
Abstract
Non-Hispanic (NH) Black, American Indian/Alaska Native (Indigenous), and NH-White men have the highest colorectal cancer (CRC) mortality rates among all other racial/ethnic groups. Contributing factors are multifaceted, yet no studies have examined the psychometric properties of a comprehensive survey examining potential masculinity barriers to CRC screening behaviors among these populations. This study assessed the psychometric properties of our Masculinity Barriers to Medical Care (MBMC) Scale among NH-Black, Indigenous, and NH-White men who completed our web-based MBMC, Psychosocial Factors, and CRC Screening Uptake & Intention Survey. We conducted exploratory factor analysis on a sample of 254 men and multivariate analysis of variance (MANOVA) on a separate sample of 637 men nationally representative by age and state of residence. After psychometric assessment, the MBMC scale was reduced from 24 to 18 items and from six to four subscales. NH-Black men’s mean scores were lowest on three of four subscales (Being Strong, Negative and Positive Attitudes) and highest on the Acknowledging Emotions subscale. Compared with both Indigenous and NH-White men, NH-Black men had significantly lower Negative Attitudes subscale scores and significantly higher scores on the Acknowledging Emotions subscale. Compared with both Indigenous and NH-Black men, NH-White men had significantly higher Being Strong and Positive Attitudes subscales scores. This study expands on previous research indicating that, among racialized populations of men, endorsement of traditional masculine ideologies influences engagement in preventive health behaviors. Our scale can be tailored to assess attitudes to screening for other cancers and diseases that disproportionately burden medically underserved populations.
Keywords
Colorectal cancer (CRC) is the third leading cause of cancer death in the United States, with one in 23 men and one in 25 women being diagnosed with CRC in their lifetime (Siegel et al., 2020). Numerous studies document an increased prevalence of CRC among men from racial and ethnic minority groups such as non-Hispanic (NH) Black and American Indian/Alaska Native (Indigenous) (Bray et al., 2018; Catchers & Doubeni, 2020; Ellis et al., 2018; Rawla et al., 2019; Siegel et al., 2020; Williams et al., 2016). In the general population, men are approximately 1.5 times more likely than women to develop CRC (Bray et al., 2018; Rawla et al., 2019; Siegel et al., 2020). While CRC incidence rates are comparable for men and women aged under 45 years, in the 55- to 74-year age group, incidence rates for men are 40%–50% higher than for women (Siegel et al., 2020). Due to both higher morbidity and mortality from CRC and a higher likelihood of diagnosis at an advanced stage of disease, it has been recommended for more than a decade that NH Black populations be screened for CRC beginning at age 45 rather than age 50 (Agrawal et al., 2005; Rex et al., 2009).
CRC incidence and mortality among men vary substantially by race and ethnicity. Notably, NH Black and Indigenous men have the highest incidence rates and lowest survival at all stages of CRC (Rawla et al., 2019; Siegel et al., 2020). Incidence and mortality rates are 1.24 and 1.47 times higher, respectively, among NH Black men as compared to NH White men (American Cancer Society, 2019; DeSantis et al., 2017), while NH Black men have the lowest 5-year CRC survival across all racial/ethnic and sex subgroups (DeSantis et al., 2019; Murphy et al., 2011; Rogers et al., 2020). Among Indigenous men, CRC incidence and mortality rates are 48.5% and 19.4% higher, respectively, than among NH White men. CRC prevalence at all subsites is higher for Indigenous mean compared with other male racial and ethnic groups (American Cancer Society, 2020; Murphy et al., 2011; Siegel et al., 2020).
Screening for CRC reduces mortality by detecting the disease at an earlier and more treatable stage; however, only 62.4% of adults aged 50–75 years are current on CRC screenings (Muthukrishnan et al., 2019; White et al., 2017). Screening rates in this age group are lowest among Indigenous people at 48.4%, while the rate for NH Blacks is 59.3% (White et al., 2017). Social determinants of health such as socioeconomic status and access to quality health care play an important role in completion of CRC screening (White et al., 2017). Importantly, screening rates for the uninsured and those without a usual source of health care are approximately 25.1% and 26.3%, respectively (White et al., 2017). Due to poor funding, Indian Health Service (IHS) facilities struggle to adhere to annual testing and follow-up colonoscopies, limiting patients’ opportunities to receive these services (Muthukrishnan et al., 2019). CRC screening barriers specific to Indigenous culture include perceived medical discrimination and mistrust, inadequacies in culturally attuned education and preventive practices, and barriers of language and geography (Daley et al., 2012; Filippi et al., 2013; Schumacher et al., 2008).
Among NH Black men, who have the highest CRC mortality among all racial/ethnic groups, extensive patient-level factors, masculine role norms, and medical mistrust are key in determining CRC screening behaviors (DeSantis et al., 2019; Rawl et al., 2019; Rogers et al., 2017). Institutional, systemic, and interpersonal racism and medical system mistrust are additional barriers to Black men’s completion of CRC screening (Atakere & Baker, 2016; Green & Kelly, 2004; Powell et al., 2016; Rogers & Goodson, 2014; Rogers et al., 2017). The impacts of systemic racism on NH Black men may prevent them from seeking health care from predominantly White institutions with ongoing racist practices (Powell et al., 2016). Although homophobia is not unique to the NH Black community, it has been identified as another barrier to the completion of both invasive CRC screening and adherence to the digital rectal exam for prostate cancer detection (Beeker et al., 2000; Hennelly et al., 2015; Winterich et al., 2009). Stronger identification with “Black culture” has been reported to correspond with higher cancer screening rates (Atakere & Baker, 2016), while multiple studies have investigated the importance of familial and social-support networks in achieving higher screening rates among NH Black men (Brittain et al., 2012; Fish et al., 2015; Rogers et al., 2017).
Numerous survey-focused studies have evaluated CRC screening uptake (Brittain et al., 2012; Green et al., 2004; Muthukrishnan et al., 2019), including the Male Role Norms, Knowledge, Attitudes, and Perceptions Associated with CRC Screening (MKAP-CRCS) tool developed by Rogers et al. (2018). The MKAP-CRCS exhibited high internal consistency among a sample of 157 NH Black men aged 19–45 years, yet this instrument was developed specifically to examine factors associated with CRC screening disparities in NH Black men via an adaptation of two other scales: the Male Role Norms Inventory–Short Form (MRNI-SF), developed by Levant et al. (2013) to determine perceptions of male norms among male and female undergraduates, and a 16-item test developed by Green and Kelly (2004) to examine NH Black men’s knowledge of CRC incidence, myths, symptoms, and screening methods. Use of the MRNI-SF is limited by the assumption that all questions can be applied across all sociogeographical contexts (Rogers et al., 2018), as well as by a small sample size and demographic variables uncharacteristic of the general Black population in the United States. Although the MKAP-CRCS is psychometrically sound, some participants withdrew prematurely from the questions disapproving sexual minorities, suggesting a need to further explore this phenomenon.
The Present Study
Although Rogers et al. (2018) previously examined the psychometric properties of the MKAP-CRCS, to our knowledge no studies have been designed specifically to examine the psychometric properties of a comprehensive survey examining masculinity barriers to CRC screening and medical care among NH Black, Indigenous, and NH White men, the three populations with the highest CRC incidence and mortality among all racial/ethnic groups and both genders (American Cancer Society, 2019; Bray et al., 2018; DeSantis et al., 2017; Murphy et al., 2011; Rawla et al., 2019; Rogers et al., 2020; Siegel et al., 2020). The first phase of this study used an online sample of diverse male groups (NH Black, Indigenous, and NH Whites participants aged 18–75 years) across the United States to assess the psychometric properties (specifically, dimensionality and internal-consistency reliability) of the 24-item, six-factor Masculinity Barriers to Medical Care (MBMC) scale (Table 1). Next, a comparison of the average scores of the 24-item scale for the above three population groups was compared with that of a reduced 18-item, four-factor MBMC scale, and the following hypotheses were formulated among the latter’s subscales: (1) Being Strong: Since a higher score means being “stronger” in regard to taking care of family and making health decisions on one’s own rather than consulting doctors for health problems, Indigenous and NH Black men would score higher than NH White men. (2) Negative Attitudes Toward Medical Professionals and Exams: Since a higher score means more negative attitudes, NH Black and Indigenous men would score higher than NH White men. (3) Acknowledging Emotions and Health Issues: Since a higher score means greater willingness to acknowledge emotion and take care of health issues, Indigenous and NH Black men would score lower than NH White men. (4) Positive Attitudes Toward Medical Professional and Exams: Since higher scores means an absence of barriers to seeking health care, Indigenous and NH Black men would score lower than their NH White counterparts.
24-item Masculinity Barriers to Medical Care Scale.

Methods
Participants
We assessed the psychometric properties of the MBMC scale in two samples of men aged 18–75 years residing in the United States—one of 254 men identified by race and a separate sample of 637 men who were nationally representative by age and state of residence and who self-identified as NH Black, Indigenous, or NH White. Between December 2020 and January 2021, in partnership with Qualtrics (Provo, UT), a commercial survey sampling and administration company, we used a consumer-panel approach to recruit participants nationwide from sources including member referrals, targeted email lists, customer loyalty web portals, permission-based networks, and social media.
Measures
Demographics
Participants were asked to indicate their (a) age, (b) current state of residence, (c) marital status, (d) sexual orientation, (e) education level, (f) health insurance status, and (g) family history of CRC, among other demographic variables described elsewhere (Rogers, Goodson, & Obidike, 2018; Rogers, Goodson, Dietz, & Okuyemi, 2018). In the sample of 254 men, most participants identified as straight/heterosexual (n = 233, 91.08%), had health insurance (n = 211, 82.42%), and had no family history of CRC (n = 214, 83.59%); and 42.64% were married (n = 109). In the sample of 637 men, most participants identified as straight/heterosexual (n = 582, 91.37%), had health insurance (n = 505, 79.28%), and had no family history of CRC (n = 471, 73.71%); 40.82% were married (n = 260). Lastly, educational attainment ranged from high school or less (n = 82, 32%) to a bachelor’s degree or more (n = 88, 34%) in the sample of 254 men, whereas educational attainment ranged from high school or less (n = 213, 33%) to a bachelor’s degree or more (n = 216, 33.8%) in the sample.
Masculinity Barriers to Medical Care
The 24-item MBMC scale (Rogers et al., 2019) initially stemmed from modification to five other existing measures that examine masculinity and attitudes and practices that preclude men from seeking health care. Guided by the Theory of Planned Behavior, the authors recruited African American men aged 45–75 years who resided in Minnesota, Utah, and Ohio to 11 focus groups to examine the influence of psychosocial determinants of men’s health on CRC screening completion (Rogers et al, 2020). To improve the scale’s face validity, the authors supplemented the focus groups with cognitive interviews with 10 CRC advocate-survivors across the United States. To improve content validity, they obtained expert item review of the scale by two leaders in Black men’s health and one expert in survey methodology. The updated MBMC scale consisted of six theoretically derived factors: (1) Provider Role, (2) Health-Related Self-Reliance, (3) Health Problem Minimization, (4) Restrictive Emotionality, (5) Fear of Being Perceived as Gay, and (6) Medical Mistrust. For all subscales, individual items were assessed on a 5-point Likert-type scale ranging from 1 (Not at all true) to 5 (Completely true).
Survey Procedures
The Institutional Review Board (IRB) at the University of Utah approved the study protocol (IRB #00113679) prior to data collection. Participants could complete the online survey from any computer or mobile device. The first page of the survey website provided informed consent information; consenting participants clicked “Yes” to be taken to the survey. Next, they were asked to select their preferred method of compensation (e.g., frequent flier miles, points toward retail purchases). The survey began with the aforementioned measures of interest for this current study.
Sample-Size Considerations
We calculated a priori estimates of the sample size needed for the various analyses. For the exploratory factor analysis, we relied on Costello and Osborne (2005), who reported that 62.3% of the factor analyses they surveyed had a participants-per-item ratio between >5:1 and <10:1. A sample size of 240 allowed for 10 participants per item. In addition, we assessed the suitability of the MBMC data for factor analysis. The Kaiser–Meyer–Olkin value was 0.80, which exceeds the suggested value of 0.6 (Kaiser, 1974). Bartlett’s Test of Sphericity (Bartlett, 1954) was statistically significant (chi square = 1938, df = 276, p > .001), further supporting the factorability of the correlation matrix. For the multivariate analysis of variance (MANOVA) tests, we used the dataset of 637 men. We used the G-Power 3.0.10 calculator (Faul et al., 2007) to estimate sample size. Using an effect size of 0.065, α = 0.05, one group, four predictors, and four response variables, the minimum sample size was 118.
Statistical Analysis
Prior to conducting the main analyses, we screened the data for potential missingness, outliers, and normality. We took a listwise deletion approach to address missingness. No data were excluded for missing values. No outliers were identified at the univariate level. At the multivariate level, approximately 14 cases (seven on each end of the spectrum) accounting for data across all items in the MBMC scale were identified as potential outliers. Lastly, an assessment of normality indicated that participants’ data on six items had a probability of skewness ranging from 7% to 41%, whereas only two items had a probability of kurtosis of 55% and 78%.
As part of the exploratory factor analysis, we followed Kahn’s (2006) recommendation to use parallel analysis to determine the number of factors to extract; this was performed using an SPSS macro developed by O’Connor (2000).
We conducted MANOVA tests to determine if there were significant differences in the subconstructs (dependent variables) denoting the MBMC scale across racial and ethnic groups. We also conducted MANOVA postestimation tests to identify the margins of responses by group and the differences between the linear predictions. Lastly, we used Tukey’s post-hoc tests to identify significant differences between racial and ethnic groups on the dependent measures (MBMC subconstructs). From the MANOVA analysis, we report the Wilks’ lambda statistic, eigenvalues, means, standard deviations, and Tukey’s post-hoc coefficients. The data were analyzed using SPSS v. 26.
Results
Exploratory Factor Analysis of MBMC Using the n = 254 Dataset
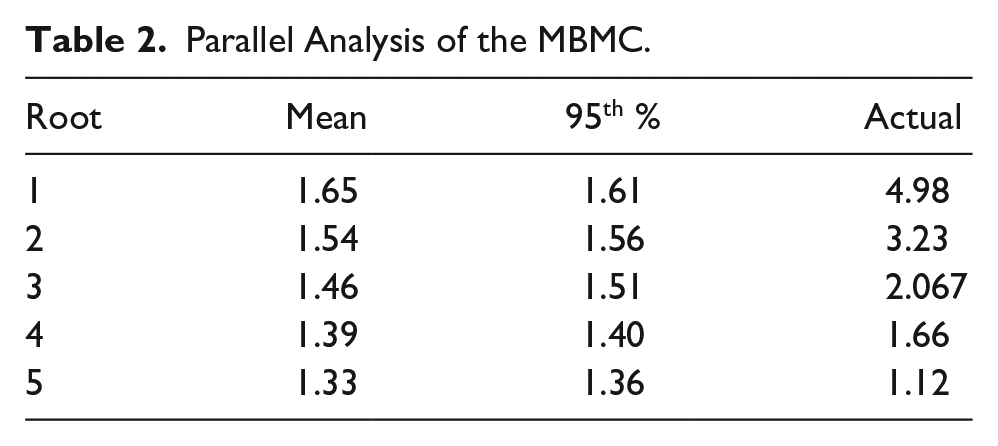
As part of the parallel analysis, we generated 1000 randomized permutations of the MBMC data. We compared the mean and 95th percentile eigenvalues derived from these extensive repetitions with the actual eigenvalues computed from the original raw data to determine the last point at which the actual raw data eigenvalue exceeded either the mean or the 95th percentile eigenvalue (Table 2). The analysis indicated that a four-factor structure best represented the dimensionality of the data and factor five was excluded. We fixed the number of factors to extract at four, as follows: Being Strong, Negative Attitudes Toward Doctors and Exams, Acknowledging Emotions and Health Issues, and Positive Attitudes Toward Doctors and Exams.
Parallel Analysis of the MBMC.
We conducted an exploratory factor analysis of the 24 MBMC items using principal axis factoring (PAF) and Oblimin rotation with Kaiser normalization. This oblique rotation criterion was chosen following Preacher and MacCallum (2003), who emphasized that orthogonal criteria “are rarely defensible because factors are rarely if ever uncorrelated in empirical studies” (p. 40). We set the minimum loading allowable to 0.35, which resulted in the removal of no items. Five items were removed because of cross-loading problems, following Tabachnick’s and Fidell’s (2007) suggestion that items that load 0.32 or greater on a second factor should be removed. One item was removed following Worthington and Whittaker’s (2006) recommendation that items lacking in conceptual interpretability be removed, and two items with cross loadings
Factor Loadings and Intercorrelations From Exploratory Factor Analysis of the MBMC.
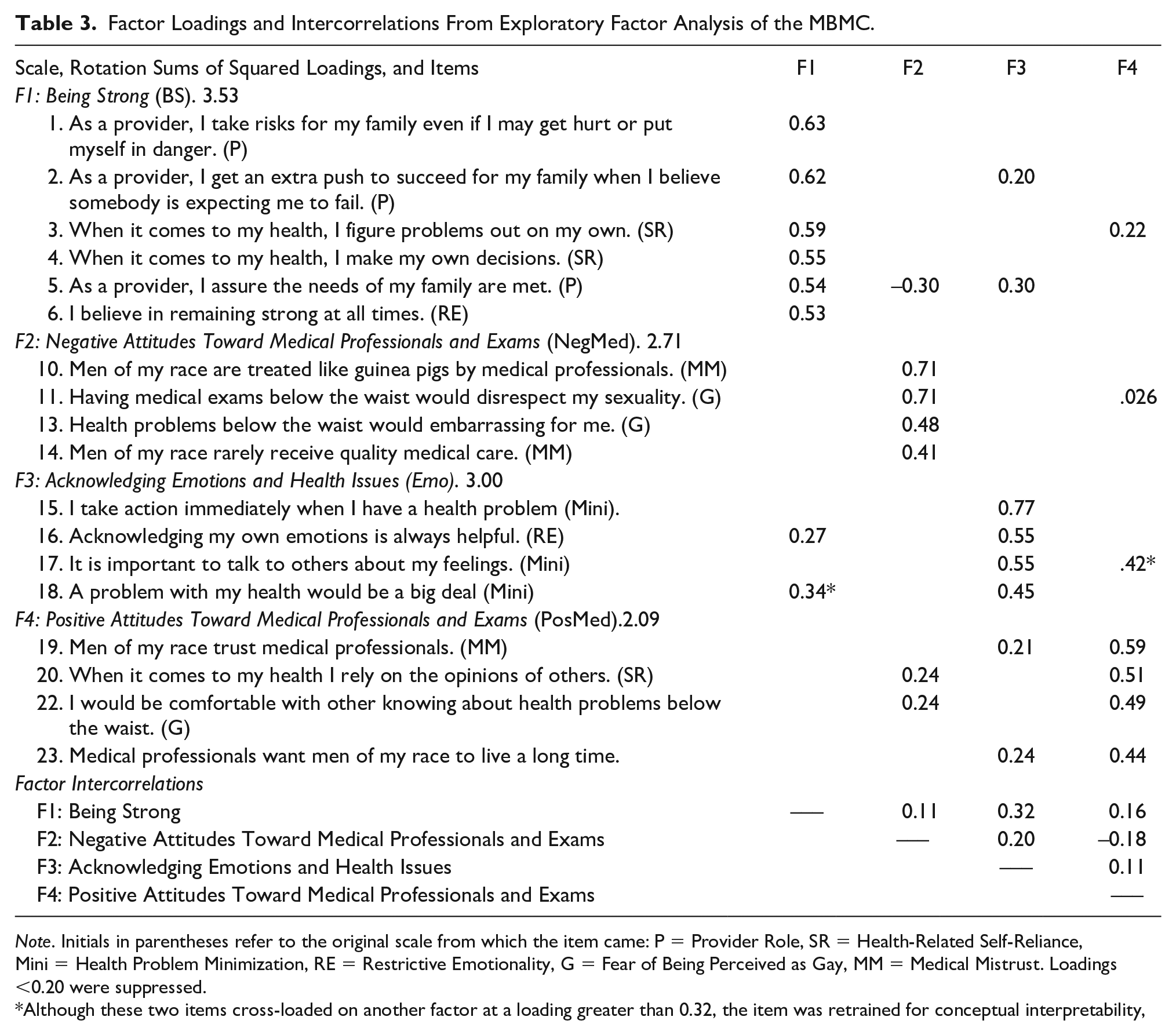
Note. Initials in parentheses refer to the original scale from which the item came: P = Provider Role, SR = Health-Related Self-Reliance, Mini = Health Problem Minimization, RE = Restrictive Emotionality, G = Fear of Being Perceived as Gay, MM = Medical Mistrust. Loadings <0.20 were suppressed.
Although these two items cross-loaded on another factor at a loading greater than 0.32, the item was retrained for conceptual interpretability,
Reliability of the Subscales Using the n = 637 Dataset
We calculated Cronbach’s alpha internal-consistency reliability (alpha) coefficients for the four MBMC subscales, first using only the NH Black men in the sample because that is the group for whom the scale was initially developed; these were: Being Strong (BS), α = 0.75; Negative Attitudes Toward Medical Professionals and Exams (NegMed), α = 0.75; Acknowledging Emotions and Health Issues (Emo), α = 0.76; Positive Attitudes Toward Medical Professionals and Exams (PosMed), α = 0.70. Using the entire sample, which also included Indigenous and NH White men, the alphas were: BS = 0.74; NegMed = 0.69; Emo = 0.71; and PosMed = 0.65.
Comparison of Racial/Ethnic Groups on the MBMC via MANOVA
MANOVA results revealed significant main effects for the MBMC subscales (Wilks’s lambda [8, 1262] = 9.22, p = .001). The proportion of the variance explained in the outcomes (MBMC subscales) by an effect is approximately 10% (~89% unexplained). Additionally, eigenvalue analysis showed two functions, with Function 1 (b = 0.10) accounting for more variance than Function 2 (b = 0.01). As presented in Table 4, on average, NH Black men had the lowest mean scores on three out of four subscales (Being Strong, Negative and Positive Attitudes), but the highest mean scores on the Acknowledging Emotions scale. Tukey’s post hoc means comparison tests showed that NH Black men had statistically significant lower scores compared with both Indigenous and NH White men on the Negative Attitudes subscale and statistically significantly higher scores compared with both Indigenous and NH White men on the Acknowledging Emotions subscale. In contrast, NH White men had statistically significant higher scores on the Being Strong and on the Positive Attitudes subscales compared with both Indigenous and NH Black men. These first three results show contrary outcomes to our first three hypotheses, whereas the fourth result was in line with our fourth hypothesis.
Descriptive and Tukey’s Comparisons for the MBMC Subscales by Racial and Ethnic Group.

Note.
Discussion
The purpose of this study was to ascertain the psychometric properties of the MBMC scale among NH Black, Indigenous, and NH White men across the United States—the three male groups with the highest CRC incidence and mortality (ACS, 2020). Participants who self-identified as NH Black had the lowest mean scores on three of four subscales (Being Strong, Negative and Positive Attitudes) but the highest mean scores on the Acknowledging Emotions subscale. NH Black men also reported on average fewer masculinity barriers on one of four subscales (“being strong” or “negative attitudes”) compared with Indigenous and NH White men. Our findings also suggest that NH Black men experience fewer masculinity barriers in attitudes toward medical professionals and exams. Our findings contrast with prior literature on medical mistrust among this population (Adams et al., 2017; Daley et al., 2012; Haozous, 2020; Powell et al., 2019).
Our study revealed that NH Black men had statistically significantly fewer negative attitudes toward medical professionals and examinations. Compared with their Indigenous and NH White counterparts, NH Black men had the lowest mean scores on this factor, indicating that they experienced the lowest masculinity barriers focused on negative attitudes. These findings were contrary to our hypothesis and prior research on the relationships among masculine role norms, medical mistrust, and engagement in preventive health behaviors such as screening for early detection of CRC in NH Black men (Christy et al., 2017; Earl et al., 2021; Hammond 2010; Nobis & Sanden, 2008; Rogers et al., 2017, 2020). Several studies outline how endorsement of traditional masculinity norms—which value strength, independence, and self-reliance—can result in delaying medical care and reluctance to seek health services, especially among NH Black men (Christy et al., 2017; Hammond 2010; Nobis & Sanden, 2008; Rogers et al., 2017, 2020). Fewer interactions with health-care providers can impede the patient–provider trust-building process, which is essential for reducing medical mistrust barriers (Hammond, 2010; Idan et al., 2020; LaVeist et al., 2009).
Additionally, present-day evidence of racial discrimination offers a key perspective in understanding medical circumspection. Hammond (2010) reported medical mistrust being greater when individuals perceived race-based treatment differences. Numerous studies have demonstrated that heterosexual self-preservation, a characteristic of masculinity, negatively corresponds with engaging in preventive health measures such as CRC screening, which are inherently invasive in nature and induce a feeling of vulnerability (Christy et al., 2017; Getrich et al., 2011; Rogers et al., 2017, 2020; Vandello & Bloom, 2013; Winterich et al., 2009). These previous findings may explain why NH Black men reported fewer masculinity barriers in our study.
NH Black men also had statistically significantly higher differences on Acknowledging Emotions and Health Issues compared with Indigenous and NH White men. On this subscale, higher scores corresponded with fewer masculinity barriers; interestingly, NH Black men reported the highest average scores. This indicates that, compared with their NH White and Indigenous counterparts, NH Black men reported the fewest masculinity barriers on Acknowledging Emotions. These findings are inconsistent with both our hypothesis and the literature on restrictive emotionality among NH Black men. Harris et al. (2011) reported that the behaviors and interactions of a sample of NH Black men attending college were influenced by a critical element of masculinity that involved appearing unemotional and unfazed. Similarly, other studies have demonstrated how placing a high value on masculinity characteristics such as fear of showing weakness and vulnerability are aspects of restrictive emotionality (Christy et al., 2017; Hammond, 2010; Nobis & Sanden, 2008). Because Black men have historically endorsed traditional masculinity norms to preserve their soundness of mind, additional research is needed to better understand why NH Black men in our study reported fewer masculinity barriers to Acknowledging Emotions and Health Issues.
By contrast, our results also showed that, compared with Indigenous and NH Black men, NH White men responded positively to questions about Being Strong that prioritized strength and individualism over the health recommendations of health-care providers or their community. It is plausible that such a result is linked to inequities across subsamples, which have historically disenfranchised NH Black and Indigenous communities and privileged NH white men to attain greater educational levels and access to health care, among others (de Brey et al., 2019; Sohn, 2017). While the relationship between masculinity and health has been explored extensively, further investigation is required of the individual aspects of masculinity that influence medical decision making among racial subgroups. Griffith et al. (2015) suggest that manhood and health are interdependent and that understanding these relationships is crucial to addressing health disparities in NH Black men. Additionally, previous research has demonstrated a positive relationship between the presence of family and social support networks and men’s health-care utilization (Brittain et al., 2012; Fish et al., 2015; Rogers et al., 2017); therefore, an excessive commitment to individualism may play a significant role in masculinity barriers to care. Our results indicated, contrary to our hypothesis, that, compared with Indigenous and NH Black men, NH White men more strongly endorsed Being Strong as a potential barrier to disease screening and care.
Several factors may contribute to our results differing from previous literature. Lack of concordance between the MBMC scale and previous findings concerning the relationship of strength, independence, and individualism to the health-care utilization practices of NH Black men suggest that our scale may not adequately reflect the attitudes of NH Black men, despite a fair Cronbach’s alpha for the subscale Being Strong (α = .75 for NH Black men, α = .74 for all subgroups). Conversely, the attitudes of the men in our sample may have changed during the COVID-19 pandemic, when the data were collected, and these changes may have differed between racial subgroups such that “Being Strong” may now hold different meanings within different communities. Understanding how perceptions of strength and individualism influence health-care utilization among NH Black and Indigenous men may provide critical insights necessary to address significant health disparities, including NH Black men having the poorest CRC survival rates (Rawla et al., 2019; Siegel et al., 2020; White et al., 2017).
Another point to consider is an insight from Gordon et al. (2013), who reported that among young fathers (aged 15–25) of different races, “Whereas the masculine norm ‘toughness’ related to negative health behaviors for these diverse young men, other masculine norms were found to be protective” (para. 25). Recent findings by Levant et al. (2021) suggest that subsets of different age cohorts of men commonly do not endorse “traditional” masculinity ideology, suggesting that future research should further examine how age cohort may be more determinative of masculinity barriers to medical care than age alone.
Finally, our results confirmed that, compared with NH White men, NH Black and Indigenous men were less likely to have positive attitudes about medical providers and institutions providing quality, equitable care. Medical mistrust among NH Black and Indigenous men has been extensively documented (Atakere & Baker, 2016; Daley, 2012; Green & Kelly, 2004; Haozous, 2020; Powell et al., 2016; Rogers & Goodson, 2014; Rogers et al., 2017); our results showed that the MBMC scale exhibited consistent medical mistrust–focused findings among these subgroups, with a fair Cronbach’s alpha for the Positive Attitudes subscale (α = 70 for NH Black men, α = 65 for all subgroups). Reasons for this mistrust among NH Black and Indigenous men include systemic and interpersonal racism, fear of experimentation, and the intrusiveness of procedures, among other factors (Adams et al., 2017; Daley et al., 2012; Haozous, 2020; Powell et al., 2019). This mistrust is compounded by other aforementioned barriers to medical care, including poverty, lack of access to quality health-care services, cultural hurdles, poor health coverage, and lack of transportation (Daley et al., 2012; Filippi et al., 2013; Muthukrishnan et al., 2019; Schumacher et al., 2008). Because medical mistrust results in delayed CRC screening and treatment, particularly for Black and Indigenous men, it is crucial for researchers and medical providers to better understand and validate this mistrust while attempting to rebuild relationships with communities that suffer abuses and prejudicial treatment from the health-care system (Guadagnolo et al., 2009; Haozous, 2020; Powell et al., 2019).
This study is not without limitations. First, on the original unidimensional provider scale, respondents did not clearly perceive that “taking risks” and “having an extra push” were negative. Second, although quota sampling methods and survey weighting were employed to improve cohort representativeness, this web-based survey might not be fully representative of the U.S. population. Third, our participants may have been confused by our vague use of the word “others” for some of our questions. For example, the statement “When it comes to my health, I rely on the opinions of others” is loaded with the two positive medical-professional-specific items (on factor 4 in the four-factor version), suggesting that our respondents may have thought that “others” meant doctors. Third, some of our items were double-barreled (two questions in one), which may have resulted in suboptimal participant responses to the Provider Role subscale. Finally, self-reported data are subject to recall, response, and social-desirability biases.
Conclusion
The MBMC scale was originally conceptualized to include 24 items and six factors. After assessment of the psychometric properties, including dimensionality and internal consistency reliability, the scale was reduced to 18 items and four factors. We then conducted assessments of evidence for validity among NH Blacks, Indigenous, and NH White men and compared these across the reduced MBMC scale. Findings indicating that NH Black and Indigenous men experience fewer masculinity barriers with regard to attitudes toward medical professionals and exams countered prior literature on medical mistrust among these populations, indicating a need to further investigate these barriers (Adams et al., 2017; Daley et al., 2012; Haozous, 2020; Powell et al., 2019). Given the paucity of interventional and psychometric research focused on increasing CRC screening uptake among men from Black, Indigenous, and people of color populations, a more thorough analysis is warranted of the impact of masculinity barriers on CRC screening, a life-saving tool.
Footnotes
Acknowledgements
The authors thank the participants who made the study possible as well as Eleanor Mayfield, ELS, for editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge financial support from 5 For the Fight and the Huntsman Cancer Institute; the V Foundation for Cancer Research; the National Cancer Institute (Grant K01CA234319), the National Institute on Aging (Grant K02AG059140), and the National Institute on Minority Health and Health Disparities (Grant U54MD000214)—entities of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, 5 For the Fight, V Foundation for Cancer Research, the Huntsman Cancer Institute, or the University of Utah.
Ethics Approval
The Institutional Review Board (IRB) at the University of Utah approved the study protocol (IRB #00113679) prior to data collection. Informed consent was obtained online from all study participants before they started the study survey.