
Abstract
Chemerin (CHEM) is a new proinflammatory adipokine involved in the immune, metabolic and reproductive processes. Low–grade state inflammation (LGSI) is a key element in the pathogenesis of metabolic syndrome (MS). Low SHBG is a good marker of male hypogonadism in MS. This study evaluated the prognostic value of selected adipokine, LGSI, and androgenic parameters in predicting the risk of MS among men. One hundred thirty-two random men aged 40 to 70 years old were enrolled. Measurements of anthropometric indices, blood pressure, and laboratory tests were carried out. A total of 62 men (47%) were diagnosed with MS. Chemerin concentrations were higher in men diagnosed with MS compared to healthy: 89.48 (78.12–112.10) vs. 77.9 (65.12–98.64) ng/mL; p = .002. Men diagnosed with MS presented with lower levels of total testosterone: 5.75 (4.00–6.57) vs. 6.40 (5.50–8.40) ng/mL; p = .0014 and SHBG: 46.58 (35.13–66.28) vs. 71.97 (56.1–92.7) nM/L; p < 0.000001. Elevated LGSI indices were demonstrated in men with MS as opposed to healthy [IL–18: 530.64 (409.12–640.56) vs. 418.85 (348.14–496.44) pg/mL; p = .000033 and hs–CRP: 2.15 (0.97–4.26) vs. 1.01 (0.41–2.68) ng/mL; p = .0057)]. In multivariate regression analysis, the highest negative predictive value in assessing the risk of MS was SHBG serum concentration, while the highest positive predictive values were: IL-18, hypertriglyceridemia, and waist circumference. Decreased SHBG levels, combined with elevated IL-18 concentrations in men showing hypertriglyceridemic waist phenotype, significantly increase the risk of MS.
Chemerin, also known as retinoic acid receptor responder protein 2 (RARRES 2), is a newly discovered adipokine (16 kDa) involved in the immune, metabolic and reproductive processes. Its presence is detected in the liver, white adipose tissue, adrenal, pituitary, placenta, and gonads.
CHEM participates in the differentiation of adipocytes and lipolysis (Muruganandan et al., 2011). CHEM is likewise involved in regulating gene expression for the GLUT-4 receptor and increases insulin resistance. Its concentrations are significantly augmented in polycystic ovary syndrome (PCOS) (Kort et al., 2015), while it declines during metformin therapy. CHEM also demonstrates proinflammatory properties and is positively associated with CRP (C-reactive protein) (Maghsoudi et al., 2015).
Most papers describing CHEM’s impact on the reproductive process refer to women, especially those diagnosed with PCOS (Kort et al., 2015). Experimental studies report CHEM’s apparent inhibitory effect on steroidogenesis in the ovaries (Reverchon et al., 2012) and Leydig cells in the testes (Li, Ma, et al., 2014). There is a lack of research concerning the assessment of chemerin in aging men, especially in the co-occurrence of MS.
Low-grade systemic inflammation, even if subclinical, is a strong predictor of diabetes and premature atherosclerosis (de Rooij et al., 2009). LGSI also accompanies syndromes with insulin resistance (PCOS, fatty liver), neurodegenerative diseases, and the aging process per se (“inflammageing”) (Esposito Katherine et al., 2005). Aging is associated with a shift in the balance between Type 1 and Type 2 cytokines in humans, increasing Th1–type responses (Sandmand et al., 2002). The primary mediators of Th1 responses include TNF, IFN–γ, and interleukins (mainly IL–1, IL–12, and IL–18). Men with diagnosed MS have a significant elevation of IL–18 levels (Herman et al., 2011).
Proper plasma concentrations of androgens have a positive effect on immunological and metabolic processes in males. Obesity and aging diminish the plasma androgen concentrations in men (Laaksonen et al., 2003).
The importance of the role of a reduced SHBG concentration as a predictive factor for the prevalence of the metabolic syndrome is constantly increasing (Moon et al., 2017; Siddiqui et al., 2018). A low SHBG serum concentration is considered an excellent early marker of male hypogonadism in metabolic syndrome (Jarecki et al., 2019). Hyperinsulinemia causes inhibition of hepatic SHBG production and affects the ectopic location of adipose tissue. An interesting study from 2019 reported that lowering plasma SHBG concentrations in young men is a predictor of nonalcoholic fatty liver disease developing in middle age (Sarkar et al., 2019).
This cross-sectional study aimed to evaluate the prognostic value of selected adipokine (chemerin) and LGSI indices (IL-18 and hs-CRP). In combination with parameters assessing androgenic status (SHBG and selected androgens), inflammatory parameters help predict the risk of MS in men.
Materials and Methods
The study was approved by local medical ethics committee “(Blinded)” at (Blinded).
Following the Declaration of Helsinki, written consent was obtained from each patient or subject after a full explanation of the purpose and nature of all procedures used.
One hundred fifty-three male subjects were recruited for the study utilizing 380 postal invitations sent to men aged 40 to 70 years old (the response rate was 40.3%).
We excluded nine men with symptoms of acute infection, three men treated with antipsychotic drugs, three men treated with insulin, two men treated with metformin, two men treated with gonadotropin-releasing hormone analogs for prostate cancer, one man treated with fibrates, and one man treated with glucocorticoids, a total of 21.
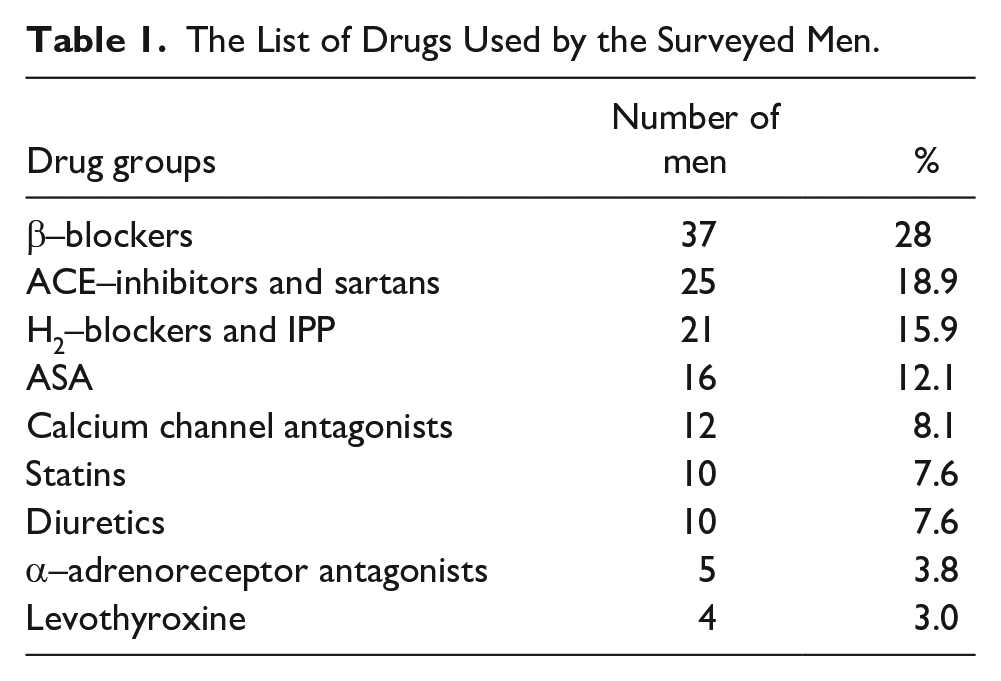
Finally, we enrolled a total of 132 men in the study. Among all study participants, seventy-three men were not taking any drugs. The others were treated with various medications, mainly older men (Table 1). Men treated with levothyroxine were euthyroid.
The List of Drugs Used by the Surveyed Men.
Waist girth was measured at the umbilicus level or the level of the maximum circumference. BMI (body mass index) was computed as
MS was diagnosed according to the International Diabetes Federation criteria (2005) (Consensus Statements, n.d.), because we believe that visceral obesity plays a crucial role in the development of metabolic syndrome, inducing LGSI with its health consequences.
Blood samples from participants were taken in the morning after overnight fasting and abstention from tobacco smoking. The samples were immediately centrifuged and frozen until they were assayed. The supernatants were divided into small parts before being stored at −70°C and thawed only once. All the samples were assayed twice simultaneously for all parameters (excluding IL–18 and CHEM), and average values were calculated.
Measurement of dehydroepiandrosterone sulfate (DHEA-S) was conducted using the ELISA method produced by BioSource Company (Belgium). The concentration of FT was determined through a radioimmunoassay method utilizing J–125 isotope labeled testosterone analog from Diagnostic Systems Laboratories Inc. (USA). TT levels were estimated by the high-sensitivity ELISA method of DRG International Inc. (USA). The concentrations of sex hormone-binding globulin (SHBG) were estimated by the immunoradiometric method manufactured by Beckman Coulter Immunotech (USA/Czech Republic). Measurement of interleukin 18 (IL-18) was performed using the high–immunoenzymatic ELISA method prepared by Medical & Biological Laboratories Co., Ltd (Japan). The hs-CRP levels were estimated using high-sensitivity immunoassays provided by BioCheck (USA). The CHEM plasma levels were determined using a commercial enzyme-linked immunosorbent assay produced by Enzo Life Sciences (USA) with a diagnostic test sensitivity of one ng/mL.
For all analyses, STATISTICA version 13.3 PL was used (StatSoft Inc., USA). All data were revealed in the form of medians with 25–75% interquartile ranges or percentages. Compliance with normal distribution was estimated using the Shapiro–Wilk and Lilliefors tests. Variables characterized by normal distribution were assessed using the t–Student test, as opposed to variables of abnormal distribution, which were estimated by way of the Mann–Whitney U non-parametric test for independent samples. The associations were measured using a non-parametric Spearman rank associations test. Results were considered statistically significant at a p-value lower than .05.
To assess factors that may affect the MS occurrence, we performed univariate and multivariate logistic regression analysis. In the univariate logistic regression model, the dependent variable was a diagnosis of MS. Independent factors were chemerin, age, waist circumference, systolic and diastolic BP, BMI, glucose, hs-CRP, IL-18, HDL-cholesterol, triglycerides, free and total testosterone, DHEA-S, and SHBG. For multivariate logistic regression, model variables with a p-value <.1 in the aforementioned univariate regression analysis were chosen.
Results
The IDF criteria for the MS diagnosis were fulfilled by a total of 62 men (47%)—Table 2. The groups did not differ statistically in the Mann-Whitney U test for age (Z = 1,0048, p = .299236) and the Chi-square test for smoking tobacco (Chi-square = 0.64396, p = .42228). The characteristics of individual groups are presented in Table 2.
The Comparison of Anthropometric, Hormonal, and Metabolic Parameters in the Groups Studied.

Note. Values are given as medians with interquartile ranges.
Men diagnosed with MS revealed a statistically significant, lower TT and SHBG, while FT and DHEA-S showed no differences. In men meeting the MS criteria, elevated LGSI indices were observed. It was also shown that men suffering from MS demonstrated higher CHEM levels than the control group.
Associations of chemerin concentrations with androgenic status, parameters of metabolic syndrome, and LGSI exponents were presented in Table 3 in the form of Spearman rank associations coefficients (CHEM plasma levels do not meet the criteria of normal distribution).
Spearman Rank Associations Coefficients Between Chemerin Plasma Levels and Hormonal, Metabolic, Anthropometric, and Inflammatory Parameters.

The Bold significance for each parameter is presented with R and p-value.
CHEM plasma concentrations were associated with most MS components (HDL-cholesterol, triglycerides, waist circumference) except systolic and diastolic blood pressure. The relationships between CHEM and particular components of MS were relatively weak. Additionally, CHEM serum levels were positively associated with LGSI indices. In contrast, CHEM plasma levels revealed no statistically significant relationships with androgenemia.
SHBG plasma levels are positively associated with age, weakly but statistically significant (R = 0.202, p = .02). The SHBG levels were significantly lower in men diagnosed with MS and revealed moderately negative associations with anthropometric features (R = −0.411; p = <0.000001 for waist circumference and R = −0.418; <p = .000001 for BMI).
SHBG plasma levels are strongly and directly associated with total testosterone (R = 0.556, p < .000001) while showing negative associations with CHEM (Table 3) and BMI (R = −0.418, p = .000001). On the contrary, SHBG revealed no associations with LGSI indices (R = −0.068: p = .438 for IL–18 and R =–.134; p = .124 for hs-CRP) and DHEA-S (R = −0.146267, p = .094).
In univariate regression analysis, eighteen parameters were evaluated (Table 4). In the multivariate analysis, we included all parameters fitting p <0.1 in univariate logistic regression for a maximum total of roughly N/20 parameters. From the remaining parameters, when there were pairs of strong associations (Rs > 0.5), we chose only one of those or offered two multivariate regression models. We created several different models (Table 5) of multivariate regression analysis to look further into the most promising factors for predicting MS.
Univariate Regression Analysis.

Note. *p < .1, **p < .05, ***p < .001, ****p < .0001.
The Bold significance for each parameter is presented with R and p-value.
Chosen Multivariate Regression Analysis Models.

The Bold significance for each parameter is presented with R and p-value.
From results in the model presented above, we excluded from further analysis:
Chemerin—due to no significance,
total testosterone—due to no significance, and a strong association between SHBG and TT (Rs = 0.56). Out of this pair, we chose SHBG for further evaluation, and
BMI—due to a strong association with waist circumference (WC being essential to us due to central obesity).
In the following model created, in addition to the remaining parameters, we included diagnostic criteria for MS with the highest statistical significance. The plasma SHBG concentration in this model slightly loses statistical significance, although the marginal p-value is probably associated with sample size. After additionally considering chemerin concentrations, SHBG still retains its statistical significance.
Forest plots showing odds ratios for MS occurrence in particular quartiles of parameters studied are presented in the supplementary file.
Discussion
The impact of age on the adipokine plasma profile seems to be well established, at least in soluble CD163, fetuin-A, osteopontin, and IL-1 receptor antagonist (Weghuber et al., 2014). Unfortunately, data regarding the relationship between CHEM levels and age are still limited. Conflicting data were visible while comparing CHEM concentrations in both sexes, primarily if they were related to different races (Takahashi et al., 2013).
CHEM can be regarded as a link between the immune and metabolic processes, acting through a factor predisposing to the development of MS and diabetes (Maghsoudi et al., 2015; Mariani & Roncucci, 2015). It was demonstrated that elevated CHEM levels occur not only in diabetic patients but also in their first-degree relatives (Xh et al., 2014). The results suggest that the CHEM concentration is positively associated with the LDL–cholesterol plasma levels, particularly that of small dense LDL, while a strong negative association with HDL cholesterol, concerning the particles of larger size, was revealed (Lőrincz et al., 2014).
Our study showed that men suffering from MS demonstrated higher CHEM levels than healthy participants (Table 2). CHEM plasma concentrations were associated with most components of MS, except for diastolic blood pressure and FPG (Table 3). In particular, the CHEM concentration was associated with pivotal and, we believe, crucial MS element, waist girth. In a metaanalysis carried out in 2014 by Li et al., no relationships between CHEM with FPG and HbA1c were demonstrated (Li et al., 2014), although in our study FGP showed a positive correlation with the CHEM concentration.
Although the classic insulin resistance tests (primarily the hyperinsulinemic-euglycemic clamp) remain a “gold standard,” studies on newly discovered adipokines, myokines, and hepatokines are now a promising and attractive approach (Park et al., 2015).
In another study, the CHEM concentrations were surprisingly much lower in men diagnosed with type 2 diabetes than healthy (Takahashi et al., 2013). It is probably the case that elevated plasma CHEM levels in obese men and men diagnosed with type 2 diabetes are associated with an accompanying LGSI rather than the intensified visceral fat deposition as a source of CHEM release (Weigert et al., 2010). The authors from Korea formulated the opposite conclusions (Cheon et al., 2017).
CHEM acts as a potent chemoattractant to antigen-presenting cells (plasmacytoid dendritic cells, macrophages, and NK cells). It demonstrates anti-inflammatory properties; therefore, it plays an immunomodulatory role (Luangsay et al., 2009). It was proved that CHEM is strongly associated with hypertension and with markers of inflammation (Gu et al., 2014). Our study also demonstrated the significant monotonic positive association of CHEM with systolic blood pressure (Table 3), although there were no differences in CHEM levels in men with diagnosed or treated hypertension compared to healthy subjects.
We showed a good association of chemerin concentrations with inflammatory parameters (Table 3).
LGSI may exert an inhibitory effect on steroidogenesis. The impact of adipokines on steroidogenesis is also significant, although it is not unequivocal. Caminos et al. demonstrated that leptin and adiponectin inhibit testosterone production in the Leydig cells, both in basal conditions and after chorionic gonadotropin stimulation (Caminos et al., 2008), while reverse actions exhibit resistin. However, plasma concentrations of the resistin and leptin are positively associated with CHEM serum concentrations. In vitro treatment with CHEM inhibited the human chorionic gonadotropin–induced testosterone production from Leydig cells (Li et al., 2014) proved through an experiment that IGF-1-induced ovarian steroidogenesis can also be modified by CHEM (Reverchon et al., 2012). A 2014 study demonstrated that CHEM and the evolutionary conservative 20-amino acid signal peptide exert a significant inhibitory effect on steroidogenesis in the gonads (Li, Huang, et al., 2014). In our study, CHEM concentrations were not associated with the biochemical parameters of androgenemia.
Subnormal testosterone may be associated with LGSI already at a young age, leading to male hypogonadism (Bobjer et al., 2013).
SHBG serum levels increase with age, and a lower SHBG concentration is considered an independent and strong risk factor for MS development (Haring et al., 2013). In particular, waist circumference appeared significantly and negatively associated with SHBG levels (Chin et al., 2013). Both regularities were also confirmed by the results of our study, although we could not demonstrate the statistically significant effect of age. Nonetheless, age and obesity, although associated with each other, have opposite effects on SHBG plasma concentrations. Through multivariate regression models in their cross-sectional study, Liao et al. revealed that SHBG is independently associated with hs-CRP (Liao et al., 2012). In our study, no significant associations between SHBG and hs-CRP as well as IL-18 were observed.
A fundamental role in diagnosing MS is assigned to waist circumference. Canadian authors have defined the so-called hypertriglyceridemic waist phenotype, EWET (Enlarged Waist Elevated Triglycerides) (Weschenfelder et al., 2017). EWET consists of a high waist circumference > or = 90 cm and an increased fasting triglyceride level above 2.0 mmol/L, and can be used as an initial screening approach to identify individuals with an increased cardiometabolic and diabetic risk (Blackburn et al., 2009). The results of our analysis confirm the vital role of visceral obesity in MS prediction (the risk increased by 18.8% for every centimeter of waist circumference above the norm).
Both IL-18 and SHBG (although no direct correlation was shown between them) are interrelated through another factor (e.g., waist circumference), which interferes with statistical analysis (confounding factors).
The present study demonstrates several restrictions and limitations that affect its value. The commonly available commercial sets for CHEM must simultaneously determine their precursors and derivatives, which have different biological activities. For example, 156– and 157– CHEM derivatives reveal vigorous activity, in contrast to the minimal activity of 152–, 154–, 155–, and 158–derivative (Zabel et al., 2005). A systematic error resulted from the method for determining CHEM, which undoubtedly influences the conclusiveness of the study results. In addition, the CHEM concentrations in our study were determined only once. We did not evaluate 25–OH–D3 serum levels in male subjects, and it is known that cholecalciferol supplementation may affect the CHEM concentrations.
In our final words, we would like to point out the significant complexity of intertwined co-relations, most not fully understood, between different parameters and the risk of developing metabolic syndrome. Widely used odds-ratios are not easily comprehended, and it is neither intuitive nor an easy-to-understand concept. It is often not correctly interpreted by readers who analyze publications and can come to wrong conclusions about the strength of the given parameter on the outcome. Odds ratios (OR) are widely presented by showing relative risk at specific values of a critical predictor while holding all other predictors constant. In reality, all these parameters multiplicatively affect the risk. Another issue at hand is that many parameters have non-linear effects of the given parameter change on the relative risk.
To bring the topic to perspective, in model 3, we have IL-18 showing OR of 1.014, while waist circumference shows OR of 1.243. This result can implicate a much bigger impact of waist circumference than IL-18 in the development of MS. OR can be interpreted like bank interest, 3% on 500$ will give more than 20% on 10$. In our study, IL-18 had an IQR of 212, while waist circumference had an IQR of 15. Calculating risk based on model 3: for IL-18 relative risk of top 25% vs bottom 25% is equal to (IQR*(OR-1))+1 = 3.968 risk vs. for waist circumference top 25% vs bottom 25% is equal to (IQR*(OR-1))+1 = 4.645. Sure, the risk is higher, but it is now only a small difference compared to 1.014 vs. 1.243 being the OR for given parameters.
Another intriguing thing is comparing a person with waist circumference within the first quartile and IL-18 within the first quartile to a person with waist circumference in the third quartile and IL-18 within the third quartile results in 4.645*3.968=18.43. It means that the obese person with high waist circumference and high inflammatory parameters has around 18.43 times higher chance of developing metabolic syndrome than the thin person with low waist circumference and low inflammatory parameters. That is taking into consideration just two parameters, while the human body is very complex and all factors multiplicatively affect the risk in logistic regression, per each parameter’s point. Worth noting is that this type of statistical analysis is used widely in the insurance industry for risk evaluation and the banking industry. That is why multivariate logistic regression, especially calculated on big groups, can estimate predictors and their importance for developing a given disease.
Key Message
Decreased SHBG plasma levels, especially in combination with elevated IL-18 serum concentrations in men showing hypertriglyceridemic waist phenotype, significantly increase MS’s risk.
Metabolic Syndrome and its consequences are complex and intertwined with each other. Worth remembering is that all predisposing factors have multiplicative, rather than additive, effects in biological organisms.
Limitations
First of all, studies with an evaluation of prognostic values would be ideally done as follow-up studies, while ours was a cross-sectional one. Small groups are another problem, though due to choosing people from the same background of (Blinded) and financial limitations (self-funding)—it was hard to achieve a bigger test group. Carrying out a metaanalysis could prove more accurate insight, but due to non-parametric results and a lack of experienced statisticians, it was impossible at the time. Another avenue worth exploring is genetic predispositions; analyzing first-degree relatives for metabolic syndrome, and its components could provide further insight into the relative risk of given parameters with family medical history.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883211034984 – Supplemental material for The Comparison of Predictive Value Among Chemerin, IL-18 and Hormonal Parameters in Assessing the Risk of Metabolic Syndrome in Men
Supplemental material, sj-docx-1-jmh-10.1177_15579883211034984 for The Comparison of Predictive Value Among Chemerin, IL-18 and Hormonal Parameters in Assessing the Risk of Metabolic Syndrome in Men by Piotr Jarecki, Waldemar A Herman, Jacek Losy and Katarzyna Lacka in American Journal of Men’s Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.