
Abstract
The primary aim of this study was to determine whether psychosocial factors, such as post-traumatic stress disorder (PTSD) and anxiety, are independently associated with the development of central serous chorioretinopathy (CSCR), a predominantly male eye disorder. A secondary aim was to verify previously determined risk factors in a veteran population. All CSCR subjects seen in one year at a veteran eye clinic were included. Chart review was performed to identify general health information as well as eye history. Univariate and multivariate analysis was performed to identify factors that were independently associated with the development of CSCR. Fifty-one cases of CSCR were identified and an additional 51 age-matched controls with healthy eyes were used for analysis. Multivariate analysis revealed that history of PTSD was strongly associated with the development of CSCR (OR = 9.43, p = .002), even more so than previously reported risk factors. Anxiety was significant at the univariate level (OR = 6.48, p = .001) but lost significance at the multivariate level. At the multivariate level, several existing risk factors were confirmed including sleep apnea (OR = 5.76, p = .004), heart disease (OR = 7.06, p = .004), smoking (OR = 5.52, p = .003) and steroid use (OR = 4.55, p = .005). PTSD was strongly associated with the development of CSCR in the veteran population studied and may represent an important modifiable risk factor.
Keywords
Central serous chorioretinopathy (CSCR) is a retinal eye disease stemming from focal fluid leakage through the retinal pigment epithelium (RPE), often resulting in blurred or distorted central vision. Occurring primarily in middle-aged men (9.9/100,000), it represents a major cause of vision-threat among this population (Kitzmann et al., 2008). Commonly cited risk factors include type A personality, steroid use, sleep apnea, pregnancy, hypertension, and male sex (Chatziralli et al., 2017). Though the underlying cause is not yet fully understood, it is thought to stem from choroidal hyperpermeability and ischemia leading to retinal pigment epithelium (RPE) dysfunction (Giovannini et al., 1997). Several studies have reported a strong association with endogenous and exogenous glucocorticoids and the development of CSCR (Chatziralli et al., 2017; Garg et al., 1997; Haimovici et al., 1997). For instance, one case-control study reported that hypercortisolism was strongly associated with CSCR, with odds ratios of 37.1 for exogenous steroid use; also, over half of their CSCR cohort had elevated 24-hour urine catecholamine levels (Haimovici et al., 2003). CSCR occurs in ~5% of patients with Cushing syndrome, roughly 1000x higher than the general population, presumably from the excess release of endogenous glucocorticoids (Bouzas et al., 1993). Potential mechanistic explanations between glucocorticoid levels and CSCR include altered ion transport in RPE cells (Arndt et al., 2001), and steroid-mediated vascular reactivity and altered sympathetic-parasympathetic autonomic activity (Tewari et al., 2006; Yang & Zhang, 2004). Notably, CSCR has been associated with psychological and behavioral factors that might also be related to cortisol levels, such as “type-A” personality as mentioned above (Yannuzzi, 1987).
Yannuzzi et al. were the first to describe the association between CSCR and “type-A” personality (Yannuzzi, 1987). Individuals with “type-A” personality are described as more aggressive, competitive, ambitious, and hostile with an increased propensity for anger (Heilbrun & Friedberg, 1988). This finding fits with the cortisol hypothesis of CSCR, as negative affectivity (e.g., anger, nervousness, contempt, fear) has been associated with increased secretion of endogenous cortisol (Buchanan et al., 1999; Hellhammer et al., 2009). CSCR has been associated with other psychosocial and lifestyle factors, such as increased risk in shift workers and those with recent psychological stress (Bousquet et al., 2016), as well as in alexithymia and emotional distress. These findings have led to further studies on the psychological features of CSCR, namely how certain aspects of “type-A” personality may lead to the development of the disease. In two separate studies, Conrad et al. analyzed patients with CSCR using a “Temperament and Character Inventory” to investigate temperament and personality profile as potential risk factors (Conrad et al., 2007, 2014). In these two studies, emotional distress was strongly correlated to the development of CSCR. However, these studies used operational definitions of “psychological stress” and “emotional distress” that do not directly translate to clinical medicine, limiting their use as a potential screening tool. For instance, the presence of post-traumatic stress disorder (PTSD), generalized anxiety disorder (GAD), major depressive disorder (MDD), and homelessness, have all been reported to lead to increased emotional distress, and are identifiable clinically with established diagnosis/screening protocols (Callahan et al., 1998; Solorio et al., 2006; Susser et al., 1989). The use of these clinical diagnoses might serve as a better tool to screen for modifiable psychosocial risk factors that could lead to higher rates of CSCR. The purpose of this study was to analyze an urban veteran population, with high prevalence of these psychosocial factors, to determine their relation to the development of CSCR.
Material and Methods
This study was performed at the VA Greater Los Angeles Healthcare System (GLA) in Los Angeles, CA as a retrospective case-control study. The study was approved by the GLA’s Institutional Review Board (IRB), PCC 2019-060442, and followed the Declaration of Helsinki and Health Insurance Portability and Accountability Act (HIPAA). Informed consent was waived in the IRB given the nature of the study. Chart review was performed on all male patients seen at the VA eye clinic between January 1 2018 and December 31, 2018. Male patients were selected due to their prevalence in the specific patient population compared to females. Male age-matched controls were randomly selected from the VA general optometry clinic. This was done in order to select patients without severe underlying retinal disease while still having a recent eye exam. Inclusion criteria for diagnosis of CSCR was evaluation by an eyecare specialist with optical coherence tomography (OCT) with confirmation of diagnosis by a retina specialist. The exclusion criteria for controls was CSCR or other underlying eye disease such as age-related macular degeneration, glaucoma, uveitis, diabetic retinopathy, and retinal detachment.
For both CSCR and control patients, demographic, ophthalmic, and systemic medical information was recorded from GLA’s computerized patient record system (CPRS). Demographic information included age and homelessness. Ophthalmic information included best corrected vision, refraction, and treatment status for CSCR cases. Systemic medical information included hypertension, diabetes, sleep apnea, insomnia, heart disease, drug-use disorder, PTSD, anxiety, depression, smoking, alcohol-use disorder, steroid use, and thyroid disease. These factors were chosen because they were readily available across patient charts, and many have been previously shown as independent risk factors for the development of CSCR (Bouzas et al., 1993; Chatziralli et al., 2017). All non-ophthalmic patient information (e.g., sleep apnea, anxiety) was obtained through non-ophthalmology charts to reduce the possibility of reporting bias due to the increased acuity of care at the retina specialty clinic compared to controls.
For data analysis, a similar approach to Chatziralli et al. was used (Chatziralli et al., 2017); namely a two-tiered analysis was implemented where potential risk factors were analyzed independently (i.e., univariate analysis), and factors determined to be significant at the univariate stage (p < .05) were further analyzed in a multivariate model. All dependent (i.e., presence of CSCR) and independent variables were treated as dichotomous. At the univariate stage, odds-ratios were calculated in conjunction with corresponding t-tests or Chi-square tests. At the multivariate stage, a stepwise backward-selection multivariate model was used to calculate odds ratios; the final model retained variables only found to be statistically significant (p < .05). The analysis used the SPSS 23.0 statistical software package (SPSS Inc, Chicago, IL, USA).
Results
In the specified time period, 51 cases of CSCR were identified; 51 age-matched controls were randomly selected. The average age of patients was 63.4 ± 13.2 years old. All CSCR and control cases were male.
Table 1 and Figure 1 demonstrate the risk factors analyzed in this study, along with their respective odds ratios and statistical significance calculated from the univariate analysis. Statistically significance risk factors at this stage were diabetes (OR = 1.13–5.99, p = .023), sleep apnea (OR = 1.88–12.15, p=0.001), insomnia (OR = 1.44–9.40, p = .005), heart disease (OR = 1.06–7.76, p = .033), PTSD (OR = 1.75–13.43, p = .001), anxiety (OR = 1.74–11.24, p = .001), smoking (OR = 1.38–6.96, p = .005), and steroid use (OR = 1.95–10.54, p < .001). Non-significance was determined for homelessness (OR = 0.24–1.63, p = .336), hypertension (OR = 0.97–5.34, p = .057), drug-use disorder (OR = 0.31–2.46, p = .79), depression (OR = 0.87–4.36, p = .105), alcohol-use disorder (OR = 0.74–4.05, p = 0.2), thyroid disease (OR = 0.31–31.1, p = .308), myopia (OR = 0.15–1.95, p = .338), and hyperopia (OR = 0.19–3.1, p = .727).
Univariate Analysis of Risk Factors for Central Serous Chorioretinopathy (CSCR).

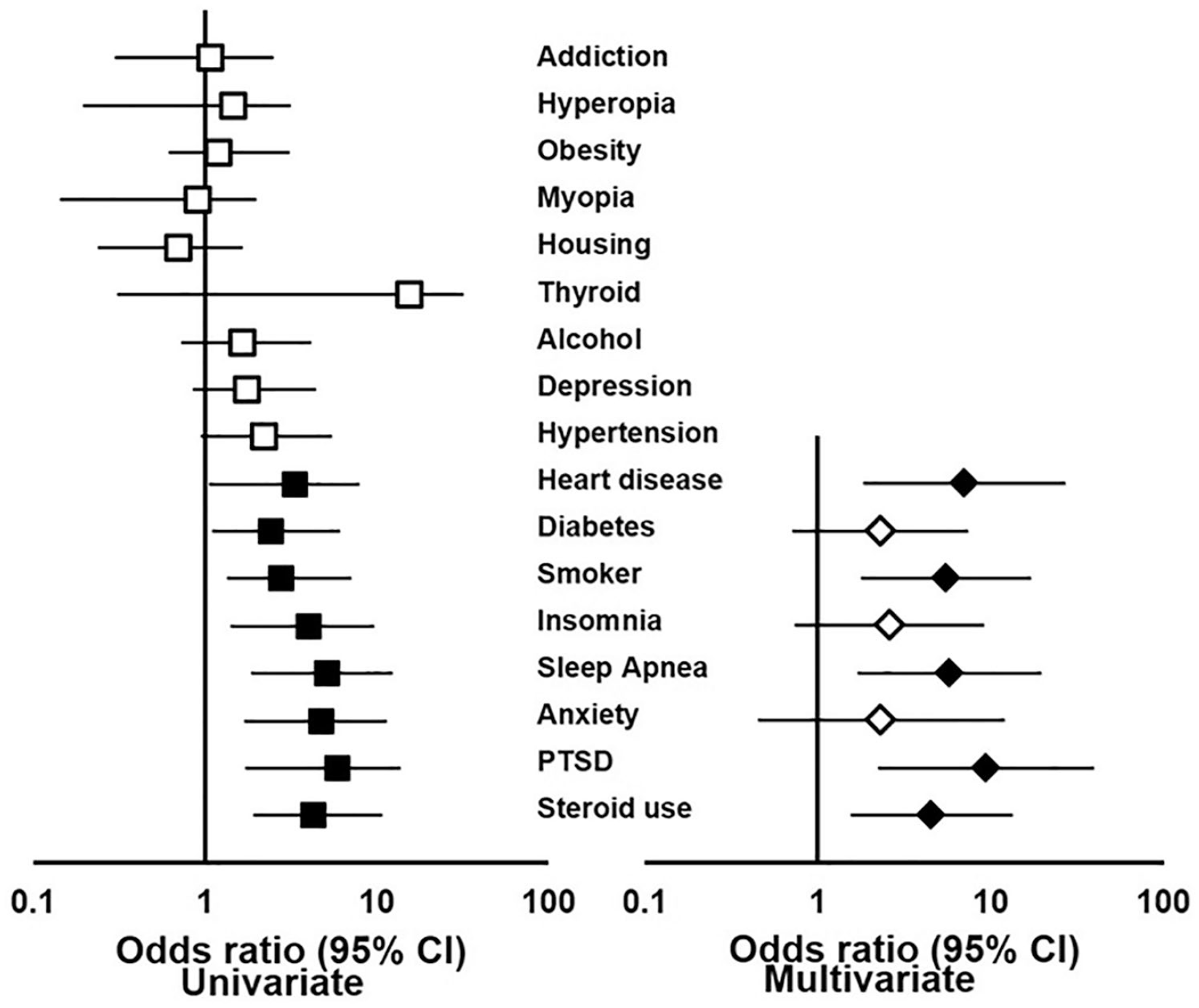
Forest plot demonstrating the 95% confidence intervals of odds ratios for the various potential risk factors in the univariate and multivariate model. Shaded shapes represent significant values, while unshaded shapes represent values that did not meet significance (p < .05).
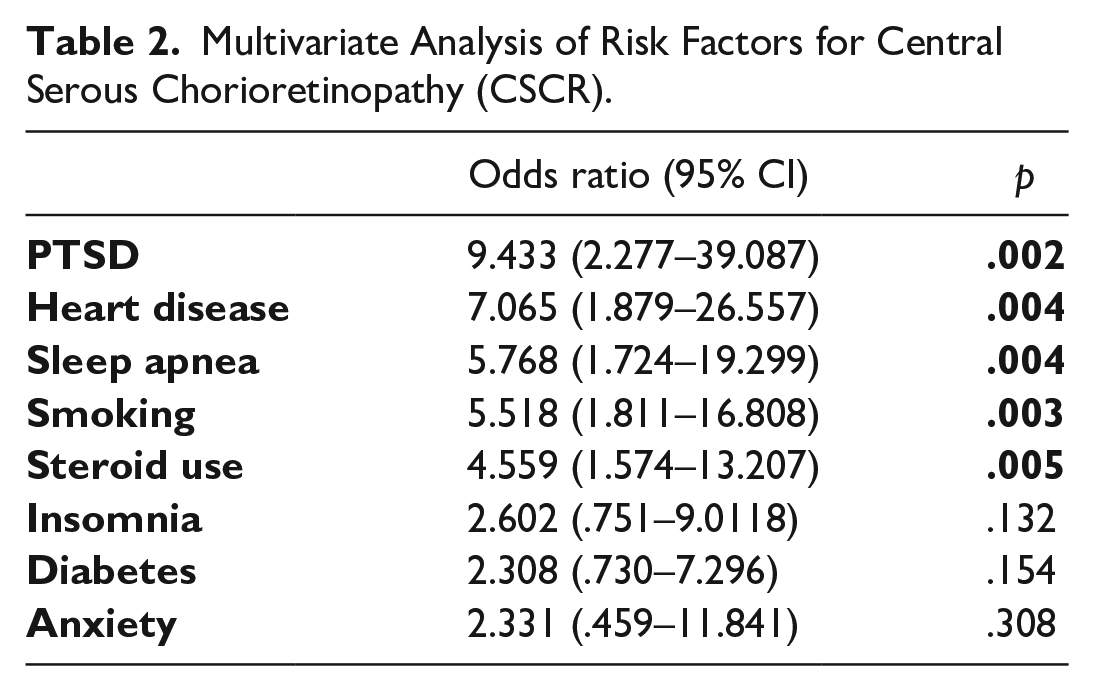
Risk factors found to be significant at the univariate stage were analyzed in a multivariate model, with the results given in Table 2 and Figure 1. Independent risk factors for the development of CSCR were sleep apnea (OR = 1.73–19.3, p = .004), heart disease (OR = 1.88–26.55, p = .004), PTSD (OR = 2.28–39.09, p = .002), smoking (OR = 1.81–16.81, p = .003), and steroid use (OR = 1.57–13.21, p = .005). History of diabetes (OR = 0.73–7.29, p =.154), insomnia (OR = 0.75–9.01, p = .132), and anxiety (OR = 0.47–11.84, p = .308) lost statistical significance at the multivariate stage.
Multivariate Analysis of Risk Factors for Central Serous Chorioretinopathy (CSCR).
Discussion
The primary objective of this study was to evaluate psychosocial risk factors for the development of CSCR in an urban, male veteran population. To that end, an established diagnosis of anxiety and PTSD were found to be significant risk factors for CSCR by univariate analysis, but only PTSD remained significant after multivariate analysis. Several other recognized risk factors were verified in this population including heart disease, smoking, sleep apnea, and steroid use. Therefore, this study not only confirms several known risk factors but also identifies PTSD as a new and important risk factor for developing CSCR.
We demonstrated that in a population of urban, male veterans, those with PTSD were significantly more likely to be diagnosed with CSCR (OR = 2.28–39.09, p = .002). In this analysis, PTSD may be a stronger risk factor than other previously described risk factors including smoking, sleep apnea and steroid use. We believe this finding was consistent with the cortisol hypothesis of CSCR. One study analyzing emotional responses and cortisol levels identified the highest levels of cortisol secretion from “uncontrollable situations” (Dickerson & Kemeny, 2004). The DSM-5 criteria for PTSD includes negative alterations in cognition and mood such as persistent and exaggerated negative beliefs, which might often be perceived as an “uncontrollable” or “impossible” situation. Additional PTSD criteria include irritable behavior, angry outbursts, hypervigilance, and exaggerated startle response, all of which are congruent with Type A personality, the classic association with CSCR. PTSD can also be associated with sleep disturbances, which itself has been identified as an independent risk factor for CSCR, such as the increased incidence of CSCR in shift workers (Bousquet et al., 2016).
This study suggests that the diagnosis of PTSD might be useful to screen or diagnose CSCR in high-risk populations. Because the diagnostic criteria for PTSD is applied ubiquitously in clinic practice, especially in centers that treat veterans, this would be an objective and powerful screening tool for high-risk populations. Although further research is needed, PTSD might be useful to predict recurrence rates, response to various treatment modalities and represent a modifiable risk factor that could help patients regain vision faster (Fok et al., 2011; Murphy et al., 2016).
Sleep apnea, smoking, and steroid use were found to be independent risk factors for CSCR in this study as well. This aligns with several other studies, including the relatively large case-control study by Chatziralli et al. which used a multivariate approach similar to the one used here (Chatziralli et al., 2017). These factors have all been related to potential mechanisms related to hypercortisolism or vascular dysfunction in CSCR (Daruich et al., 2015; Edwards et al., 2014; Xue et al., 2010). We found that heart disease was an independent risk factor (OR = 1.88–26.55, p = .004) for CSCR in this population. Heart disease has been confirmed by some studies (Tittl et al., 1999), with potential mechanisms involving coagulation/vascular dysfunction, but called into question by others (Chatziralli et al., 2017). In our study, heart disease represented the second largest risk factor for CSCR, even greater than exogenous steroid use, although 95% confidence intervals are overlapping.
An important difference between the population used here and other similar studies was the average age of patients with CSCR. Although we controlled for age between case and control subjects, the average age of our subjects was 63.4 years, compared to 44.6 and 48.3 years reported in other case-control studies (Chatziralli et al., 2017; Fok et al., 2011). This could be explained by the higher national average age (64 years) of veterans compared to non-veterans (41 years).(Profile of Veterans: 2014, Data from the American Community Survey, 2016) This demonstrates that although CSCR is classically associated with middle aged men, it is also prevalent in older demographics. The increased age of CSCR patients in our study points out the difficulty in diagnosing the disease in elderly patients, as its clinical features can overlap with age-related macular degeneration (ARMD) which is prevalent in elderly populations. Therefore, in certain clinical situations it may be useful to consider PTSD to help distinguish CSCR from AMD.
The major limitation of this study was its relatively small cohort size causing the confidence intervals to be large and overlapping; thus, effect size cannot be compared between risk factors. The statistical significance of many previously reported risk factors held, suggesting the sample size was large enough for the purposes of exploring new risk factors. Lastly, prevalent cases of CSCR were used during chart review rather than incident cases, therefore causality cannot be ascertained.
In summary, this analysis demonstrated that PTSD was strongly associated with the development of CSCR in an urban, male veteran population. Further study should be done to examine the benefits of PTSD treatment for the resolution of CSCR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by an Unrestricted Grant from Research to Prevent Blindness.
Ethical Declaration
All authors mentioned in this manuscript have agreed upon authorship, read and approved the manuscript. The manuscript has not been published elsewhere.
Informed Consent Declaration
Given the nature of this chart review study, informed consent was waived. No identifiable patient information was recorded during the performance of this study.