
Abstract
Mexican-origin men are at increased risk of developing non-alcoholic fatty liver disease (NAFLD). The purpose of this qualitative research was to assess Mexican-origin men’s knowledge and cultural attitudes toward NAFLD and their interest in risk reduction. Semi-structured interviews were conducted with 11 Spanish-speaking Mexican-origin men who were considered high-risk of having NAFLD according to transient elastography (FibroScan®) continuous attenuation parameter (CAP) scores (≥280). Audio recordings of these interviews were transcribed and interpreted in their respective language to facilitate data analysis using NVivo 12. A thematic codebook was developed, from which the research team identified emerging themes. Findings demonstrated limited knowledge about NAFLD and in general chronic liver disease among Mexican-origin men. Cultural attitudes appeared to both enhance and mitigate their perceived risk for NAFLD. Interviews also revealed high interest levels for reducing NAFLD risk, with family and loved ones acting as the main motivators for engagement in healthier behaviors. Inclination toward family-based interventions was reported as a subject of interest for this high-risk population. This qualitative study suggests that the development of a NAFLD-specific intervention approach for Mexican-origin men may be feasible and should consider a familial and cultural context centered in improving lifestyle health behaviors.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is a metabolic disorder that has been identified as the most common form of chronic liver disease in the United States with an estimated prevalence of 24.1% in the general population (Kallwitz et al., 2015; Younossi, Anstee, et al., 2018; Younossi et al., 2019; Younossi, Koenig, et al., 2016). The NAFLD spectrum progresses from benign buildup of fat in the liver to severe liver tissue inflammation and damage (non-alcoholic steatohepatitis [NASH]) to liver cirrhosis (Byrne & Targher, 2015; Chalasani et al., 2018). NASH is currently the second most common cause of hepatocellular carcinoma (liver cancer) in the United States across all populations (Charlton et al., 2011; Fazel et al., 2016). As with many other chronic diseases, obesity status is a crucial contributor to NAFLD, and refined carbohydrate consumption and physical inactivity have been highlighted as prime risk factors (Byrne & Targher, 2015; Rich et al., 2018; Younossi, Anstee, et al., 2018). Given the rising trends of obesity in the United States, it is expected that NAFLD will become the leading cause of liver-related morbidity and mortality in the United States by the year 2030 (Estes et al., 2018; Marcellin & Kutala, 2018). Currently, the annual economic burden in the United States of direct medical costs related to NAFLD is estimated to be about $103 billion (Kallwitz et al., 2009; Younossi, Blissett, et al., 2016).
Hispanic and Latino individuals, who currently comprise about 17.8% of the U.S. population and possess the highest rates of obesity (Daviglus et al., 2014), have demonstrated to also have a high prevalence of NAFLD (Kallwitz et al., 2009; Rich et al., 2018; Williams et al., 2011). Mexican-origin men in particular exhibit the highest NAFLD rates of any U.S.-based racial/ethnic group (Agbim et al., 2019; Akinkugbe et al., 2018; Fleischman et al., 2014; Lazo et al., 2015; Weston et al., 2005; Williams et al., 2011) with an estimated incidence rate of 29.6% versus 20.5% for non-Hispanic White men and 16.3% for non-Hispanic Black men (Lazo et al., 2013, 2015). Among Hispanic and Latino subgroups (Cuban, Puerto Rican, Dominican, and South and Central Americans), men of Mexican origin have among the highest suspected prevalence of NAFLD based on elevated aminotransferase levels (Fleischman et al., 2014; Kallwitz et al., 2015). Among older Mexican-origin men in the United States, liver cancer ranks as the second leading cause of death (American Cancer Society, 2018; Le et al., 2017; Paik et al., 2019; Venepalli et al., 2017; Younossi et al., 2015).
Given the heavy burden of NAFLD among people of Hispanic decent more generally and Mexican-origin men in particular, it is critical to implement strategies to reduce NAFLD risk in this population. Modifiable factors such as healthy eating and increased physical activity have been previously identified as the areas of priority for interventions focused on NAFLD given their potential to slow and even reverse early stages of the disease (Agbim et al., 2019; Younossi, Loomba, et al., 2018). Lifestyle interventions focused on weight loss, including changes in diet and physical activity, for Hispanic men are reported to be feasible and effective when they are appropriately tailored for gender and culture (Garcia et al., 2019). However, there are currently no qualitative studies that address how Mexican-origin men understand NAFLD and its associated health risks that could inform the development of NAFLD-specific prevention and intervention strategies targeted at this extremely high-risk population.
This article aims to assess Mexican men’s knowledge related to NAFLD, the cultural and gender factors they believe impact their NAFLD risk, and their interest in risk reduction. This article is based on qualitative semi-structured interviews among a subsample of Mexican-origin men who participated in a cross-sectional population study in Southern Arizona. We posit that the promotion of culturally tailored NAFLD interventions could have an important impact on the reduction of NAFLD among Mexican-origin men in the United States.
Materials and Methods
Participants and Setting
Participants were recruited from a cross-sectional population study designed to identify the prevalence of NAFLD in a community-based sample of Mexican-origin adults in Southern Arizona from May 2019 to March 2020. Briefly, during the recruitment and informed consent process, participants obtained basic information on NAFLD risk factors and the implications of developing and living with NAFLD. Participants then completed questionnaires related to demographics and personal health information in their preferred language (English or Spanish), completed anthropometric measurements, provided a cheek swap for DNA collection, and completed transient elastography (FibroScan®) as part of a clinical visit. The first author (E.A.V.) of this article was responsible for obtaining written informed consent and performed clinical visits of all male participants in this cross-sectional study. This ensured gender and cultural appropriateness and strengthened the trusting relationships between research staff and participants. After the clinical visit, participants were contacted via telephone to conduct two weekdays and one weekend 24-hr dietary recall administrated by University of Arizona Cancer Center’s Behavioral Measurement and Interventions Shared Resource (BMISR). All research activities were approved by the University of Arizona Institutional Review Board (#190238078).
Qualitative interviews were conducted among a subpopulation of participants who successfully completed all activities of the cross-sectional population study. The purpose of the qualitative arm of this study was to engage more deeply with participants surrounding their experiences of study participation with the intent to draw conclusions that could be applied to the development of culturally congruent NAFLD prevention and intervention programs.
Eligibility criteria for qualitative participants included that they (a) speak Spanish; (b) identified as having NAFLD, according to their FibroScan® continuous attenuation parameter (CAP) scores (≥280 dB/m) (Karlas et al., 2017); and (c) self-identify as first-generation Mexican immigrants according to results of the Acculturation Rating Scale for Mexican Americans II (ARSMA II) (Cuellar et al., 1995). Participants received an explanation about the qualitative interviews during their clinical assessment visit and provided written consent to be contacted if they met eligibility criteria for these interviews. A total of 104 men completed all study-related activities for the cross-sectional study. From this sample, 27 eligible men were contacted on a rolling basis starting September 2019 to determine their interest in completing the interview. Participants completed interviews over a time frame of 1 week up to 3 months after the completion of their dietary recalls. Due to the onset of the COVID-19 pandemic, a total of 11 interviews were conducted before the close of data gathering in early March 2020. While the resulting sample size was slightly smaller than anticipated, research has identified that a sample size of 12 or even smaller can be sufficient in cases where the conversations are in-depth and where the sample population is homogeneous, as was the case in this study (Boddy, 2016). Figure 1 provides a visualization of a participant flowchart for men who completed interviews that serve as the basis for the present qualitative assessments.
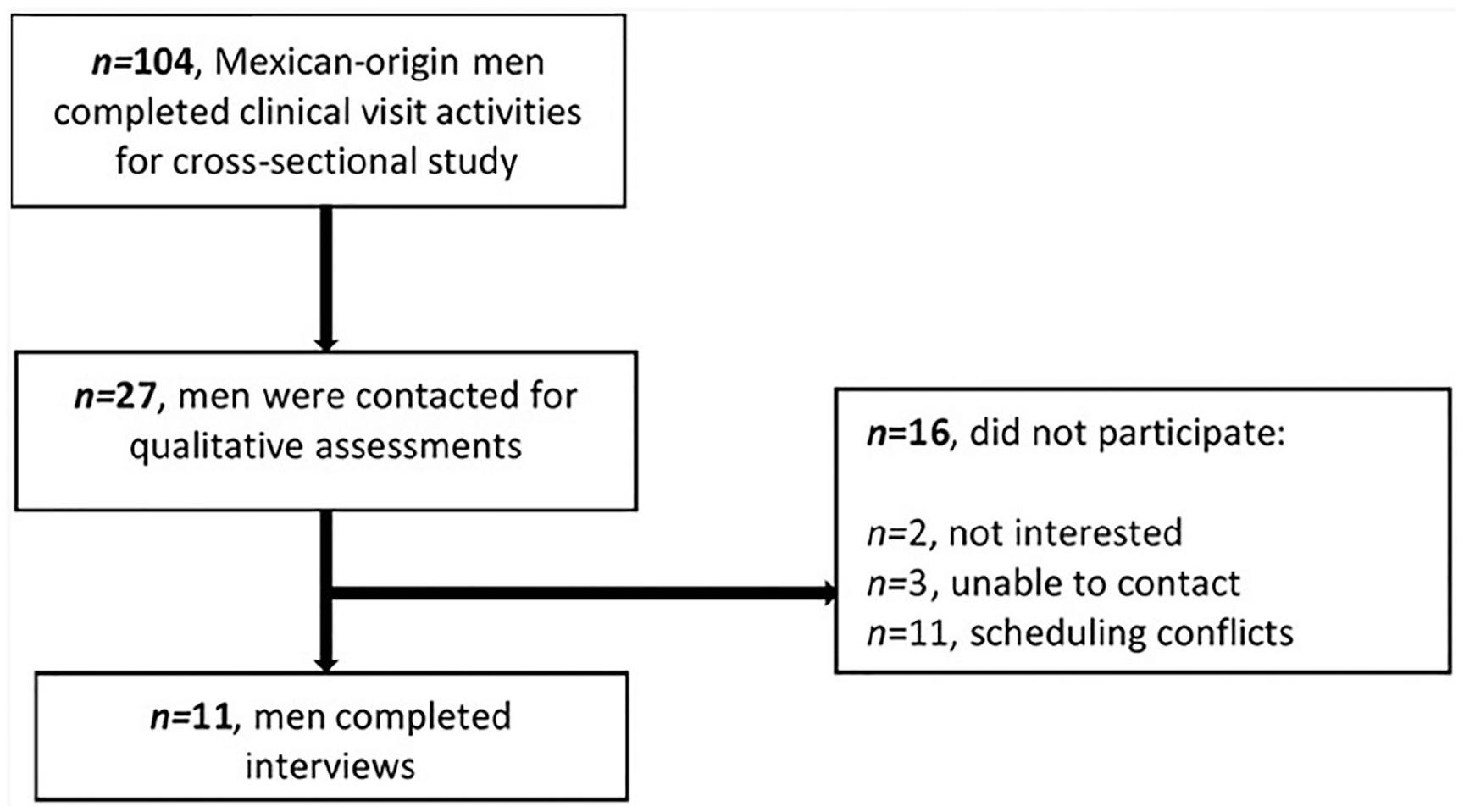
Participant Flowchart for Qualitative Assessments.
Data Collection
Individual in-depth interviews were conducted in Spanish with 11 Mexican-origin men using a semi-structured interview guide (Supplemental Material). These interviews were scheduled according to participants’ preferred days/times and conducted by the first author (E.A.V.) who identifies as a bilingual Mexican-origin male. Interview sessions lasted approximately 60 min, and participants were compensated US$25 for their time. All interviews took place in a private room at the University of Arizona’s Collaboratory for Metabolic Disease Prevention and Treatment.
Data Analysis
Interviews were audio-recorded and transcribed in their original language to facilitate data interpretation. The first and second author (R.M.C.) conducted data analysis using a directed thematic analysis approach in which they identified thematic patterns from the interview data. Coders developed a primary codebook where broad themes from the used moderator guide were included as major categories. Coding procedures also included a constant comparison methodology where arising themes in the data were discussed by the coders and added to the codebook when appropriate. During this process, coders observed that data saturation had been reached as relevant conceptual categories emerged (Dworkin, 2012). Collapsed data highlighted the following broad themes: (a) limited knowledge related to NAFLD health risk, (b) cultural and gender influences on NAFLD risk, (c) high interest in NAFLD risk reduction, and (d) recommendations for an NAFLD-specific intervention. Selected quotes include participants’ age and an alias name for participant confidentiality purposes. The coders utilized NVivo 12 (QSR International) software to facilitate and conduct data management and analysis.
Results
Participant demographic characteristics (n = 11) of this foreign-born sample are reported in Table 1. The sample’s mean age was 46.3 ± 9.5 years, ranging from 30 to 61 years of age, and the mean weight and body mass index (BMI) were 102.8 ± 12.7 kg and 33.3 ± 3.2 kg/m², respectively. Five participants (45.5%) reported a yearly family income of <US$29,999 and eight (72.7%) reported attaining a high school education or less. Only five (45.5%) participants reported having access to a primary care provider and six (54.5%) reported having health insurance coverage. Five men (45.5%) reported being hypertensive and only one (9.1%) participant reported being diabetic.
Participant Characteristics of Spanish-Speaking Mexican-Origin Men.

Qualitative Analysis Results
The preliminary results presented in this article highlight the following themes: (a) limited knowledge related to NAFLD health risk, (b) cultural and gender influences on NAFLD risk, (c) high interest in NAFLD risk reduction, and (d) recommendations for an NAFLD-specific intervention. The following segments present these results with selected participant quotes to facilitate interpretation of these findings.
Limited Knowledge Related to NAFLD Health Risk
It was a common experience for study participants to have learned about NAFLD for the first time during recruitment and study consent process for the cross-sectional study. Eight men of this subsample expressed a lack of knowledge of NAFLD before their participation. Pedro, a 58-year-old participant, stated, “First of all I did not know anything before this [the cross-sectional study], anything. I did not know what NAFLD was. Nothing, nothing, nothing.” In addition, a small number of men (n = 3) had basic and limited knowledge about NAFLD that was introduced to them through family and friends. Overall, participants had an incomplete understanding of the disease, its implications for overall health status, and NAFLD’s heavy impact on the Mexican-origin community. Subsequently, slightly more than half (n = 6) reported that participation in the cross-sectional study increased their knowledge and awareness of the disease.
Those who stated having prestudy knowledge about NAFLD had generally acquired that information from family members and internet sites and mostly lacked in-depth or specific knowledge. When asked whether he knew what NAFLD was before this cross-sectional study, Elias (age 61) answered, “In a way, I already knew about it. My mother is a caregiver so all the time ‘como cuchillo de palo’ [meaning through constant repetition], advising us about our diet.” Others, like Fernando (age 44), had received information from sources outside the family. He said, “Well . . . on the internet, it talks about fatty liver, it talks about some other diseases such as hepatitis, but I don’t know if fatty liver is the same as hepatitis or if it is something different.” Even in cases where participants had family history of fatty liver (n = 4), men lacked specific knowledge and awareness of the disease. Pedro (age 58) shared, “. . . I believe that a brother of mine died of that [NAFLD] because the doctors told him, but he did not believe it.”
Even among this small sample of Mexican-origin men, there was a wide variety of perceptions of possible risk factors for NAFLD, although most study participants expressed low levels of knowledge related to risk factors. When referring to factors that would put someone at a higher risk of developing NAFLD, David, a 42-year-old participant, stated, “I have no idea to be honest. I do not know if it is due to my diet or if it is through genetics, I have no clue.” Of note, although the moderator guide did not include questions related to alcohol consumption nor did the cross-sectional study beyond screening for consumption to assess NAFLD, some men assumed that alcohol was still a primary risk factor, which largely stemmed from having family members or friends who had suffered from cirrhosis. Jesus (age 51) described, I had previously heard about [liver disease] from my family members who said that they had experienced some repercussions. But most of those who suffered from those types of symptoms were specifically in the case of alcohol. So, from alcohol, drugs, and this is what I think carries some repercussions that in one way or another caught up with them and affected them.
A minority of men correctly identified that NAFLD could afflict individuals who are not overweight or heavy drinkers, a notion that was acquired after their participation in the cross-sectional study. Josue, a 37-year-old male, shared, “Yeah, well, this disease basically does not depend much on your physical composition. Honestly, I used to think that this only happened on people who drank . . . or to chubby people.” The role of NAFLD as a risk factor for other chronic and metabolic disorders was also mentioned by six (n = 6) participants. As Pedro (age 58) concluded, “. . . other diseases could be avoided, other diseases that come with fatty liver that can be prevented. With this we can prevent it before it turns into something more serious. Many, many diseases can be prevented.” Only one sample participant (1/11) reported substantial knowledge of NAFLD risk factors that he acquired from college acquaintances: “Well, it has to do with the intake of greasy foods and sugar excess while its risk is magnified in people with obesity and overweight. It can also be promoted by genetic agents” (Luis, age 30).
Cultural and Gender Influences on NAFLD Risk
Participants shared several ideas about how their Mexican culture affected health in the areas of nutrition, family and gender dynamics, and attitudes toward self-care and medical care and medications. These factors may serve to both increase and, in some cases, mitigate risks for developing and managing NAFLD.
Most men (n = 10) considered the traditional Mexican diet to be healthier than the conventional American regimen because it incorporates more fresh vegetables and salads in meals. Participants also concluded that the conventional American diet tended to include more fats and fast foods compared with Mexican diets, which was tied to the fact that Mexicans generally prefer to cook and eat at home. Therefore, consuming and adopting a Westernized diet was linked by participants as a risk factor to being unhealthy. For example, José (age 45) stated, Well, I think that the majority [of Americans] eat a lot of food on the street while we, well it [our food] is made at home. It seems to me that it is healthier to eat at home than someone who says they eat out.
Several men said that the quality and selection of ingredients, cooking practices, and portion sizes were also important indicators of the nutritional status of a meal. In some cases, participants determined that Mexicans had a health advantage in these areas. For example, David (age 42) said, I think that Hispanic food is healthier because it has way fresher vegetables and the way to prepare it. Also, for example, what Hispanics do is, and I do not know if Americans do, but we have a lot of vegetable soups and in vegetable soup is where all the vitamins go. Another thing is the type of seasoning that is used is rather more natural, it does not come with so many chemicals, salts and with so many things like that.
In other instances, participants (n = 6) recognized that certain elements of Mexican cultural eating habits—particularly large portion sizes—were potentially harmful to health and therefore to NAFLD risk reduction. As Fernando (age 44) described, We Mexicans eat our food and I think that the problem is in the portion sizes, in the quantity, because that is what we do, but I don’t know if it is because we like to eat well or because we eat a lot, I don’t know.
A few participants (n = 3) tied this lack of portion control to the demands of their physical labor, restricted time during the workday, and the unique needs of men for eating more. For example, Jose (age 45) shared, “I think that men should eat a little more than women because women are mostly at the house, or I don’t know. But you do exercise more [as a man] at work and all that.”
Participants in this sample of Mexican-origin men also identified individual and social barriers to healthy behaviors commonly associated with cultural and gender norms. Pedro (age 58) emphasized, Many times [spouses] want to be accommodating, and they give us like five tortillas. They think they are helping us, but they are not helping us. You have to cut the amount a little, just one, because nobody is going to help you more than yourself.
Fernando (age 44) also noted, “I think that if I want to take care of myself with a meal that truly only benefits me, and only me, then I would need to make my food separately.” These cultural and gender dynamics were recognized by some participants as barriers to the adoption of healthier behaviors and weight management.
Some men noted culturally informed attitudes toward health care use and self-care that could influence how they would respond to NAFLD or other health risks. Some of the men reported uneasiness about taking medications and visiting the doctor. This concept is crucial when intending to reduce barriers to early screening and detection of NAFLD. For instance, Elias (age 61) visited his primary care physician in Mexico after the cross-sectional study visit and stated his preference for adopting a healthier lifestyle over taking medical treatment: The doctor told me I had two options. He tells me, “I think you can have a lab treatment, or you can get on a diet.” I told him, “You know, I prefer to go on a diet, I don’t need the medicine.”
Fernando (age 44) also recognized his preference for preventive measures that would spare him the need for medical interventions down the line: If it is about risk, and if there is risk for me to develop it [NAFLD] or if it would affect my health and I need to go to the emergency room or something, if I will get to that, then I prefer to take better care of my health now.
Over half the sample (n = 7) highlighted the importance of caring for their bodies by improving their eating habits, increasing physical activity, and maintaining other healthy behaviors to reduce NAFLD risk and thereby avoid the future need for health care. Rafael, a divorced 53-year-old man, highlighted self-care as a crucial component of being healthy: . . . you must be proactive with your organism. There are people who do not care or have someone. I have already lost everything. I am alone right now, so I must take care of myself. And you know, if I don’t take care of myself, who is going to take care of me?
Elias (age 61) also shared how important it is for him and his partner to improve their eating patterns due to the different comorbidities that they have: My wife, what does she not have? She has diabetes, high blood pressure, suffers from arthritis so constantly I tell her, “We have to take care of each other, you because of all the things you have and I because of what little I have.” So, I keep telling her that we have to take better care of what we eat.
High Interest in NAFLD Risk Reduction
Participants expressed high levels of interest in reducing their overall risk of NAFLD. Here, we explore the changes that study participants were making as a result of participation in the cross-sectional study and their motivators for adopting healthier behaviors.
According to self-reported statements collected during the interviews, all sample participants (n = 11) incorporated changes to dietary habits and almost half (n = 5) increased their physical activity levels in response to study participation. Participants shared that obtaining new information during the cross-sectional study inspired them to adopt healthier behaviors moving forward, such as eating better quality foods and engaging in more leisure time physical activity. About one third of the men (n = 4) sought out help from other health care providers after participating in the cross-sectional study due to feeling concerned about their health status.
Several participants indicated that participating in the study and obtaining the free FibroScan® allowed them to consciously improve the way they perceive their health by changing their eating routine and limiting certain major food groups like fats, added sugars, and red meat consumption. One participant said, “I can’t correct the past, but when you gave me those results. . . believe me, my diet has changed, and I went to get treated.” (Josue, age 37). Another man shared that his participation in the study resulted in him changing his dietary behaviors and taking action to consult with his doctor regarding his long-term cholesterol issues. His doctor responded with surprise: . . . he said, “what are you doing?” he says, “your cholesterol is in the best shape. . . Your cholesterol and your glucose status are exceptional. Your bad cholesterol,” he says, “is in a normal range, different from and much lower than what you previously had.” (Jesus, age 51)
Three participants reported having achieved significant weight loss from the time of their initial visit in the cross-sectional study to the time they participated in the interview (between September 2019 and March 2020). For instance, Jesus (age 51) shared, I realized that I had to change many areas, in the way I eat and in my sedentary habits. And then I started following through and thank God I’m seeing that there have been results. Right now, I went and weighed myself and I think I already have lost almost 26 pounds.
Another participant said, “I am working and I am seeing results. But like I told you, I lost like 35, 30, 35 pounds. I used to weigh 245, right now I am around 200, about 210” (Pedro, age 58). This finding indicates that an early detection and screening of NAFLD and education might be a viable element to consider in the development of NAFLD risk reduction strategies for Mexican-origin communities.
Regarding motivations for change, many participants (n = 7) indicated that their family and loved ones were their primary inspirations for engaging in healthier behaviors related to NAFLD risk reduction. Josue emphasized the importance of being there for his children in the long-term: Maybe I am very extreme because when you see something is failing, all my attention goes there. Why? Because I want to live a little longer for my children. I want to be there when they get married, when they leave for college—not in that order right?—but I do want to be there for them. So, I do want to take care of myself.” (Josue, age 37)
Meanwhile, Hector (age 51) stated, . . . “it doesn’t matter that much to me if I die,” the Mexican says. “So what?” Right? “That is what I was born for.” But if someone tells me, if we change the strategy and they tell me: “Look, if you die, your son will need you.” That is how they open your eyes a little more. “Yes, it is true.” So that’s where I am going to become aware. It is not so much what affects me, but what affects my family. I love my family very much, that’s why I’m saying for me, I would love for the family to be involved [in a program/intervention], because there is a total change, right? The Mexican always thinks “I don’t matter, my family matters.”
When men were asked specifically about their interest in participating in an NAFLD-specific intervention centered on weight loss and the promotion of healthy lifestyle behaviors, all men (n = 11) expressed interest. For example, Josue (age 37) stated, Of course, as I said if this information can help others, we can save I don’t know how many lives or prevent diseases. Let’s say, increase the life span of Latinos or even the Anglos. I don’t know . . . That way we can spend a little more time with our children.
Similarly, all 11 study participants stated being interested in attending cooking classes designed to improve nutritional intake and promote weight loss. David (age 42) said, Yes, I would like that for my health . . . if you or your assistants could teach me how to eat well, healthy, I would be willing to, honestly. Because I do lack a little of knowledge in that area, and I have many, I have many, many doubts . . . if you could help me, it would be the best thing that happened to me.
Elias (age 61) explained, I think [healthy eating] is important for our lives. Because we can avoid many things, like diseases. I come back to the same point, if we share, if we can share with more Mexican Latinos and we can share with them a way to educate ourselves [about how to prepare] our meals, that’s it, we can avoid a lot of diseases.
Recommendations for NAFLD-Specific Interventions
In this final section, we present what the participants seek to gain from future NAFLD-specific interventions and their guidance on components that they would like to see in such interventions.
When asked about their preferences for how interventions should be organized and oriented, participants (n = 11) stated an interest in involving the whole family in intervention approaches to generate a more holistic impact on the family unit. These responses reflected cultural and gender norms such as familismo that encouraged them to prefer more family-oriented approaches. Hector (age 51) responded the following after being asked about familial involvement: “Well, I think it would be more beneficial if it could be with my partner, the family, right? Involving the family because it is a change for everyone.” Luis (age 30) also emphasized on familial involvement due to the significance of social and cultural environments within Mexican homes when he shared, “Yes, because there are some obesogenic factors that have to do with our family environment.”
In addition, most of the men (n = 8) expressed that they believed the intervention should be tailored specifically to a Mexican-origin audience and reflect relevant cultural, social, and gender norms. Rafael (age 53) provided a detailed explanation when describing the dynamics of implementing healthy behaviors as someone coming from Mexico to the United States: It is a very serious problem [to adopt a healthy lifestyle] because the Mexican lifestyle here [in the U.S.] is not the same thing as over there [in Mexico]. There is no time, no time. We don’t rest well, we don’t balance [foods] well, and the information on, “oh you should you eat this or that,” does not work because they don’t tell people why.
Fernando (age 44) also described the importance of food culture in the Mexican household when sharing his perceptions on why participating in an intervention for Mexican-origin adults would help him with improving his eating behaviors, ` the things that we, our people “nuestra raza” has is the habit of, if you’re going to eat, you’re going to eat and go hard at it! And often it’s not good because you eat more than your body needs. So that is what I think our biggest problem is.
In terms of recruitment, some men noted that reaching male participants would pose an additional challenge. For example, Elias (age 61) stated, “. . .men need a lot of time investment. Women do not need as much. Women are a little more adventurous than men.” Meanwhile, Luis (age 30) said, Yeah, the subject of health is going to matter more to men than the aesthetic aspect. He has less social pressure than women, who have much more social pressure, especially in the north [of Mexico], northern women are much more socially pressured to be thin.
Discussion
Studies centered on Mexican-origin individuals related to NAFLD are scarce. At the same time, obesity and type 2 diabetes trends continue on the rise (National Center for Health Statistics, 2016; Rodríguez & Campbell, 2017), positioning this population at an even more elevated risk of NAFLD (Agbim et al., 2019; Daviglus et al., 2014; Lazo et al., 2015). This analysis explored concepts related to Mexican-origin men’s knowledge and information about NAFLD, their cultural perspectives, and interest in taking action to reduce NAFLD risk following by recommendations toward future interventions. Findings evidenced low levels of knowledge and awareness of NAFLD in this high-risk community-based sample of Mexican-origin men. Less than one third of the interviewed participants demonstrated even a limited understanding of NAFLD or liver disease, and what information they did have come from informal sources including family, friends, and internet searches. Similar results were reported in Mexican-origin women as part of a sequential analysis from this same cross-sectional study (Morrill et al., 2021). Most participants were also unable to identify common risk factors for NAFLD and shared a common misperception regarding alcohol consumption as being the prime risk factor for all liver disease, a finding supported by previous work with Mexican adults in the United States and in Mexico (Flores et al., 2012, 2018).
Mexican-origin culture emerged as an important component of men’s perceived risk of NAFLD. Participants shared different concepts in how being of Mexican decent may both increase and lessen their risk of developing and managing NAFLD. Almost all men agreed to their dietary regimen being healthier than the conventional Western diet due to the quality and selection of ingredients and cooking practices performed predominantly by their domestic partners. Indicators of acculturation such as frequent “eating out” or adopting high calorie dense diets were deemed as damaging for overall health status. However, men also described large portion sizes, family eating pressures, norms of masculinity, and demands of strenuous work routines to be impediments to healthy lifestyle choices for traditional Mexican households. Previous studies centered in Hispanic males and their perceptions related to healthy behaviors encountered similar socioenvironmental barriers (Garcia et al., 2017; Larsen et al., 2014; Valdez et al., 2019). Some of the men also expressed their lack of routine and preventive health screening procedures unless they experienced some sort of medical emergency. Interestingly, NAFLD was identified by participants as a risk factor for other chronic diseases. This could open the pathway for health communication strategies centered for NAFLD prevention that could motivate behavior changes for other health outcomes.
A pervasive finding from this study was the men’s high level of interest in mitigating their NAFLD risk. Participants were motivated about taking care of their physical health by adopting healthier eating patterns and increases in leisure physical activity to improve their health and reduce their risk of developing NAFLD and other chronic diseases. In fact, all interviewed participants reported the incorporation of changes in dietary habits due to the brief delivery of health information provided during their participation in the cross-sectional study. Participants’ main motivation to engage in healthier behaviors derived from their family, loved ones, and particularly their children—a known embedded concept in Mexican culture (Ahluwalia et al., 1999). All men also shared being interested in taking part in an NAFLD-specific intervention that would primarily focus on weight loss and the promotion of healthy lifestyle behaviors. What is more, despite reticence to engage with medical services, after learning about their high steatosis scores, a subsample of participants consulted further medical assistance as a concern about their liver health status arose after receiving the FibroScan®.
Another notable theme was the appeal of the entire family unit to partake in this intervention to produce a larger impact among all home members. Mexican-origin men appear to be more likely to participate in prospective studies that would help them reduce their risk of NAFLD via weight management and improving dietary components if involvement from their support system at home is incorporated within the model of a culturally appropriate intervention. The promotion and awareness of liver health and the adoption of healthy lifestyle choices appear to collectively be a feasible avenue to address the burden of NAFLD in Mexican-origin adults. Strategies targeting familial involvement in Hispanic men engaging in healthy behaviors have demonstrated to be promising in terms of recruitment, and for partaking in future programs or interventions (Ahluwalia et al., 1999; Garcia et al., 2017; Valdez et al., 2017).
Given the scarcity of research on this topic and the heavy burden of NAFLD among Mexican-origin men (Agbim et al., 2019; Akinkugbe et al., 2018; Fleischman et al., 2014; Lazo et al., 2015; Rich et al., 2018; Williams et al., 2011), the literature suggests a clear need for more research exploring the disproportionate effects of liver disease and risk reduction factors among Mexican-origin men (Flores et al., 2012, 2018). Future programs and interventions should acknowledge and capture cultural components in their models to promote a more practical adoption of healthy behaviors and utilization of health care services by underserved populations. Non-invasive procedures such as transient elastography are reliable screening options that should be available to these populations as a routine preventive measure for chronic liver disease (Kanwal et al., 2021).
Strengths and Limitations
The main strength of this study includes the participation of a hard-to-reach and high-risk population for NAFLD. In addition, the approach of having a male bilingual/bicultural staff member responsible for research activities increased the cultural congruency of these interviews. The study also had some limitations. For instance, measuring participants’ response to the cross-sectional study was hindered by the variations in time elapsed between completing their clinic visit and participating in the semi-structured interview. These variations presented differences in participants’ levels of effort to implement lifestyle changes or to follow-up with a health care provider following study participation. Similarly, the onset of the COVID-19 pandemic limited the number of participants for these qualitative assessments. However, as previously mentioned, data saturation was reached. Finally, the fact that health information related to liver disease was provided to participants during recruitment and the informed consent processes challenged our ability to discern their exact levels of knowledge related to NAFLD prior to study participation.
Conclusion
This qualitative study broadens our understanding of NAFLD-related knowledge and attitudes within a highly understudied and at-risk population of foreign-born Mexican men in the United States. Further research should be focused on recognizing and understanding the opinions and views of Mexican-origin men as these may contribute to informing best practices for educating and alerting this population about the potential consequences of living with chronic liver disease. In addition, lifestyle and weight loss interventions centered on cultural norms and families could enhance participation in clinical research in this area for this high-risk population.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883211063335 – Supplemental material for A Qualitative Analysis of Mexican-Origin Men’s Knowledge and Cultural Attitudes Toward Non-Alcoholic Fatty Liver Disease and Interest in Risk Reduction
Supplemental material, sj-docx-1-jmh-10.1177_15579883211063335 for A Qualitative Analysis of Mexican-Origin Men’s Knowledge and Cultural Attitudes Toward Non-Alcoholic Fatty Liver Disease and Interest in Risk Reduction by Edgar A. Villavicencio, Rebecca M. Crocker and David O. Garcia in American Journal of Men's Health
Footnotes
Acknowledgements
The authors acknowledge salary support by the University of Arizona Health Sciences Center for Border Health Disparities for R.M.C. We also would like to acknowledge our clinical partner, Arizona Liver Health, for providing space for our clinical study visits and for conducting all liver FibroScans® as well as the University of Arizona Collaboratory for Metabolic Disease Prevention and Treatment for the space to complete the semi-structured interviews.
Author Contributions
E.A.V., R.M.C., and D.O.G. were involved in conceptualization; E.A.V. and R.M.C. were involved in formal analysis; D.O.G. was involved in funding acquisition; D.O.G. was involved in investigation; D.O.G. was involved in supervision; E.A.V. was involved in writing—original draft; E.A.V., R.M.C., and D.O.G. were involved in writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Cancer Society (Institutional Cancer Research Grant number IRG-16-124-37), the National Institute on Minority Health and Health Disparities under award number K01MD014761 (Garcia), and the University of Arizona Health Sciences Center for Border Health Disparities.
Ethics Approval
All study procedures were approved by the University of Arizona Institutional Review Board (IRB #1902380787).
Informed Consent Statement
Written informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.