
Abstract
Men remain underrepresented in behavioral weight loss trials and are more difficult to recruit compared to women. We describe recruitment response of men and women into a mixed-gender behavioral weight loss trial conducted within 36 rural primary care clinics. Participants were recruited through primary care clinics via direct mailings (n = 15,076) and in-clinic referrals by their primary care provider (PCP). Gender differences were examined in response rate to direct mailings, study referral source, and rates of proceeding to study screening, being eligible, and enrolling. Men had a lower response rate to direct mailings than women (7.8% vs. 17.7%, p < .001). Men (vs. women) responding to the mailing were more likely to respond by opt-in postcard (64.6% vs. 56.8%) and less likely to respond by phone (33.9% vs. 39.6%), p = .002. Among potential participants contacting the study (n = 2413), men were less likely to report being referred by PCPs (15.2% vs. 21.6%; p < .001), but were just as likely to proceed to screening, be eligible, and enroll. Men and women were more likely to proceed to screening when referred by PCPs (93.3% vs. 95.4%) compared to direct mailings (74.2% vs. 73.9%). Enrolled men were older (p < .001), more likely to be married (p = .04), and had higher levels of education (p = .01). Men were less likely than women to respond to direct mailings and to be referred by their PCP, but after contacting the study, had similar screening, eligibility, and enrollment rates. Encouraging and training providers to refer men during clinic visits may help recruit more men into primary care-based weight loss trials.
Weight loss interventions support that both men and women can successfully lose weight across a variety of intervention techniques (Robertson et al., 2017; Williams et al., 2015); however, men are largely underrepresented, constituting only 27% of randomized controlled trial participants (Pagoto et al., 2012). One challenge of recruiting men into weight loss trials is selecting an effective recruitment strategy (Rounds & Harvey, 2019); however, few empirical studies report or analyze their recruitment methods and enrollment rates by sex (Pagoto et al., 2012).
Successful strategies for recruiting men into behavioral weight loss interventions are not well described. Generally, men are more likely to respond to recruitment materials that use concise text and images of men in leadership roles (Ryan et al., 2019). However, even when men-specific targeted messages are incorporated in recruitment materials, men’s screening rates may not improve (Crane et al., 2016). Targeted messaging also has been successful in recruiting at-risk populations (Crane et al., 2020). Furthermore, many behavioral intervention materials were designed with women in mind (George et al., 2012), which can negatively influence men’s interest due to perceptions of dieting and masculine identity (Archibald et al., 2015; de Souza & Ciclitira, 2005; Grace et al., 2018; Rounds & Harvey, 2019; Sabinsky et al., 2007). Conversely, men are more likely to enroll in behavioral interventions when recruitment materials are socioculturally targeted (Kelly et al., 2019; Morgan et al., 2016), or when they are medically referred to lose weight (Elliott et al., 2020).
One potential solution to increasing the recruitment of men incorporates using primary care clinics as a referral source. Past studies focusing on recruitment from primary care clinics for mixed-gender behavioral weight loss interventions report a wide range of men’s enrollment from 16% to 56% (Ahern et al., 2016; Appel et al., 2011; Bennett et al., 2012; Christian et al., 2011; Eakin et al., 2014; Eaton et al., 2016; Foley et al., 2016; Greaves et al., 2008; Hardcastle et al., 2013; Kumanyika et al., 2012; Logue et al., 2005; Ma et al., 2013; Parra-Medina et al., 2004; Ross et al., 2012; Wadden et al., 2011). Commonly used recruitment strategies include direct mailings to patient populations, referrals from primary care providers (PCPs), and brochures available at the clinics (Ahern et al., 2016; Appel et al., 2011; Bennett et al., 2012; Christian et al., 2011; Eakin et al., 2014; Eaton et al., 2016; Foley et al., 2016; Greaves et al., 2008; Hardcastle et al., 2013; Kumanyika et al., 2012; Logue et al., 2005; Ma et al., 2013; Parra-Medina et al., 2004; Ross et al., 2012; Wadden et al., 2011). However, response rates of these recruitment strategies for men and women are not widely reported in the literature.
The present study compares recruitment response characteristics across men and women for a behavioral weight loss trial conducted within 36 rural primary care clinics. Comparisons across men and women are made for response rates to direct mailings, study referral sources, screening, eligibility, and enrollment rates, and baseline characteristics. This study directly compares recruitment response metrics for men and women in a primary care behavioral weight loss trial.
Methods
REPOWER (Rural Engagement in Primary Care of Optimizing Weight Reduction) is a pragmatic cluster randomized trial investigating three care delivery models of a behavioral weight loss intervention (Befort et al., 2016). The study was approved by a central Institutional Review Board (IRB) and the VA Nebraska-Western Iowa IRB. Primary recruitment strategies included direct mailings and in-clinic referrals by PCPs. Direct mailings were sent to patients identified by each clinic as potentially eligible patients based on age (20–75 years old), obesity status (body mass index [BMI] 30–45 kg/m2), rural zip code, and a clinic visit within the past 18 months.
Patients who were interested in the study contacted the central study team via voicemail, email, or opt-in postcard. The central study team responded to interested patients, provided them with additional information about the study, and gave them the opportunity to screen for eligibility. Patients screening eligible could then enroll in the study after receiving clearance to participate from their PCP and completing a BMI verification visit at their primary care clinic. Full recruitment details are previously described (Befort et al., 2020).
Measures and Analysis
Direct mailing response rates were calculated as the percent of patients sent a mailing (minus undeliverable mailings; n = 197) who contacted the study. Referral source was determined via self-report and categorized as direct mailing, in clinic referral, or other (friends/family, clinic websites, local advertising, and social media). Screening rate was calculated as the percent of patients contacting the study who chose to screen for eligibility; eligibility rate is calculated as the percent of patients screened who were eligible for participation; and enrollment rate is calculated as the percentage of eligible patients that enrolled in the study. Descriptive statistics, t-tests, and chi squared analyses were used to characterize gender differences using IBM SPSS Statistics 23 with p < .05 and 95% CI.
Results
Mailing Response
The mailing responses rate was lower for men (n = 515/6598, 7.8%) compared to women (n = 1470/8319, 17.7%), p < .001. Additionally, men were more likely than women to respond to the mailing by opt-in postcard (64.6% vs. 56.8%, respectively), and less likely to respond by phone (33.9% vs. 39.5%, respectively), p = .002; see Table 1.
Mailing Response Rate and Mode of Responding, by Gender a .

Note. aMailing recipients with missing gender information (n = 159) were excluded.
Respondents with missing mode of contact (n = 41) were excluded.
Other response category includes email and social media.
Referral Source
A total of 587 men and 1839 women contacted the central study team. Compared to women, men reported higher rates of referral from mailings (76.6% vs. 66.8%) and lower rates of referral by their PCP (15.2% vs. 21.6; p < .001); see Table 2.
Referral Source of Individuals Who Contacted Study, by Gender a .
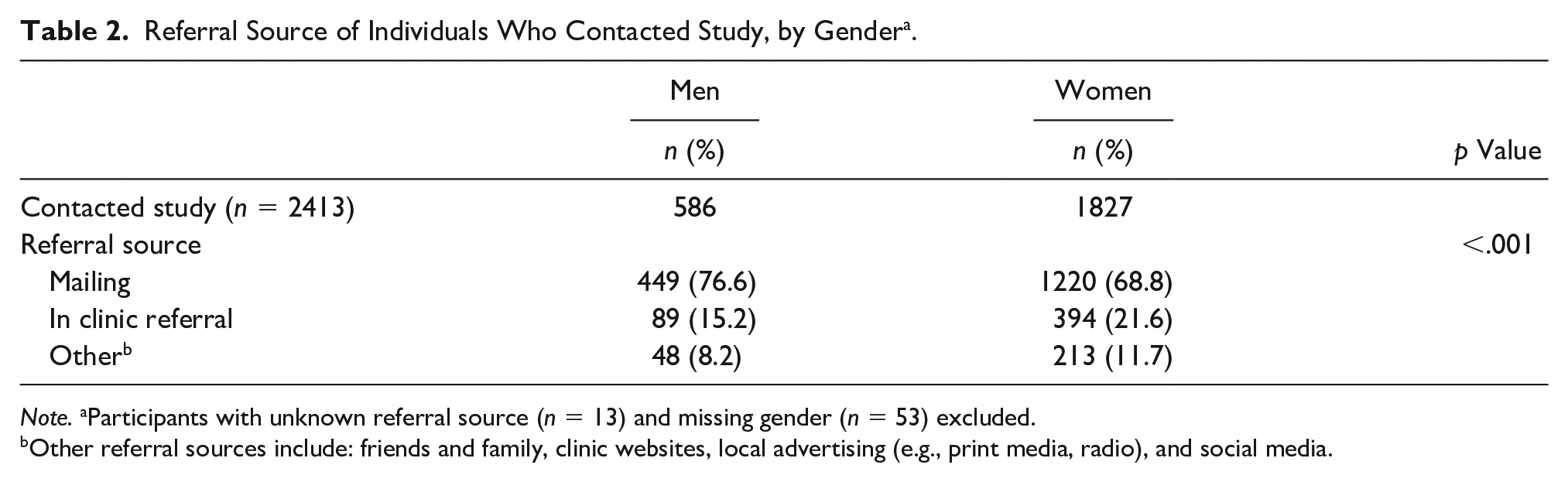
Note. aParticipants with unknown referral source (n = 13) and missing gender (n = 53) excluded.
Other referral sources include: friends and family, clinic websites, local advertising (e.g., print media, radio), and social media.
Screening, Eligibility, and Enrollment Rates
Men and women who contacted the central study team had similar rates of proceeding to screening (78.2% vs. 80.6%, respectively), being eligible (92.6% vs. 91.1%), and enrolling in the trial (78.5% vs. 81.9%). Comparisons of screening, eligibility, and enrollment rates by gender were also examined within referral source subgroups (mailing versus in clinic referral). Again, no difference between men and women was observed (Table 3). Both men and women were more likely to proceed to screening when they were referred in clinic by a PCP (93.3% and 95.4%, respectively) versus by mailing (74.2% and 73.9%), p’s < .001. Among enrolled participants (n = 333 men and 1099 women), men and women had similar BMI, but men were older (p < .001), more likely to be married (p = .04), and more highly educated (p = .01) compared to women (Table 4).
Screening, Eligibility, and Enrollment Rates by Gender and Referral Source a .

Note. aOther referral sources were not included in this table.
Characteristics of Enrolled Participants, by Gender (n = 1432).

Discussion
Men have largely been underrepresented in weight loss trials, and more effective means of recruiting them are needed. Although direct mailing was an effective recruitment strategy overall in this study, men were about half as likely as women to respond to direct mailings. When men did respond, they were more likely to respond via opt-in postcard versus by phone. Similarly, another primary care-based behavioral weight loss program sent direct mailings and found a higher response rate among women (28.6%) compared to men (19.7%; Hardcastle et al., 2008). Other weight loss trials that recruited with direct mailings have not reported gender-specific response rate; however, women enrolled at higher rates compared to men (Ahern et al., 2016; Ross et al., 2012). These findings indicate that direct mailings alone may not be sufficient for recruiting men and women equally and that additional cost-effective outreach recruitment strategies are necessary to target men. One example of this is from Crane et al. (2020) who recruited for a weight loss trail using community-wide outreach; they reported that strategic radio ads accounted for recruiting 50% of men screened versus only 6% of women screened. Similarly, another weight loss intervention recruiting only men found that a 1-week newspaper ad campaign was the most effective, leading to 67 (65.7%) enrolled men compared to the 35 (34.3%) enrolled from worksite recruitment, email newsletters, social media, and recruitment posters combined (Rounds & Harvey, 2019). Future studies will need to investigate the role of these additional strategies within the context of recruitment in tandem with PCP referrals.
Our findings indicate that men were less likely to report being referred by their PCP than women. Comparisons for this finding is difficult to make across existing literature due to many primary care weight loss trials not reporting the number of men and women directly recruited by PCP referrals (Ahern et al., 2016; Appel et al., 2011; Bennett et al., 2012; Christian et al., 2011; Eakin et al., 2014; Foley et al., 2016; Greaves et al., 2008; Hardcastle et al., 2013; Kumanyika et al., 2012; Logue et al., 2005; Ma et al., 2013; Parra-Medina et al., 2004; Ross et al., 2012; Wadden et al., 2011). Only one behavioral weight loss study was identified that exclusively recruited through PCP referrals allowing for comparisons of enrollment rates across gender as a result of PCP referrals. In that study, 211 participants were enrolled, of which only 21% were men (Eaton et al., 2016). It is uncertain if Eaton et al.’s (2016) lower proportion of enrolled men is due to PCPs referring fewer men than women, if PCP referrals are less effective for engaging men to enroll than they are for women, or a combination of the two. However, the present study’s finding that participants referred by their PCP proceeded to screening and enrollment at a higher rate compared to those referred by mailings regardless of gender indicates that increasing the PCP’s role in recruiting men is one possible strategy to increase men’s participation in future weight loss interventions.
We found that screening, eligibility, and enrollment rates did not differ between men and women after initial contact was made. This finding suggests that if men can be engaged during the recruitment process, men’s enrollment should improve proportionally. Recruitment strategies for men ultimately need to consider that men report being less likely to perceive themselves as overweight or obese (Tsai et al., 2016), and report being less likely to engage in health-seeking behavior (Banks & Baker, 2013; Galdas et al., 2005; Thompson et al., 2016; Wang et al., 2013; Yousaf et al., 2015) compared to women. In addition, men report different motivators (e.g., to enhance physical activity and strength training) and barriers (e.g., negative perceptions of “dieting” or giving up screen time; Rounds et al., 2018) associated with weight management. As such, recruitment materials and verbal communication from providers should be tailored to meet perceptions and needs of men.
Special consideration may be necessary when recruiting younger men. Among the enrolled participants, men were older than women. Younger men compared to older men have lower rates of health-seeking behaviors (Mackenzie et al., 2006; Thompson et al., 2016; Yousaf et al., 2015), which may make them more difficult than older men to recruit through primary care practices. E-mail recruitment, in addition to mailings, may be effective for younger adults (Tate et al., 2014); however, response rates to mailings and emails have not been reported across men and women and different age groups. Future research will need to investigate the role of alternative recruitment strategies across sex and age groups.
A limitation of this study is the predominately white non-Hispanic sample from rural Midwestern communities; further research is needed to verify these findings in more ethnically and geographically diverse populations. Additionally, the number of actual PCP referrals for men and women is unknown in this study; thus, it cannot be determined the extent to which PCPs referred fewer men and/or if men were less likely than women to contact the study after being referred. Strengths of the study include the large sample size across numerous primary care settings and the important contribution to a very limited literature on recruitment of men.
In conclusion, compared to women, men were less likely to respond to direct mailings, more likely to respond by opt-in postcard versus phone, and less likely to report their PCP referred them. However, men who contacted the study had similarly high rates of enrollment compared to women. Physician referrals may be a valuable tool in bolstering male recruitment into future practice-based lifestyle interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The parent trial is funded by the Patient Centered Outcomes Research Institute (OTO-1402-09413).