
Abstract
Despite the substantial adverse psychological impact of testicular cancer, few interventions have sought to improve psychosocial functioning and stress-related biomarkers in young adult survivors.
Testicular cancer is the most prevalent non-skin cancer among men in late adolescence and early adulthood, with incidence rates rising on average 1% each year over the last 10 years (National Cancer Institute, 2019). Advances in multimodal therapy afford young men with testicular cancer survival rates upwards of 95%, underscoring the importance of research focused on long-term survivorship (Chovanec et al., 2021). Thus, ensuring robust health-related quality of life is essential in this group. This population faces both psychological and physical impact from potential loss of a reproductive organ and long-term functional impacts of chemotherapy and surgery (Smith et al., 2018). In fact, many long-term sequelae are more severe and persistent in those receiving chemotherapy, including peripheral neuropathy, hypogonadism, infertility, fatigue, secondary malignancies, long-term hearing loss, sexual dysfunction, cognitive impairment, and cardiovascular disease (Fung et al., 2018). Psychosocial impact is also substantial and reflects gaps in the self-regulation of goal-driven activities and emotion (Hoyt et al., 2017). This includes body image disruption, social relationship difficulty, fertility and sexual distress, masculinity threat, work-related problems, loss of agency, and worry about the future (Hoyt & Penedo, 2021). Many of these physical and psychosocial adverse effects operate in part by pro-inflammatory and physiological stress pathways (Bower et al., 2011).
Of particular focus have been changes in neuroendocrine regulation and related stress physiology, inflammation, and angiogenesis (the development of vascularization of a tumor). Basic research on neural-immune signaling indicates that pro-inflammatory cytokines can signal the central nervous system to generate (or exacerbate) behavioral and physical changes after cancer (Antoni et al., 2006). For instance, there is growing evidence that pro-inflammatory cytokines negatively impact cancer-related fatigue, pain sensitivity, mood state, and cognition (Bower et al., 2011). Cytokines mediate and control inflammatory and immune responses and one of the effects of the chronic activation of the stress response is an increase in the release of various pro-inflammatory cytokines such as C-reactive protein (CRP), IL-6, and TNF-α. Furthermore, psychological distress can influence tumor progression via many different pathways including pro-angiogenic processes.
The hypothalamic-pituitary-adrenal axis (HPA) is the central regulatory system for controlling the release of stress hormones (i.e., cortisol), and HPA activity has a role in regulation of inflammatory processes and a link to a variety of health outcomes in cancer survivors as well. Moreover, findings in cancer patients suggest that diurnal cortisol rhythm may be shaped by behavioral coping strategies (i.e., self-regulation) (Diaz et al., 2014; Hoyt et al., 2014), including young adults with testicular cancer (Darabos & Hoyt, 2020).
Young adult testicular cancer survivors identify the key self-regulatory processes of goal adjustment and emotion regulation after cancer, as critically related to their health-related quality of life (Hoyt et al., 2016). Notably, both emotion and goal-related self-regulation can elicit inflammatory and biological stress activity (Darabos & Hoyt, 2020; Hoyt et al., 2013; Khan et al., 2020). Biobehavioral factors, including psychological stress and altered inflammatory and neuroendocrine processes, also appear to underlie poor self-regulation, depressive symptoms, and behavioral comorbidities (e.g., fatigue, sleep disturbance, cognitive dysfunction) and may even contribute to cancer progression over time (Lutgendorf & Sood, 2011; Miller et al., 2008). Thus, there is significant need for developmentally appropriate biobehavioral interventions for young cancer patients in emerging adulthood in order to decrease the adverse impact of diagnosis and treatment. Indeed, evidence is building for the clinical significance and scientific promise of biobehavioral interventions, or those that target biological mechanisms and processes and can favorably influence important neuroendocrine (e.g., cortisol), immune (e.g., pro-inflammatory cytokines), and angiogenic pathways (Hoyt & Penedo, 2021).
The primary purpose of the current analysis was to examine the effects of GET versus an active control on salivary stress and circulating inflammatory and angiogenic markers in young adult survivors of testicular cancer who have undergone chemotherapy in the prior 2 years. In this preliminary investigation, we hypothesized that those receiving GET would demonstrate steeper diurnal slopes of salivary cortisol and alpha-amylase (sAA), and lower overall cortisol and sAA output, and lower plasma levels of C-reactive protein (CRP), interleukin-6 (IL-6), interleukin-1-receptor-a (IL-1ra), tumor necrosis factor-α-receptor-2 (TNFαRII), and vascular endothelial growth factor (VEGF), at post-intervention compared to those in the control condition.
Methods
Participants
Young adult (ages 18–39) men treated by chemotherapy for testicular cancer were identified via medical record review or by clinic referral at a large urban Comprehensive Cancer Center. Potential participants were screened by a research assistant for eligibility. Participants were enrolled between January 2017 and December 2019.
Eligible patients were between the ages of 18 and 39 years, had a confirmed diagnosis of testicular cancer (any stage), completed chemotherapy within 2 years prior, and had English fluency. Notably, the 2-year period after chemotherapy is marked by intensive surveillance because of heightened risk of recurrence in this period (Chovanec et al., 2021; Lieng at al., 2018. This can be both physically and psychologically demanding. Participants were also screened to exhibit sub-optimal self-regulation as evidenced by a score of 1.8 or below on the Goal Navigation Scale (Hoyt et al., 2013) or a score of 4 or greater on the Distress Thermometer (DT) (National Comprehensive Cancer Network, 2013). The Goal Navigation Scale of the Cancer Assessment for Young Adults (CAYA), which has been designed and validated for young adult men with testicular cancer (Hoyt et al., 2013), measures goal navigation skill, while the DT is a single-item visual analog screening tool for psychological distress with a 0–10 range in which a score of 4 or greater signals more significant distress levels.
Men were excluded if they had a lifetime history of severe mental illness (i.e., schizoaffective disorder, schizophrenia, psychosis), active suicidality, presence of disorder that compromises comprehension (e.g., dementia), a self-reported medical condition or medication use known to confound biomarker assessment, or reported daily smoking (Nicolson, 2008; O’Connor et al., 2009).
The CONSORT enrollment diagram is presented in Figure 1.

CONSORT flow diagram.
Procedures
Following written informed consent procedures, participants completed questionnaires via a secure HIPAA-compliant online platform and collected saliva (as described below) at home across 2 consecutive days. Immediately following collection days, they attended an in-person session in which they provided blood samples and were randomized (1:1 in blocks of 10) to either GET or ISP. Participants repeated questionnaires and biological sample collection after the last intervention session.
Participants were given $50 at each data collection point for a total of $100. Each site’s institutional review board approved study procedures [University of California Irvine IRB# 2018-4676, Memorial Sloan Kettering Cancer Center IRB# 16-491].
Notably, this trial was underway prior to the onset of safety protocols in response to the COVID-19 pandemic. Responsive to institutional and public health guidelines, we immediately ceased collecting biological samples and subsequently began delivery of the intervention sessions remotely. Thus, this deviation from plan resulted in a smaller than planned sample size for this analysis, which includes only those men with biological samples collected at baseline.
All biomarker assays were conducted by the Core Laboratory of the Clinical and Translational Science Center (CTSC) at Weill Cornell Medicine.
Intervention Delivery
All intervention sessions were delivered by a mental health interventionist with a minimum of master’s-level training. All interventionists received intensive training prior to intervention delivery and weekly supervision from a licensed clinical psychologist. Sessions were audio-recorded to monitor treatment fidelity to their respective manuals. Both conditions consisted of six sessions delivered over 8 weeks. See Figure 2.
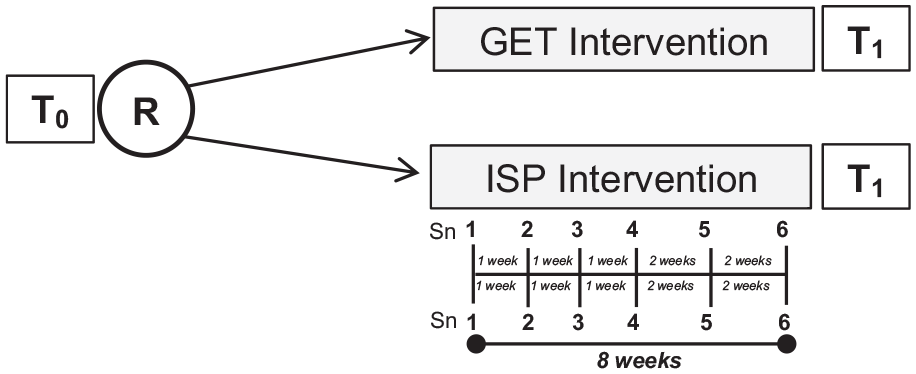
Study schedule.
Goal-Focused Emotion-Regulation Therapy (GET)
GET is designed to enhance self-regulation through improved goal navigation skills, improved sense of meaning and purpose, and better ability to regulate specific emotional responses (Hoyt et al., 2020). GET draws heavily from the principles of Hope Therapy (Cheavens et al., 2006), with an emphasis on goal navigation skill building. A focus is on identifying values-derived goals and learning skills to navigate a process of sustained movement toward them in the short-term future. Topics addressed include ensuring that goals are manageable and values-driven, goal refinement, generating pathways toward goal fulfillment, and managing blocked or challenged strivings. GET is meant to foster agentic thinking and includes training in basic cognitive restructuring and emotion-regulating coping skills.
Individual Supportive Psychotherapy (ISP)
ISP is a widely used community-based supportive care intervention in psychosocial oncology (Payne et al., 1997; see also Breitbart et al., 2018), and was adapted for use with young adult testicular cancer survivors. ISP relies heavily on supportive listening with a focus on the therapeutic use of genuineness, unconditional positive regard, and empathic understanding. The overall approach emphasized maintaining focus on the cancer experience and supporting participants in the “here and now” by creating a sense of being understood (Payne et al., 1997).
Measures
Diurnal Salivary Stress Biomarkers
Daily diurnal salivary cortisol and sAA were assessed via saliva samples collected with Salivette collection tubes (Sarstedt, Inc., Newton, NC) at three times on each sample collection day. Salivary markers were measured over two days at baseline and again post-intervention.
Participants were instructed to collect saliva samples upon awakening, 8 hr later, and at bedtime by removing the cotton swab from the Salivette and holding it between the cheek and gum for two minutes until the cotton swab was saturated (Nicolson, 2008). Participants subsequently placed the cotton swab back into the Salivette and secured the top. A written log was utilized to record adherence to collection instructions. To avoid sample contamination, they were instructed to avoid brushing their teeth, eating, or drinking within 20 min before sampling and told to keep samples refrigerated. Samples were returned either in person or by express mail. Upon receipt, Salivettes were stored in a −20◦C freezer until analysis. Concentrations of salivary free cortisol and sAA were measured in duplicate using a commercially available enzyme immunoassay without modification to the manufacturer’s recommended protocol (Salimetrics, Carlsbad, CA). The lower detection limit was 0.04 μg/dL for salivary cortisol, and 0.1 U/mL for sAA.
Values at each collection time were averaged across the 2 days. Two indices were computed for baseline and post-intervention including diurnal slope and area under the daily curve with respect to ground (AUCg) as a measure of total daily output. Slope values correspond to the decreasing (or increasing) pattern across the day in which lower values indicate a more flat or blunted pattern compared to higher slopes. Higher values on AUCg are indicative of relatively more overall daily cortisol production.
Plasma Inflammatory and Angiogenic Markers
Blood samples for measurement of circulating inflammatory markers were collected by a trained phlebotomist via venipuncture into EDTA tubes, placed on ice, centrifuged at 4°C for 15 min for harvesting of plasma within 30 min, and stored at −80°C until subsequent batch testing. Five biomarkers that have pro-inflammatory and/or angiogenic properties (CRP, IL-6, IL-1ra, TNFαRII, VEGF) were measured. All plasma samples were run in duplicate using procedures recommended by the assay manufacturer; for MesoScale Discovery (MSD [Rockville, MD]) assays, each biomarker was assayed as a single-plex: CRP (MSD, lower limit of detection: 0.0014 mg/L), IL-6 and VEGF (MSD, lower limits of detection: 0.1 and 0.2 pg/mL, respectively), TNFαRII (MSD, lower limit of detection: 0.2 pg/dL), and IL-1ra (R&D Systems [Minneapolis, MN] Quantikine ELISA; lower limit of detection: 18.3 pg/dL). Higher values indicate more overall circulating levels of the respective biomarker.
Demographic and Clinical Information
Demographic information, past/current psychosocial service use, support needs, intervention preferences, and perceived barriers were assessed through Likert-scale ratings and open-ended items. Additional demographic and clinical data, including body mass index (BMI) and testicular cancer-related treatment information, were assessed via medical record review and via self-report. In addition, medical co-morbidities and physical health symptoms were recorded; comorbidities were assessed by the Charlson Comorbidity Index (CCI) (Charlson et al., 1987). The CCI results in a weighted score in which a score of zero indicates no present comorbidities and a higher score is indicative of more medical comorbidities.
Data Analysis
All biomarker values were transformed with a log 10 transformation to correct for nonnormality. Data were analyzed using multiple linear regression. Primary analyses entered treatment group and baseline values of predicted outcome variable to model change in biomarkers over time. Analyses controlled for participant age (in years), BMI, medical comorbidities (Charlson Comorbidity Index score), race/ethnicity (ethnic minority status), and time since medical treatment completion, given their likelihood to influence immune and neuroendocrine functioning (Nicolson, 2008; O’Connor et al., 2009). Analyses were conducted on the analytic sample and repeated on the entire randomized sample, as described.
This analytic approach was adopted in post-hoc testing to test the possibility of differential effects based on level of distress at study entrance, as assessed by the DT.
Results
Characteristics of the sample are presented in Table 1. Participants were, on average, 28 years old, were most likely to be single or unmarried, with a majority having earned at least a 4-year college degree, reporting an annual household income greater than $45,000, and currently employed. Approximately 43% of participants identified as an ethnic or racial minority. Participants received chemotherapy as part of primary medical treatment for testicular cancer with an average time since chemotherapy completion 13.1 months (SD = 10.8). All participants also received surgical intervention including orchiectomy (100%) and retroperitoneal lymph node dissection surgery (~60%). The majority of participants (95.5% of GET participants and 86.4% of ISP participants) reported no medical co-morbidities on the CCI, and therefore this was not included in model testing. Among those included in the analytic sample, 89% attended all six intervention sessions (11 participants randomized to GET and 13 participants randomized to ISP).
Young Adult Testicular Cancer Survivors, Demographics by Group.

Note. Some categories do not equal 100% due to missingness.
Intervention Effects
Salivary Stress Markers
There were no significant group differences for AUCg or diurnal slope for salivary cortisol or sAA at baseline or at post-intervention (p’s > .05; see Table 2 for descriptive statistics).
Descriptive Statistics for Salivary Stress Markers and Circulating Markers of Inflammation at Baseline and Post-Intervention.
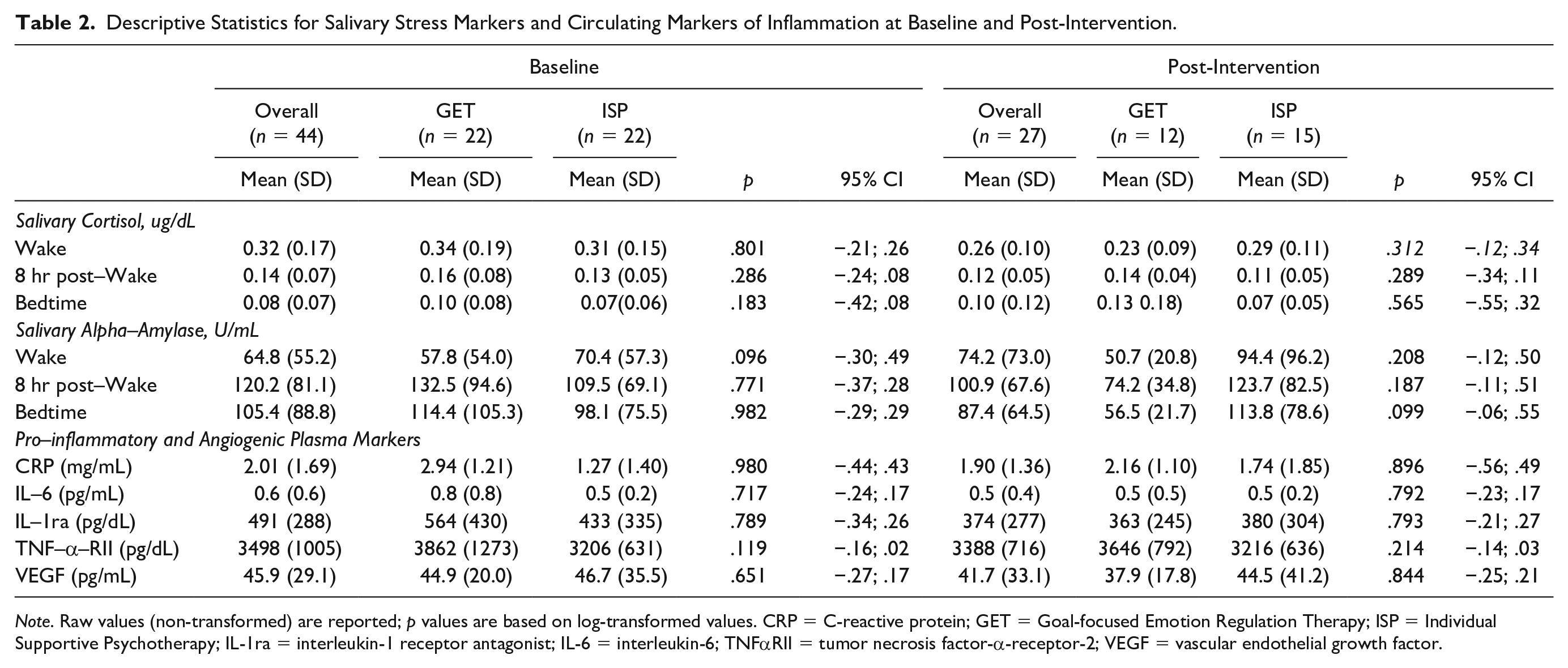
Note. Raw values (non-transformed) are reported; p values are based on log-transformed values. CRP = C-reactive protein; GET = Goal-focused Emotion Regulation Therapy; ISP = Individual Supportive Psychotherapy; IL-1ra = interleukin-1 receptor antagonist; IL-6 = interleukin-6; TNFαRII = tumor necrosis factor-α-receptor-2; VEGF = vascular endothelial growth factor.
From baseline to post-intervention, sAA AUCg decreased in those receiving GET (Cohen’s d = .67), while small increases were observed for those in the ISP group. However, as shown in Table 3, there was no significant effect of group for pre to post change in sAA AUCg (β = −.19, ns) or for change in sAA diurnal slope (β = .06, ns). However, group assignment was significantly related to change in cortisol AUCg (β = −57, p < .05). Cortisol AUCg decreased from baseline to post-intervention for those receiving GET (Cohen’s d = 0.45) and decreased slightly for those receiving ISP (Cohen’s d = 0.11). The effect of group on change in salivary cortisol slope approached significance (β = −56, p < .10).
Intervention Effects on Salivary Stress Markers.

Note. b0 = White (non-Hispanic); 1 = ethnic minority.
p < .10; *p < .05.
Although not statistically significant, in both groups the slopes of sAA (Cohen’s d = 0.24 for GET; 0.23 for ISP) and cortisol (Cohen’s d = 0.14 for GET; 0.07 for ISP) became flatter from baseline to post-intervention.
Plasma Inflammatory and Angiogenic Markers
There were no significant group differences for plasma levels of CRP, IL-6, IL-1ra, TNFαRII, or VEGF at baseline (p’s > .05; see Table 2 for descriptive statistics) or at post-intervention.
Regression analyses for plasma biomarkers are shown in Table 4. There were no significant effects of group for CRP, IL-6, TNFαRII, or VEGF (p’s > .05. However, group assignment was significantly related to change in IL-1ra from pre- to post-intervention (β = −64, p < .05); Cohen’s d = 0.65).
Intervention Effects on Plasma Biomarkers.

Note. b0 = White (non-Hispanic); 1 = ethnic minority.
p < .10; *p < .05; **p < .01.
Notably, decreases were observed in both groups from baseline to post-intervention for CRP (Cohen’s d = 0.14 for GET; 0.06 for ISP), IL-6 (Cohen’s d = 0.26 for GET; 0.22 for ISP), and VEGF (Cohen’s d = 0.29 for GET; 0.14 for ISP).
Post-Hoc Tests
In one set of post-hoc analyses, we examined whether there were group by level of entrance cancer-related distress (DT score) interactions with baseline to post-intervention changes in biomarkers. There was a significant group by distress interaction for changes in IL-1ra controlling for all identified covariates. Participants receiving GET who reported relatively more distress at study entry exhibited greater reductions in IL-1ra (B = −0.17, p = .047) than those with lower distress, and the opposite pattern (more distress, smaller reductions in IL-1ra) was observed for those in ISP (B = 0.05, p = .214) though this was not significant.
Discussion
There are currently no biobehavioral interventions designed specifically to promote targeted elements of self-regulation that are matched to the challenges experienced by cancer survivors in emerging adulthood. Most interventions tested in this population, though few, are designed generally for cancer survivors and then retrospectively tested in young adults. The primary aim of this pilot study was to demonstrate the preliminary impact of the GET intervention on salivary stress and pro-inflammatory and/or angiogenic biomarkers.
The current study examined the effects of GET versus an active supportive listening control (i.e., ISP) on salivary diurnal stress markers and circulating inflammatory and/or angiogenic markers in young adults with testicular cancer who received chemotherapy within the last 2 years. Compared to those receiving ISP, those who participated in GET exhibited significantly lower daily cortisol output at post-intervention. Patterns of decreasing sAA and multiple plasma markers (especially IL-1ra) from baseline to post-intervention were also observed in GET and within ISP, and effect sizes for changes over time were small to moderate. In addition to the pro-inflammatory markers, VEGF was examined as a marker of angiogenesis, or the physiological development of blood vessels in tumors (Shaik-Dasthagirisaheb, 2013). VEGF is considered a mediator of angiogenesis and inflammation and is involved in tumor development and metastasis in testicular germ cell tumors (Fukuda et al., 1999).
The results of this pilot randomized trial comparing GET to the ISP intervention were encouraging and provide some indication that the GET intervention might work to mitigate cancer-relevant pro-inflammatory and stress-related processes in this young adult survivor group. GET demonstrated promising trends in biological outcomes relative to ISP, as reflected in effect size changes from baseline to post-intervention in those receiving GET. A larger randomized trial is needed to build from these preliminary results to determine overall efficacy and clinical impact. Additionally, these results may be useful in optimizing the intervention for future trials. For instance, post-hoc testing on biomarker changes revealed a pronounced effect of GET for those with higher levels of distress, even though all participants were selected to have significant distress levels. It might be that GET can have optimal impact on adverse cancer impacts (e.g., cognitive impairment, pain, fatigue, mood disruption) for those with overall lower baseline self-regulation. In sum, these preliminary results are encouraging of the utility of the GET intervention; however, a larger scale RCT is necessary to evaluate its potential efficacy.
These results must be considered in light of several limitations. Although reductions in daily cortisol output and reductions in systemic inflammation have known relationships with better health-related quality of life in cancer patients (Lutgendorf & Sood, 2011; Miller et al., 2008), this study lacked a distal follow-up assessment of biological processes. The possibility that further change occurred over time cannot be determined in the current study. Also, this study relied on saliva collection over only 2 days at each assessment with three samples collected per day. However, between-group differences might be more reliable when observed across a longer period (Segerstrom, 2020; Segerstrom et al., 2014). The small sample size, in part reflecting the noted premature end of collection of biological samples due to the COVID-19 pandemic, is noteworthy. Small pilot studies such as this provide critical opportunities to optimize and refine biobehavioral interventions; however, they should not be mistaken for studies designed to establish efficacy. Thus, the pilot nature of this analysis should not preference statistical significance but rather effect size estimates, and patterns of change.
It should also be noted that this sample likely does not reflect the full spectrum of young adults with testicular cancer. All participants were receiving care at a large comprehensive cancer center, reported a relatively high annual household income, and the majority were engaged in full-time employment. Such factors may reflect relatively high overall functioning, which could also be related to the high level of adherence to study procedures. More feasibility testing may be needed in a more representative sample. Finally, we indicate that a large portion of our sample received Retroperitoneal Lymph Node Dissection surgery, which also may not be consistent with general samples of testicular cancer survivors.
This is the first pilot randomized controlled trial to demonstrate an impact of GET on reductions in overall daily cortisol output as well as a pattern of decreases in circulating inflammatory and angiogenic markers in the short-term among young adult survivors of testicular cancer. Larger trials will be needed to distinguish the impact of these interventions and observe the possibility that changes can be sustained or change over time. Given the adverse health impact of testicular cancer and lack of biobehavioral interventions tailored to young adults, these findings provide preliminary evidence to underscore further research with the goal of discovering whether goal-focused interventions alter immune and neuroendocrine processes in this population.
Footnotes
Acknowledgements
We acknowledge and thank Raymond Carrillo Ceja, Marisa Heule, Nisha Joshi, Mary Carol Mazza, and Sean Ryan for their contributions, and Yuan-Shan Zhu and Tamara Crowder at the Core Laboratory of the Clinical and Translational Science Center (CTSC) at Weill Cornell Medicine for their performance of biomarker assays. We also acknowledge the support of the Chao Family Comprehensive Cancer Center Biobehavioral Shared Resource, supported by the National Cancer Institute of the National Institutes of Health under award number P30CA062203. We also thank the study participants for their time and contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences National Institutes of Health, through Grants UL1TR000457 and UL1TR001414. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. Study sponsors played no part in study design; collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication.