods regularly and a personal distaste for unhealthy foods. Interestingly, several participants reported displaying compensatory behavior by eating healthily to compensate for their lack of PA and/or unhealthy food choices. As explained by a participant, “Because if I don’t do anything about my physical change, like activity, maybe I can do something about my diet.”
Social Factors
Social influence from peers or family was also a strong external factor motivating PA levels, which was reported by many. A few participants commented that their food choices were largely influenced by peer pressure and/or their family’s choice of food. As mentioned by a participant, “When they (friends) encourage us to eat more healthily, then we will feel more motivated to do.”
Environment Factors
A few participants reported being more willing to exercise with the knowledge of sports facilities nearby, while others reported easy access to healthy foods as cues to eating more healthily. For some, monetary incentive was a useful motivator to exercise, for example, by participating in a health program (refer to Table 3 for related quotes).
Perceived Self-Efficacy
Although not directly elicited from participants, a proportion of them commented on the influences full-time NS had on them. They felt that full-time NS had helped increased their mental strength and taught them ways to exercise. As mentioned by a participant, Army let me see what I might look like physically with more exercise, so if I had not gone to the army, then I wouldn’t have seen all those changes. . . I wouldn’t be as motivated to exercise as I did not exercise regularly prior to enlistment. . .
Another participant commented, “There are certain exercises that you picked up along the way in the army, like uh how to do certain static exercises. I never did static exercises before I enlisted, but now I do.” However, there was little or no mention of full-time NS influencing their subsequent diet and sleep habits.
Discussion
Guided by constructs of the HBM, this qualitative study explored factors, barriers, and motivators influencing perceived weight change and tracked body weight changes in a group of Asian young men 12 months post full-time NS. Many of them thought they had gained weight following the transition out of full-time NS and attributed this to decreasing PA levels and increasing consumption of unhealthy food. Despite the perceived weight gain, many did not display immediate concerns. Also, knowing the benefits of regular exercise-related PA and healthy eating did not lead them to prioritize the healthy lifestyle, citing reasons of time constraints, inertia to comply, or lack of access to sports facilities and healthy food options. Motivators toward a healthy lifestyle tended to be internal factors, while external motivators included peer or familial influence and environmental factors.
Many young men perceived that they were more susceptible to weight gain after leaving full-time NS and attributed it to lifestyle changes that occurred post full-time NS. They reported engaging in less exercise-related PA and indulging in more unhealthy food post-NS, compared with during full-time NS. This concurs with findings from the Millennium Cohort Study whereby moderate-to-vigorous activity declined significantly in those who were discharged than those who were still in the military (−17.8 percentage points vs. −2.7 percentage points; Littman et al., 2015). In addition, a Finnish study revealed that conscripts (Mage = 20.7 years) tended to favor fast food, soft drinks, and beer in their free time (Bingham et al., 2009) and the consumption of vegetables was low during leave days, reflecting a penchant for energy-rich, nutrient-poor foods in off-duty conscripts. Some young men in the study also alluded to stress-induced eating, which is not an uncommon factor contributing to the development of obesity (Torres & Nowson, 2007).
Contrary to perceptions of weight gain, slight decreases in actual body weight and BMI and increases in waist circumferences (WC) were observed in our group of young men. Studies have demonstrated that a lack of PA can result in weight loss due to decreased muscle mass (Manini et al., 2007), whereas high WC has been associated with reduced PA levels (Du et al., 2013; Stewart-Knox et al., 2012) and unhealthy food choices (Bermudez & Gao, 2010; Duffey et al., 2012). This is of concern as WC is an established risk indicator for future cardiovascular diseases, particularly in Asians compared with Caucasians.
Of greater concern is the indifference young men in this study showed toward the consequences of their perceived weight gain. Mendis et al. had similar findings, whereby Australian young men (n = 30; aged 17–25 years) at an increased risk of developing chronic diseases (WC ≥ 94 cm) were nonchalant of the consequences of weight gain, citing that weight gain was not an issue “that affected them personally at this stage of their lives.” Moreover, some Australian young men believed being overweight was normal and acceptable, citing added advantages associated with a big build (Mendis et al., 2014). It appears that physical appearance is a primary concern for many young men, a finding that was also reflected in our study.
Indeed, consistent with studies examining men’s perspectives of health behaviors (Ashton et al., 2015; Walsh et al., 2009), the young men in our study reported the value of regular exercise on mostly benefiting their physical appearance (e.g., looking good and fit) and physical health (e.g., reducing future chronic illness). Interestingly, only a few expressed the value of healthy eating and among those who did, the focus was to aid weight loss and enhance physical appearance. Taken together, these findings resonate with studies relating hegemonic masculinity with poorer health behaviors, such that in aligning with masculine ideals, men tend toward valuing exercise for building muscles and controlling weight, whereas healthy eating was associated with being less “macho” (Connell & Messerschmidt, 2005; Eisler, 1995; Young & White, 2000). This emphasis on body image by young men may not be surprising given that body image concerns has increased over the past few decades (Kelly et al., 2015).
Understanding barriers to certain lifestyle choices in this pivotal period of adulthood is critical to informing relevant interventions for young men and helping them develop healthy lifestyle habits for the future. This study identified the main barriers to engaging in exercise-related PA were personal factors such as not viewing exercise as a priority, time constraints, and exhibiting inertia to resume routine exercise. These findings concur with results from earlier studies that young men generally experienced a lack of time, motivation, and commitment to exercise regularly (Ashton et al., 2015; Chiu et al., 2016; Mendis et al., 2014; Walsh et al., 2009). Busy lifestyles among young men such as a full class schedule, work, and social activities (Walsh et al., 2009) resulted in the prioritization of these obligations over PA. Social and environmental factors further compound this problem, adding to existing barriers.
Our findings are congruent with findings from earlier studies whereby discouragements from friends and family, a lack of people to exercise with (Chiu et al., 2016), and family upbringing tapered toward a sedentary lifestyle (Ashton et al., 2015) hindered PA. Environment barriers such as costs of gym memberships, difficult access to different sporting activities (Ashton et al., 2015), and lack of sporting facilities (Chiu et al., 2016) were also not uncommon in deterring young men from exercise-related PA. This highlights the importance of creating readily-accessible and reasonably-priced sports facilities to cater to this age group. Perhaps incentives in the form of subsidized gym memberships would be a viable initiative to spur young men toward engagement in regular exercise-related PA (Mendis et al., 2014).
Largely similar to PA, the drive to eat healthily was impeded largely by personal factors. The belief that healthy eating was not a priority or need and a prioritization of taste over nutrition were main personal barriers. This finding coincided with an earlier study that reported young men (aged 18–24 years) disliked the taste of fruits and vegetables (Walsh et al., 2009), hence being a huge deterrent to eating healthily. Taste ranked the top factor influencing food choices over factors like nutritional value among adults in both an American (Glanz et al., 1998) and Singaporean study (Tham, 2011), highlighting that nutritional concerns were of a lower priority compared with taste when making food choices. Furthermore, the perceived effort required to adhere to healthy eating patterns regularly was also a huge deterrent (Ashton et al., 2015). Similar to earlier studies reporting that young men have insufficient time to plan, shop, prepare, and cook healthy meals (Ashton, Hutchesson, et al., 2017; Munt et al., 2017), the young men in our study reported time constraints as another major barrier. With insufficient time to cook healthy meals at home, most young men would resort to eating out. However, environmental factors such as lack of access to healthy food (Ashton, Hutchesson, et al., 2017; Tham, 2011) and higher costs of healthy foods (Ashton et al., 2015; Tham, 2011) then become barriers to healthy eating.
This study identified that cues to action or motivators to exercise-related PA and healthy eating were mostly due to internal factors, followed by external factors. The current findings are consistent with earlier studies that reported that the feeling of accomplishment in learning and developing new sports skills (Ashton et al., 2015) was a huge driver of PA. Previous meta-analyses have revealed that mastery-approach goals were generally positively associated with performance attainment (Hulleman et al., 2010; Van Yperen et al., 2014), supporting the notion that the desire to achieve certain levels of fitness standards can often drive PA. This relates to intrinsic motivation, a concept aligned with the self-determination theory (Ryan & Deci, 2000), which suggests that people are driven by a need to grow and gain fulfillment. This refers to gaining mastery over challenges and taking in new experiences to develop a cohesive sense of self and engaging in activities for the inherent rewards of the behavior itself rather than external rewards. Similarly for diet, internal factors such as personal preferences and palates were reported and supported by earlier studies that men are more likely to select food based on “habit” and “taste” than women (Glanz et al., 1998; Walsh et al., 2009).
External factors such as peer or familial influences also encouraged the engagement of exercise-related PA. A British study revealed that adults (aged 22–51 years) felt compelled to exercise when committed to a team because of the expectations of others (Edmunds et al., 2013), concurring with findings from this study whereby more than half of young men reported the importance of peer influence on their exercise regimen. Monetary incentives also appeared to entice young men to do more exercise in this study. This observation is supported by a study that revealed young adults and men were more likely to prefer receiving financial incentives over older people and women in health behavior studies (Giles et al., 2016). Mendis et al.’s study also revealed that young men were more receptive to gym memberships than cash incentives (Mendis et al., 2014) perhaps because gym memberships addressed the issue of the high costs of these memberships and provided motivation to exercise, especially if a group of friends received these gym vouchers together.
Social influences driving healthy eating were also reported and supported by previous findings (Ashton et al., 2015; Munt et al., 2017). This is not surprising considering that eating is a “national obsession” in Singapore and a means of socializing with friends and family (Tham, 2011). Interestingly, many were motivated to eat healthily as a form of compensation for the lack PA and/or unhealthy food choices. This behavior, known as compensatory health behavior, may be detrimental long-term as they do not “effectively compensate for all negative effects” of the unhealthy behavior (Amrein et al., 2017; Knäuper et al., 2004). Hence, addressing these misconceptions is imperative.
Implications for Research and Practice
This study shows that there remains a need to educate our young men on misconceptions about certain lifestyles and health and tailoring healthy lifestyle programs to address their motivators and barriers to facilitate behavior change. This study observed that NS increased young men’s self-efficacy in exercise-related PA. This alludes to the potential for NS to provide knowledge and skills training in health behaviors to this group of young men, so as to prepare them for leaving the structured environment of full-time NS. Besides teaching effective and time-efficient exercises for postarmy life and the importance of nutrition and making diet decisions, NS could facilitate opportunities for these men to pursue recreational sports, which they can continue post-NS, as well as opportunities to practice making healthy food choices.
In addition, this study has revealed that weight and BMI alone may not be useful indicators of adiposity in young men. Instead, monitoring WC changes may be more indicative of changes in body composition and increased adiposity, at least in the short term. An emphasis on the prevention of weight gain, particularly increases in WC, through information platforms preferred by young adults, for example, social media, may be an alternative way of promoting health in this age group.
Strengths and Limitations
Strengths of the current study include being the first to investigate and establish barriers and motivators influencing lifestyle in young men transiting out of a highly regulated environment of full-time NS in a multi-ethnic Asian context. The methodology of using in-depth interviews instead of focus groups ensured freedom of expression without being conscious of others in a social setting. However, it is acknowledged that our findings may be subjected to recall bias as participants were asked to recall changes to their lifestyle behaviors from 12 months ago. Other limitations include sampling bias as the majority of our participants were university students (92.3%) and of Chinese ethnicity (88.5%), and thus our results may not be generalizable to young men in other professions and of other ethnicities. Following up these participants in the future, through conducting longitudinal interviews, will be valuable to provide deeper insights into how these young men have adapted to their transition out of full-time NS in the longer term.
Conclusion
Guided by the HBM, this qualitative study uncovered drivers of lifestyle behaviors related to exercise-related PA and healthy eating among young men as they transit out of full-time NS in an Asian context. Aligned with concepts from the HBM, our findings are valuable in informing health promotion strategies and interventions in this generally hard-to-reach group and young people in general. Mitigating key barriers and enforcing key motivators would enable better transition out of full-time NS or other types of military service not only in the Asian context, but may also be applicable to countries that have short-term mandatory training for their citizens. Further research can be conducted to better understand weight changes in young men over a longer period of time post full-time NS or after leaving military service.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883221074788 – Supplemental material for Transiting Out of Full-Time National Service: A Qualitative Study of Barriers and Motivators of Weight Change in Young Adult Men in Singapore
Supplemental material, sj-docx-1-jmh-10.1177_15579883221074788 for Transiting Out of Full-Time National Service: A Qualitative Study of Barriers and Motivators of Weight Change in Young Adult Men in Singapore by Mary Foong-Fong Chong, Hui Xian Lim, Beverly W. X. Wong, Zi Han Chi, J. K. Inthujaa, Falk Müller-Riemenschneider, Bobby K. Cheon, Alexander W. Gorny and Kee Seng Chia in American Journal of Men’s Health
Footnotes
Acknowledgements
We would like to thank the participants for their contribution to this study. We would also like to thank Ms. Chan Yong Jiet, Mr. Jarrett Tan, and Dr. Leong Wai Siang for their help in the recruitment logistics for this study.
Availability of Data and Materials
The data sets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
This study was conceived and designed by M.F.-F.C., A.W.G., and K.S.C. Data were collected by H.X.L. and J.K.I. H.X.L. was a research staff (BSc) and J.K.I., an undergraduate intern during the research period. Transcripts were checked by H.X.L. and Z.H.C. Analyses were conducted and interpreted by H.X.L., Z.H.C., and M.F.-F.C. The manuscript was drafted by M.F.-F.C., H.X.L., and B.W.X.W., with input from F.M.-R, B.K.C., A.W.G., and K.S.C. The final manuscript was reviewed and approved by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was internally funded by the Saw Swee Hock School of Public Health, National University of Singapore, under its War of Diabetes Seed Fund. The funders had no role in study design, data collection and analysis, or preparation of the manuscript.
Ethics Approval and Consent to Participate
This study was given ethical approval by the National University of Singapore’s Institutional Review Board (Reference Code: B-16-290 and Approval Number: NUS 3290). The authors declare that written informed consent was obtained from all participants. This method of consent was approved by the NUS IRB.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.